
Abstract
Anxiety disorders are among the most common pediatric mental health concerns, affecting nearly one in ten U.S. children, and often present as unexplained somatic complaints in school health offices. In rural Montana, limited access to behavioral health care compounds these challenges. This quality improvement project tested a nurse-led case-finding protocol (≥3 unexplained somatic visits in 6 weeks) followed by targeted anxiety screening using the Screen for Child Anxiety Related Emotional Disorders (SCARED) administered in both child self-report (SCARED-c) and parent-report (SCARED-p) versions, within a Screening, Brief Intervention, and Referral to Treatment (SBIRT) framework. Of 430 students, eight met case-finding criteria, six completed screening, and five screened positive. All received a nurse-delivered brief intervention and counseling referral. Guided by Plan–Do–Study–Act cycles, the project demonstrated feasibility, sustainability, and the critical role of school nurses in early anxiety recognition within resource-limited settings.
Keywords
Anxiety disorders are among the earliest and most prevalent psychiatric conditions in children, with onset commonly before age 11 (Lebrun-Harris et al., 2022). In the USA, pediatric anxiety diagnosis increased by 27% between 2016 and 2020, affecting nearly one in ten children, exceeding global prevalence estimates (Garcia-Adasme et al., 2021; Merikangas et al., 2009). The COVID-19 pandemic further amplified this burden, as depressive and anxiety symptoms among youth doubled, and approximately 20% reported clinically significant anxiety symptoms (Fortuna et al., 2023).
Despite the availability of effective treatments, access to care remains limited, particularly in rural settings. In Montana, nearly all counties are designated mental health professional shortage areas, and fewer than 100 psychiatrists serve the entire state, leaving many communities without adequate behavioral health resources (Montana Healthcare Foundation [MHCF], 2024, p. 5). These system-level constraints are reflected at the local school level, where existing mental health supports, including a school counselor, a district therapist, and a therapist from a federally qualified health center, are stretched beyond capacity in a high-demand environment. Recent legislative requirements mandating parental consent prior to performing a mental health evaluation in clinical or nonclinical settings have further constrained early identification efforts (Montana Code Annotated § 40-6-702(1)(a)(iv), 2025). Although evidence-based interventions such as cognitive-behavioral therapy (CBT) and selective serotonin reuptake inhibitors (SSRIs) are available, fewer than half of affected children receive appropriate treatment (Walter et al., 2020).
At the project site, a rural Montana elementary school serving approximately 430 students, nearly all students (97%) qualified for free or reduced-price lunch, according to district administrative records (2024), indicating concentrated socioeconomic disadvantage, a well-established risk factor for pediatric anxiety and other mental health disorders (Bitsko et al., 2022). Further, access to behavioral health services was limited to a single school counselor, a district therapist, and intermittent support from a federally qualified health center. The school nurse reported frequent student visits for unexplained somatic complaints, yet no standardized process existed to identify anxiety or guide referral outside of crisis-based pathways. Recent state requirements for written parental consent further constrained universal mental health screening, thereby increasing reliance on nurse judgment during routine health office visits. Together, these local conditions created a clear need for a feasible, nurse-led approach to early anxiety identification and response.
Anxiety in children frequently presents as somatic complaints, including headaches, stomachaches, and fatigue (Li et al., 2021; Sackl-Pammer et al., 2018). These physical symptoms often serve as early indicators of distress and frequently prompt visits to the school health office, positioning school nurses as key professionals in early identification and response.
Surveys indicate that although school nurses commonly identify anxiety as the most prevalent mental health concern among students, few report using standardized assessment tools or structured interventions, and most express a need for additional training (Muggeo & Ginsburg, 2019). These findings also align with national surveys indicating that the scope of school nursing has expanded to include behavioral and mental health assessment, intervention, and care coordination (Hoskote et al., 2022; National Association of School Nurses [NASN], 2022).
Recognizing the need for earlier identification and intervention, the U.S. Preventive Services Task Force now recommends routine anxiety screening for children and adolescents beginning at age 8 (U.S. Preventive Services Task Force, 2022). In addition, the American Academy of Pediatrics recommends universal suicide risk screening for youth ages 12 and older and targeted screening for children ages 8–11 when clinically indicated (American Academy of Pediatrics, 2023). Consistent with these recommendations, NASN affirms that student behavioral health and wellness must be prioritized and that school nurses are frequently the initial point of access for identifying mental health concerns, determining appropriate interventions, and coordinating referral and follow-up care (National Association of School Nurses [NASN], 2022). Despite this consensus across national clinical and professional guidance, barriers such as limited training, lack of validated tools, and challenges with parental consent continue to impede the adoption of school-based mental health screening (Hoskote et al., 2022; Muggeo & Ginsburg, 2019; Siceloff et al., 2017; Villarreal & Peterson, 2025).
Students with mental health concerns frequently present to the school health office with psychosomatic complaints, and school nurses are positioned to conduct mental health assessments, apply screening tools, and initiate timely referral and follow-up when indicated (Perron et al., 2021). While universal screening for anxiety or mental health risk has been implemented in several middle and high school settings to identify need and refer students for support (Connors et al., 2022; Drymond et al., 2023; School Mental Health Quality Guide [NCSMH], 2023), there is less evidence of nurse-led Screening, Brief Intervention, and Referral to Treatment (SBIRT) style protocols in these age groups that include brief intervention and treatment referral. This quality improvement (QI) project focuses on this important gap by implementing and evaluating a school nurse-led SBIRT protocol using the Screen for Child Anxiety Related Emotional Disorders (SCARED) tool in a rural Montana elementary school. Guided by the Plan-Do-Study-Act (PDSA) framework, the project assessed feasibility, identified process barriers, and evaluated early outcomes, contributing novel evidence to support early, school-based mental health interventions in resource-constrained settings.
Methods
Quality Improvement Framework
This quality improvement (QI) project used the PDSA framework to develop and implement a school nurse-led SBIRT protocol to identify anxiety in a rural elementary school. PDSA cycles were used, short, iterative tests of change to refine workflow, materials, and role responsibilities in real time. The six-week project timeline aligned with an elementary term segment and staffing feasibility and is consistent with rapid-cycle QI conventions used to test and adapt processes in school settings (Langley et al., 2009; Nevedal et al., 2021).
Setting and Context
The project was conducted at a rural Montana elementary school serving approximately 430 students in grades K-6, 97% of whom qualified for free or reduced lunch, indicating most are living below the federal poverty line. The implementation window was January 22-March 1, 2024. The Frontline electronic health record (EHR) system was used to document student health office visits, including somatic complaints.
Project Team
The intervention team included a Doctor of Nursing Practice (DNP) student, the lead school nurse, the school principal, the school counselor, the district mental health therapist, and a licensed therapist from a Federally Qualified Health Center (FQHC). The school nurse received a 60-min orientation covering SCARED administration/scoring, the brief-intervention script, and documentation, including role-play and a laminated cue card (breathing, progressive muscle relaxation prompts, and cognitive coping statements). The substitute nurse received 15 min of training prior to coverage days. The DNP student conducted fidelity spot checks weekly (correct scoring and delivery of key psychoeducation elements).
At project launch, two full-team stakeholder meetings were held to co-design the SBIRT protocol and develop parent-facing communication materials. During the six-week implementation period, the DNP student and school nurse met weekly to review the case-finding and screening process, address workflow challenges, and collect project data (six meetings in total). Additionally, project initiation and wrap-up meetings were conducted with the DNP student, school nurse, and principal to focus on protocol review and outcome evaluation. Regularly scheduled meetings allowed the team to track progress, troubleshoot challenges, and keep stakeholders actively involved in the process.
Ethical Considerations
The Montana State University Institutional Review Board reviewed this initiative and issued a Quality Improvement (QI) determination on January 5, 2024 (Protocol Ref #1124), concluding that it did not meet the federal definition of human subjects research under 45 CFR 46 and therefore did not require IRB oversight. The purpose was to improve a local clinical workflow within one school, using an existing, evidence-based tool (SCARED) and standard nursing practices; no randomization, experimental procedures, or data collection beyond usual care occurred. The DNP student accessed only aggregate, de-identified process data, and no identifiable information left the school system. Independent of the university determination, district policy required active parental consent for participation and adherence to FERPA- and HIPAA-aligned privacy safeguards. These requirements were fully followed.
Eligibility Criteria
Students were eligible for screening if they met all of the following criteria: (1) enrolled in grades 3–6 (ages 8–12), (2) English-speaking, (3) not currently receiving behavioral health services, and (4) had visited the nurse three or more times for unexplained somatic symptoms (e.g., headache, stomachache, fatigue) during the six-week project window. Students with chronic medical diagnoses explaining their symptoms or those already receiving behavioral health services were excluded.
Screening Tool
Anxiety was assessed using the SCARED tool. The tool was selected because of its robust psychometric properties in youth, support in U.S. evidence reviews, and the American Academy of Child and Adolescent Psychiatry (AACAP) clinical practice guideline (Birmaher et al., 1999; Viswanathan et al., 2022; Walter et al., 2020). The tool was administered in both child self-report (SCARED-c) and parent-report (SCARED-p) versions. Both the child and parent versions include 41 parallel items, each rated on a 3-point Likert scale from “not true” to “very true.” Scores range from 0 to 82, with a threshold of 25 or higher indicating clinically significant anxiety (Birmaher et al., 1999).
Case-Finding and Targeted Testing Procedures
Screening refers to the systematic use of a tool or process with all students or a defined population subset, whereas case-finding involves assessing individuals who present with identifiable risk indicators in routine clinical practice (National Center for School Mental Health [NCSMH], 2023; Speechley et al., 2017). In this project, recurrent somatic nurse visits functioned as the case-finding trigger, followed by targeted SCARED testing, brief nurse-delivered intervention, and referral within an SBIRT workflow. Each week, the school nurse reviewed EHR logs to identify eligible students and contacted their guardians by phone using a standardized script. Guardians could choose one of the following participation methods:
Complete and return the SCARED-p form and signed consent at home, after which the nurse administered the SCARED-c at school. Schedule an in-person appointment for the guardian and child to complete both SCARED-p and SCARED-c with the nurse. Request forms for completion with a primary care provider.
For in-school screening, the nurse administered and scored the SCARED-c immediately. All students who screened positive advanced to the brief intervention step of the SBIRT protocol.
School Nurse–Led Brief Intervention
For students who screened positive for clinically significant anxiety, the school nurse delivered individualized, evidence-based brief interventions. These interventions included psychoeducation about anxiety and its somatic manifestations, introduction of coping skills, feelings identification, and environmental supports. Each nurse-led intervention was intentionally limited to approximately 3–5 min to emphasize feasibility and minimal interruption to academic time.
Psychoeducation was delivered one-on-one by the school nurse during each student's screening appointment. The nurse used age-appropriate language and visual diagrams to explain the mind-body connection and the physiological basis of anxiety. These sessions included discussion of how anxiety manifests physically, normalization of these experiences, and the relationship between thoughts, feelings, and physical sensations.
The nurse modeled and practiced deep breathing, progressive muscle relaxation, and positive self-talk with each student. For some, these techniques reinforced coping skills previously introduced in classroom social-emotional learning lessons; for others, they were entirely new. Each student received guided practice to ensure proper technique and understanding of when to apply these strategies.
Students demonstrating greater functional impairment at school (e.g., frequent health office visits or academic disruption) received daily nurse check-ins for one week before tapering to weekly sessions. Students with milder symptom interference were scheduled for weekly check-ins from the start, with frequency adjusted as needed based on student progress or parent/teacher feedback. To support skill application both at school and home, each student created a personalized coping kit. Each coping kit included simple self-regulation tools, such as a stress ball, a small fidget, and a card with breathing exercises and affirmations. In collaboration with teachers, the nurse also set up a “coping corner” in the nurse's office, a quiet space with bean bags, sensory bottles, and charts showing calming strategies that students could use when they felt overwhelmed.
Teachers were informed about which techniques had been taught to individual students, allowing for reinforcement of these strategies during classroom activities. By working together, the nurse and teachers helped align classroom strategies with those offered in the nurse's office, providing students with a more streamlined experience of support throughout the day.
Referral to Treatment
After the brief nurse-led intervention, students who screened positive for anxiety were referred for further mental health services, in line with the school's existing protocol. The nurse communicated screening results and clinical concerns to guardians and obtained consent for referral to the school guidance counselor or, when appropriate, a community-based mental health provider. Referral decisions were individualized based on student need and resource availability.
The school nurse collaborated with the counselor to ensure timely follow-up and coordinated care. Documentation of referrals, communication with guardians, and barriers to accessing further treatment were recorded on individual student tracking forms and in the Frontline EHR.
Students referred to counseling or outside therapy continued to have access to nurse-led check-ins, conducted daily or weekly, as well as support within the school. The nurse shared educational materials and local mental health contacts with families to encourage continued follow-up. This multi-tiered approach gave students both immediate support at school and clear pathways to longer-term care.
Data Collection and Analysis
Demographic data collected were limited to student grade and gender to protect confidentiality. All data were entered into the Frontline EHR and a Microsoft Excel spreadsheet. The Frontline EHR and Excel spreadsheet tracked student eligibility, parent screening approach, consent status, SCARED screening completion and scores, and all referral actions.
Quantitative data included the number of students eligible for anxiety screening, the number of students screened (with returned consent/assent), the number of students who screened positive (SCARED-p or SCARED-c score ≥25), and the number of days from initial identification to screening completion. Identification rate was calculated as the percentage of students for whom the nurse-initiated screening consent communication out of all identified as eligible. Referral rate was calculated as the percentage of students referred for treatment out of those testing positive. Referral completion rate was the percentage of students connected with mental health support out of those referred.
Data were systematically collected using structured nurse tally sheets and individual student trackers. The weekly Nurse Data Tally Sheet captured core process metrics, including number of students identified, guardian response to invitation (proceed/not interested/could not reach), completed SCARED screenings, positive/negative results, referrals made, and method of identification (e.g., somatic symptoms). Additional notes and barriers were recorded weekly.
Individual Student Trackers documented key process milestones and communication attempts for each student, including number of somatic visits to the school nurse, guardian contacts, screening form distribution and return, consent status, screening and intervention completion, and referral actions, with space for notes on barriers or unusual occurrences. Referral completion status was defined as documented engagement with a school-based or community mental health provider following referral.
All project data were stored on the district's encrypted, password-protected drive. Paper tally sheets, and individual student tracker sheets were filed in folders secured in the nurse's locked cabinet; the office door was locked when not occupied. Access was limited to the school nurse and the DNP student. The spreadsheet contained only nonidentifiable variables (grade, gender, screening status) and no names or student identifiers. No data were shared outside the district.
Qualitative Data Collection and Analysis
Qualitative data were collected through multiple sources to evaluate implementation barriers and stakeholder experiences. Primary data sources included narrative comments and perceived barriers to SBIRT implementation, as tracked weekly on tally sheets, student trackers, and Pareto charts (bar charts ordering causes from most to least frequent to identify the “vital few” contributors).
Structured feedback on acceptability and feasibility was obtained through standardized questions administered to the school nurse at the conclusion of the implementation period. These questions assessed the perceived utility, integration with existing workflows, adequacy of resources, and sustainability of the SBIRT protocol. Additional qualitative feedback was gathered through open-ended email questionnaires completed by the nurse and direct communications from parents and teachers, which were documented in the weekly tally sheets.
Rapid content analysis was used to examine qualitative data (Nevedal et al., 2021). Key themes were identified through review of weekly narrative logs and stakeholder feedback. This approach provided a systematic way to capture recurring patterns related to acceptability, feasibility, and perceived value across stakeholder groups. To enrich this analysis, school staff, parents, and students were invited to share written or verbal feedback about their experiences during implementation, offering a fuller picture of the protocol's impact in the school setting.
Process Modifications Across PDSA Cycles
The SBIRT workflow was refined over three iterative PDSA cycles.
During the first cycle, the project team identified a critical procedural gap: the district's only available mental health screening consent form was specific to annual suicide screening for sixth graders. Because no consent process existed for broader mental health or anxiety screening in younger students, the team adapted and expanded the suicide screening consent to create a new, general mental health screening consent form. This revision enabled parent/guardian consent for the anxiety screening protocol and ensured compliance with district policy and state regulations.
In the second cycle, the team identified referral barriers related to the school counselor's limited capacity. To reduce delays, the school nurse took the lead in initiating referrals and coordinating follow-up care. Psychoeducational resources, including visual supports, coping kits, and classroom-based sensory tools, were introduced to strengthen accessibility and engagement.
In the third cycle, the team observed that school nurse absences resulted in referral delays and gaps in continuity. To maintain consistency, substitute nurses were trained in the SBIRT protocol so that screening and intervention could continue during staff absences.
Results
Quantitative Findings
Six of the eight identified students (75%) returned parent consent/assent forms and completed the SCARED screening tools. The time from eligibility identification to screening completion ranged from 6 to 29 days, with an average of 16.5 days. Prior to implementation, no structured case-finding trigger, standardized anxiety assessment, or defined referral workflow existed beyond nurse clinical judgment and crisis-based response. Although screening occurred within the same academic term, the delays highlighted continuing challenges in contacting families, obtaining consent, and managing staffing variability, which the team addressed through real-time process adjustments. Of the two identified students who did not complete testing, one guardian declined, and one guardian opted to monitor the student at home. An additional student met case-finding criteria but was excluded due to a chronic medical condition.
All participating students completed both the SCARED-c (child self-report) and SCARED-p (parent-report) forms. Notably, perfect agreement was observed between child and parent forms for all students: each pair of scores either both met or both fell below the clinical threshold for significant anxiety symptoms. The distribution of school nurse office visits by visit type during the pilot period is shown in Figure 1.
Screening and Intervention Outcomes
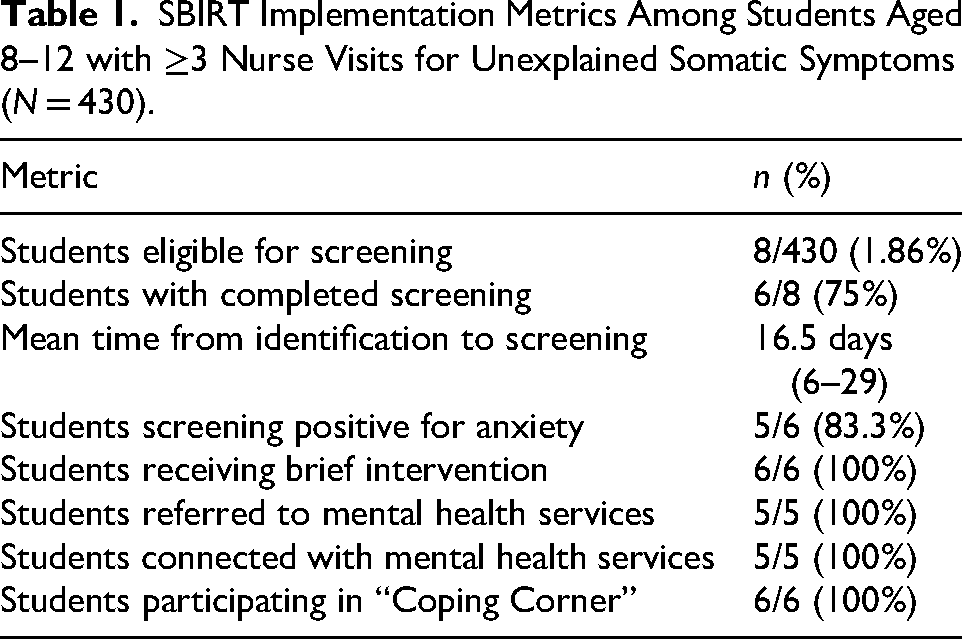
Of the six students screened, five (83.3%) scored at or above the clinical threshold (≥25) for symptoms consistent with an anxiety disorder. All five students who screened positive received a brief nurse-led intervention consisting of psychoeducation and coping skills instruction. Additionally, all five students were referred to mental health support services, including school-based counseling, family therapy, or community mental health providers, resulting in 100% referral and referral completion rates. The SBIRT workflow and screening outcomes are illustrated in Figure 2, and key process and outcome metrics are summarized in Table 1.
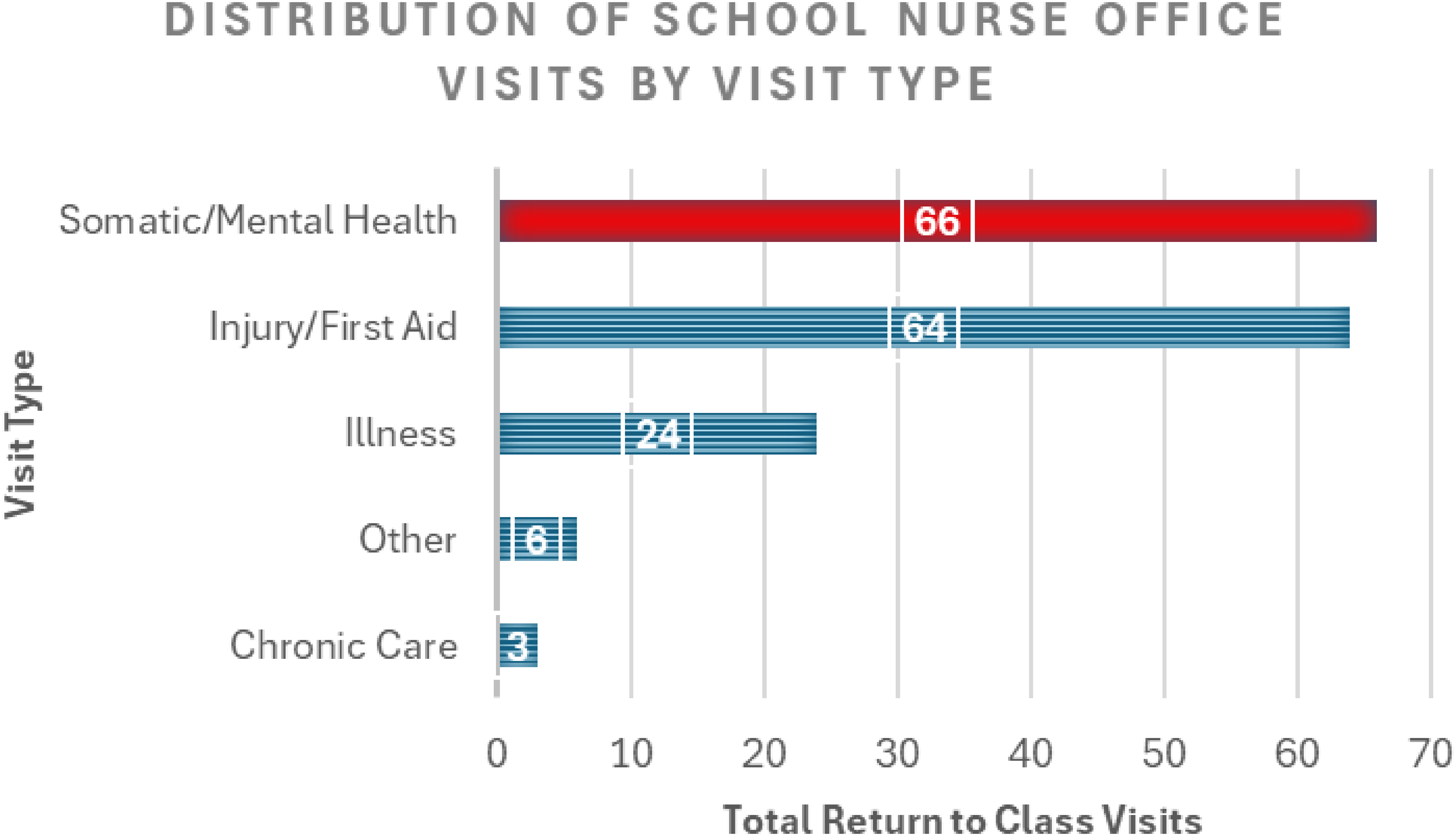
Distribution of school nurse office visits by visit type among return-to-class encounters during the pilot period (n = 163).
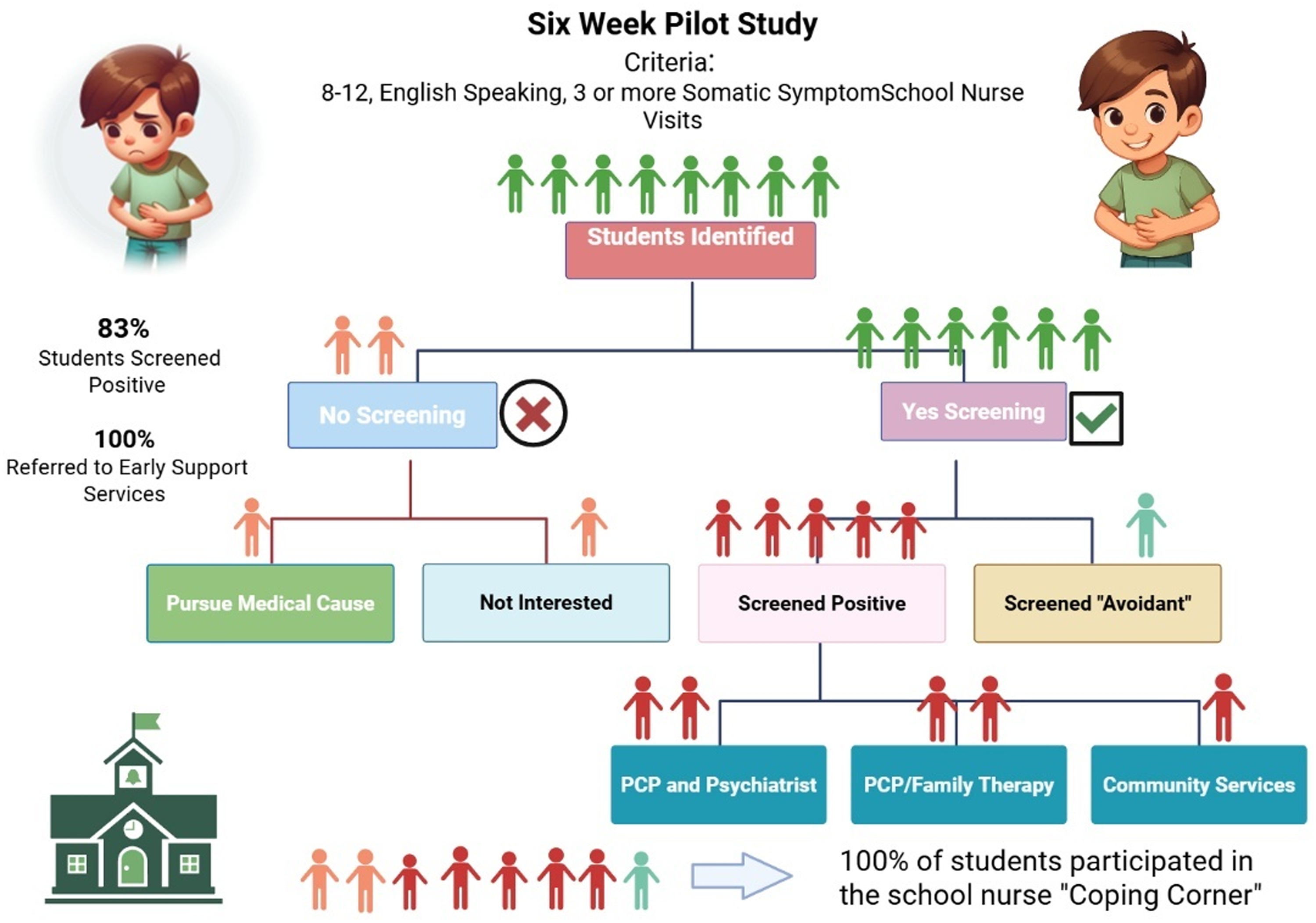
Flow diagram of the nurse-led SBIRT protocol for students aged 8–12 with ≥3 nurse visits for unexplained somatic symptoms (N = 430).
SBIRT Implementation Metrics Among Students Aged 8–12 with ≥3 Nurse Visits for Unexplained Somatic Symptoms (N = 430).
Perceived Barriers, Acceptability, and Feasibility
The quality improvement project identified several obstacles in the screening process, including scheduling conflicts, limited resources, and variations in the prioritization of individual cases. Barriers to screening and referral included the need for reminder calls to guardians to respond to requests, complete consent forms, or return the screening tool (21.4%), inability to contact a guardian (14.3%), and the school nurse's absence due to illness or other reasons (10.7%).
Qualitative Findings
Parent, Student, and Staff Feedback
Parent feedback supported the acceptability and feasibility of the nurse-led screening and response process. In one case, a parent realized, through conversations with the school nurse, that her child's somatic complaints consistently occurred when the guardian was out of town. At first, the family and staff considered a possible physical cause. The screening process, however, shifted attention to separation-related anxiety, and the student subsequently scored high on the separation anxiety subscale of the SCARED tool (Birmaher et al., 1997). This insight allowed for more targeted support and communication between the school, family, and student.
In another case, a parent who had not previously participated in school activities attended parent–teacher conferences for the first time after the school nurse reached out.
Teachers also reported an increase in help-seeking behaviors and reduced requests to leave the classroom among students receiving brief intervention and referral to treatment. Several students expressed appreciation for the coping resources provided and reported greater comfort and confidence in managing their somatic symptoms.
School Nurse Perspective
Qualitative feedback from the school nurse provided deeper insight into implementation challenges and the intervention's broader impact. She noted: The project has altered my workflow as it fills the end of my day with calls, student, teacher, [and] staff interactions. I do see how when anxiety screening continues it will slow as more students will have already been identified. I also see how we can make different improvements for student check-ins that will have the same student nurse relationship and outcome desires.
The nurse described positive effects on her professional practice and morale: My practice as a school nurse has improved my morale as I am able to see nearly instant improvements and successful coping skills being implemented. It has built nurse–parent relationships that did not exist prior to this project. Students have expressed thanks for caring for them and being an adult they can come to within the school.
She also observed changes in student engagement and trust: The kids identified are happy to check in and have me as a trusted adult in the school building.
On the screening approach, she reflected: Our inclusion criteria easily picked out possible and accurate students. I do feel as though the three somatic symptoms will lead to the most accuracy.
In describing parent engagement, the nurse reported: Four parent relationships have been very supportive and thankful. These four were open to the idea that their child could have anxiety and wanted to move forward to help get them tools/support. One parent was very much against the idea of anxiety being a possibility, but this was also a great conversation because it brought light to a possible GI issue that can be followed up on by this nurse now.
Regarding lessons learned, she noted: It is important to put an expected return date for parent screeners and consent forms. Follow up is key. With follow up I was able to identify the barrier in care being needed for [primary care provider] and help provide resources/information. It is always important to have two forms of communication as often a verbal conversation may be forgotten or not fully understood in so many health cases.
Finally, she summarized the broader value of the project: Anxiety screening is a proactive approach to our mental health crisis. Identification and referral is key to start building tools to combat additional and future mental health needs. This simple step is opening the door to making mental health real, okay, and treatable/manageable.
Discussion
This school nurse-led quality improvement project demonstrated the feasibility and value of integrating a structured SBIRT protocol for case-finding-triggered targeted anxiety testing into routine health office visits. Somatic complaints were the most common reason students saw the nurse, highlighting an important opportunity to use these visits to identify underlying mental health concerns. Implementation through Plan-Do-Study-Act cycles supported flexible adjustments to staffing limitations and workflow challenges.
The high rate of positive screenings and successful referrals points to both the appropriateness of the SCARED tool and the central role school nurses can play in connecting students to mental health services. Parent and child screening scores were closely aligned. The unusually high concordance between parent- and child-reported SCARED scores may reflect the same-week, nurse-facilitated completion process and brief psychoeducation provided to families, which could have aligned parent–child understanding of anxiety symptoms more closely than in previous research. This level of agreement was stronger than what most earlier studies have found, where parents and children typically demonstrate only moderate concordance on the SCARED (Behrens et al., 2019; Birmaher et al., 1999; Popp et al., 2017). The nurse-led, collaborative process may have played a role in helping families recognize and describe anxiety in similar ways.
Although the time from identification to intervention could be shortened, the protocol represented a clear improvement over existing practice by providing school nurses with a structured, evidence-based pathway for early anxiety identification and response during routine health office visits. This finding aligns with prior literature demonstrating that nurse-led, workflow-integrated mental health interventions can improve timeliness and coordination of care without requiring additional staffing or resources (Hoskote et al., 2022; Muggeo & Ginsburg, 2019; Perron et al., 2021). Together, these findings are consistent with the growing evidence that school nurses are essential for early detection and intervention of anxiety, particularly in rural and under-resourced communities, where access to behavioral healthcare remains limited (Bitsko et al., 2022; Thomas et al., 2025). These findings also coincide with national surveys indicating that school nurses frequently identify anxiety as a leading concern but often lack standardized tools or training to respond effectively (Muggeo & Ginsburg, 2019), as well as with broader shifts in the profession toward expanded mental health leadership roles despite persistent structural barriers (Hoskote et al., 2022). Recent evidence indicates that targeted mental health training programs improve school nurse preparedness, confidence, and implementation capacity, particularly when paired with administrative and policy support (Thomas et al., 2025).
Limitations
Requiring active parental consent likely reduced participation relative to opt-out models, which have been shown to yield higher response rates and more representative samples in school-based research (Totura et al., 2017). This project followed district policy requiring active consent. This project was conducted in a single rural elementary school with a small sample, which may limit generalizability. In addition, outcomes were assessed over six weeks, so the longer-term sustainability and impact on students remain to be determined.
Recommendations
Building on this work, future QI and research initiatives should test the approach in more diverse settings, incorporate digital and streamlined workflows, create culturally and linguistically inclusive materials, and follow students over time to assess sustained impact. Prior school-based mental health initiatives suggest that culturally responsive and linguistically tailored interventions improve engagement and acceptability among families from diverse backgrounds, particularly when delivered by trusted school personnel (Villarreal & Peterson, 2025).
Implications for School Nursing
This project filled identified gaps in the literature by providing standardized assessment tools, structured intervention and targeting training to support school nurses in meeting student mental health needs. This project demonstrates that school nurses, when equipped with structured protocols and administrative support, can deliver feasible, high-impact behavioral health interventions, consistent with NASN position statements that emphasize the nurse's role in behavioral health identification, intervention, and care coordination (NASN, 2022; Thomas et al., 2025). Embedding nurse-led SBIRT within multi-tiered systems of support may shift school nursing from reactive care to proactive, whole-child wellness.
Conclusion
This quality improvement initiative demonstrates that a school nurse–led SBIRT protocol can be feasibly implemented and sustained in a rural elementary school without additional resources. Using the SCARED tool alongside brief interventions and coordinated referrals enabled early identification of anxiety symptoms that might otherwise have gone unnoticed. Using PDSA cycles, the protocol was adjusted in real time to address day-to-day workflow challenges and was well received by students, families, and staff. These findings point to the important role of school nurses in early mental health intervention, particularly in resource-constrained communities. Broader adoption of this model could strengthen school-based behavioral health systems and improve outcomes for children with anxiety, especially in rural and underserved settings. Future efforts should test this model across diverse school contexts and incorporate digital tools to streamline consent, screening, and follow-up.
Supplemental Material
sj-docx-1-jsn-10.1177_10598405261455898 - Supplemental material for Implementation of a School Nurse-Led Case-Finding and Targeted Anxiety Testing Protocol (SBIRT-Informed) in an Elementary School: A Quality Improvement Initiative
Supplemental material, sj-docx-1-jsn-10.1177_10598405261455898 for Implementation of a School Nurse-Led Case-Finding and Targeted Anxiety Testing Protocol (SBIRT-Informed) in an Elementary School: A Quality Improvement Initiative by Donna Ruth, Margaret Hammersla and Andrea Tanner in The Journal of School Nursing
Footnotes
Acknowledgments
The authors thank the school nurse, staff, and students at the participating Montana elementary school for their support and commitment to improving student health. Gratitude is also extended to the Montana State University College of Nursing faculty, particularly Dr. Elizabeth Johnson, for their mentorship, and to the ANEW Rural Ready Nurse Practitioner Scholarship and the Behavioral Health Workforce Education and Training (BHWET) program for their financial and educational support.
Ethics Approval
Institutional Review Board determination was obtained from Montana State University (January 5, 2024), classifying the project as nonhuman subjects research under 45 CFR 46. District-level research approval was also secured. Written guardian consent and child assent were obtained prior screening.
Author Contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data are not publicly available to protect student privacy under FERPA and HIPAA guidelines.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.