
Abstract
A paradigm shift is underway in the training of professional counselors. It involves a shift in orientation from an input-based or traditional model of training to an outcomes-based or competency-based model of training. This article provides a detailed description of both input-based and outcomes-based training and instructional methods. It illustrates these differences in how counselor trainees are taught to work with clients with health and mental health issues.
Keywords
A paradigm shift is occurring in the training of health and mental health professionals today. It involves a shift in orientation from an input-based to an output-based or outcomes-based instruction. Typically, counselor training programs that employ input-based or traditional instructional methods focus on mastery of knowledge through lectures, directed reading, discussion, and minimum client contact. Here, learning is typically evaluated by examinations, term papers, and other written assignments (Miller, 2010). This contrasts with outcomes-based instruction with its focus on mastery of competencies through simulated counseling activities, coaching, client feedback, and reflection. Here, learning is more likely to be evaluated with demonstration of learned skills, rubrics, portfolios, and other forms of objective-structured assessments. Furthermore, whereas input-based instruction is guided by core curriculum standards, outcomes-based instruction is guided by core competency standards (Sperry, 2010).
In the current era of accountability in health and mental health care, outcomes-based and competency-based learning is quickly becoming the norm for training competent professionals. This is not to imply that the input-based learning is no longer considered important and useful, but rather that it will assume a more limited role in the education and training of professional counselors. Certain required courses in graduate counseling programs such as Legal and Ethical Issues in Counseling, Life Span Development, and Research Methods will likely to continue to be taught with largely input-based instructional methods. In contrast, clinically oriented courses, particularly prepracticum, practicum, and internship courses will be largely outcomes-based and competency-based training experiences.
This article provides a detailed description of input-based instruction, followed by a detailed description of outcomes-based instruction. Then, it illustrates how two courses required of mental health and family counseling students are taught from an input-based model and from an outcomes-based model where health issues are involved. First, these two models of instruction and evaluation are compared and contrasted.
Contrasting Views of Instruction and Evaluations
A useful way of comparing and contrasting these two models of instruction is with Miller’s (1990) pyramid and conceptualization of clinical competence. There are four progressive levels of competence in the pyramid. The first level, “knows,” is the base of the pyramid and represents factual knowledge gained by reading and studying didactic materials. The second level, “knows how,” represents the ability to use knowledge in a particular context. The third level, ‘‘shows how,’’ reflects the trainee’s capacity to appropriately interview and provide counseling intervention in a simulated or practice situation. The fourth level, “does” is the top of the pyramid and represents actual counseling practice in a real-life setting (Van der Vleuten, 2000).
Miller’s pyramid is also useful in comparing and contrasting the assessment and evaluation methods utilized in both instructional models. Input-based or traditional methods of assessment such as written tests and oral examinations can be quite useful in assessing “knows” and “knows how” but such indirect measures are too limited in assessing the higher levels of competence. Since assessing counseling competence at the “shows how” and “does” levels is central in the outcome-based or competency model, more direct and sophisticated methods of evaluation are required. For example, direct observations of counselor-trainees interviewing clients and providing counseling interventions is more appropriate and effective in evaluating the “shows how” level of competence, whereas assessment of the “does” level would involve evaluating an intern’s overall counseling competence in live or videotaped supervision. In both instances, rubric-based evaluation can provide immediate and objective feedback.
For counselor education programs, the challenge is to develop training strategies and assessment methods, particularly rubrics, to address the “shows how” level of competency.
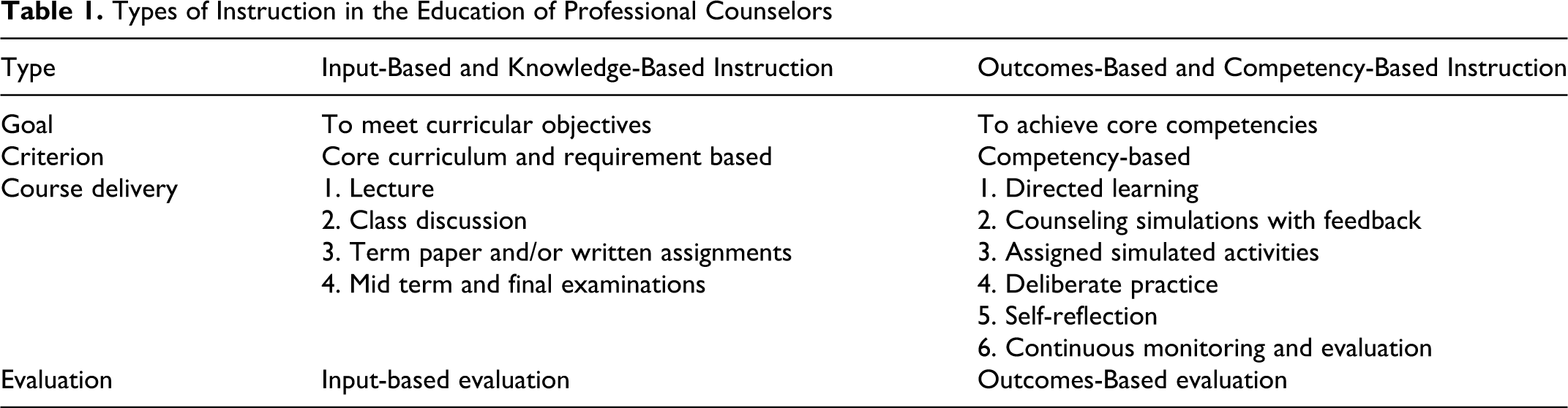
Table 1 characterizes both the input-based and the outcome-based training models in terms of goals, criterion, course delivery, and evaluation method. The following two sections describe and illustrate these models in considerable detail.
Types of Instruction in the Education of Professional Counselors
Input-Based Instruction
Input-based instruction is the traditional mode of instruction characteristic of most graduate education, including counselor education for quite some time. Its basic goal is to meet course objectives in a core curriculum. As such, it focuses primarily on the acquisition of knowledge and understanding which is the primary criterion, and secondarily on skill acquisition. It is also standards-based form of instruction. In the training of professional counselors, a standards-based program prepares students for meeting the requirements of licensure or certification. This means a student is expected to achieve passing grades in designated courses. This is followed by meeting requirements for supervised experience and passing state and/or national licensing or certification exam. Licensure or certification is achieved after all these standards and specific requirements are met. In this model, license or certificate holders are presumed to have achieved a minimal level of competence in a given professional specialty based on completion of specified requirements. Accordingly, they are deemed capable of the independent practice of a counseling specialty, which means direct supervision is no longer required. In recent years, this assumption has been challenged.
The delivery of such input-oriented instruction presumes that a given input of knowledge and understanding is necessary to achieve competency. Accordingly, the primary mode of instruction is the direct delivery of instruction through a lecture format. The lecture format might consist of a formal delivered presentation alone or aided by overhead or PowerPoint slides. It could be video assisted or include a demonstration. Instructors who can deliver lecture material in an interesting and entertaining manner are typically given high ratings by students. Class discussion is considered important in grounding the lecture material to be grounded in the student’s experience. Assigned activities such as required readings, term paper, and other written assignments are intended to complement and extend the instructor delivered material. Examinations, whether written or oral, are intended to assess knowledge acquisition. Input-based evaluation is given an air of respectability when course grades are quantifiable in terms of total points from exams, papers, and other assigned activities.
Illustration of Input-Based Training and Instruction
Following are examples of how two required counselor education courses are commonly taught from the perspective of an input-based model of instruction.
Psychopathology in counseling
Basic to the delivery of this course are lectures, videos, and course readings on the parameters of psychopathology. The use and particularly the limitations of the medical model on which Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition—Text Revision (DSM-IV-TR) is based are discussed. Considerable discussion occurs in many counselor education programs emphasizing the strength-based focus of the counseling profession. This course typically focuses on the principal diagnostic categories: anxiety disorders, mood disorders, psychotic disorders, substance abuse disorders, eating disorders, and the personality disorders. The limitations are discussed. In training counselors to become sensitive to a client’s health issues, students are taught the value of coding Axis III (medical conditions) of the DSM. The role of diagnosis and treatment options for counselors is discussed. Videotape demonstrating the diagnostic features of these disorders are shown and discussed in general terms. A term paper on an approved topic involving a specific diagnostic condition is a major requirement. Students are expected to pass a midterm and final exam on diagnostic conditions. For all practical purposes, the delivery of this course basically repeats the Abnormal Psychology course that many counseling students took as an undergraduate.
Family counseling
This course is lecture and discussion based. Lectures are enhanced with videotapes of various approaches and required readings. Family counseling is situated in relation individual counseling, and its history and origins are articulated. Couples counseling as a type of family counseling is discussed and illustrated. The basic terminology and systems theory are explained and family dynamics and the family life cycle are described. An overview of family therapy approaches with an emphasis on Adlerian, structural, strategic, object relations, cognitive behavioral, narrative, and solution focused. In training counselors to become sensitive to the role and impact of health issues on family dynamics and functioning, appropriate case material is introduced and discussed. Videotapes of these various approaches are viewed in class followed by general discussion. A term paper on an approved topic is a major requirement. Successful completion of the course typically requires students to pass a knowledge-focused examination/examinations.
Outcomes-Based Instruction
Outcomes-based instruction, also called competency-based learning, is increasingly common in graduate program as regional accrediting bodies and specialty accreditation standards have begun to require it. In this instruction model, the goal is for students to achieve a level of sufficiency in both knowledge of counseling theory and in counseling skills and practice. The criterion for completing a graduate program is not simply knowledge acquisition as in the input-oriented model but also a measurable level of competence in counseling practice at or above the minimal level of competence. It has been noted that the current competency movement is influencing licensure and certification boards to require applicants to demonstrate competence in counseling practice in addition to knowledge of counseling theory.
The delivery of outcomes-based instruction differs from input-oriented instruction. The difference ranges by degrees depending on the course. For instance, greater differences will be noted in prepracticum, practicum, and internship courses than in more didactic course. The designation-directed learning represents the main difference. Directed learning may include focused lecture, but it includes simulated activities which involve assessment of the learner’s performance evaluation.
For example, in teaching the process of writing case conceptualizations the instructor may begin by defining and describing case conceptualizations and presenting examples of adequate and inadequate conceptualizations. This is followed by guidelines for developing an adequate conceptualization. Then graded case material (easy to more complex) is provided for which students follow the guidelines and draft a case conceptualization. Then the instructor reviews the student’s draft and provides immediate feedback. In a prepracticum course, simulated counseling encounters can effectively promote the learning of specific counseling practice competencies. In dyads with one student in the counselor role and the other in the client role, the “client” presents with a scripted problem which is then processed by the “counselor” for 10 min. If the “counselor” gets stuck or off track the instructor provides immediate feedback evaluation in the form coaching, and if no coaching is indicated, the instructor provides immediate feedback guided by a rubric which assesses the “counselor’s” performance on observable criteria.
Other forms of delivery include assigned simulated activities which occur between class meetings. These may include case conceptualization exercises, diagnostic evaluation interviews, simulated counseling encounters, and so on. Since research shows that deliberate practice and self-reflection significantly increase counseling practice competencies, these activities may be assigned. For example, practicum and internship students can be assigned to keep a journal in which they reflect on how they handled or could have handled given counseling challenges. From an outcome-oriented perspective, practicum and internship experiences offer training multiple opportunities to receive ongoing feedback of their counseling performance from supervisors, and from clients utilizing ultrabrief rating scales such as the Outcomes Rating scale and Session Rating scale (Miller, Duncan, Brown, Sorrell, & Chalk, 2006).
Illustration of Outcomes-Based Training and Instruction
Following are examples of how two required counselor education courses are commonly taught from the perspective of an outcome-oriented, competency-based model of instruction.
Example: Psychopathology in counseling
In addition to providing an overview of the anxiety disorders, mood disorders, psychotic disorders, substance abuse disorders, eating disorders, and the personality disorders, this course requires students to achieve a minimal level of sufficiency in conducting diagnostic evaluations, writing initial evaluation report, and providing counseling interventions for specific diagnostic conditions. A basic directed learning strategy for achieving competence in assessing and diagnosing psychopathology is the use of selected videotape that demonstrate effective diagnostic interviewing for specific diagnostic conditions. Before the video clip is shown, the diagnostic criteria for that condition are presented. While viewing the video are asked to carefully observe how the diagnostic interview is conducted to assess DSM criteria and rule-in and rule-out other diagnostic considerations. Class discussion after the video focuses on identifying specific criteria elicited in the interview. Assigned simulated activities require students to achieve sufficiency in accurately utilizing the DSM and diagnosing 10 clinical cases. Specific written and verbal feedback reinforce this competency. Students are also expected to conduct two complete diagnostic evaluations and prepare an initial evaluation report following a protocol of 11 sections including presenting problem, mental status exam, case conceptualization including a cultural formulation, a 5-axis DSM diagnoses, and a detailed treatment formulation and plan. These reports are rubric evaluated with specific feedback. The third competency involves implementing a counseling intervention for a specified diagnostic condition. Previously, transcriptions of earlier sessions of a simulated case are enacted in class. Students then provide a session transcription of a follow session which is rubric evaluated. A final written examination involves two cases in which students evaluate case material and diagnose Axes I, II, and IV. Students also engage in self-reflection on their learning experience and log it. Since individual psychopathology is expressed within a family context, students are oriented to the Global Assessment of Relationship Functioning (GARF) scale by means of short video clips of the five ranges of family functioning and associated Axis I disorders. Like the Global Assessment of Functioning scale (GAF), GARF can also be included in Axis V, and students are expected to do so.
Example: Family counseling
In addition to providing an overview of the origins of family counseling and systems theory, this course requires students to achieve a minimal level of sufficiency in conducting family assessments and initiating family interventions. Assessment of family functioning and resilience is emphasized by means of the genogram, measures of family functioning—particularly family resilience and the Beavers Interactional scales. Trigger tapes are utilized to teach the use of a rating scale for family functioning, and case material is utilized to teach the correct use of the genogram. Family interventions are introduced with videotapes of the family therapy approaches: Adlerian, structural, strategic, object relations, cognitive–behavioral, narrative, and solution focused. Assigned simulated activities require students to assess four families using these methods and developing an assessment report with a systemic case conceptualization and treatment plan. Written reports of the family assessment are rubric evaluated as is the brief class presentations of one of these assessments. Students also learn a method of coaching parents through simulation exercises. Then, they utilize this method to coach two sets of the parents they have previously assessed. The cases are then written up and submitted along with the transcriptions of that coaching. The instructor then evaluates this material with the aid of rubrics which provide focused feedback to the student. Students present one of the reports and the transcription to the class.
Concluding Note
The shift from input-based to outcomes-based instruction is underway and will continue to gain momentum. Paradigm shifts are like that: new way inevitably replaces traditional and time-honored ways of doing things. Colleagues who have read the above descriptions of these two forms course delivery report their surprise at how different course delivery and evaluation was for between the two forms of instruction. Not surprisingly, because this shift involves significant changes in how courses are planned, delivered, and evaluated, these changes can be expected to engender discomfort, fear, and suspicion among some counselor educators and supervisors. Grieving the passing of the old ways of training counselors is to be expected. At the same time, the expectation is that there will be noticeable positive changes in student competence and confidence as they complete outcomes-based training and enter practice as licensed counselors or therapists.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.