
Abstract
R.E.A.L. therapy is a novel approach that merges rational emotive and logotherapy techniques in a creative manner for families. This model teaches skills aimed at enhancing meaning and attachment in the family, building social literacy skills and personal insight through emotion recognition, and addressing negative thinking patterns through evidence testing. As traditional “talk therapy” may exclude young children from participating in family psychotherapy, the hands-on activities presented in this article may serve to engage the whole family in the therapy process.
R.E.A.L. therapy—rational emotive attachment–based logotherapy—is a novel approach for family therapy. It is holistic, targeting cognitions, emotions, family attachment, and meaning. Integral to R.E.A.L. therapy is family engagement in creative activities, as meaningful engagement promotes mental health and resilience to well-being concerns (L. L. Armstrong & Manion, 2013; Frankl, 1986). This article outlines the key tools and techniques, as well as a case study, for applying R.E.A.L. therapy to family-based treatment for child and youth mental illness.
Components and Rationale for R.E.A.L. Therapy
Logotherapy
Child and youth mental illness has increased 45% between 2006 and 2015 (Canadian Institutes of Health Information, 2015). Mental illness that begins before age 25 tends to be chronic, with substantial negative outcomes, including family difficulties or breakdown (Mental Health Commission of Canada, 2010). From a logotherapy perspective, these family difficulties—or challenges to a family’s sense of meaning—can emerge from the stress of having a child with mental illness (J. Lantz & Harper, 1992a). This existential meaning crisis is filled by the development of problems and symptoms—creating a family stress response that further compounds child and youth mental illness (Asarnow, Jaycox, & Tompson, 2001; J. Lantz & Harper, 1992b). In popular mental illness treatment models, the concept of “meaning” is often ignored in family therapy. Research has found that a meaningful life is vital for developing resilience to, or coping with, mental health concerns and suicidal thoughts (Frankl, 1986; Wong & Fry, 1998; Wong & L. Wong, 2006). Enhancing meaning in therapy is transformative in controlling symptoms and forming healthy, functional patterns of family interaction (J. E. Lantz, 1982).
Logotherapy, a meaning-based approach, encourages the inner spiritual resources of creativity, hope, the capacity for choice, and the making of responsible decisions in order to live a meaningful life (Frankl, 1986; Lukas 1986). A self-reported meaningful life for children includes the belief that one has influence over some things that happen in life, self-esteem, openness to new experiences, and hope for the future (Erikson, 1964; Markstrom & Kalmanir, 2001; Search Institute, 2009; VanderVen, 2008). In recent randomized control trials with students, logotherapy significantly enhanced meaning and purpose as well as significantly decreased symptoms of depression in comparison to control group participants (Robatmili et al., 2014).
Logotherapy was developed by Viktor Frankl, an Austrian psychiatrist, for suicidal adolescents and further refined based on his experience in concentration camps. Primary to logotherapy are the notions that people have the freedom to make choices under any circumstance and that, with choice, comes responsibility (Frankl, 1986). Another key tenet is that life has meaning under all circumstances and that each person must discover the meaning potential of each situation (Frankl, 1986). Logotherapy is therapy through meaning (Frankl, 1986). The goal of a logotherapy approach to family treatment is to help parents and children uncover, discover, and make use of meaning opportunities in family life (J. Lantz & Harper, 1992a). Children are generally able to experience fewer impediments in finding meaning than adults (J. E. Lantz, 1982).
Pathways to meaning include (1) creating a work or doing a deed (e.g., creating something for others, valued work), (2) experiencing something (e.g., engagement in valued activities, experiencing nature), (3) encountering someone (relationships with others), and (4) choosing our attitudes (thought changing). Tools to uncover meaning in logotherapy include dereflection, paradoxical intention, and Socratic dialogue. Dereflection involves directing a person’s attention away from the problem toward something engaging or valued. Dereflection is not meant to be “avoidance,” as avoidance is known to enhance symptoms. Rather, it involves using a helpful tool to step back from an emotionally overwhelming “cliff edge” to have the strength to face the important issue or thought pattern head-on. Dereflection is meant to help clients emotionally de-escalate, so that they are able to connect with the moment to address thinking that led to the cliff edge or connect with an experience that is perceived as meaningful. Paradoxical intention is the opposite of avoidance: exposure, but using a deliberate attempt to evoke humor. Logotherapists also use metaphors and storytelling, along with Socratic dialogue to stimulate critical thinking and to illuminate ideas.
Rational Emotive Therapy
Rational emotive (behavior) therapy (RET) is a primary complement of logotherapy (Hutchinson & Chapman, 2005). It is an active-directive, empirically based approach to psychotherapy developed by Albert Ellis (2004). The goal of RET is to enhance critical thinking and problem-solving skills, showing the family how the misinterpretation of events is causing problems. RET teaches more rational ways to interpret situations. Like logotherapy, in RET, people are responsible for their own well-being and the use of humor to overinflate concerns is a key teaching tool. The primary tenet of RET is that what we think leads to how we feel, and that feeling will last as long as we have irrational thoughts (for families with younger children, a more child-friendly way of phrasing “irrational thoughts” may be “stinky thoughts”). Anger, sadness, and fear mask the basic experience of pain and pleasure. Irrational beliefs underlying these feelings include (1) shoulds, (2) musts, and (3) awfulizing (catastrophic) thinking. Like in cognitive–behavioral approaches, such thinking is addressed scientifically through examining activating events, beliefs, consequences, disputes for “stinky” thoughts, and effects (on feelings and behaviors; see Table 1). RET is simpler than Beckian cognitive approaches, as family members only have to remember three types of irrational (stinky) thoughts in RET instead of numerous cognitive distortions. Attitude changing is also a component of logotherapy but is fairly unclear in the literature: A grafted RET approach provides a more replicable means of addressing problematic thinking in family therapy.
R.E.A.L. Therapy Thought Record.

Creativity and Attachment Building
Encouraging creativity, or being playful, in family therapy is a key ingredient in attachment building among family members (Creed & Kendall, 2005; Gil, 1994; Walter & Petr, 2006). Attachment injuries can occur through family difficulties adjusting to child illness or mental illness, damaging secure relationships (Cloutier, Manion, Walker, & Johnson, 2002). Play therapy provides opportunities for “mutual attunement,” which is central to the development or reestablishment of positive, secure attachments (Malchiodi & Crenshaw, 2014). When family members participate in, or listen to, arts-, story-, or play-based therapeutic activities together, thoughts and feelings are engaged in a hands-on, multisensory manner (Gil, 1994; Lowenstein & Sprunk, 2010). Deeper communication than in traditional talk-based therapy can be unlocked, as creative activities move therapy from the intellectual, cerebral world of adults to the world of imagination and creativity familiar to children (Bailey & Sori, 2000). Play is the language of children (Gil, 1994). Moreover, “talk” therapy can be limited with very young children due to their stage of language development, marginalizing them in family therapy (S.A. Armstrong & Simpson, 2002; Johnson & Thomas, 1999). Hands-on activities acknowledge the developmental levels of all family members and allow for even young children to actively participate in family therapy sessions (S. A. Armstrong & Simpson, 2002).
There is a body of research to suggest the benefits of a hands-on, artistically or technologically enhanced, multisensory, experiential learning approach (Malchiodi, 2005). In particular, a multisensory approach to therapy enhances authentic, effective dialogue because it taps into people’s different verbal, visual, or tactile learning and expressive strengths (Malchiodi, 2005). Whether through art, play, music, movement, enactment, or creative writing, incorporating creativity into therapy engages the whole person, affects the brain, and leads to better memory for therapy concepts, self-discovery, and change (Malchiodi, 2005). In R.E.A.L. therapy, RET and logotherapy activities are presented in a play, hands-on manner to enhance attachment and child engagement. R.E.A.L. therapy is, therefore, meant to foster family intimacy and interconnectedness through building antidotes to the three poisons of suffering: disconnection, meaninglessness, and the despairs of an irrational (stinky) thought process.
R.E.A.L. Therapy Tool Examples
Dereflection: Distraction Activity Game
As noted, dereflection is not meant to be a pathway to avoidance. One must step back from the cliff edge in order to examine it rationally, without overwhelming feelings getting in the way. Through dereflection, clients can de-escalate and ask themselves, “How am I right now?” they can notice the feelings as they happen and gain awareness of whether the situation is calling on them to make a choice: A choice for new, meaningful actions or new thinking that can help them stay away from the emotionally overwhelming cliff edge. A choice in response to the question, “Is this who I want to be in this moment?”
For the dereflection, distraction activity game, a therapist can choose any game that takes less than a minute to play. Therapists practicing a R.E.A.L. approach can use a card game like “snap” whereby clients say snap or slap a card in the center of the table when they see pairs as two cards are flipped. Once the deck of cards runs out, the player who has the most cards wins (the therapists makes sure the client wins). For this exercise, therapists have one member of the family volunteer to play with the therapist to avoid the possibility that some people may have a decrease in happiness if they were to lose the game against another family member. Prior to playing the game, the volunteer family member is instructed to think about a really bad day. When he or she is thinking about this bad day, the therapist gets him or her to rate feelings from 0 (feeling bad) to 10 (feeling good). Following this rating, we play the game. The client is asked to rate their feelings again after completing the game. Clients and observing family members are usually surprised at how feelings changed following the very brief game. In a R.E.A.L. therapy script, the therapist can say, Sometimes even doing very brief activities can make us feel a lot better. Sometimes these activities just make us feel a little bit better. Strong feelings are like standing at the edge of a cliff. When our toes are at the edge of a cliff, we can’t think clearly. These activities can be enough to calm us down a little bit and bring our toes away from the edge of the cliff so that we can think more clearly.
Dereflection: Pasta Dance
Humor is often a key element in healing (Frankl, 1986). When an entire family engages together in the pasta dance dereflection activity, it usually results in shared laughter. For homework, when feeling tense after a difficult day, family members practice the pasta dance together or use other dereflection exercises (e.g., diaphragmatic breathing—“belly balloon” breathing or imagery). R.E.A.L. therapists can use the following script and carry out the activity with the family to model the actions for them: Stand comfortably and imagine that you are a long piece of pasta. Hop into the pot of boiling water (everyone hops forward). Feel yourself bounce around in the boiling water, hopping around the pot. As you bounce around and begin to cook, notice yourself becoming softer (everyone dances around with their bodies becoming more and more relaxed). Softer. Softer. Finally, you’re cooked and you feel yourself gently falling down onto a plate (sit softly back in therapy chairs). You feel yourself let go entirely of the hardness in your soft, relaxed state.
Dereflection: Imagery
A therapist following a R.E.A.L. approach can have family members create a dereflection image to use when feeling tense. Specifically, therapists have family members collectively describe a relaxing scene or favorite family memory that uses all five senses, if possible. Scenes have included being on a beach, walking in a forest, driving in the country, petting a cat, lying under warm covers, and so on—whatever image is most relaxing or enjoyable for the particular family. Following the detailed description of their scene, if family members agree that they enjoy art, therapists then have them draw their dereflection image to use as a reminder cue before they practice using imagery. Between sessions, therapists can also create a personalized guided imagery audio recording for the family, using their words and their description of the scene. Clients have indicated that having the audio recording, at least initially, facilitates their ability to use imagery in order to cope with stressors or to calm down, until the use of imagery becomes more automatic. The recording and the drawing provide an activity that the family can practice together.
Paradoxical Intention: Fear Charades
Paradoxical intention is intended primarily for anxiety, insomnia, or sexual dysfunction (Frankl, 1986). Regarding fears, when family members attempt to avoid the things that they fear, the fears grow bigger. In paradoxical attention, clients try out the things they fear in an “over-the-top” manner to evoke humor. To provide initial exposure in session when family members experience many fears, and to begin decreasing the fears, family members can play “fear charades.” In session, family members acting out the things that they fear in a playful manner, while other family members guess the acted feared situation or object.
Metaphors Fostering Teaching, Learning, and Socratic Dialogue
The following metaphors are used to illustrate logotherapy concepts, foster Socratic dialogue, provide a visual demonstration, or highlight the relationship between RET irrational thoughts (stinky thoughts—shoulds, musts, and awfuling thinking) and feelings:
Pink elephant
The pink elephant exercise serves to teach clients why telling themselves such things as “not to worry about [x],” or “I must go to sleep,” or “I must not have this thought” are not helpful. It also demonstrates the value of dereflection or meaningful engagement. Before teaching clients dereflection, mindfulness, or distraction tools, a therapist taking a R.E.A.L. therapy approach can use the pink elephant exercise to explain the value of these tools in a creative, hands-on manner. More specifically, the therapists asks family members to visualize a pink elephant in the room. We agree on whether he is big or little, his ears are up or down, his trunk pointing is up or down, and whether his tail is long or short. Once we have agreed on his features, the therapist says, “I’d like you to see this pink elephant, really see the elephant. Can you see him?” (pause). “Now I’d like you to stop thinking about the pink elephant. Stop thinking about him ….. What are you thinking about?” The vast majority of the time, family members indicate that they are still thinking about the pink elephant. The therapist then goes on to say, “I’d like you to notice your feet on the floor, the hardness/softness of the chair beneath you, notice what your hands are doing, notice the colors of the walls around the room …” (pause). “What’s going on for you right now.” Clients typically respond that they are thinking about their chair and the room and are then asked what happened to the pink elephant. Clients smile and respond that he went away. Therefore, the therapist indicates that dereflection or other engaging distraction activities, rather than telling ourselves not to worry (etc.), can help turn our negative thoughts into background noise. For the rare client who stops thinking about the pink elephant when the therapist tells them to stop thinking about the pink elephant, the therapist can ask them what they are focused on. Generally, they are already using a preexisting good dereflection tool and the therapist can highlight this as a key strength.
Can’t touch this wall
The “can’t touch this wall” exercise may be helpful for clients who make the irrational deduction that thinking something will cause something to happen (e.g., if I think I will eat that food that I’m allergic to, when faced with it, I worry that I will end up eating it). For this exercise in family therapy, a therapist taking a R.E.A.L. approach might have clients stand about 1 m from a wall and say, “I can’t touch this wall.” The therapist can ask them to keep repeating I can’t touch this wall as they move closer and closer to the wall. Finally, even though they are saying, I can’t touch this wall, they find themselves touching the wall. The therapist then asks, “What just happened?” Clients indicate that they touched the wall. In response, the therapist can note, Even though you told yourself that you can’t touch the wall, you touched the wall. This shows us that we don’t have to act out on our thoughts. A thought is just a thought. We have a choice whether to listen to our thoughts or whether to choose a different action in response.
Left foot
In order to illustrate the connection between our thoughts and our feelings, for attitude changing/thought challenging, in a creative manner to engage clients, the left foot exercise can be used. The following is the left foot script: Imagine that I get up to go get my cup of coffee. As I’m going across the room, I step on your left foot. What do you feel? (Clients respond “pain” or oww”). How long do you think that feeling would last? (Clients typically respond, “a short time”). Now as I’m walking back across the room to my seat, I step on that same foot again. What do you feel? (Sometimes clients still say “pain,” other times they respond with an angry statement. Keep repeating this exercise until clients come out with an angry—or sad—response beyond pain). How long do you think that feeling would last? (When clients move from a pain response to an angry or sad response, they generally say that the feeling will last quite a bit longer). Isn’t it interesting. I did the same thing to you [X number of] times. The situation was the same, but you reacted differently the last time than you did the other time(s). You said (whatever the clients’ statements were). What’s causing you to feel different? It’s not the situation that’s different. I would suspect that the last time thoughts got in your head. As long as you have those thoughts, you’re going to continue to be (angry/sad). Those thoughts (e.g., she should have been more careful: anger/what did I do to deserve this: sadness) block the brief, short-lived, natural emotions of pain or joy in different situations. Our negative feelings of anger, sadness, or worry will last as long as we continue to have negative thoughts. If we can change our thinking, then we can change the way we feel. At certain times, we want to feel emotions such as grief following loss or fear in dangerous situations, but other times we want to be able to have control over our difficult feelings and we can do that by changing our thinking or our behaviors.
Ernie and Bert
In order to further highlight for families the relationship between thoughts, behaviors, and feelings, as well as to explore the fact that two people can feel differently in response to the same situation, therapists can use an Ernie and Bert story: Ernie and Bert both fail a math test at school. They both feel sad about failing. Shortly after getting the test results back, their friends invite them out to have cake and ice cream while watching a baseball game. Ernie agrees to go with his friends, despite feeling sad about failing. Bert doesn’t feel like going out, so he just heads home. At the end of the day, Ernie is feeling much better, since he had such a good time with his friends. He also has figured out where he went wrong on the math test and thinks about what he might be able to do in order to pass the next test. At the end of the day, Bert, who sat at home moping all day, is feeling even more miserable. He thinks that it’s the end of the world that he failed the test and that he’ll never graduate from school, and he will never get a job that he wants when he grows up. As you can see, both Ernie and Bert experienced the same negative situation, but they acted differently and they thought differently about it. Therefore, they felt differently at the end of the day.
Feeling Recognition: Enhancing Emotional Literacy
In the R.E.A.L. therapy model for families, emotions are helpful biological “alarm” bells. They alert clients as to whether they are having a helpful feeling (e.g., sadness in response to grief) or whether there is an irrational belief (a stinky thought), when a false alarm is going off. In order to change one’s thinking, a clear insight into one’s emotions, as well as the potential emotional experience of family members to build attachment, is necessary.
To enhance emotional literacy in family members and emotion language use, a therapist can create emotion cards. This game is a variation of “go fish.” The six basic global feelings are happy, sad, fear, anger, surprise, and disgust. In PowerPoint or Word, the therapist can create a deck of 36 cards. More specifically, set the slides or page size to 8.5 × 11 landscape and insert six 2 × 3 tables that fill six pages. Fill each of the tables with the six basic emotions, print the six pages and paste them onto card stock, and then cut out the 36 cards. The therapist can then deal four cards to each player including oneself. Pairs that people hold in their hands initially do not count as pairs—only count pairs if a card is received from another player. Players take turns asking each other such things as, “do you have sad?” If the other player has the requested card, then he gives one such card to the player who asked for the card. Upon receiving a matched pair of cards, the person names a situation in which they might feel that emotion and why. R.E.A.L. therapists may then ask the family what other emotion someone else might feel in that same situation and why. Whenever the therapist receives a matched pair, he or she could discuss a situation in which some people might feel that emotion, rather than self-disclosing. The family is still asked what other emotion someone else might feel in the same situation that was discussed by the therapist. To be more poignant, situations relevant to information already learned from the family may be helpful.
If someone asks for a card from another player who does not have such a card, the other player says go fish and the asking person must pick a card from the top of the draw pile of remaining cards. Pairs of cards are placed in front of the player who discusses them, removed from one’s hand. The game ends when either one person is out of all of their cards or when all but one player is out of all their cards, depending on how fast the game has progressed (therapist’s discretion). For homework, clients may be asked to each identify a feeling that they had, name the situation in which they had that feeling, suggest what led to that feeling, and note how and why someone else might feel differently in the same situation. Family members are asked to collaborate on this at-home exercise.
Challenging Stinky Thoughts: Crown of Thoughts
To carry out a thought record visually, family members can make paper crowns to wear. On colorful post-it notes, parents and children write down their stinky thoughts and then stick those post-it notes to their crowns on their heads. When wearing their thoughts, family members visually demonstrate the feelings that go along with those thoughts by making the facial expressions. They also walk around with the negative thought post-it notes and mumble aloud what their negative thoughts are. Following this, the family discusses what this was like for them to do this and to hear others’ negative thoughts. Stinky thoughts can then be challenged through evidence testing to derive a new, healthier way of thinking about the situation. The new, healthier thoughts can then be pasted to the crown, taking off the old thought. Family members subsequently make the feeling faces associated with these new thoughts that they are wearing and wander around saying these new thoughts aloud. Following a debrief with the family about this experience, all of these thoughts and feelings are written on a thought record (i.e., Table 1). For homework, each family member uses the thought record to write down a situation that triggers stinky thoughts and feelings. Parents and children work together to challenge those beliefs and derive, and write down, new healthier thoughts and feelings in those situations. If motivated, family members can continue to use their crowns at home for this exercise or simply use the thought record.
Problem Solving: Comics
To help family members problem solve, and to move clients from “stuck” situations, therapists following a R.E.A.L. approach can predraw stick figure comics relating to their current issues. The therapist can choose issues that are problematic patterns of behavior for the family. On blank faces and empty thought bubbles, family members are asked to draw their feelings and thoughts in relation to this situation (Where does this situation lead you?). Typically, they will draw their current sequence of thoughts, feelings, and behaviors that leads to a “stuck situation,” which can be enlightening for them. Following this, another copy of the same situation is presented and family members generate new, more helpful thoughts or statements, and therefore feelings, in this same situation or to problem solve a new way of behaving. Family members draw the new behavior in the blank panel provided (for an example, see Figure 1). For homework, clients can be sent home with additional simple comics produced by the therapist related to their present concerns in order to solve problems together.
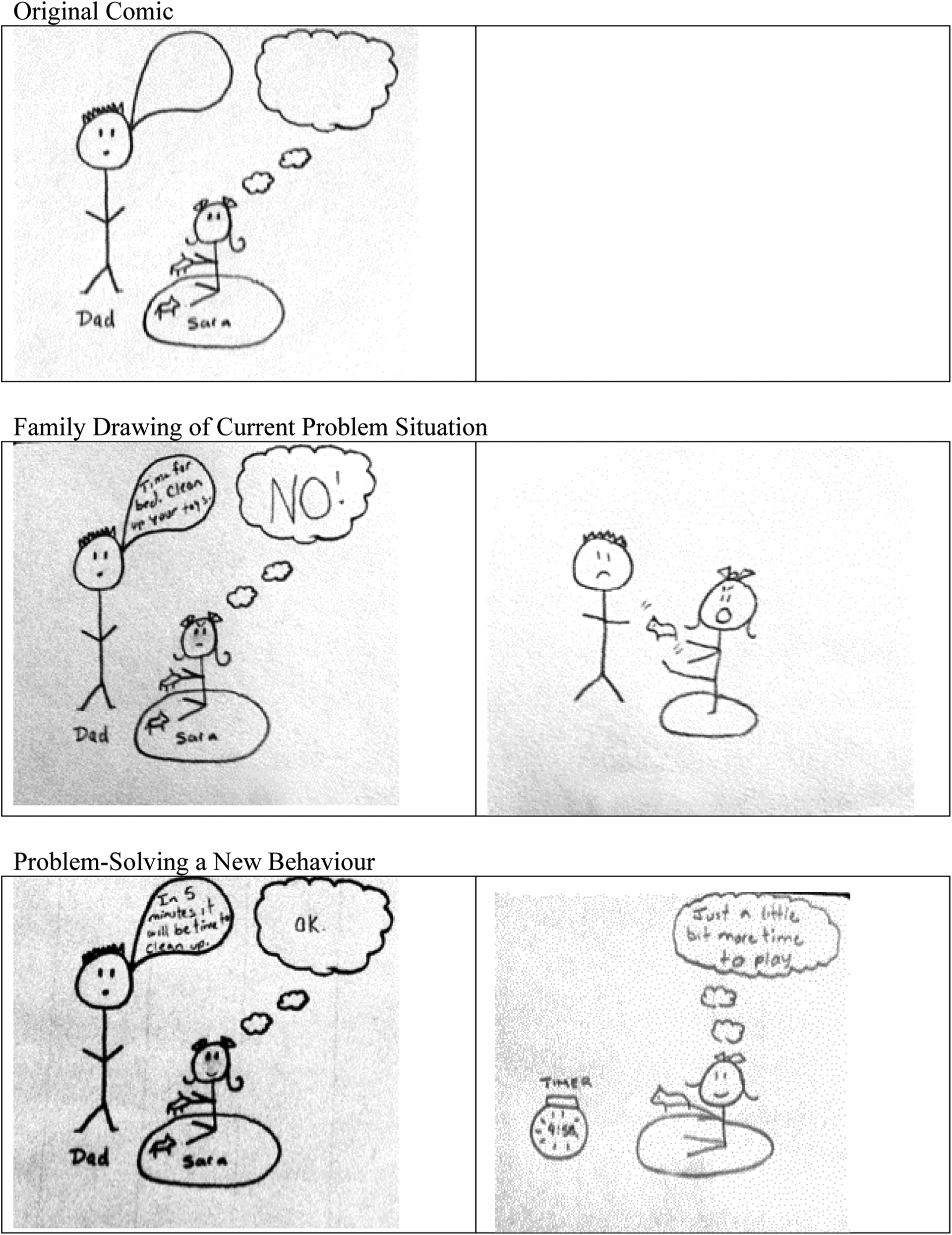
Problem-solving comics.
Relapse Prevention: Radio Show
To highlight all of the therapy tools used across R.E.A.L. therapy family sessions, R.E.A.L. therapists may use a hands-on way to test learning. More specifically, the therapist could set up a microphone and encrypted (password protected) computer to record the final session as a mock radio show. Free programs such as Audacity can be used to record on a Mac or Windows computer. During the session, the therapist pretends to be different “call-in listeners.” Family members are the “experts” who answer the call-in questions. When the therapist dramatizes call-in listeners’ questions, the family experts are asked about how to address issues that are the same as the issues that the family had faced. Family members describe new ways of thinking, acting, or other “tools” that were helpful for them. Following the recording, the therapist can make a copy for the family to keep and review if similar difficulties emerge in the future (e.g., by saving to a flash drive or burning to a CD).
Clinical Case
Amy, a 10-year-old girl, and Kyler, an 8-year-old boy, presented with their parents for family therapy. Amy was exhibiting symptoms of generalized anxiety, as was her mother, Jennifer. Amy was afraid of falling asleep in her own room and had been sleeping in her parents’ bedroom for several years. She also feared failure and would not try difficult homework. Most evenings, when given difficult homework, she would whine and raise her voice until her parents would complete the homework for her. At least once per week, Amy would cry and raise her voice until she was given her choice of family game or restaurant over other family members’ preferences. Amy had little awareness of others’ feelings and the impact of her behavior on their feelings.
Although Kyler did not meet full diagnostic criteria for obsessive-compulsive disorder, he exhibited a number of obsessions. For example, he would not drink out of a blue cup, as he feared contamination with germs, given that it was once left out with milk while on a family vacation. He washed his hands and bathed far longer than his parents thought reasonable (i.e., 4 min hand washing instead of the public health recommendation of washing as long as the “happy birthday” song duration), as he was concerned about cleanliness. These fears seemed to emerge following a misinterpretation or overinterpretation of a comment that his parents had made (e.g., “Make sure you use soap to get clean”).
Jennifer’s fears predominantly revolved around health or safety, primarily stemming from the time that she became permanently deaf in one ear as a child following an illness. In front of her children, she would “google” symptoms if anyone expressed a concern. Ben, the father, had successfully received previous treatment for alcoholism as well as symptoms of depression and anxiety. Prior to his own individual treatment, Ben indicated that he worked long hours and was relatively absent from his family. Over the past year, he had been trying to build closer relationships with his wife and children. He wanted to continue building a strong attachment relationship with his family as well as address their anxiety through a R.E.A.L. therapy approach: Enhancing meaning through giving, creating, experiencing with one another, and cultivating helpful attitudes.
Session 1 (Following the Intake Assessment Sessions): Full Family
– Storytelling highlighting the family’s values and positive experiences presented during intake to discuss “meaning strengths” to build upon during therapy.
– Introduction to the concepts of choice and responsibility: Discussion of emotions as “fire alarm bells” that tell us of a real threat or reasonable emotion (i.e., grief) versus alarms that highlight our need to choose responsible action; attending therapy in response to family distress is such a choice.
– Ernie and Bert metaphor was used to describe how two people can feel differently in the same situation to introduce emotional literacy concepts.
– Given difficulties with emotional literacy, and to develop emotional language, engage family in emotional literacy card game.
– Homework: Identify a feeling, name the situation in which they had that feeling, and suggest how and why someone else might feel differently in the same situation; family members were asked to collaborate.
Session 2: Full Family
– Reviewed homework.
– Pink elephant in the room metaphor used to teach about dereflection.
– Dereflection tool presented: Distraction activity game to help Amy de-escalate when feeling angry; also to help both children and Jennifer turn focus from anxiety-provoking thoughts to brief, meaningful pursuits; de-escalate to gain the strength to eventually be able to turn toward anxious thoughts, analyze them, and change them (when they learn the future tools).
– Homework: Try out dereflection activities discussed; rate feelings before and after.
Session 3: Full Family
– Reviewed homework.
– Left-foot metaphor to socialize the family to the connection between thoughts and feelings.
– Further discussion of emotions as “alarm bells”—biologically relevant or alerting us to shoulds, musts, or awfulizing thoughts; feelings alert us to a “meaning potential”: we can choose our attitude!
– Crown of thoughts activity to replace stinky thoughts with more helpful, rational thoughts; write on thought record.
– Carry out thought record homework collaboratively (activating event, belief, consequences, disputes for stinky thoughts, and effects on feelings and behaviors) using stinky thoughts experienced during the week.
Sessions 4, 5, and 6: Parents Alone
– Reviewed homework
– Socratic dialogue, psychoeducation, and problem-solving regarding “googling” and exhibiting other anxious behaviors around children, giving in to demands (homework and sleeping arrangements).
– Discussed meaning of deafness for Jennifer: She had been studying music at university when she lost her hearing in one ear; music became monophonic and lost its pleasure; devastating for her; pursued computer science instead; meaning: Jennifer would not have met her computer scientist husband if the illness resulting in deafness had not occurred. Old attitude: “This was the worst thing that ever happened to me as I cannot enjoy music anymore the way it used to move me.” New attitude: “Sometimes when a door closes, a window opens and good things can happen. Even illnesses that result in bad things can change a person’s life for the better in many other ways.”
– Thought records for health-related and safety fears (minimal concerns after new, meaningful attitude toward illness and deafness).
– Homework: Try the discussed new problem-solving strategies for child’s demands or exposure behaviors (e.g., rewarding “sleeping in own room,” “homework completion,” and “blue cup drinking” behaviors with tokens for shared activities with parents—such as choice of family game, choice of family television program for an evening).
Session 7: Full Family
– Reviewed homework
– Further dereflection strategies for anxiety: Pasta dance, imagery, and belly balloon breathing (diaphragmatic breathing).
– Fear charades for initial exposure to fears, humorous to reduce intensity of fears.
– Homework: Continue daily practice of dereflection strategies at home, use of dereflection when anxious, monitor effect on anxiety (before and after); use helpful, previously learned thought-changing and problem-solving strategies following decrease in anxiety after using dereflection.
Sessions 8–13: Individual Sessions With Each Child
– Reviewed homework
– Problem-solving comics to reach meaningful outcome rather than current negative outcomes (avoidance or impacting others negatively: Amy); comics and further crown of thought exercises also used for stinky versus helpful thoughts for anxiety-provoking situations (Kyler).
– Exposure homework, using dereflection tools to calm down before and during exposure; monitoring mood before and after exposure to fears.
Session 14: Parents Alone
– Assess progress; therapeutic goals met.
– Troubleshoot minor problems.
Session 15: Full Family
– Relapse-prevention radio show.
Outcome
Jennifer and Ben appeared to develop a meaningful, secure attachment relationship with their children. Amy became aware of her own and others’ feelings and was respectful of others’ needs. She expressed her feelings in a calm manner and no longer exhibited emotional outbursts at home. She was willing to try tricky homework and would ask her parents questions when stuck but would no longer ask them to do her homework for her. By the final session, Amy was sleeping in her own room, with the exception of a night that she was feeling ill. Kyler was able to use his dereflection activities and helpful thinking to address his fears. He was no longer worried about blue cups, lengthy washing, or other initial concerns. Although Jennifer still experienced some health-related anxiety when her children indicated unfamiliar symptoms, she no longer expressed these worries to her children. She also noted that her anxiety was significantly reduced from initial levels, as she reframed her own illness history in a meaningful, positive manner. Both Jennifer and Ben reported increased feelings of parental competence and problem-solving ability. They noted an enhanced sense of meaning in their life, due to improved parent–child relations. The family was also meaningfully engaged in activities collaboratively decided by all members, as demands by Amy were no longer present.
Implications
The list of activities and discussion tools presented here is not an exhaustive list of possible creative options to use in R.E.A.L. family therapy. The hope is that the reading of this article will stimulate further thought and creative applications integrated into rational emotive and logotherapy techniques for children.
Logotherapy, in particular, as well as creative structured play activities, is often discussed outside mainstream therapy literature. In comparison to other species, human lives are shaped by values, purpose, and the search for meaning. Outside of the logotherapy movement, Carl Rogers (1964) also recognized that distress occurs when there is a discrepancy between one’s values—that which one would find meaningful—and one’s current behavior. Reducing this discrepancy, living one’s values, minimizes distress (Rogers, 1964). Logotherapy goes one step beyond living one’s grand values to reframing even traumatic situations in helpful, meaningful ways and looking for small meaning potentials in everyday life (Frankl, 1986). Despite logotherapists’ and Rogers’ recognition about the importance of values or meaning, corresponding with the dearth in the research literature, mainstream treatment often continues to ignore meaning, resulting in a key gap in service delivery. R.E.A.L. therapy fills this gap and blends meaning with a mainstream, evidence-based approach. To date, a pilot study of a R.E.A.L. approach has been carried out through the D.R.E.A.M. program—Developing Resilience through Emotions, Attitudes, and Meaning (L. L. Armstrong, 2015). Using a R.E.A.L. approach for mental health education with young children, the D.R.E.A.M. program implements the majority of these activities in a classroom setting. Compared to a control group, these tools were found to significantly enhance meaning—hope, self-esteem, sense of agency, and openness to new experiences. More rigorous research and research with families in therapy settings has yet to be carried out, but current findings are promising. Moreover, participants indicated that the R.E.A.L. tools were highly engaging.
To germinate meaning recognition in a family, whereby even small children can recognize meaning, all members of the family system must be engaged (J. Lantz & Harper, 1992a). As traditional talk therapy approaches can exclude children in family therapy (S. A. Armstrong & Simpson, 2002; Johnson & Thomas, 1999), a creative approach—that also serves to build attachment—is “child friendly” to reach even the youngest members (Malchiodi & Crenshaw, 2014). In a fast-paced society, enhancing meaning through shared family activities inside and outside of the therapy office may ease the stress of family living (Fulkerson et al., 2006). Creative tools in therapy can, therefore, provide a model for such at-home, attachment-building parent–child activities. Shared creative family activities are one foundation for the development of meaning and purpose (Frankl, 1986). Therefore, it would seem that creative activities should regularly be incorporated into family therapy in order to fully meet client needs, better engage children who may feel excluded from therapy, and make the sessions meaningful.
The key goal of R.E.A.L. therapy with families, applying skills in meaning-enhancing, creative ways, is to develop the antidotes to the three poisons of suffering: Move from (1) disconnection to (re)attachment; (2) meaninglessness to fostering meaning by engaging families in activities that enhance creativity, experiencing, attitudinal change, and giving; and (3) irrational (stinky) thoughts to rational, healthy ways of thinking that do not cloud the experience of pain, pleasure, and meaning. Given the importance of values, meaning, engaging all family members, and addressing thinking, it seems critical for family therapy to begin incorporating and investigating the use of a R.E.A.L. approach: creative, meaningful, whole person, whole family.
Footnotes
Acknowledgment
I would like to acknowledge the past educators who inspired my use of creative activities in family therapy and who taught me some of these tools. In particular, I would like to thank Dr. Jane Ledingham, C. Psych., Dr. Ian Manion, C. Psych., Dr. Jean Grenier, C. Psych., Dr. Brian MacDonald, C. Psych., and Dr. Simon Davidson, M.D.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.