
Abstract
Patients arriving in the Accident and Emergency Department tend to be moved about throughout the care journey. Although each trolley bed had a tray table attached at the end of the bed for clinical use, its space was limited and additional equipment might be left on the bedside cabinets. Hence these items were easily left behind when patients shifted to another care area. The tray table attachments on the trolley beds became the focus of a redesign effort to improve storage capability in this mobile, dynamic environment. Through the combined use of human factors and design thinking methods, a successful proof of concept was realized.
Keywords
The human factors team employed design thinking and collaboration with hospital staff to enable easy access to the multiple items needed for bedside care.
Consider the following scenario. The Accident and Emergency Room (A&E) received a patient, Mr. Derrick, who survived an unfortunate traffic accident but suffered severe traumatic injuries with substantial hemorrhaging. As the paramedics rolled Mr. Derrick in from the ambulance bay, he was transferred onto a trolley bed within the resuscitation area, and the assigned emergency resuscitation team began working against the clock.
A portable vital signs monitor (which also functioned as a defibrillator if needed) was connected to Mr. Derrick and placed on top of the trolley bed’s cardiac tray table (Figure 1) at the foot of the bed. As the rest of the team focused on stabilizing Mr. Derrick, one of the doctors urgently requested a pint of blood by filling out the necessary paperwork. The blood product arrived in a cooler box and was placed on the bedside cabinet next to the patient’s trolley bed, ready to be used.

In the busy A&E room, the tray table attachment was used extensively, and patients would be shifted to different areas throughout their treatment process.
As the A&E got busier that morning, Mr. Derrick was rolled into the observation area in another section of the A&E for further monitoring and care. The resuscitation team handed Mr. Derrick off to be looked after by the care team in the observation area. As the new care team’s doctor reviewed the proposed care plan, he queried if Mr. Derrick had received his blood transfusion and, given the urgency of the situation, ordered two more pints of blood to be collected in person by one of the nurses. Mr. Derrick received his blood transfusion and was recovering smoothly.
It was only many hours later, when another staff member asked out loud whom the pint of blood resting on a bedside table was for, that the care team realized the existence of the initial two bags of blood for the first time. Because the blood product had been out of its cooled state for far too long, it was ruined and thus discarded.
Human Factors and Design Thinking at the Front Lines
This was one of the stories presented by Changi General Hospital Singapore’s A&E Clinical Service Quality Committee to us, the in-house human factors team. Although it may be easy to identify some of the issues at play here (e.g., lack of communication when critical items arrived, making the blood products more visually salient), we also noted the chaotic nature of the environment and the lack of a system to store and keep track of a patient’s items.
Unlike in a ward setting, patients in the A&E were wheeled from point to point along their care journey before getting discharged or transferred to a bed in one of the wards. The resulting movement of the patient posed a risk that items would be left behind. Thus, a project was initiated to focus on developing a means to accommodate all the essential tasks and items required to care for an A&E patient. Efforts were not directed at other aspects of the problem (e.g., lack of communication).
For the in-house human factors team, this was an opportunity for us to explore using design thinking methodologies, in conjunction with the usability analysis and ergonomic design considerations typically associated with human factors. Like human factors, design thinking emphasizes user-centric approaches to understand the problem. Based on an ethnographic approach toward users, design thinking provides a systematic way of generating creative and novel solutions focused on users’ needs, pivoting on solving issues at their root cause rather than providing only product solutions that users might not require (Brown, 2008; Fraser, 2006; Kelley & Kelley, 2013).
We formed a small team with design thinking collaborators from the National University of Singapore’s Engineering Design and Innovation Centre (EDIC). The project lasted about a year and involved a series of planned observations, interviews, and surveys before we finally prototyped a viable solution. This article details the approach our team took and reports on the project findings as well as the eventual design prototype that came out of our efforts.
Understanding the Context of the Problem
After an introduction of methods from both human factors and design thinking, we decided on a series of ethnographic observations within the A&E to understand the context of the problem. To avoid jumping to conclusions and focusing blindly on one aspect of the situation (e.g., handing over of information and items), we planned on observing the A&E in its entirety, paying attention to environmental, procedural, and equipment issues that may have contributed to the mismanagement and misplacement of care-related items. This observation also gave the team an opportunity to become familiar with the A&E operations.
Our team was split into two pairs. Each collaborator from EDIC was paired with a hospital representative from the team so as to facilitate access within the A&E. Each pair was scheduled to observe various 2-hr periods in the A&E, after which the pair would quickly return to the office to download and document all the details while the memory was still fresh (Figure 2). The observation periods were generally in the morning, when the A&E was known to be the busiest. We had decided on 2 hr because we anticipated that any longer would have resulted in information overload on the observers. A total of 10 2-hr observations were conducted over a period of 1 month.
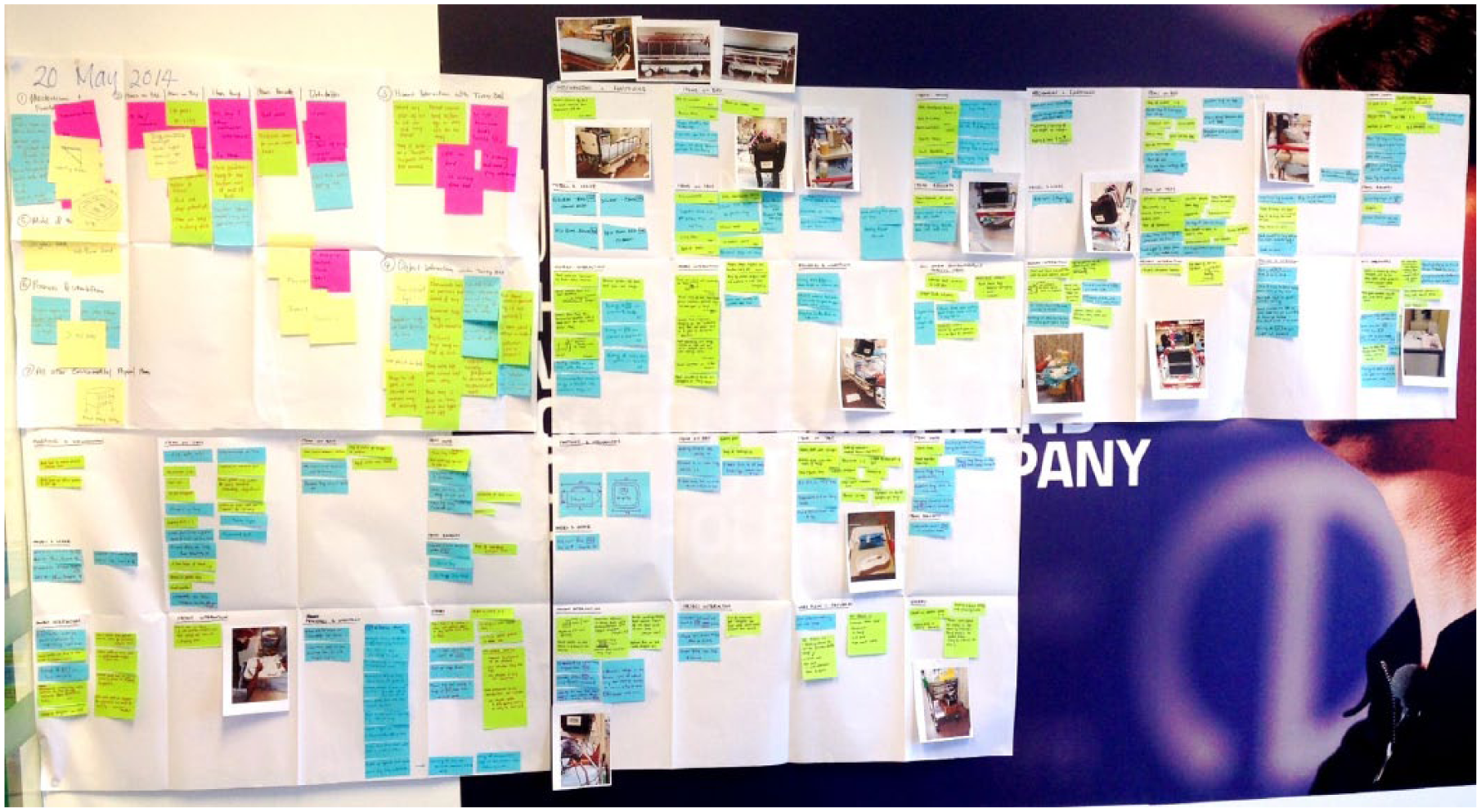
Captured in sticky notes and photos, the observation details are subsequently categorized on a shared wall within the team.
Notable observations include the following:
No incidence of items being misplaced was noted during the observation period.
Despite the dynamic A&E environment, staff were able to adapt to the change in space or availability of equipment to complete the tasks at hand. For example, when there was a lack of space for documentation, the staff used the vitals monitor device as a solid writing surface. In another example, case notes were wedged in the visible space between the push handles and mattress.
Two brands of trolley beds were being used in the A&E, each with its own tray table attachment design. Additionally, within each brand, multiple models of tray tables were available with different working heights. They fundamentally served the same purpose.
Often, because of space constraints, a patient’s personal items were placed on the mattress at the foot of the bed or wedged under the mattress. At times, additional care items, such as old case records, were also placed at the foot of the bed.
Because of the need for mobility in a cramped environment, the trolley beds were designed to be narrow, and the sides were kept clean of loose or hanging items. Various monitoring devices had been known to get knocked over when hung along the outside edge of the trolley bed.
The vast amount of space under the trolley remained largely unused because of reachability and visibility limitations. It was mainly used to store bulky patient belongings or thick case records. Should the patient change beds, items under the bed might be forgotten.
For its prime location, the tray tables accommodated numerous other items, aside from the monitoring devices that they were primarily designed to hold.
As the series of observations continued, we felt the need to look deeper at how the detachable tray tables at the end of each trolley bed were utilized. Most trolley beds were fitted with flat plastic tabletops, which feature vertical stands that attach onto the foot of the trolley beds. Besides those bedside activities directly dealing with the patient, it appeared that many actions also involved the use of these tray tables. For example, caregivers used that space to hold items required for a procedure or to provide a firm surface for note taking. During our observations, we noted the following:
The tray table mostly held items, including current and past records, requested medication, care equipment, and, more often, the vital signs monitor, which occupied the entire tray table when being used.
From time to time, the tray table would be used to temporarily hold procedural equipment (e.g., phlebotomist’s kit, when a blood draw from a patient is required).
Patients were also observed to use the tray tables to consume their food while sitting at the foot of the bed.
Tray tables may be high, so some nurses had difficulty lifting the heavy vital signs monitor (Figure 3). At times they had to reach near the height of their shoulders, which is known to be fairly effortful (Mital, 1984; Sanders & McCormick, 1993).
Temporary safety straps were used to secure the vital signs monitor onto the tray table, preventing it from dropping, especially during transit.
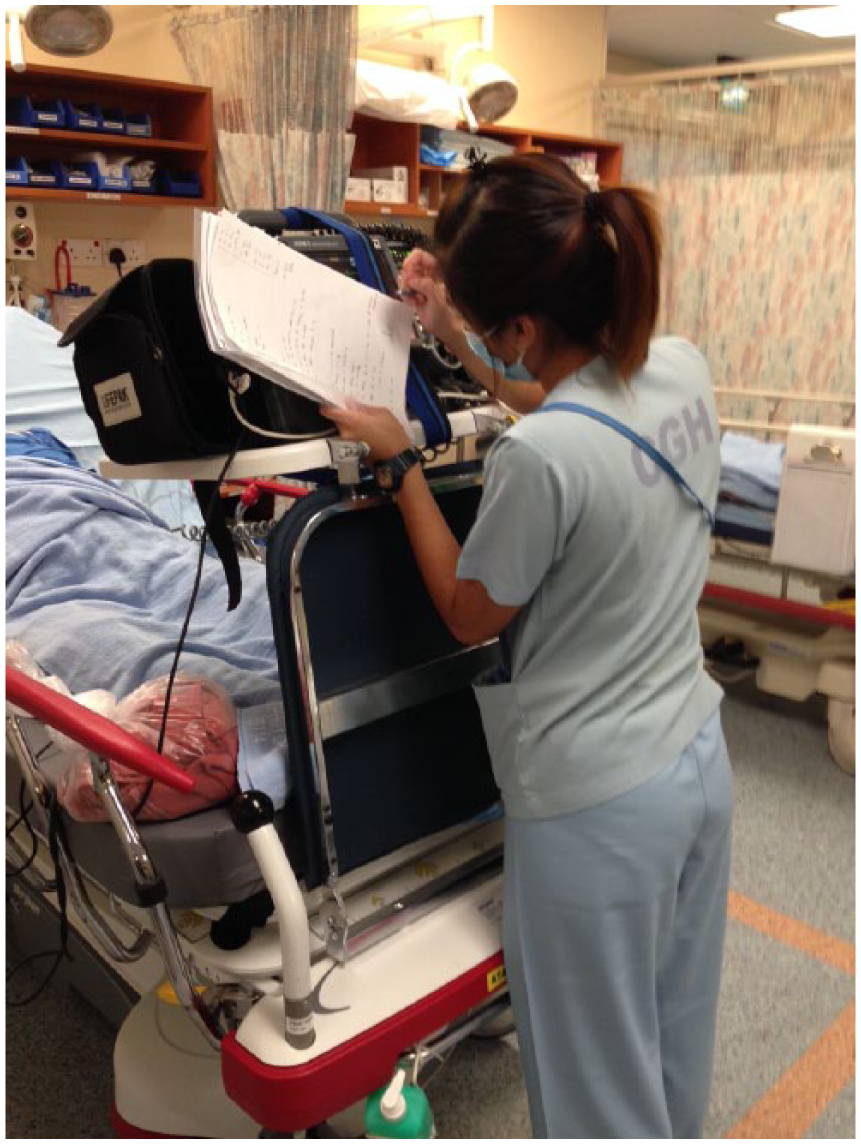
Nurse using the vital signs monitor as a solid surface for note taking. Height of monitor was at shoulder level, occasionally requiring extra strength to lift the heavy equipment.
A common design thinking strategy for identifying gaps and opportunities is to come up with “how might we” questions. In reviewing our data and experiences, we noted three key opportunities:
How might we limit the number of items placed on the trolley/environment?
How might we increase the visibility of items placed on the trolley/environment?
How might we organize items placed on the trolley/environment?
Amid the various possible solutions the team discussed, we decided to focus on the trolley-bed tray table attachment as a possible target for developing a more organized storage device. Given the many A&E activities that centered on the tray table, improving the tray table should significantly contribute to improving the A&E’s care operations.
Identifying Frequently Used Items During Patient Care
To begin our efforts on redesigning the tray table, we first had to understand all the various items with which our A&E staff had to interact while caring for a patient, which meant identifying frequently used items and where they are usually located. Because it is impractical to accommodate everything, an effective tray table design should therefore accommodate high-priority items and facilitate their use during routine care for patients.
Below is a list of all the items that have been identified as those commonly used in the A&E setting, based on the findings from our observations. From this list we created a paper-based survey, which was used to poll A&E staff regarding each item’s frequency of use as well as its importance in the care of the patient.
A&E cordless phone
Blood bag
Blood sample bottles
Hand sanitizer
Hypocount meter
Infusion pump
Intravenous (IV) kit tray
Kidney dish
Patient’s belongings
Patient’s document
Team sign tag
Torchlight
Ventilator
Vital signs monitor
White clipboard
The survey form used pictures and checkboxes for quick and easy responses, and its paper form allowed for convenient polling of staff whenever they had a few minutes to spare. This approach was critical given the fast-paced work environment in the A&E as well as the limited and precious shift rest periods. We surveyed 38 nurses, 10 doctors, and 2 transporters.
Survey participants were asked to identify items that were used in “every case,” “almost every case,” “occasionally,” or “rarely.” The top five items used in every case were the in-house cordless phone, hand sanitizer, IV kit, team sign tag (indicating to which resuscitation team the patient belonged), and the white clipboard where key care information was documented (see also Figure 4). The top five items used in almost every case were the vital signs monitor, oxygen tank, infusion pump, hypocount meter, and blood sample bottles.

Items that were generally found on the tray table more than 50% of the time.
Items that were placed on the tray table more than 50% of the time were the vital signs monitor, kidney dish, IV kit, hypocount meter, blood sample bottles, torchlight, in-house cordless phone, and patient’s documents.
Results from the survey helped us identify the items we needed to consider when redesigning the tray table attachments, namely,
Vital signs monitor
Hypocount meter
IV kit tray
Cordless phone
Blood sample bottles
Patient’s case notes
Clipboard
Team tag
Hand sanitizer
Redesigning and Prototyping an A&E Trolley-Bed Tray Table
With the information at hand, we began brainstorming about what the improved tray table should look like (Figure 5). Some key features that were different from the previous tray-table design were as follows:
Expandable tabletop that allowed for additional 50% of working space
A trough within the table to accommodate smaller objects that tend to roll around
Hooks under the tray table for hanging equipment or other loose items. The hooks also made it easier for nurses to hang the heavy vital signs monitor, instead of placing it at the relatively higher tabletop.
A recessed framework to reduce protrusion of large equipment hanging off the frame
A translucent document pocket to hold frequently accessed notes and paperwork
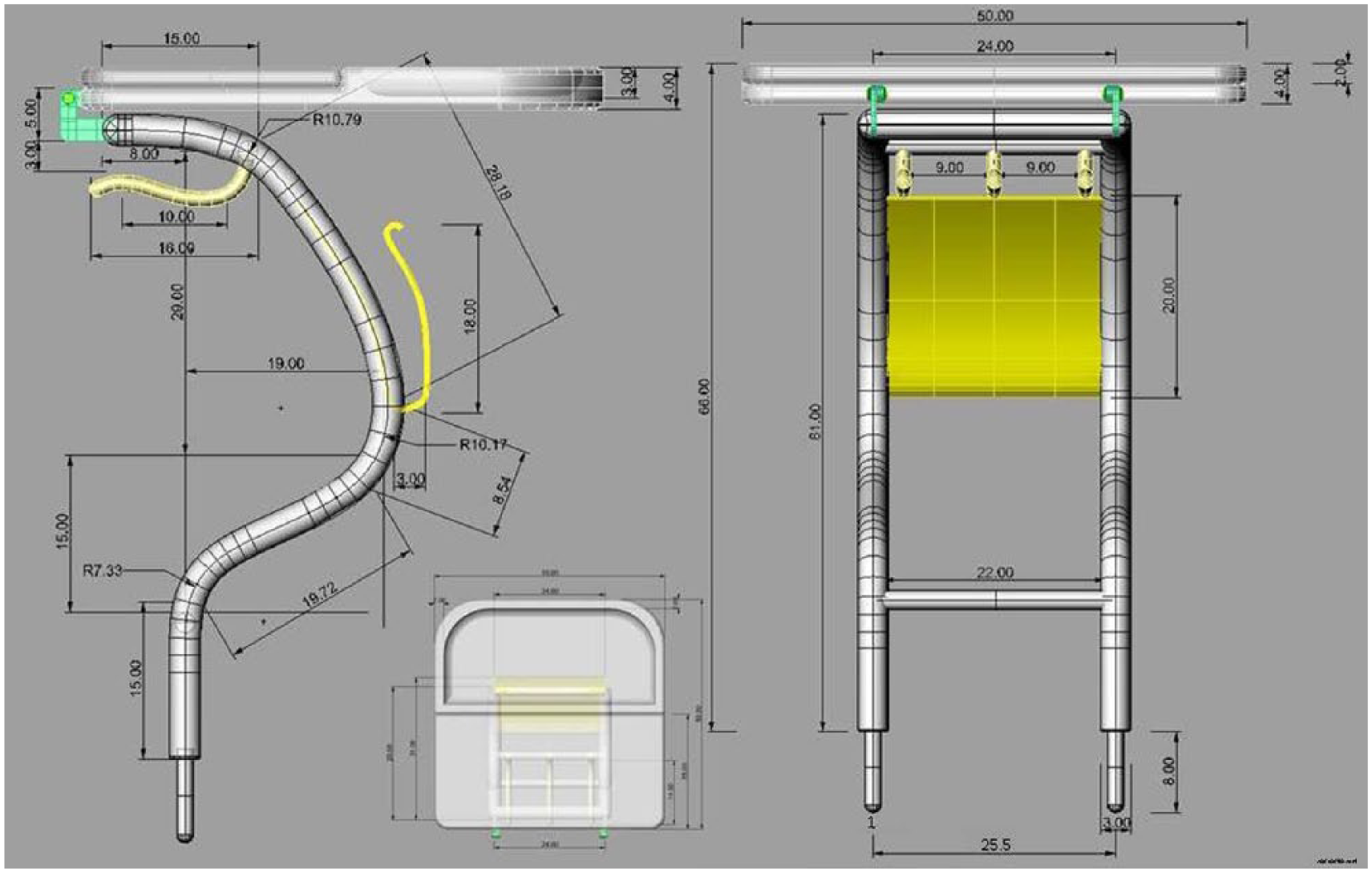
Design drawings of the prototype tray table.
A small, 1:10-scale prototype (Figure 6) was first built to help conceptualize our design further. It aided us in testing new ideas and allowed for easy modifications and adjustments. The small prototype was also easy to transport and present to various stakeholders to solicit comments and suggestions. After gathering all the inputs, we finalized the design and advanced it toward developing a full-scale prototype for the next level of functional trials.
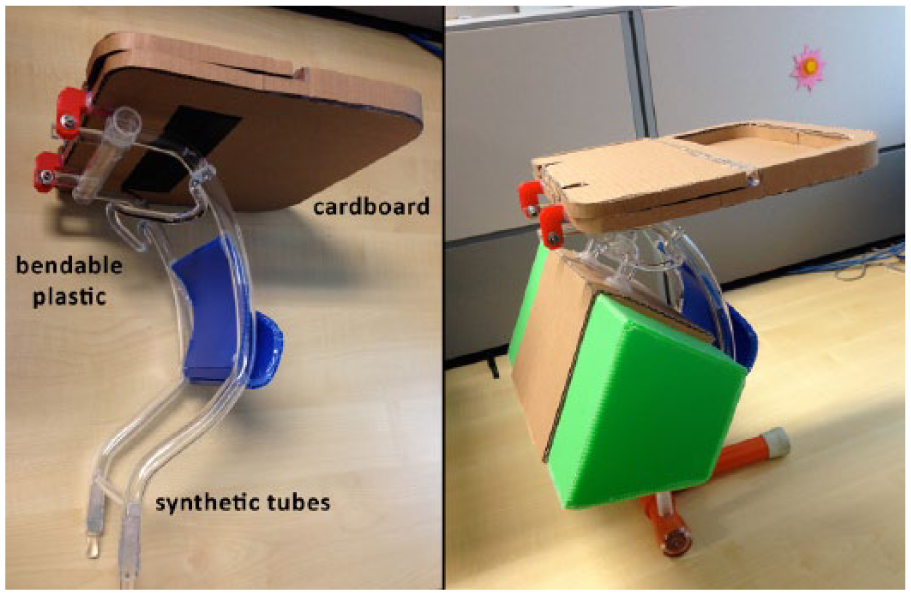
A rudimentary 1:10-scale prototype, made using cardboard, plastic, and synthetic tubes.
The full-scale prototype (Figure 7) was fabricated at the university’s laboratories using easily accessible materials, such as wood, aluminum, and carbon fiber. As such, materials used on the prototype were not representative of what the final product should consist of. Typically, the tabletop would be composed of molded plastic, but a section of the tabletop design was easier for us to shape by manipulating wood directly and thus resulted in a heavier tray table.

A full-scale prototype of the tray table was fabricated to facilitate functional trials.
We were satisfied with a prototype that enabled us to perform full-scale simulations. Nonetheless, there were too many risks to try to fabricate an operational prototype for the A&E, and for that reason, formal work flow and task analyses could not be conducted to fully understand all the benefits and unintended consequences of the redesigned tray table attachment.
The full-scale prototype was fitted onto a trolley bed in the A&E, and various simulations were conducted based on common scenarios and actual equipment (Figure 8). Volunteer staff who participated in the simulations provided positive comments and were quick to point out the advantages of the new design over the existing setup. For example, the vital signs monitor hanging under the tray table meant that the tabletop was kept clear and could be used for documentation or to hold other essential items.

The full-scale prototype being used in simulations, where additional equipment can now be hung under the tray and on the expandable tabletop.
When fully loaded, the redesigned tray table attachment could accommodate at least five more frequently used items, including bulky equipment such as the vital signs monitor, cooler box, and phlebotomy kit. It should therefore significantly improve staff’s workflow efficiency and ability to deliver care.
A notable limitation with the redesign was how the curved frame extended 20 cm over the mattress, reducing the space patients would have when lying down. The curved frame reduced the protrusion of bulky items hanging out into the busy walkway. Although we do not think this design would adversely affect most of our patients, who are generally Asian and of smaller build, the occasional taller patients would find the already small trolley bed even more cramped. This design limitation should be addressed in future iterations.
Successful Collaboration and Lessons Learned
From our simulations with the full-scale prototype, we concluded that we had a viable proof of concept. However, the team could go no further because we lacked the capabilities to feasibly manufacture and operationalize our design. We share our efforts here in hopes of fueling the interest of medical equipment companies to consider looking at enhancing the designs of tray table attachments. It is through their expertise in development and production that we could one day see and use such innovations in our health care system. We would be happy to work with interested parties willing to take this idea to the next level.
Nothwithstanding these limitations, our yearlong project was an example of a successful collaboration between professionals working in human factors and design thinking, as well as between academic and health care institutes, in exploring innovation at the front lines. As with most user-centric approaches, we see a common language within human factors and design thinking, which made it easier to collaborate creatively, solve problems, and generate solutions (Lindberg, Noweski, & Meinel, 2010). Partnering with academic practitioners also increased our hospital’s research and development capabilities and provided us with opportunities to access prototyping and fabrication tools (e.g., 3-D printers, laser cutters) otherwise not available in our hospital.
Footnotes
We thank Patricia Loh for her involvement in this project as well as members of Changi General Hospital’s Accident and Emergency Clinical and Service Quality Committee and the various A&E staff who provided us with valuable support, input, and feedback.