
Abstract
Emergency response to a pandemic requires health care systems to initiate many activities. One of these activities is providing the public with information and guidance about the symptoms and the actions that need to be taken. A dedicated call center should facilitate the public need. Such a call center needs to be carefully designed to protect the call takers from potentially being infected by other staff members. An ad hoc facility has the flexibility to adjust to evolving demands and constraints. This article presents the need, the concerns, and the guidelines used to design such call center during the COVID-19 pandemic outbreak.
Keywords
Emergency response to a pandemic requires healthcare systems to initiate many activities, including a dedicated call center. This paper presents the need, concerns and guidelines used to design a call center during the COVID-19 pandemic.
The Situation
In March 2020, the World Health Organization declared the rapidly spreading coronavirus (COVID-19) outbreak a pandemic (World Health Organization, 2020), acknowledging that the virus would likely spread to all countries on the globe. Being a respiratory virus, it is transmitted through respiratory droplets (Bourouiba, 2020), and it appears that people can spread the virus even if they do not have symptoms. The State of Israel had begun attempts to tackle the virus several weeks earlier, as overseas visitors had already infected people throughout the country.
The Need for Reliable Clinical Consulting
A key component of responding to an emergency involves providing information to the public in a timely manner. Health authorities need to give the public reliable answers to clinical concerns they might have (Fallon et al., 2011). Professional answers to these questions instruct callers about what to do if they have valid symptoms and reassure those with nonvalid symptoms. As the need arises, additional emergency health care services can quickly be set up in places such as abandoned buildings and in temporary tents to fill sudden high demand.
In Israel, in order to provide a nationwide response system, the Israeli Ministry of Health asked the national emergency medical services (EMS; Magen-David-Adom) to extend its call center reach and provide basic phone diagnosis and triage through its well-known emergency dial-in phone number and proven emergency call centers. Within 5 hours, the call center responded to the requirement and started to provide the new service, without interfering with the level of service required for the general emergency calls that the call center receives from the public. On a normal day, these call centers respond to about 6,000 emergency calls, but the expectation was that the number of calls would jump dramatically with calls from people who were concerned about symptoms they had. The need for additional capacity within a few days led to an ad hoc solution that was flexible enough to evolve as the demand for information and the guidelines for protecting the teams developed. Feedback and ideas from the working teams also assisted in shaping the processes and the work environment. Extending the current service with an ad hoc solution facilitated a short planning process, a characteristic that was important due to the ongoing changes in requirements and constraints. Protecting the safety of the scores of additional call takers recruited to handle these calls required careful call center design.
The Design Process
At the first phase of the crisis, the Ministry of Health instructed people who developed symptoms of the disease to call the emergency phone number. The goal was to identify people with valid symptoms and get them tested for the virus at home or at dedicated facilities, reducing the chances that they would infect others if they had to travel to a medical center.
To handle the calls, a short protocol was developed. It led the call taker through several questions to help them understand both what type of symptoms the caller currently had, as well as to estimate what the chances were that the caller was infected by the virus, depending on whom they had met and the places they had visited. This protocol was evolved as more information about the disease and the methods to handle it were collected. Callers with relevant symptoms were added to a list of people to be tested for the virus, while all other callers were informed that they were not at risk and that they could continue with their normal routines. All the calls were documented using dedicated software that was available to all call takers and was connected to the EMS command and control information system.
Design Guidelines for the Call Center
Little was known about the pandemic progression at the beginning of this crisis. The requirements evolved with the realization of the risks and infection vector. The leading factor for the ad hoc facility was the increasing need for call takers, and the design of the facility developed to provide the needed seats under the constraint of limiting the chances for infection. Thus, the design was not a response to a clear list of requirements, but an evolving process that changed its shape almost on a daily basis as a response to new information regarding the volume of calls and the measures that needed to be implemented in order to protect the call takers. A short list of the design guidelines can be found in the sidebar.
A list of the design guidelines
Identify the disease infection vector.
Find measures that can protect the workforce from this danger.
Design a work environment that implements these measurements.
Collect feedback from the workforce on their feelings about the work environment.
Make necessary changes to accommodate the workforce concerns.
The call center design had three components (Bitan, 2020).
The Work Environment
As it became clear that the coronavirus was spreading through people who were infected before they showed symptoms, the main challenge was how to arrange the work environment in a way that would reduce the chances of infection and minimize the number of others who would be affected in case one of the call takers was diagnosed with the disease. The infection of even one call taker could require many other call takers to be quarantined and the cessation of the entire call center until it was disinfected and the staff replaced. In the first few hours, the service was provided through the standard call center, but as the demand developed, it was extended to an ad hoc facility. The focus was on designing a work environment that could host tens of call takers in 24/7 work shifts and reduce the chances for spreading the virus.
To quickly host the call takers, a dedicated tent was built in the parking lot of the EMS national command and control center (see Figure 1). The tent was equipped with a dedicated air-conditioning system that could circulate the air in the tent. Special attention was given to design an optimal seating plan inside, prioritizing distance over efficiency. In this case, the goal was to maximize the number of call takers while maintaining a safe distance between them.

A dedicated tent was built in the parking lot.
In order to reduce the number of workers who might be infected, the new call center was divided into six work sections to limit the number of people working in each space. The main sections were separated with simple plastic curtains that marked the section’s boundary. The call takers were seated at a safe distance of 2 m from each other, and their desks were set in rows, one behind the other, to make sure that they were not sitting face to face, again to keep a safe distance from each other. The 2-m distance was also kept between the seats, with an empty seat that maintained the distance between every two call takers (see Figure 2). In addition, each workstation was protected by a cardboard divider on three sides (see Figure 3). Keeping this safe distance allowed call takers to work without face masks, an artifact that would make phone communication hard to understand. A receptionist located at the front desk at the entrance to the tent registered the call takers and provided them with a color-coded tag that marked the area they were assigned to.
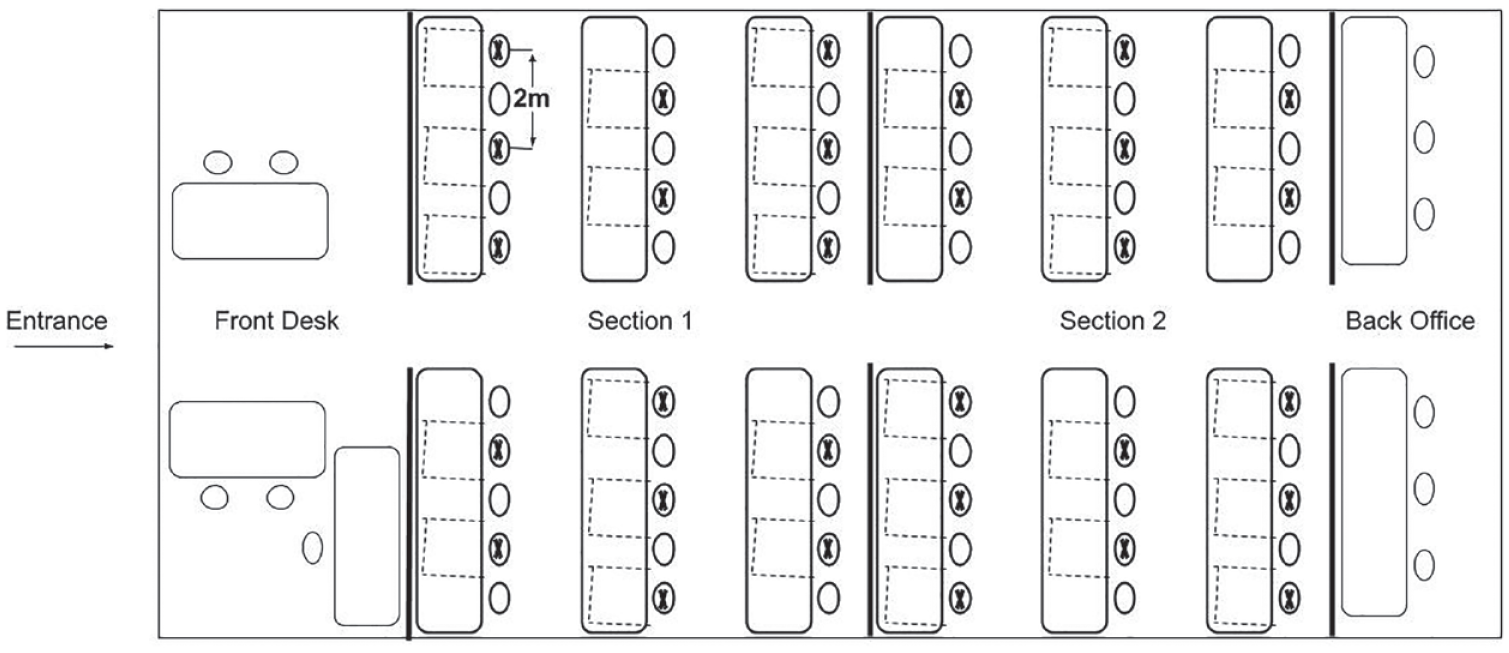
Floor diagram. The Xs indicate occupied seats, thick lines indicate plastic curtains between sections, and dashed lines indicate cardboard divider for each workstation.

A workstation protected by a cardboard divider on three sides.
The Equipment
The dedicated tent had 60 standard workstations, each equipped with a phone connected to a phone switch and a laptop computer. The number of active workstations was later reduced to 30 as new regulation that limits the number of people that can work in the same space was published. Dedicated web application software that was installed on all workstations was used by call takers to document the communication. The application was developed specifically to handle the COVID-19 outbreak calls, but it was using the existing infrastructure and user interface to reduce the chances for software glitches and the need for extensive training. An interface to the EMS command and control system transferred the details of callers needing to be escalated and tested. In addition, each workstation was equipped with a printed card of the call protocol that described the call procedure, and the main contacts for calls that needed to be escalated. Following the Ministry of Health instructions, at the beginning of the shift, the call taker cleaned the workstation using disinfectant, which was positioned on each desk.
The Human Operators
The call takers’ positions were staffed with volunteers who usually act as emergency medical technicians in the EMS ambulances. They received three hours of training for how to answer the calls, triage the callers, and operate the information system. A video-based training tool was used to train call takers to operate the software. As emergency medical technicians with basic medical knowledge, specific training for the task had to focus only on the reported symptoms, and the procedure to handle the different cases.
Call takers worked in 12-hour shifts. To reduce the chances of call takers gathering during breaks, only one person from each work section could take a break at any given time. As the guidelines for physical distancing evolved, the call takers were divided into three teams that had strict instructions not to mix – only call takers from the team were assigned to work on a shift.
How it Actually Operated
All phone calls received by the EMS dispatch center were first screened between the emergency command center (that continued to operate under normal conditions) and the new coronavirus call center. The number of calls in the first few days jumped to 20,000, and as the pandemic spread throughout the country, the number jumped to 80,000 calls per day. The call centers were staffed with 700 volunteers who worked in three shifts, 24 hours a day. It was operated for 2 months and was replaced by a new temporary facility that is bigger and implements many of the insights gained from the first tent, including better air-filtering, and more distance between workstations. No one was infected by COVID-19 while working in the call center.
Conclusions
The response to an event that evolves as a crisis unfolds must rely on flexibility and ad hoc solutions. The organization need to keep adapting and changing its settings and procedures based on new information about the crisis. Quick response to a pandemic can save lives, but these measures should also protect the caregivers. Responsible designs that take into consideration the evolving characteristics of a disease provide a safer work environment for call takers, ensuring that they will be able to operate even when a pandemic continues to spread throughout a community. A short list of action items for an evolving crisis can be found in the sidebar.
A list of action items for an evolving crisis
Update the response measures.
Define the service that needs to be provided.
Identify dynamic bottleneck changes.
Implement ad hoc solutions that can be quickly modified.
Keep changing and adapting as new information arises.
Footnotes
![]()