
Abstract
The aim of this study was to compare refugee children’s psychological well-being before and after brief family therapy. Families from Bosnia-Herzegovina with one child aged 5–12 years received three family therapy sessions. Psychological assessments using the Erica play-diagnostic method and parental interviews were made before and after the intervention. The main finding was that more children built normal sandboxes (showing no pathological findings)
There are more than 40 million refugees and displaced people in the world, almost half of whom are children (U.N. High Commissioner for Refugees, 2010), and many of those children are severely affected by different forms of organized violence. It is a big challenge to find interventions that provide appropriate means for meeting the needs of refugee families in their new host countries.
The experience of war and violence increases the risk for psychological distress and the development of psychiatric disorders in children (Rousseau, 1995). When refugee families leave their country of origin, they may also leave behind their culture and support systems. However, their ability to overcome the emerging adversities still remains intact (Voulgaridou, Papadoupoulos, & Tomaras, 2006). Adaptability and cohesion within families seem to protect the emotional well-being of very young children following traumatic exposure (Laor et al., 1996). One study demonstrated the need to take social context and the meaning of events into account when examining the impact of war exposure on psychological well-being (Jones & Kafetsios, 2005). Parents are influenced by their children’s coping success or failure (Almqvist & Hwang, 1999). Garbarino and colleagues claimed that young children will continue to cope with difficult situations, as long as their parents are not pushed beyond their stress-absorption capacity (Garbarino, 1991). A holistic approach is necessary when working with young refugees (Papadopoulos, 1999).
Peltonen and Punamaki (2010) observed that increasing research is available on the preconditions for being able to improve the child mental health of the children, but less is known about how to translate these findings into effective interventions to help traumatized children. The authors concluded on the basis of their literature review that substantial additional work needs to be done to develop effective preventive interventions and treatments for children traumatized by exposure to the trauma of armed conflict. Concerning small children, Ehntholt and Yule (2006) concluded that there are as yet relatively few publications on interventions for war-affected children under the age of eight.
Ehntholt and Yule (2006) noted in a summary of assessments and treatment of refugee children and adolescents who have experienced war-related trauma that a phased model of intervention is often useful. They also pointed out that employing a holistic approach is crucial. Several surveys focus on the importance of the parental role and on considering the whole family system in supporting children and youth. A study with a brief, community-based parenting intervention for Vietnamese American immigrant parents showed that the participants reported a greater intention to show expressive love to their children as well as increased parental empathy after the intervention (Wong et al., 2011).
A study of Kosovar refugees with a mean age of 13 years showed that a psychosocial treatment program consisting of individual, family, and group sessions gave results with improvement in overall psychosocial functions for all but those in a subgroup of severely traumatized patients with complex psychiatric disturbances (Möhlen, Parzer, & Brunner, 2005). Another psychosocial intervention program, a randomized controlled trial, evaluated the effects on small children (5-year-olds) in Bosnia and Herzegovina. The program consisted of weekly support group meetings for mothers over a 5-month period (Dybdahl, 2001). The intervention program had positive effects both on the mothers' and the children’s mental health.
A cognitive model of posttraumatic stress disorder (PTSD) has been successfully applied to refugee children (Ehlers & Clark, 2000) and has been described in two case vignettes (Vickers, 2005). A randomized, controlled trial showed that both child-centered play therapy and trauma-focused cognitive-behavioral therapy were effective in reducing symptoms of traumatized refugee children in the United States according to reports from both children and parents (Schottelkorb, Doumas, & Garcia, 2012). Bernardon and Pernice-Duca (2010) have pointed out the need for a systemic family perspective, including a narrative therapy approach when considering the development, maintenance, prevention, and resolution of PTSD in children and adolescents. In a study of Cambodian refugee families in the United States, the authors stress that, because the family is the center of life for these families, healing must occur within this family context (Wycoff, Tinagon, & Dickson, 2011). Thus, the few studies carried out in this field indicate a need for more research work to be done in this area, as well as pointing out that family interventions are preferable.
During the period 1992–1995 about 50,000 people came from Bosnia-Herzegovina and received permission to stay permanently in Sweden (Migrationsverket, 2009). There is a Swedish study (Alinder, Ralphsson, Bjar, Wessman, & Lindfors, 1998) of family treatment sessions in the homes of eight refugee families coming from Bosnia. The refugees themselves reported positive effects resulting from these family sessions.
The present study of refugees from Bosnia-Herzegovina also focused on the families. An approach combining intervention with family therapy sessions and the play-diagnostic Erica method (Sjolund, 1981) designed for younger children was chosen.
Method
Participants
Refugee families from Bosnia-Herzegovina were asked to participate in this study by a nurse at a medical health center or through contacts with social workers in the communities where the families lived. The diagnostic interviews were done between 1995 and 2000. The families had arrived between 1992 and 1995. Fourteen families initially participated in this study. One participated only in the baseline interview, two families did not participate in the family therapy sessions; one family did not attend the evaluation session after the intervention. Thus, it was possible for us to evaluate 10 children, 5 boys and 5 girls. The index children had at baseline interview between zero and three siblings. In five cases, they had one sibling. These 10 families had been in Sweden an average of 4 years (range 2–7 years) before baseline data were collected. The average age of the children on arrival in Sweden was 4.5 years (range half-a-year to 9 years). The inclusion criteria were (1) coming from Bosnia-Herzegovina, (2) having permission to stay in Sweden permanently, and (3) having at least one child in the family between 5 and 12 years old.
Procedure
Parents in all families were interviewed by the same interviewer designated here as Interviewer 1 (one of the family therapists) about background factors, present situation, and symptoms of the index children at baseline. In five cases, both parents were present at the interview. The index children participated in the Erica play method (Danielsson, 1986; Sjolund, 1981) with three observations carried out by Psychologist A. After baseline evaluation, the intervention consisting of three family therapy sessions was carried out by the first author and by Interviewer 1. The sessions were offered with an average interval of 1 month between sessions (range between 2 weeks and 3 months). All sessions lasted less than 1 hr. In one case, there was an extra session lasting less than 20 min with a family where one of the parents who had not been present at the previous family sessions also participated.The children completed a follow-up sandbox observation carried out by Psychologist A between 3 months and 18 months (mean time 11 months) after the third family session. The parents were interviewed by an independent interviewer (not part of the research team) designated here as Interviewer 2 about the parents’ evaluation of the symptoms of the index children using the same symptom scale used by Interviewer 1. Results from seven children are available (Table 1).
Evaluations of Sandboxes by Two Psychologists Before and After the Intervention With Symptom Rates Shown.
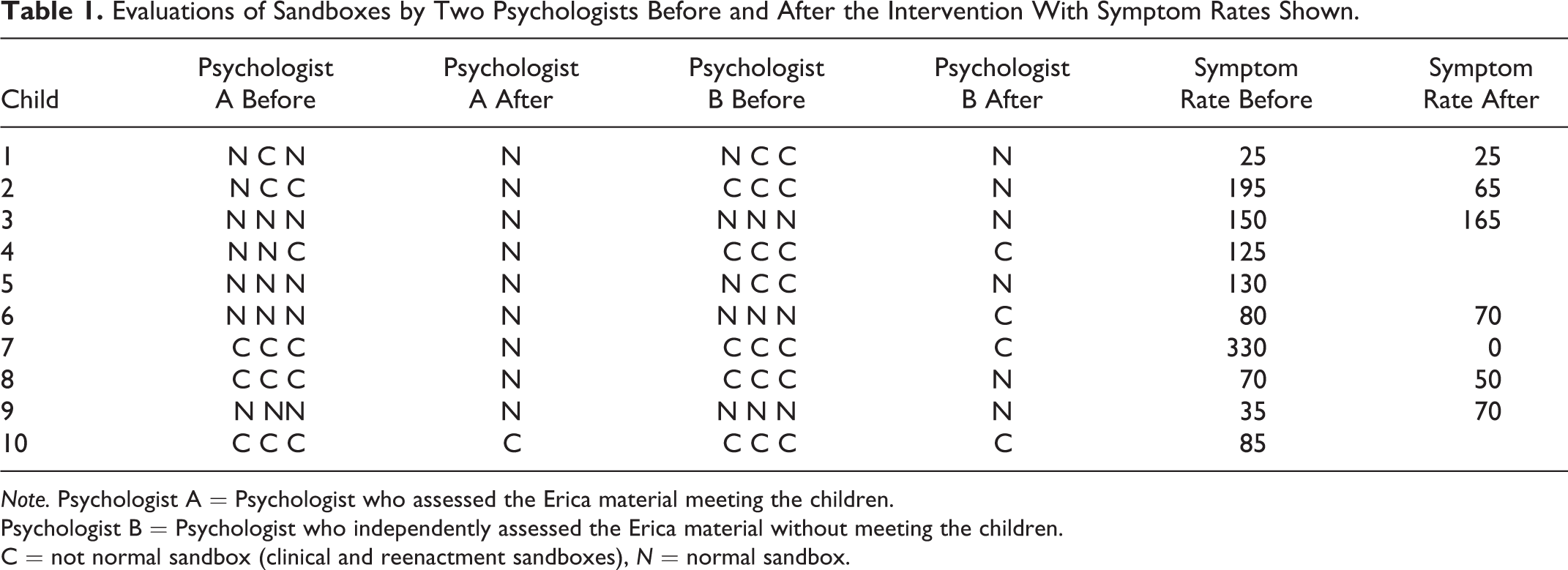
Note.Psychologist A = Psychologist who assessed the Erica material meeting the children.
Psychologist B = Psychologist who independently assessed the Erica material without meeting the children.
C = not normal sandbox (clinical and reenactment sandboxes), N = normal sandbox.
Instruments/Measures
The parents were asked about the symptoms of the index child. The Symptom Checklist (Cederblad & Höök, 1986) used was developed by McFarlane, Allen, and Honzik (1954) and revised by Jonsson and Kälvesten (1964). The parents were asked about the presence of 33 different symptoms including sleeping problems, somatic disturbances, anxiety, and aggressiveness in their children. Each symptom was scored as being normal or abnormal according to an operational scale. The cutoff score for having clinical symptoms is 300.
During the interview before the intervention, the parents were asked questions about their family composition, closeness to the war, and the nature of their escape from the war, religion, language, when leaving their home country and arrival in Sweden if the family members arrived together or separately, if the parents had told about the escape in advance, if they themselves had had traumatic experiences, symptoms of the children, if they had separated from persons close to them and what things the children had left in the home country. Of the total of 10 children, 9 in this study had been together with one or both parents during the war. Two children had not been in the war area.
Psychological diagnostics were done with the children according to the Erica method, which is both a play-diagnostic and a play-therapy method. This method has its roots in the World Technique, utilizing a standardized material (Lowenfeld, 1950). The Erica method uses similar methods and tools as in the World Technique of Lowenfeld, with the difference that it is using clearly distinguishable diagnostic and therapeutic applications (Mattson & Veldorale-Brogan, 2010).
In the study, Psychologist A, who had evaluated the Erica method before and after the intervention with family therapy, was blind to the background and symptoms of the children. The photographs of the sandboxes, the written notes about the activities of the children, and what the children said during the assessments were also assessed by independent Psychologist B, who was blind to the background and symptoms of the child, as well as to the order of the four sandboxes created by each child. The assessments made by the independent psychologist are less certain because the Erica method includes objective assessments in the sandboxes together with an assessment of the child acting during the play session where expressions and feelings are observed—assessments that cannot be fully written down in notes. Concerning the interrater reliability, the assessments of the psychologists were in accordance for 80% in the assessments before the intervention and 78% when all assessments are included. For first observations φ = .62, p < .026; second observations φ = .72, p < .009; third observations φ = .73, p < .008, and fourth observations φ = .41, p = .197. The assessments by the two psychologists differed for 9 of the 40 sandboxes; Psychologist B rated the nine sandboxes as not normal while Psychologist A rated them as normal.
If at least one sandbox of the series of three sandboxes was a “clinical world,” the child’s series was assessed as “not normal”. An index was created to include the Erica assessments from both psychologists, giving a value of “0” for a normal sandbox and “1” for a clinical sandbox. When their assessments differed, the value given was “0.5”; thus, a child could be given a rating of 0, 0.5, or 1.
The Erica play method was standardized by Olsson (2006). The Swedish nonclinical sample was used as a reference (R group) for the refugee children group (Björn, Bodén, Sydsjö, & Gustafsson, 2011).
Intervention
The study group received three sessions of family-based therapy where the index children participated together with their families including siblings. Themes in the family therapy sessions were the present situation, former life situation before the war, the escape from the home country from each family member’s point of view, role changes, network and thoughts of the future, and coping strategies in the family. The purpose of giving the family these sessions and going through these themes was to give everyone the possibility for being involved and to be able to share together experiences and thoughts with the aim of supporting the whole family. The intervention was influenced by systemic and narrative approach with crisis and salutogenic theory as the framework (Antonovsky, 1987; Cullberg, 1978; White & Epstein, 1990). Family members including siblings were involved in talking during the sessions. Small children were able to make drawings or play with toys in the same room if they wished to do so.
Both in the diagnostic interviews and family therapy sessions, an interpreter was used. Knowledge of the role of interpreter, as well as ethical and cultural awareness, is of great importance (Björn, 2005).
Statistical Method
Interrater reliability of the assessments of the sandboxes was calculated with φ-statistic. Comparisons of the situation before and after intervention were analyzed with Wilcoxon signed-rank test (two-tailed). All statistical tests were performed with SPSS-version 14.0.
Ethical Considerations
The ethical principles of autonomy, non-maleficence beneficence, and justice were considered. Concerning autonomy, the families had agreed to participate in the study and they knew they could interrupt their involvement at any time. One dilemma to consider was that talking about traumatic experiences could remind them about hard times and thus possibly worsen their present mental condition. On the other hand, there is a possible gain measured by taking into account the principle of beneficence. The goal was to help the family members to leave traumatic experiences behind and continue their life in a better way. The work with the family therapy sessions was done independent of race, gender, social, economic status, ethnicity, and so on. The study was approved by the Ethics committee of the University of Linköping (93092)
Results
Psychiatric Symptoms According to the Parental Interview
The majority of the children showed few if any overt psychological symptoms according to the data from parental interviews at baseline assessment (Table 1). One boy was judged on the basis of the data to have symptoms on a clinical level and one boy to have moderate symptoms.
The most common symptoms were aggressive symptoms and stomach problems. There was a tendency to show improvement (as seen in even lower symptom scores after intervention), but this tendency was not statistically significant.
Erica Method
Four of the 10 children in the intervention group had normal sandboxes in all three observations before the intervention. After the intervention, 9 of the 10 children built one normal sandbox. The change is significant even if counting the combined ratings p = .046 (Table 2).
Evaluations of Sandboxes by Two Psychologists Before and After the Intervention.
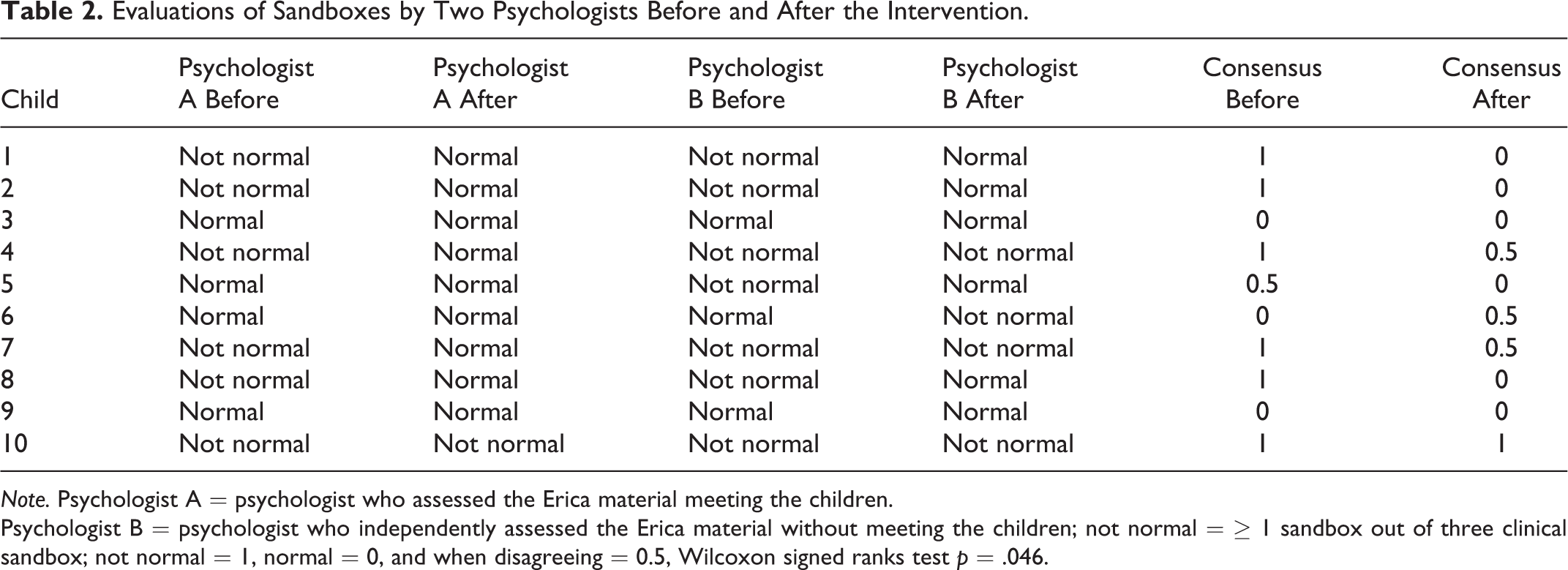
Note.Psychologist A = psychologist who assessed the Erica material meeting the children.
Psychologist B = psychologist who independently assessed the Erica material without meeting the children; not normal = ≥ 1 sandbox out of three clinical sandbox; not normal = 1, normal = 0, and when disagreeing = 0.5, Wilcoxon signed ranks test p = .046.
Analysis of Conflicts and Relations
Seven children shaped a conflict after the intervention. Before the intervention with family therapy, two children had shaped a conflict in Observation 1, four children in Observation 2, and four in Observation 3 (Table 3).
Shaping a Conflict and Shaping a Positive Relation in the Sandbox.
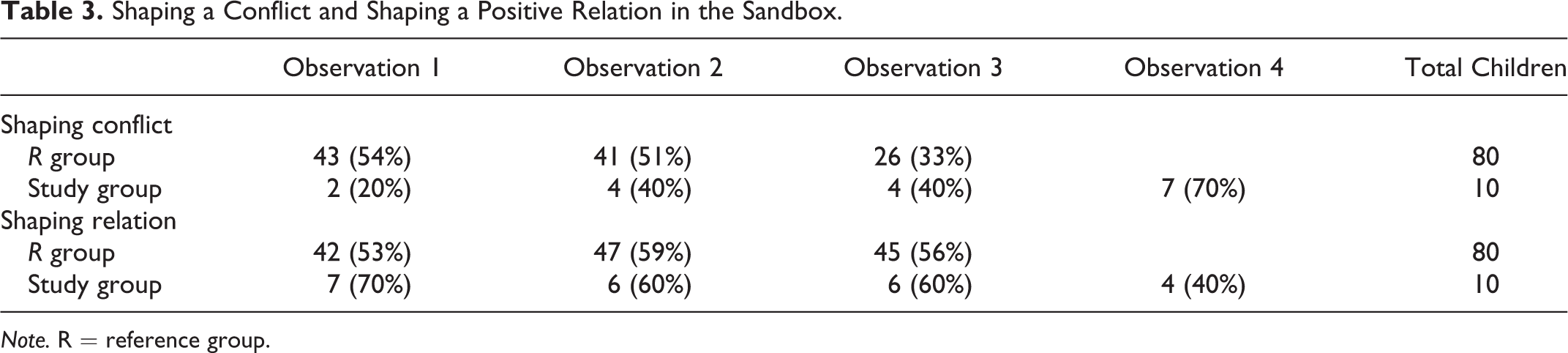
Note.R = reference group.
There were four children who shaped a positive relation after the intervention. Before the family therapy intervention, there were seven children who had shaped a positive relation in Observation 1, six children in Observation 2, and six in Observation 3 (Table 3).
In summary, the main results seen after the intervention are significantly more normal sandboxes than before, more conflicts, and fewer positive relations shaped in the sandboxes. There were no significant changes concerning symptoms evaluated by parents.
Discussion
In contrast to the results from the parental interviews, results from the children’s play in the Erica diagnostic setting pointed to the presence of psychological problems in some children. After short-term family therapy, there was an improvement in a majority of cases; before the intervention there was at least one not normal sandbox, but after the psychological assessments and the intervention there was one normal sandbox—a change indicating better psychological well-being.
Psychological projective methods are valuable in getting more information about thoughts and feelings, especially from younger children who are more difficult to interview than older children. We note this because several investigations of refugee children have been limited to older children who are easier to interview. One reason for using a projective method was to find out more information from children who might not provide this in an interview.
More children shaped a conflict during the sandbox diagnostic sessions after the intervention than before. One might infer from this that the children were no longer as reserved after the intervention as they had been before, so they could then allow themselves to act out conflicts more easily than had been possible before. There are refugee families who use silence and denial as a family survival strategy in dealing with previous traumatic experiences. The husband tries to protect his wife, the wife her husband, the parents their children, and the children their parents (Almqvist & Broberg, 1997). The family therapy sessions together with diagnostic sessions in the sandboxes may have challenged the use of denial as a family strategy and may have helped the children to become more open about their inner thoughts and feelings. There were fewer children who shaped a positive relation after the intervention than before, but the percentage that could create a positive relation was about the same as in the Swedish reference group (Olsson, 2006). One possible explanation that the children showed more positive relations before the intervention and in comparison to the Swedish reference group could be that by trying to keep together and not letting emotions take over, the children found it to be easier to show positive relations than to show conflicts.
The limitations in this study are that the sample is small and also that only the parents were interviewed concerning the symptoms of the children and not the children themselves. The lack of a control group is also a limitation. One objection to the results could be that Psychologist A made observations that were biased in some way. However, the results from the independent Psychologist B supported the finding that a greater percentage of the refugees created not normal sandboxes. Psychologist B also had higher percentages of assessments of not normal sandboxes than Psychologist A who made the observations. The representability of the sample might have been influenced by the recruitment procedure. In this study, we did not know the psychological health of the parents. Ajdukovic and Ajdukovic (1993) found that the emotional well-being of the mothers was the best predictor of the emotional well-being and adaptation in children. Since the children and their families had been in Sweden an average of 4 years, their experiences after arriving in Sweden could have influenced their psychological well-being. Another possible limitation is that the length of time between the family intervention and the follow-up sessions varied from family to family. Another limitation is that only one evaluation of sandboxes using the Erica method after the intervention with family therapy sessions was compared with three evaluations before the intervention.
Independent of the causes of traumatic experiences of these children, refugee children do constitute a risk group. The finding that there is sometimes a discrepancy between results from interviews with parents about their children and results from the assessments of the children (Björn et al., 2011) points to a need to focus on the child. This view is in accordance with the Convention on the Rights of the Child (United Nations General Assembly, 1989). Working with immigrant and refugee families challenges us to move beyond the cultural norms and imperatives that we take for granted, so that we can learn about the strength, resilience, and richness of families from other cultures (Mirkin, Kamya, McGoldrick, & Hardy, 2008). Carr (2009) has presented evidence from meta-analyses, systemic literature reviews and controlled trials indicating the effectiveness of systemic interventions for families of children and adolescents with various difficulties. Systemic interventions include both family therapy and other family-based approaches.
In this study, three sessions were offered, none of which lasted longer than 1 hr. To conclude, it might be valuable to offer all refugee families a few family therapy sessions and to focus in these sessions on common themes such as the family’s present situation, their life situation before the war, their escape from home country, role changes, and network and coping strategies in the family all with the aim of supporting them in the new country to which they came in their escape from a war situation.
Footnotes
Acknowledgments
The authors thank Elisabet Berg, social worker, for interviewing parents and for being the co-therapist in the family therapy sessions, Psychologist Anna-Karin Åkerman for the assessments of the Erica play diagnosis, IngBeth Larsson, PhD for interviewing parents after the intervention, and associate professor Ann-Charlotte Hermansson for valuable comments on the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the County Council of Östergötland and the Swedish Migration Board.