
Abstract
Family counselors often counsel families where children are at increased risk of maltreatment. Yet there exists a paucity of free, brief, face-to-face, standardized, assessment instruments designed for family counselors to assess child abuse. To address this paucity, the authors created The Juhnke, Henderson, Juhnke Child Abuse and Neglect Risk Assessment scale. The scale is an evidenced informed instrument that considers 20 child maltreatment risk factors identified by the U.S. Department of Health and Human Services (USDHHS) Office of Child Abuse and Neglect. The primary purpose of the scale is to facilitate a thorough maltreatment assessment and to generate guidelines that can be used, in conjunction with clinical judgment, to aid in the creation of an effective child protective agency report and potentially facilitate effective intervention.
In 2010, child protective service (CPS) agencies received more than 3.3 million reports for alleged maltreatment of nearly 6 million children (U.S. Department of Health and Human Services, Administration on Children, Youth, and Families [USDHHS], 2010). Nearly 1.8 million of those reports were investigated (USDHHS, 2010), and 695,000 children were estimated as being maltreatment victims (USDHHS, 2010, p. 22). In that same year, another 1,537 children died from documented maltreatment (USDHHS, 2010, p. 58). Regretfully, these numbers likely underreport the actual numbers of children who suffer maltreatment or die from abuse-related behaviors, because many child abuse victims go unrecognized or unreported (P. Granello, personal communication, February 5, 2011).
The Family Journal has published superior articles specific to pertinent child maltreatment topics for marriage and family counselors. These articles include Bean, Softas-Nall, and Mahoney’s (2011) piece on potential challenges specific to mandated reporting and therapeutic implications, Hunter’s (2006) encompassing literature review of child sexual abuse and the important implications for marriage and family counselors, and Lewis’ (1993) thought-provoking article on child sexual abuse and potential theoretical dilemmas for family counselors. In addition, many other scholars have directly or indirectly reported the relevancy of maltreatment and the significance of maltreatment to the marriage and family counseling process (e.g., Adams, 2006; Miller, Veltkamp, Lane, Bilyeu, & Elzie, 2002).
However, despite The Family Journal’s coverage of maltreatment and the substantial ramifications for marriage and family counselors, no articles have been published within The Family Journal or elsewhere that provide a free, brief, face-to-face, standardized child maltreatment assessment instrument specifically designed for family counselors. Thus, the primary intent of this article is to describe The Juhnke, Henderson, Juhnke Child Abuse and Neglect Risk Assessment scale and the scale’s use as an aid to facilitate a thorough assessment of child sexual or physical abuse, or neglect. The article will further provide a brief overview of the scale’s general response guidelines.
Evidenced Informed
The Juhnke, Henderson, Juhnke Child Abuse and Neglect Risk Assessment scale is evidence informed. The scale’s 20 child maltreatment risk factors are founded upon risk factors identified by the USDHHS Office of Child Abuse and Neglect and noted as important to child maltreatment assessment (Cage & Salus, 2010). The majority of these risk factors were utilized by the first and second authors when assessing and intervening with children believed to be experiencing maltreatment during their combined 26 years of counseling and were helpful in making a thorough maltreatment assessment.
Why Use Mnemonics?
Twenty independent maltreatment risk factors are difficult to recall, especially during an emotionally charged maltreatment assessment. Before the scale was created, the first author would query children related to their maltreatment experiences and attempt to simply remember maltreatment risk factors from his earlier training. These experiences were less than optimal and there were times he forgot to ask pertinent information regarding specific risk factors that were highly correlated with maltreatment. To address this situation and aid counselors-in-training, as well as less experienced and practicing counselors, the authors created a scale that utilizes a mnemonic memory aid format. This format is designed to promote family counselors’ recall of critical maltreatment risk items and ensure a thorough, multidomain maltreatment assessment.
Patterson, Dohn, Bird, and Patterson’s (1983) and Juhnke’s (1994) seminal research demonstrated the effectiveness of mental health trainees utilizing mnemonics within the suicide assessment process. Their findings indicated students who used mnemonic memory aids were statistically better able to recall important risk factors than those who simply learned multiple assessment factor lists. They further found that students who utilized mnemonics facilitated more thorough assessments and more accurately scored clinical vignettes.
Today, mnemonics are broadly utilized as a means to recall important factors and sequences and to remember relevant instructions. For example, the American Association for Suicidiology (2012) encourages counseling professionals to utilize the mnemonic, IS PATH WARM, when assessing suicide risk. Medical professionals frequently use mnemonics such as, Every Little Boy Must Pray, to remind providers the specific order of drugs to be given when attempting to resuscitate patients’ whose hearts have stopped (epinephrine, lidocaine, bretylium, magsulfate, and procainamide; C. Weiner, personal communication, February 6, 2012). Law enforcement professionals use mnemonics such as GO WISELY to help them thoroughly investigate a crime scene (grounds, object, warrant, identification, station, entitlement, lawfully, and year; D. Macintosh, personal communication, February 7, 2012). The U.S. military commonly use mnemonics like the Four Fs (find, fix, flank, and finish) and BRASS (breath, relax, aim, slack, and shoot) to aid soldiers in their assigned charges and enhance memory recall (J. LoBrutto, personal communication, February 6, 2012). Given both the research demonstrating the benefits of mnemonics and the widespread application of mnemonics to aid factor recall and memory, the authors’ believed utilizing mnemonics for the scale would generate greater recall of the 20 USDHHS Office of Child Abuse and Neglect maltreatment factors.
To ensure selection of the most appropriate counseling intervention, decision of whether or not to consult with/report to CPS and to help protect the family counselor from potential liability, the counselor should always convene a maltreatment risk assessment committee or utilize the “four out of five” rule (Juhnke, Granello, & Granello, 2010). Here, the family counselor describes the case, the maltreatment risk factors identified via the Juhnke, Henderson, and Juhnke Child Abuse and Neglect Risk Assessment scale, the intended intervention, and the potential CPS report. The family counselor then consults with the committee of five licensed mental health professionals to determine whether the proposed intervention and CPS report is clinically, ethically, and legally appropriate. If the committee or four out of the five professionals believe the proposed intervention and CPS report are appropriate, the family counselor commences the plan and the report. As always, consultation with one’s clinical supervisor/supervisors, legal counsel, and professional liability insurance’s risk management division is warranted.
The Scale and Risk Factor Scoring
The Juhnke, Henderson, Juhnke Child Abuse and Neglect Risk Assessment scale is atheoretical in nature. It is not connected to a family counseling or systems-specific theory or model. The scale was created to serve family counselors as one component of an overall thorough children’s maltreatment assessment process and takes approximately 8–10 min to administer. Therefore, the scale can be easily administered during part of an initial clinical intake session or immediately upon suspecting child maltreatment.
The scale is comprised of 20 independent risk factors identified by the USDHHS Office of Child Abuse and Neglect as important to child maltreatment assessment (Cage & Salus, 2010). Five individual risk factors are used to form a mnemonic with a total of four separate mnemonics (i.e., BBATCH, SPACY, SCRAPP, CARDS). Each mnemonic corresponds to one of four critical maltreatment domains (i.e., physical, familial/milieu, demographic, and emotional/behavioral domains). The individual mnemonic critical domains are then linked together via the sentence, A BBATCH of SPACY SCRAPP CARDS. The intent of utilizing the mnemonic format is to assist family counselors’ risk factor recall and promote thorough, multidomain assessments.
Each factor receives an individual factor score. Out of the 20 risk factors, the presence of four specific risk factors requires immediate CPS consultation or reporting. These maltreatment factors include buttocks burns, thigh, history, and report. Each of these factors receives either a score of “80” or “0.” The remaining 16 individual risk factors receive scores of either “5” or “0” points depending upon the presence of factor criteria. The possible total score range is between “0” and “400” (see Table 1). The individual mnemonic and its corresponding factors are indicated below with a description of each factor. The risk factors that are preceded by an asterisk indicate factors typically requiring immediate CPS consultation and/or reporting.
The Juhnke, Henderson, Juhnke Child Abuse and Neglect Risk Assessment Scale

Note. Instructions: Each risk factor has a value of either “80” or “0,” or “5” or “0.” Scores of “80” require immediate CPS consult/report. Scores of “80” or “5” indicate risk factor presence. Scores of “0” indicate risk factor absence. Place an “X” in the corresponding “CPS consult/report” box when a score of “80” for an individual risk factor is circled. Add the total score for each maltreatment mnemonic and sum to compute the total score. Add the total number of “CPS consult/report” “Xs” for BBATCH and SPACY mnemonics; sum the “total Xs” box. Double check total score accuracy by adding each column’s subtotal score, summing, and comparing to total score box. Match the total score with Table 2’s general response guidelines. CPS = child protective service; BBATCH = buttocks burns, anal, thigh, clothing, history; SPACY, substance, poverty, away, caring, young; SCRAPP = smell, coming, report, accident prone, previous; CARDS = cowering, age, regression, disability, shrinking.
Physical Domain: BBATCH (Buttocks Burns, Anal, Thigh, Clothing, History)
*Buttocks burns or burns around the anogenital region, or on the backs of hands, or on both hands, especially if severe
Here, the marriage and family counselor is verbally assessing the child to determine whether the child has burns on the buttocks region, burns around the anogenital region, or burns on the back of the hands. Specifically, the family counselor will query the child regarding the existence of such burns. Should burns exist, the family counselor will seek information regarding how the burns were inflicted and by whom (e.g., self, parent/parents, siblings, others, etc.). Burns to both hands or especially severe burns are highly suggestive of child physical abuse. Eighty (80) points is scored if any of the above factors are present. Presence of this maltreatment risk factor alone or in combination with other factors typically requires immediate CPS consultation and/or reporting.
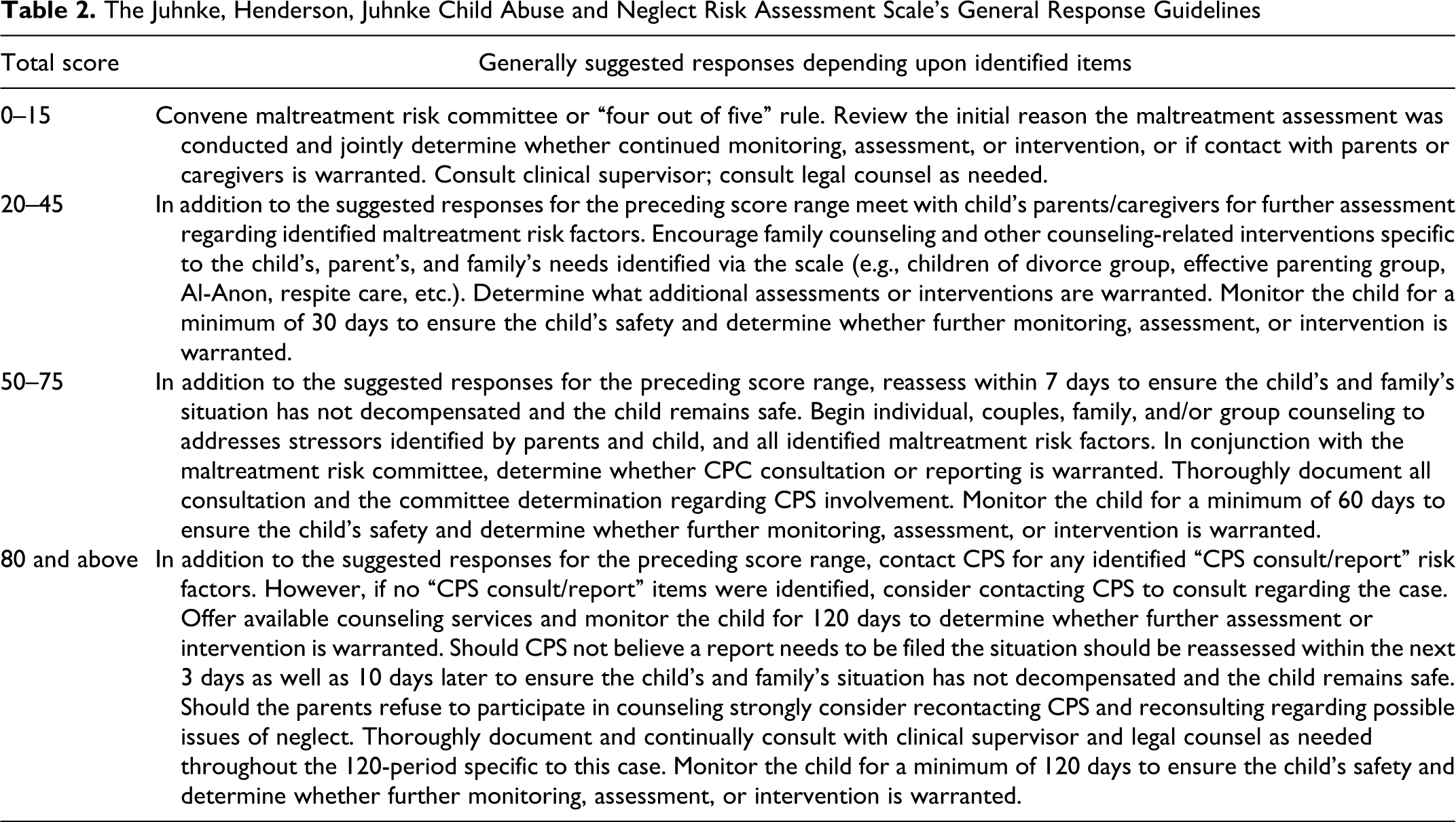
The Juhnke, Henderson, Juhnke Child Abuse and Neglect Risk Assessment Scale’s General Response Guidelines
Anal or genital itching, pain, or bleeding, sudden enuresis or encopresis onset, or difficulty walking or sitting
Children complaining about or experiencing anal or genital itching, pain, or bleeding, or sudden enuresis or encopresis onset, or having difficulty walking or sitting due to anal or genital itching, pain, or discomfort, or who are observed wincing or flinching when beginning to sit or stand receive five (5) points. The enuresis or encopresis factors for this item do not reflect developmental- or age-related, wetting or soiling mishaps common to very young children. Rather they reflect the sudden onset of enuresis or encopresis with a child who had theretofore not had wetting or soiling issues.
*Bruises or injury to inner thigh areas, genitalia areas, areas between the eyes and nose, or on facial checks, neck, tips of shoulders, or inner arm areas
Bruises or injury to the inner thigh, genitalia, areas between the eyes and nose, or on facial checks, neck, tips of shoulders, or inner arm are atypical of accidents and suggestive of potential abuse. Therefore, family counselors will query children regarding any bruising or injury to these areas. Specifically, the family counselor will want to investigate who was with the child at the time of the injury or bruising, whether the injury or bruising came about via accident or play or was the result of “punishment” or “correction” given by a caregiver or other person. Eighty (80) points are scored on this factor for any indications of such injuries. Presence of this maltreatment risk factor alone or in combination with other factors typically requires immediate CPS consultation and/or report.
Wearing clothing that covers the body and may be inappropriate in warmer months, such as wearing a turtleneck sweater in the summer (be aware that this may possibly be a cultural issue instead). Clothing is typically designed to cover one’s body. However, in this case, the family counselor is assessing for children wearing clothing that suggests the child is attempting to cover bruises, burns, or injuries suggestive of abuse or the weight loss caused by neglect. Although, the caveat “Be aware that this may possibly be a cultural issue instead” is included by the USDHHS Office of Child Abuse and Neglect (Cage & Salus, 2010, p. 12), the more significant assessment issue is whether the worn clothing appears out of fashion with other children at the same time and place. An example would be if the majority of children on the day of the assessment are wearing flip flops, shorts, and loose-fitting tops or t-shirts and the child being assessed is wearing a bulky jacket, long-sleeve sweatshirt, heavy jean pants, and boots. Also, if the clothing worn seems particularly incongruent with the day’s temperature and humidity (e.g., wearing a heavy, long-sleeve sweatshirt, and blue jeans in 95° heat), and it does not appear that the clothing was merely a 1-day anomaly but rather worn on consecutive days in such intense heat, the factor’s criteria are met and the child receives five (5) points.
*Burns or injuries out of proportion to the history provided by caretaker or beyond the child’s developmental stage or development
This factor is specific to the caregivers’ suspect description of how burns or injuries occurred, or injuries or burns that appear incongruent with a child’s cognitive or physical development. Examples of this might include a caregiver indicating the 5-year-old child’s (a) severe and extensive burns on both hands occurred as a result of the child’s “simply playing with matches” or (b) extensive trauma to her inner thighs occurred by riding her mountain bike “too hard” through the woods. Eighty (80) points are scored on this factor. Presence of this maltreatment risk factor alone or in combination with other factors typically requires immediate CPS consultation and/or report.
Familial/Milieu Domain: SPACY (Substance, Poverty, Away, Caring, Young)
Substance abuse by parents
Substance abusing parents have a higher probability of neglecting and abusing their children. Thus, parents who are substance dependent or actively abuse substances place their children at greater maltreatment risk. However, there are many issues that family counselors need to investigate specific to this risk factor and, as is the case with most risk factors, there exists varying degrees of risk based upon the situation. For example, when a child appears to be functioning well and does not appear to be maltreated, parents who sometimes abuse alcohol or cannabis may not warrant a CPS report. However, parents who are dependent and constantly abusing substances such as methamphetamines or heroine, and neglecting their children due to their substance abuse or dependence warrant CPS report. Thus, for the purposes of this assessment, if one or more parents or caregivers in the home frequently abuse substances and their substance abuse seem to be negatively impacting children five (5) points are assigned to this factor. If no substance abuse is occurring by parents, zero (0) points are assigned. Family counselors are encouraged to be familiar with the mandated reporting law in their states and to adapt the scoring of this factor accordingly.
Family living in poverty
Although many families living in poverty are loving, supportive, and nurturing, the USDHHS indicates poverty is a significant maltreatment risk factor. Therefore, if the family is living below the subsistence level the family counselor will query the child regarding typical food intake, running water, heating and cooling, and safe and adequate living conditions. Because the USDHHS notes poverty as a maltreatment correlate, families living in poverty receive five (5) points on this factor.
History of running away from home
Children who experience maltreatment frequently have a history of running away from home in an attempt to escape maltreatment or improve their quality of life. When assessing the child for maltreatment, the family counselor will query the child regarding running away behaviors and the reasons for same to determine if the running away behaviors were in response to maltreatment. An absence of running away behaviors results in zero (0) points on this factor. Whereas running away behaviors result in a score of five (5) points.
Report needing to care or caring for younger siblings
Caring for younger siblings is correlated with children of maltreatment. Therefore, the family counselor should query children to determine whether they are caring for younger siblings in the absence of caregivers or whether they perceive an inordinate need to care for younger siblings who need protection or nurturing due to parental absence, neglect, or abuse. Family counselors should determine the frequency of caring and the extent to which the child is caring for younger siblings. The absence of this factor provides zero (0) points on this factor. However, if they are providing age inappropriate levels of care, nurturing, protection, or support due to parental maltreatment they receive five (5) points.
Having young parents
Young parents can be very nurturing, loving, and protective of their children. However, there exists a high correlation between young parents and maltreatment. When assessing for maltreatment, family counselors will determine whether young parents understand their children’s physical, emotional, social, intellectual, and psychological needs. Due to the correlation between young parents and maltreatment, parents over the age of majority receive zero (0) points, and parents under the age of majority receive five (5) points on this factor.
Demographic Domain: SCRAPP (Smell, Coming, Report, Accident Prone, Previous)
Smell of urine or feces or poor personal hygiene
This factor involves more than developmental- or age-related lack of hygiene or personal care. It also does not reflect developmental- or age-related infrequent or occasional wetting or soiling mishaps. Instead, this factor reflects recurrent or frequent wetting or soiling that is atypical for the child’s age and developmental stage, or the lack of clean clothing suggesting a lack of proper adult supervision, care, or nurturance. Children who fulfill this factor receive five (5) points.
Coming to school too early or not wanting to leave school, and/or indicating a possible fear of being at home
This factor does not represent the typical eager to please or strikingly inquisitive child. Instead it represents a child who is anxious or fearful of being at home or who has little parental nurturance or support, or who lacks adequate food and shelter at home. This is a child who comes early to school to find shelter, food, safety, or the nurturance of an adult. Often these children will attempt to gain support and nurturance through a trusted teacher, custodian, nurse, or other support staff, or a volunteering parent. Frequently, they do not want to return home, because home is a place of danger, emotional strife, or emptiness, or home does not provide adequate heat, cooling, or accommodation. Children who fulfill this factor receive five (5) points.
*Report of maltreatment (self-report or report by other)
Anytime children report maltreatment by others, immediate action must be taken. Here, the family counselor will query the child to determine: what type/types of maltreatment have occurred, who perpetrated the maltreatment, when the maltreatment occurred, where the maltreatment occurred, who else may have been maltreated, and others in addition to the chief perpetrator who may have participated in or known about the maltreatment and failed to respond. Eighty (80) points are scored on this factor. The presence of this factor alone or in combination with other factors requires immediate CPS consultation and report.
Described by parents or caregivers as “accident prone”
Maltreating parents and caregivers frequently describe maltreated children as accident prone. Such allegations are often used by perpetrators in an attempt to “explain away” any physical injuries or suspect behaviors that could alert others to the child’s maltreatment. Whenever a family counselor is informed that a child is accident prone, the family counselor will pay closer attention for potential incongruencies between the explanations of physical injuries indicated by the children in question and the persons’ making the statement. The family counselor also will query the child and seek the child’s account of injuries and how those injuries were sustained. The USDHHS encourages evaluators to pay attention to such caregiver statements. For that reason, parents or caregivers who report children as accident prone receive five (5) points on this factor. However, it should be noted that some children are less coordinated and have less hand–eye coordination or visual acuity than peers of similar ages. Hence, they may sustain more injuries in comparison to peers. Points from this factor alone should be viewed with great caution. Instead, family counselors should consider this factor only in combination with other high-risk factors.
Previous sexual or physical abuse of child
Parents and caregivers who have previously maltreated children or have a history of maltreatment are at increased risk of continuing or repeating such behaviors. Consequently, the USDHHS notes this risk factor is correlated with maltreatment. Family counselors treating families that have experienced previous maltreatment should query parents, caregivers, and children regarding previous maltreatment, precipitators to that maltreatment, and reported changed behaviors since the maltreatment episodes. Specifically, the family counselor will want to know how the previous perpetrator, other parents or adults in the family system, and children will respond differently should the precipitators from the previous maltreatment arise again, and how they will inform the family counselor of any potential concerns before maltreatment occurs. Additionally, the family counselor will want to seek releases of confidential information to understand the degree and previous types of maltreatment accusations and the findings of any investigations. In this way, the family counselor can monitor the situation and keep close watch for any suspect behaviors or situations which seem similar to the previous maltreatment situations. Furthermore, the family counselor will want to determine whether there exists any outstanding court or CPS actions that remain in effect with the family. Fulfillment of this criteria results in five (5) points.
Emotional/Behavioral Domain: CARDS (Cowering, Age, Regression, Disability, Shrinking)
Cowering, withdraw, or demonstrating fear of adults or inordinate fear of men or women
Once again, the scale is not encouraging criteria fulfillment simply based upon typical developmental and age appropriate behaviors demonstrated by very young children. Instead, these are atypical behaviors. For the most part, they will display with an age inappropriate intensity. Thus, demonstrations of cowering, atypical withdraw or fear of adults, or inordinate “blanket” fear of all men or all women fulfill this criteria. Family counselors should be cautious not to revictimize the child by forcing engagement with the counselor. Rather, the family counselor should slowly build trust and opportunities for engagement. Additionally, the family counselor should query the child regarding possible past or current maltreatment and query caregivers regarding the child’s atypical behaviors to determine how to best respond to the child’s needs. Fulfillment of this criteria results in five (5) points.
Age inappropriate seductive behaviors and/or more sexual knowledge than is age appropriate, especially in younger children
There exists a correlation among young children demonstrating seductive behaviors or sexual knowledge beyond their presenting age and maltreatment. Thus, the USDHHS includes this as a risk factor. Family counselors encountering young children presenting in a seductive manner or with more sexual knowledge than is age appropriate will investigate how the children learned these behaviors and knowledge. Children presenting with either inappropriate seductive behaviors or more sexual knowledge than is age appropriate receive five (5) points on this factor.
Regression to earlier developmental levels or less mature behaviors
Regressive behaviors or demonstrating behaviors that are less mature than the child’s actual chronological age or development are risk factors identified by the USDHHS as suggestive of maltreatment. Here, family counselors will want to query the child, parents, teachers, and others as to the onset of the regressive behaviors and attempt to determine whether these behaviors may correlate with potential maltreatment trauma. Children demonstrating regression to earlier developmental levels or demonstrating behaviors that are less mature than they had previously attained and had generally maintained are awarded five (5) points on this criteria.
Having an emotional, physical, or developmental disability
Regretfully, children who are emotionally, physically, or developmentally challenged can be easy targets for perpetrators and have a higher incidence of maltreatment. Although many families with challenged children provide loving and nurturing environments, the additional stressors and needs of challenged children have the potential to tax the family system and push parents and siblings past their limits. Thus, the USDHHS identifies children with emotional, physical, or developmental disabilities at risk, and for the purposes of this scale, those families with such challenged child members receive five (5) points on this factor. Family counselors treating children and adolescents with emotional, physical, or developmental disabilities should pay special attention to this and other risk factors to ensure the safety of these special needs children.
Shrinking away from or dislike physical contact (e.g., may not tolerate physical praise, such as a pat on the back)
Children who shrink away from or dislike physical contact may be attempting to establish appropriate boundaries after maltreatment. Although an appropriate touch on the shoulder or pat on the back may be intended as a means to demonstrate support, children who have been maltreated may experience such behaviors as caustic. These behaviors also may provoke unintended flashbacks of maltreatment or increased arousal with defensive posturing by the child. Thus, the shrinking away or dislike of physical contact may be suggestive of children who have experienced maltreatment. Children presenting with these behaviors receive five (5) points on this assessment.
Total Scale Score Range
The scale offers general response guidelines based upon the total scale score. Table 2 reviews the general response guidelines for the range of possible total scores. These suggestions are presented in a general template format that encourage the family counselor to adapt and mold the general response guidelines to the assessed child’s specific needs, the unique situation, and other idiosyncratic issues such as the child’s age, protective factors such as having one parent or multiple relatives committed to protecting the child, and the severity of the behavior, drug use, or maltreatment.
Limitations
Despite the many positives related to the scale, the scale has limitations. The Juhnke, Henderson, Juhnke Child Abuse and Neglect Risk Assessment scale cannot precisely identify every child who has or is experiencing maltreatment. Furthermore, it cannot tell each family counselor how to respond to every maltreated child or situation. Thus, the scale was designed to serve as one component within an organized and thorough maltreatment assessment process that should include other components, such as psychological testing, clinical interviews with the alleged perpetrator/perpetrators, nonperpetrating parents and relatives, siblings, and teachers, as well as other components deemed necessary to make an informed and logical intervention with the child and family. The suggested responses should be viewed as general in nature and modified to meet the specific idiosyncratic needs of the child and the family system. Additionally, the presence of any one maltreatment risk factor not identified as requiring CPS consultation and report does not mean the child was, is, or will be maltreated. However, a significant clustering of high-risk factors suggests increased risk. Additionally, scores with single factors such as disabilities, regression, or running away may not by themselves suggest potential maltreatment risk but may suggest a person’s need for more general family counseling services. Concomitantly, whatever decisions made should be made in conjunction with input from one’s supervisor, legal counsel, and a team of skilled and experienced marriage and family counselors who are knowledgably in maltreatment risk assessment. Stated differently, the Juhnke, Henderson, Juhnke Child Abuse and Neglect Risk Assessment scale provides suggested templates that must be modified as necessary to address the specific needs of the child and ensure the child’s complete safety. The resulting intervention should be constructed in a manner that will provide the greatest degree of safety for the child. Finally, it is noted that the scale warrants further research. Such investigation is currently in process and expected to begin within the year.
Conclusion
The Juhnke, Henderson, Juhnke Child Abuse and Neglect Risk Assessment scale demonstrates potential utility for family counselors who wish to conduct a child maltreatment assessment. The scale is easy to use and provides a thorough assessment based upon risk factors identified by the USDHHS as important to the maltreatment assessment process. These risk factors ensure the assessment reviews four separate domain areas important to the child. Administration and scoring time are minimal. The scale also addresses the paucity of free, face-to-face, standardized maltreatment instruments and provides family counselors another instrument in their assessment arsenal.
Footnotes
Acknowledgments
The authors thank the following persons for providing consultation, review, and discussion of risk factors, mnemonics, data, or additional suggestions regarding the scale and article: Thelma Duffey, LPC, LMFT; Beth A. Duroydoye, Ed.D., NCC; Paul F. Granello, Ph.D., LPCC-S; Shane Haberstroh, Ed.D., LPC, NCC, AAC, ICAADC; Michael Karcher, Ph.D., Ed.D.; Mr. Joseph Lobrutto; Mr. Douglas Macintosh; Michael Moyer, Ph.D., LPC; Nathaniel Ivers, Ph.D., LPC, NCC; Jeremy Sullivan, Ph.D., LP, LSSP; Felicia Castro Villarreal, Ph.D., LSSP, and Ms. Cheryl J. Weimer, RN.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.