
Abstract
This study explored concussion knowledge, education, and organizational policies among school nurses (n = 12) and youth athletic program leaders (n = 14) in the Philadelphia area from June-September 2023. Using semi structured interviews, questionnaires, and thematic analysis, three themes emerged: (1) School nurses and youth athletic program leaders know their roles in concussion management but welcomed more education. (2) System-level gaps in concussion oversight beyond organized sports exist for younger children, those injured via non-sport related mechanisms, in recreational settings, or during free play. (3) Challenges in concussion care exist including lack of concussion awareness, parental engagement, language barriers, and access to health care. Although both school nurses and athletic leaders generally possess baseline concussion knowledge, they identified missed cases, particularly non sport related injuries, and insufficient return to play or return to learn procedures in recreational environments. Findings highlight the need for targeted, community specific concussion education to address disparities in youth concussion management.
Introduction
Concussion, a mild traumatic brain injury, is a common childhood injury impacting millions of youth under the age of 18 every year. These injuries significantly impact the day-to-day lives of the pediatric population and therefore require timely and accurate diagnosis, treatment, follow-up, and ongoing support to limit potential sequela impacting recovery outcomes. Despite the high rates of children sustaining a concussion through sports, around one-third experience a concussion through non-sports-related mechanisms such as non-organized play in recreational settings (Roby et al., 2024). Differences in concussion diagnosis and care have been observed across mechanisms of injury. Youth injured outside of organized sports are more likely to experience later presentation to specialty care, less concussion-specific diagnostic evaluation, greater symptom burden, more frequent visio-vestibular abnormalities, and greater disruption to daily functioning, including school participation and sleep (Means et al., 2021; Roby et al., 2024). Further concussion disparities have been identified in the literature. Non-Hispanic black youth have been noted to be less likely to sustain a concussion from sports-related activities. Differences in exposure and type of sport participation related to socioeconomics can contribute to racial and ethnic disparities in concussion education and incident reporting (Haarbauer-Krupa et al., 2018; Wallace et al., 2021), access to care, diagnosis, and follow-up (Mohammed et al., 2023; Pate et al., 2022).
“Youth sport” broadly includes organized athletic activities like club sports or high school teams (e.g., soccer team), as well as informally organized sports activities that occur at recreational centers or in after-school programming. Youth living in under-resourced areas or in families with lower incomes have been challenged by the rising costs of organized sports participation (The Aspen Institute Project Play, n.d.), more frequently are in need of after-school or summer childcare, and as a result, may access this type of less structured programming. In addition, this type of free play and less formal sports activity is part of the fundamental structure for typical days for all youth during school.
In recreational and educational settings, responsible parties such as school nurses, youth athletic program leaders, like coaches and recreation center staff, play a key role in injury prevention and identification. Youth athletic program leaders are responsible for teaching proper techniques and strategies for concussion prevention, such as the age-appropriate introduction of sport-specific strategies like heading the ball in soccer (e.g., intentional contact by the head to redirect the ball) and body checking in hockey (e.g., intentional physical contact used to separate an opponent from the puck). If an injury occurs, youth athletic program leaders need skills in injury recognition, removal from play, and communication with parents regarding next steps. Youth athletic program leaders are also responsible for integrating their athletes back into play after an injury. A systematic review of literature published between 2010 and 2018 by Feiss et al. (2020) revealed that coaches are often knowledgeable about physical signs and symptoms of concussions, but there are gaps in knowledge regarding the emotional symptoms of concussion, return-to-play protocols, and differences in concussion recovery between adults and children (Feiss et al., 2020). There has been much more attention paid to youth concussion in more recent years. Understanding if these gaps remain is important, allowing targeted interventions, such as those directed towards increasing youth athletic program leader communication with youth athletes and their families on concussion topics, to be implemented (Kroshus et al., 2023).
Similarly, school nurses play an integral role in concussion care, including identifying any potential concussion-related injuries, supporting concussion recovery, and coordinating the return-to-learn (RTL) and return-to-play (RTP) processes (National Association of School Nurses, 2021). School nurses are often knowledgeable about concussion identification and management, but gaps exist, including knowledge of up-to-date concussion evidence and advances in clinical practice recommendations, a lack of school support and resources, and inconsistent concussion recommendations from community health care providers (Hess et al., 2024; Pietz et al., 2021; Welch Bacon et al., 2018). As was seen with coaches, educational interventions have been demonstrated to improve pediatric concussion knowledge and management skills among school nurses, however those effects have not been sustained in the absence of any standardized mandate (Berz et al., 2022).
Currently, concussion educational requirements for individuals working within youth athletics depend on individual state laws, which usually apply to interscholastic sports or alignment of a club team with a National Governing Body (NGB) which have their own policies on concussion education (Asgari et al., 2025). Recreational settings (e.g., YMCA, community recreational programs) are neither interscholastic nor under the NGB umbrella, and thus, are not covered by state laws or NGB regulations. Similarly, continuing education on concussion for school nurses may not be specifically required by school districts, and thus, they may also lack current information on latest advances in concussion care. Given that youth sustain concussions across diverse contexts, including organized sports, non-sport-related mechanisms such as motor vehicle crashes, and recreational activities and free play, it is important to understand gaps in concussion knowledge for practitioners working with youth in these settings.
To further explore the nature of these gaps, the present study aimed to describe perceptions of school nurses and youth athletic program leaders from predominantly urban settings about their concussion knowledge, education, and organizational policies in concussion prevention, identification, and recovery in order to identify potential barriers affecting concussion-related care for children they support.
Methods
Study Design and Participants
Semi-structured qualitative interviews were conducted with youth athletic program leaders and school nurses responsible for youth in school settings, recreational organizations, and club sports. Participants were recruited through existing relationships with youth sports organizations and recreation centers within the Philadelphia area and the Pennsylvania School Nurses Association through flyers, word of mouth, and email. Eligible participants included youth athletic program leaders (i.e., coaches, supervisors, volunteers) and school nurses who worked in Philadelphia or the surrounding communities. Prior to the interview, participants completed a brief electronic survey (25 items for nurses and 26 items for youth athletic program leaders) via REDCap containing self-reported demographic information, including education level, medical experience, previous experiences with concussion education and care, and self-reported ratings on concussion knowledge and comfort levels caring for youth with concussion. Participants provided electronic documentation of consent before completing the survey and audio-recorded interviews. The study protocol was determined to be exempt by the Children's Hospital of Philadelphia Institutional Review Board (Approval No. 23-020900, Philadelphia, PA).
Interview Guide and Data Collection
The interview guide was developed by the study team and consisted of open-ended questions and a series of discussion probes designed to explore concussion knowledge, education, and organizational policies related to concussion prevention, identification, and recovery, as well as perceived barriers to care. Interviews followed a semi-structured format with approximately 19 core open-ended questions; follow-up prompts and probes were used flexibly to clarify responses and to explore participants’ experiences in greater depth, resulting in variability in the total number of questions asked across interviews. The same interviewer conducted all interviews remotely, which were recorded via a conference call platform, audio transcribed, and de-identified. Transcripts were reviewed by the study team against audio files to verify accuracy and uploaded to NVivo (version 12) to manage coding and thematic analysis. The team applied a descriptive content analysis approach (Hsieh & Shannon, 2005). A code book was developed for each cohort, youth athletic program leaders and school nurses, based on the interview guide, with new codes added as the initial interviews were analyzed. One research team member coded all interviews. A second research team member coded 20% of interviews. Discrepancies were reconciled and definitions were refined. Overall, inter-rater coding resulted in ≥90% congruence. Themes were developed based on school nurse and youth athletic program leader responses within coding categories.
Results
Participant Characteristics
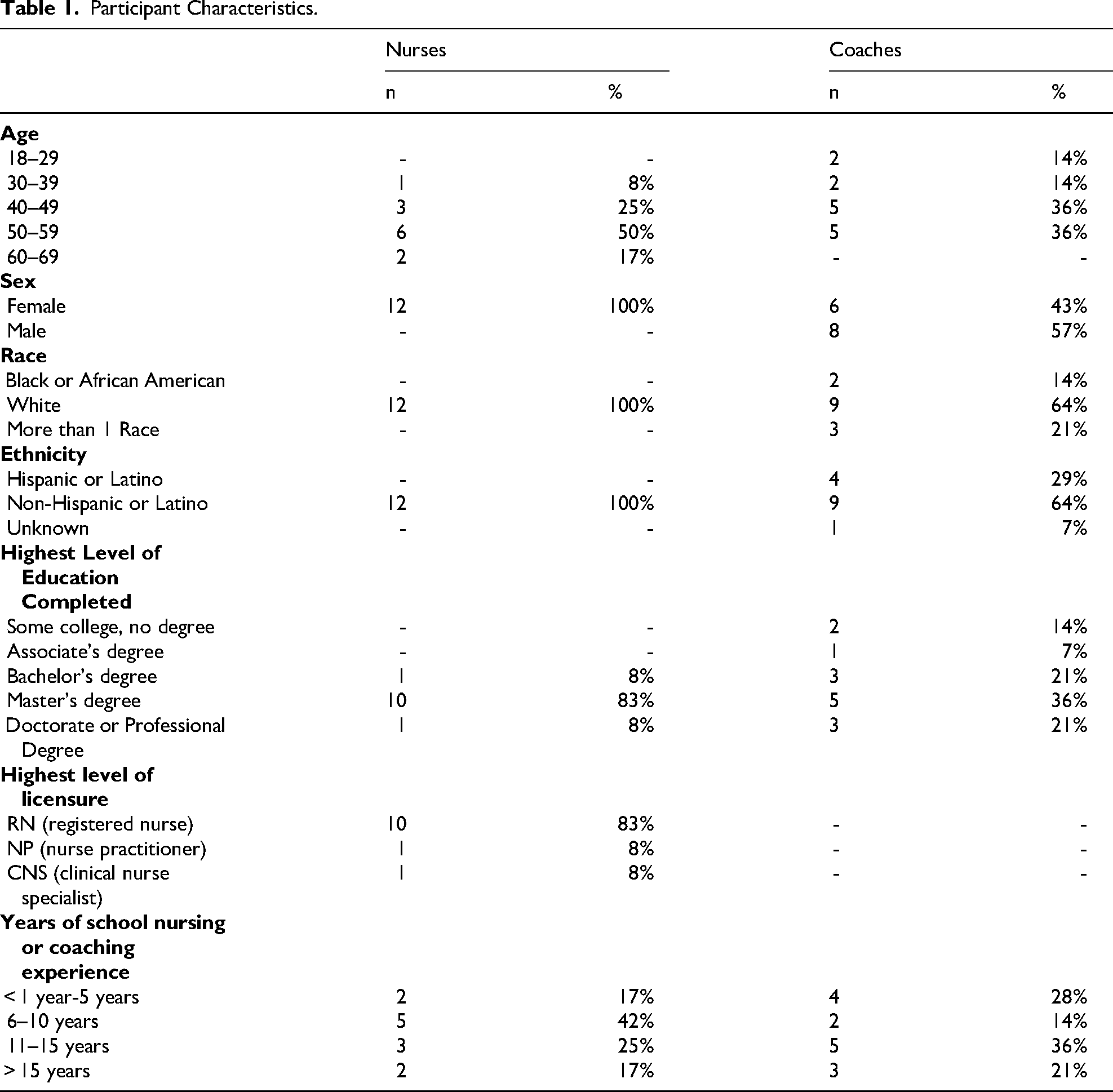
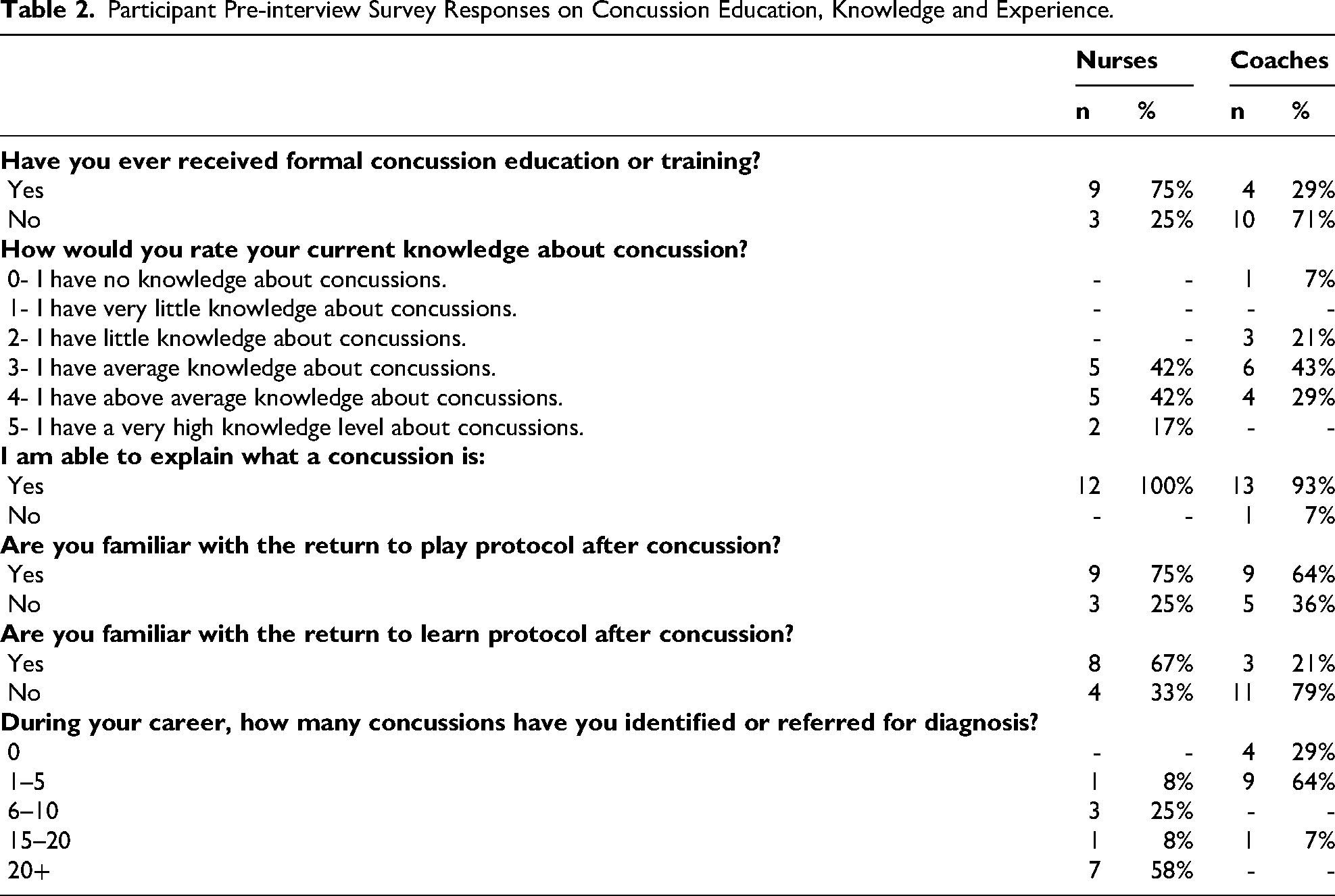
The sample of 26 participants included school nurses (n = 12, 100% female) youth athletic program leaders (n = 14, 43% female), ages 23–62 (median: 49.5) years from Philadelphia County and the surrounding area. Interviews were conducted between June and September 2023 and lasted 41.5 min on average (range: 17–72 min). One youth athletic program leader participant was excluded from analysis due to insufficient interview audio data. Table 1 outlines the demographic characteristics of the sample and education/licensure levels. Many of the youth athletic program leaders supervised or coached multiple sports, with the most common being soccer (64%) and basketball (36%). Table 2 includes participant education, knowledge, and experience with youth concussion as reported in the pre-interview survey. Of note, 25% of the school nurses and 71% of youth athletic program leaders reported that they never received formal concussion training.
Participant Characteristics.
Participant Pre-interview Survey Responses on Concussion Education, Knowledge and Experience.
Interview Themes
Three main interview themes emerged: (1) Youth athletic program leaders and school nurses know their roles in concussion management but welcomed more education; (2) System-level gaps in concussion oversight beyond organized sports; (3) Barriers to concussion care.
Theme 1: Youth Athletic Program Leaders and School Nurses Know Their Roles in Concussion Management but Welcomed More Education
The first theme highlighted that school nurses and youth athletic program leaders were knowledgeable about concussion and recognized their role in concussion care, however they would welcome more tailored education and up-to-date training to support their care for youth in community settings. Both participant groups reported an understanding of concussion signs and symptoms, with many responding with accurate descriptions of concussion symptoms, such as headaches, dizziness, and light sensitivity. In addition, they also recognized their respective roles in concussion care and described acting within the scope of their responsibilities for youth concussion identification. Youth athletic program leaders and school nurses alike noted that they were often the first point of contact for youth sustaining a concussion and were responsible for them while under their supervision. They described their pivotal roles in encouraging youth and their parents to pursue medical concussion evaluations, prompting their expressed need for additional training and education. “If I see something that's going wrong with the kid, if it's any of those symptoms I mentioned earlier, I would just take them out of the game and have the parents take them to a doctor.” Youth Athletic Program Leader A “Well, I can’t diagnose, but I’m the first line of defense… I make a decision to contact a parent to take them for more involved medical attention.” School Nurse B
Both school nurses and youth athletic program leaders were aware that once diagnosed with a concussion, clearance is needed by a trained medical professional prior to the return to youth sports activities. School nurses relied on medical notes for return to activity plans (either return to learn (RTL) or return to play (RTP)) and helped implement those plans in settings where sports personnel are not available. Similarly, youth athletic program leaders recognized their role in re-entry to activity, also relying on medical clearance notes for readiness to return to play, but expressing need for additional training in this area. Youth athletic program leaders did not work through RTP protocols individually with athletes but rather relied on medical personnel or athletic trainers to complete RTP protocols. Youth athletic program leaders also stated that, in conjunction with a medical provider's recommendation for clearance, they used their judgment regarding reintroducing players back into full sport participation. “I usually go off of what the doctor says, and then I see how they are when they’re there…. So, even though you may be cleared from the doctor, you might not be ready to get back. [The doctors] give me my first green light, and then I determine if I think they are actually ready.” Youth Athletic Program Leader C “So, I don’t do that (RTP protocol); the athletic trainer would do that. So one, they’re cleared, then they have that paperwork, and the athletic trainer, based on what sport they’re playing, would go through that process.” School Nurse D
While both groups were found to be knowledgeable, they welcomed additional tailored education and training. Despite school nurses’ familiarity with concussion protocols, they expressed that up-to-date concussion education or training would better equip them to provide the most current concussion management best practices and help support student outcomes in the school setting. Many continuing education modules for school nurses do not contain concussion education, representing a missed opportunity. “…it would be helpful to have an updated review, if there's new protocols, or if we’re not doing something anymore, or if there's new forms, or a new paper to refer to. I’m not adverse to learning something new or changing up what the plan is. I welcome learning about whatever the best way is to take care of the kids so we can get them back to class. I mean, my role as a school nurse is to keep kids healthy, and illness prevention, and health promotion” School Nurse B
In comparison, most of the youth athletic program leaders reported receiving no formal concussion education prior to beginning their roles in urban youth sports settings. Concussion education requirements differed depending on whether a youth athletic program leader was with an organized sport (i.e., high school or club) or a recreational sport (i.e., recreation centers, YMCA). Youth athletic program leaders of organized sports were required to complete concussion education prior to starting their job and some had continuing education requirements. In contrast, youth athletic program leaders from recreational settings often were not required to complete concussion education and thus, sought out concussion education on their own. “So through the national soccer organization there was some formal training—each year there's a requirement that needs to be done in terms of understanding concussions, identifying the symptoms, and then what's the next steps, and return to play…. As well there's a requirement to do some concussion testing through the state organization.” - Youth Athletic Program Leader E “Concussion education- that's not required of a volunteer coach. I was able to participate in that training through our organization, but it is not a full requirement.” Youth Athletic Program Leader F
Several youth athletic program leaders who did not receive concussion education instead based their concussion knowledge and care on personal concussion experience. “I don’t know everything about concussions. I just know what I taught myself from experience. I would probably do a lot better if I had a training or knew a little more about it.’ Youth Athletic Program Leader C
Theme 2: System-Level Gaps in Concussion Oversight Beyond Organized Sports
The second theme highlighted system-level gaps in concussion oversight beyond organized sports, particularly affecting youth injured in recreational settings, free-play environments, and non-school-based activities. Youth who sustain a non-sport-related concussion outside of school or organized sports pose a challenge for school nurses in returning them to normal activities. In addition, youth athletic program leaders in recreational settings did not always have formalized protocols for returning to activity, like their counterparts in organized club sports or schools.
As noted in Theme 1, school nurses were aware of concussion-related care, and the importance of RTP and RTL protocols. However, the school nurses highlighted the difficulty in managing students who are not engaged in school athletics. “In general, we do use return to learn and return to play. We don’t always have the ability to enforce the return to play if they’re not a school athlete. We can of course, stress to the parents that until they’re cleared academically, they should not be participating in extracurricular sports, but it doesn’t always happen.” School Nurse G
In addition, younger children, specifically elementary school-aged, presented different challenges. They are often overlooked in structured return to activity plans. The school nurses noted a lack of guidelines around returning younger children to general free play and recreational activities. School nurses also reported challenges getting the complete injury history from younger-aged children, making concussion identification and management challenging when working with younger age groups. “One of the struggles we have is that the students are ready to come back, and they bring us a note that is a return to play or a return to activity, and we’re kind of in a tough spot with that because we don’t have an athletic trainer. So we have a gym teacher, who is with a class full of 30 or 40 kids. So their ability to monitor the return to play is just not possible…. And I know with athletics in high school and things like that and trainers they’re better equipped to handle that.” School Nurse H “I think also with the younger kids, the biggest challenge is having a difficult time getting the full story. And if it is not witnessed by an adult and the student just can’t even tell me what happened or how bad it was… That makes it difficult….” School Nurse I
Compared to organized sports that have formal concussion protocols, recreational centers may not have protocols or requirements for RTP as they are not governed by state laws for interscholastic sports or NGB policies. Recreational center concussion protocols also may not require communication with health care providers regarding clearance. This affects both injuries that occur as part of recreational activities and those who may have sustained a concussion in another setting but are spending time with youth athletic program leaders in a recreational center (e.g., summer camp). As a result, due to insufficient guidelines, decision-making around RTP in these settings is frequently informal, and may rely on subjective assessments, child self-report of symptoms, or parental choice on whether their child can participate in activities. “I’d say, ‘Did your mommy say you could come play?’ Pretty much that's it.” Youth Athletic Program Leader J
Theme 3: Barriers to Concussion Care
Theme three highlighted challenges in concussion care within urban community settings, including lack of youth concussion awareness among families, parental engagement, language barriers, and access to health care (i.e., insurance type, transportation). Both youth athletic program leaders and school nurses perceived lack of access to care as a major barrier for diagnosis, recovery, and re-entry into school or sport. For example, they reported challenges around language barriers, insurance, and transportation limitations (lack of resources or cost of transportation). “We have a lot of non-English speaking kids in our schools. And that continues to be a little bit challenging because it is a variety of languages…. Usually, if the child doesn’t [speak English], mom and dad don’t either. But that's another challenge as well, because you’re trying to relay that the child should be seen. I am not always 100 percent sure that they’re understanding that that's what I am saying.” School Nurse H “There's a lot of students in the population that I care for that don’t have insurance. Some of them don’t wanna go to the doctor because they have to pay a large copay…. There's a lot of lack of resources where I am.” School Nurse K
An additional parental barrier reported by youth athletic program leaders was parents either minimizing concussion due to a lack of concussion awareness or not being forthcoming about their child accessing appropriate health care evaluations for concussion clearance, despite youth athletic program leaders’ and school nurses’ encouragement. School nurses also noted barriers with children not self-identifying that they had an injury. “Busy families that think ‘oh, it's not a big deal. Kids bump their heads all the time.’ I think that would be the biggest challenge, is just not taking that seriously.” School Nurse I “Barriers to concussion identification would be, number one, the student not self-identifying, not coming to an adult, sharing what's happening with them or that they fell…or got hit. Number two barrier would be parents not following up with students’ symptoms.” School Nurse K
Discussion
School nurses and youth athletic program leaders play a pivotal role at the front-line for concussion identification and prevention and reintegration of injured children into daily activities. This is particularly true for children in less resourced environments, where participation in organized sports is less than in other more resourced settings and there is more reliance on community-based recreational centers for after-school or summer childcare. Through thematic analysis of qualitative interviews with urban school nurses and youth athletic program leaders, important themes emerged.
Although most of the youth athletic program leaders and school nurses had adequate knowledge of concussion care, they saw benefit from receiving updated education and welcomed opportunities for it. In our sample, one quarter of school nurses and three quarters of youth athletic program leaders had no formal concussion training. This desire for updated education is amplified by the fact that concussion guidelines evolve rapidly as research expands. Approximately every four years, the International Concussion in Sport Group (CISG) meets to discuss current concussion research and guidelines. The most recent consensus statement in 2023 outlines current best practices and tools for concussion identification and provides management recommendations. As an example, previously, complete physical and cognitive rest was the recommendation for concussion recovery (Willer & Leddy, 2006). However, current evidence indicates that relative rest 24–48 h after injury can be followed by increasing light aerobic activity that does not severely worsen concussion symptoms, such as walking, safe and controlled stationary bike cycling or daily activities that do not significantly worsen concussion symptoms, beginning at 24–48 h after injury (Patricios et al., 2023). Youth athletic program leaders and school nurses would be better equipped to support the youth in their care if armed with these latest recommendations. Continuing education for these professions does not always include updates to concussion knowledge, so identifying a mechanism to deliver these educational updates, perhaps through a concussion certification program, is important.
This study also illustrates the gap in concussion education and policies between organized and recreational sports. Organized sports (i.e., club sports or interscholastic teams) integrate mandated concussion education, best concussion practices, and structured RTP guidelines, in contrast to non-organized sports or recreation organizations (i.e., recreational centers) that often do not have such requirements. Education for coaches has been shown to increase concussion knowledge and attitudes (Daugherty et al., 2019). In our sample, most of the youth athletic program leaders from recreational organizations did not receive any concussion education, while those from organized sports (i.e., club or school) had completed some structured education required as part of their role. This is likely tied to state laws and policies that govern sports. In 2011, Pennsylvania passed the Safety in Youth Sports Act (101 of 2011) requiring schools to develop RTP policies for student athletes with concussions, coaches to undergo yearly concussion education, and students and parents to review a concussion information sheet. However, this law only lays out penalties and guidelines for high school level athletics (Safety In Youth Sports Act—Enactment, 2011). Recreational sports, as well as sports involving younger age groups, are not addressed by this law (McGowan Lowrey, 2018). In addition, concussion consensus statements outlining identification and management guidelines, from which policies are often derived, are predominantly tailored towards athletes, specifically high school-aged, and their return to graded activity and sport. These findings highlight an important blind spot with regard to development and dissemination of policies and procedures governing concussions sustained outside of organized sport.
From a nursing perspective, similar themes emerged. For a student who is not returning to an organized sport and therefore does not benefit from guidelines and structured monitoring, school nurses reported this responsibility falling on them and needing to rely on health care professional notes to implement and manage the return to learn and activity plans. This can prove challenging for school nurses in their integral role as care coordinators in the context of the continuing education limitations described above and when, in a limited resourced setting, the scope of practice of a school nurse is wide and requires coverage of a larger number of children than in a more resourced school system. School nurses also reported a lack of policies and guidelines in place for the management of younger children with concussion. Since concussions in the 5–12 year-old age range are sustained predominantly through recreational or non-sport related injuries, school nurses need to have guidance that supports recovery through age specific school reintegration protocols (Roby et al., 2024). As existing concussion guidelines often do not apply to younger children and their specific age-related needs, they pose a risk of being overlooked in structured return to activity plans. Lastly, when concussions are sustained outside the school or sport setting, there is the potential for fragmented communication between the family and the school setting resulting in inadequate coordination among all relevant stakeholders (e.g., classroom teacher, physical education instructor, school nurse, guidance counselor). Empowering school nurses, with both education and resources, to assert their role as the hub of communication to oversee and coordinate concussion management represents an opportunity to integrate concussion care with the holistic care of the child in the educational setting.
School nurses and youth athletic program leaders also identified several barriers to concussion care for the youth they serve, including language barriers, access to transportation, and insurance type. These disparities have been previously found in concussion care in specialty clinics and emergency department settings (Mohammed et al., 2023; Pate et al., 2022). Importantly, such barriers can significantly hinder the recovery process for youth diagnosed with a concussion, as timely and consistent follow-up care is essential for symptom resolution and return to activities of daily living. These barriers are not unique to concussion care and are observed in mental and behavioral health, oral health, and in health care in general (Dickman et al., 2017; Hoffmann et al., 2022; Mahmood et al., 2024; Serban et al., 2024; Tumin et al., 2019). Broadly in pediatric health care, there has been exploration of innovative ways to facilitate access, including telemedicine or school-based health clinics. These strategies can likely encompass concussion care and may represent opportunities to overcome some of these barriers identified in the interviews.
Limitations
As with any structured interview study, broad generalizability can be challenging. School nurses and youth athletic program leaders were enrolled from the general Philadelphia and surrounding areas. Additional research in rural areas or areas without access to a concussion specialty care center is needed to better understand concussion knowledge and needs in those areas. The school nurse sample was exclusively white, non-Hispanic, and female, which may have limited the range of perspectives related to lived experience, educational pathways, and professional experiences; a more diverse sample may reveal additional themes.
Conclusion
Through in-depth interviews, this study examined the concussion knowledge, education, and organizational policies of school nurses and youth athletic program leaders from urban areas to identify gaps and barriers in the prevention, identification, and management of concussions among children. Despite their pivotal role in interfacing with injured youth, continuing education on concussions is lacking for these professions. Existing concussion policies and procedures leave gaps in the care of younger children, and those who sustain their injuries via non-sports mechanisms, and in recreational settings—creating an environment for disparities in concussion outcomes. These findings can drive targeted concussion education and policy development, specifically in elementary schools, recreational centers, and community-based after school programs, to help address disparities for youth concussion in urban community settings.
Compliance with Ethical Standards
The study protocol was reviewed by the Children's Hospital of Philadelphia and classified as exempt (minimal-risk) research (Approval No. 23-020900). Participants provided informed consent electronically prior to beginning the survey and interview.
Footnotes
ORCID iDs
Author Contribution(s)
Funding
Funding for this research has been provided by Centers for Disease Control and Prevention Grant U01CE003479 (Arbogast/Master) and National Institute of Neurological Disorders and Stroke of the National Institutes of Health award number K23NS128275 (Corwin).
National Institute of Neurological Disorders and Stroke, National Center for Injury Prevention and Control, (grant number K23NS128275, U01CE003479).
Disclaimer
The findings and conclusions in this manuscript are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention nor the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.