
Abstract
Empathy is directly related to one’s satisfaction with a romantic partner, and therefore, most approaches to couples therapy explicitly address empathy as a means for creating positive relational change. Imago relationship therapy (IRT) is practiced extensively worldwide yet lacks research validating its effectiveness. Given IRT’s focus on developing empathy within the members of the romantic partnership, it is important to examine how empathy contributes to change in relationship satisfaction. This random and controlled study examined the impact of 12 weeks of IRT treatment on individual (N = 60) empathy levels. Results showed a significant interaction between time and condition and found significant increases in treatment group empathy levels at each of three assessment points. These findings begin to emphasize the impact of IRT on couple empathy levels and highlight the potential benefits of using this particular therapeutic modality to promote positive relational change within romantic relationships. The research would have benefited from greater diversity within the sample and a greater understanding of the specific therapist interventions that impact client couple empathy levels.
The Impact of Imago Relationship Therapy on Empathy Levels
Research continues to show that caring and supportive relationships are directly linked to psychological and physical well-being. Those individuals experiencing more supportive relationships have better outcomes on measures of well-being, higher levels of life satisfaction, and lower rates of morbidity and mortality (Collins et al., 2014; Holt-Lunstad & Smith, 2012; Lakey & Orehek, 2011; Uchino, 2009). Essentially, caring and supportive relationships allow individuals to thrive on multiple levels (Feeney, Collins, Van Vleet, & Tomlinson, 2013).
While there is a wide range of approaches to couples therapy, a number of these approaches have been found to be empirically effective methods for strengthening relationship satisfaction and reducing relational distress as well as reducing individual psychological symptoms (Snyder, Castellani, & Whisman, 2006). Researchers have explored the effectiveness of emotion-focused couples therapy and behavioral couples therapy through a number of clinical trials, and they have observed significant reductions in relationship distress (Beach, Dreifuss, Franklin, Klamen, & Gabriel, 2008; Lebow, Chambers, Christensen, & Johnson, 2012). Recently, researchers have started to investigate interpersonal, cognitive-systemic, and communication-focused couples therapies and have found similar positive outcomes of increased satisfaction and decreased levels of distress (Snyder & Halford, 2012).
Empathy and empathic communication are essential elements of successful relationships. References to empathy and its importance can be found throughout the current research literature but rarely is it explicitly studied. How empathy is both given and received within a relationship is directly related to one’s satisfaction with a romantic partner (Cramer & Jowett, 2010). Dijkstra, Barelds, Groothof, and Van Bruggen (2014) have shown that higher levels of empathic communication enhance the partner bond and positively influence the continued development of healthy partner interactions. Therefore, most approaches to couples therapy address empathy as a means for creating positive relational change (Marmarosh, 2014); however, it also remains important to try to measure empathy.
The present study reviews one particular approach to couples therapy, imago relationship therapy (IRT; Hendrix, 1988/2008), and evaluates the impact that 12 sessions of IRT had on the empathy levels of participants. More than one thousand certified imago therapists are currently practicing in over 30 countries around the world (Imago Relationships International, n.d.). Although IRT is practiced extensively worldwide, there is a dearth of empirical research validating its effectiveness. Given that IRT devotes significant time and attention to the enhancement of empathy in the relationship (Muro, Holliman, & Luquet, 2015) and views empathy as the primary task of relationship work (Mason, 2005), it is both necessary and critical for IRT to be empirically evaluated.
Empathy and Couples Therapy
Empathy is defined as an emotional response of compassion caused by witnessing someone else in need. Often this response is identical or similar to the feelings of the observed individual (Dijkstra et al., 2014; Stocks, Lishner, Waits, & Downum, 2011). Empathy also involves considering the viewpoint of another by thinking about his or her motives (Hawk et al., 2013). Unlike sympathy, empathy involves sensitivity to the extent of situations as well as the ability to read nonverbal cues about another’s emotions and communicate feelings of care (Underwood, 2002). Despite the long-held view of empathy as solely an affective response, research has demonstrated that empathy includes both affective and cognitive elements (de Kemp, Overbeek, de Wied, Engels, & Scholte, 2007). We define empathy as an affective response to another that involves the regulation of emotion and the cognitive capacity to understand the perspective of another (Decety & Jackson, 2006).
While empathy may be experienced in varying circumstances and with different individuals, when experienced within a romantic relationship, it plays a critical role. Empathy aids in the development and preservation of pair bonds, being that it forms a key element of emotional support and is therefore a correlate of relational satisfaction (Cramer & Jowett, 2010; Dijkstra et al., 2014; Rostowski, 2009). Higher levels of empathy are related to multiple aspects of positive relationship building between romantic couples (Perrone-McGovern et al., 2014). On the other hand, responses that lack empathy relate to increased tension and conflict in the relationship (Carrère, Buehlman, Gottman, Coan, & Ruckstuhl, 2000). Enhancing empathy within a relationship is a developmental process as well as a practice in discovery. This relational progression involves a willingness to embrace our negative emotions that are often closely connected to our relational wounds. The more conscious we are of our personal emotions, the better we are at understanding and responding to the emotions of our partner (Hill, 2010).
A practitioner’s particular therapeutic goals will vary depending on his or her theoretical orientation and the presenting problems of the client dyad. While teaching and encouraging empathy between the couple, the therapist must sustain empathic attention in order to create the necessary safe environment (Livingston, 2009; Marmarosh, 2014). Considering this, it is understandable that almost all couples therapy approaches prioritize empathy development: cognitive–behavioral treatment (Patterson, 2005), behavioral approaches (Jacobson & Margolin, 1979), object relational perspectives (Bagnini, 2012; McCormack, 2000; Scharff & Scharff, 1991; Siegel, 1992), self-psychological approaches (Leone, 2008; Livingston, 1995; Solomon, 1985), and attachment-focused treatment (Johnson & Whiffen, 1999). The emotion-focused therapy (EFT) approach and Gottman’s approach are two of the most widely known and utilized forms of couples therapy alongside IRT. Both of these approaches have developed a strong research base and have shown to be effective with multiple populations and multiple presenting issues (Greenberg, 2010; Gottman & Gottman, 2008). While there are many similarities between these approaches and IRT, IRT is unique in its explicit focus on empathy between partners. The Gottman method and EFT in particular pay close attention to and emphasize the importance of the therapist being empathic (empathic attunement) and creating an environment of safety and acceptance, and IRT therapists work to encourage the partners in the couple to develop this level of empathic communication with one another (Holliman, Muro, & Luquet, 2016).
Imago Relationship Therapy (IRT)
IRT (Hendrix, 1988/2008) is a theoretical and applied methodology for working with couples in committed relationships (Martin & Bielawski, 2011). The theory integrates psychodynamic approaches (e.g., ego psychology, attachment theory, and object relations psychology), transactional analysis, and cognitive–behavioral approaches and contends that unconscious factors play a significant role in the selection of a partner (Zielinski, 1999). IRT theorizes that unconscious partner selection creates an opportunity to heal a connection that was lost in childhood by increasing empathy, understanding, and communication (Love & Shulkin, 2001). Imago therapists actively teach and help couples apply specific empathy-building skills through a number of explicit exercises (e.g., the couples dialogue, the imago work-up, the parent–child dialogue and holding exercise, behavior change request dialogue, caring behaviors; see Imago Relationships International, 2014, for more detail). Mason (2005) has stated that “IRT has made empathy the central task of relationship work” (p. 150).
Only a few nonrandomized, noncontrolled research studies have been conducted that lend support to IRT as a beneficial treatment methodology (Hannah, Luquet, & McCormick, 1997; Hannah et al., 1997; Luquet & Hannah, 1996). These studies attempted to evaluate participant well-being and marital satisfaction over time, but no research to date has included a control group, a randomized sample, or measurement of change in empathy levels. Additionally, none of these studies measured IRT over more than 6 sessions despite the average number of sessions for couples therapy being 11.5 (Doherty & Simmons, 1996). Despite these weaknesses in study design and lack of robust measurement tools, the research does give some indication of treatment benefits. Considering the widespread practice of IRT around the world and its fundamental emphasis on the enhancement of empathy in couples therapy (Muro et al., 2015), robust research studies of the practice of IRT and its impact on client empathy levels are imperative.
The Present Study
Using experimental design, the present study examined the impact of 12 sessions of IRT treatment on empathy levels of couples experiencing relational distress. We hypothesized that the treatment group would achieve significantly higher levels of empathy over the course of their 12 sessions of IRT, whereas the control group would not show significant changes in empathy. Additionally, we hypothesized that the treatment group would show a clinically significant increase in empathy scores.
Method
Participants
The research team solicited participants specifically interested in relationship counseling through postings on professional and community listservs. These treatment-seeking couples were provided with a web link that led to a description of the study and allowed them to review the inclusion criteria and initiate the screening process. To participate in the study, at least one member of each couple needed to score in the distressed range (i.e., mean less than 100) on the marital adjustment test (Locke & Wallace, 1959) and be living together for at least 1 year. Individuals were not included if they had received psychiatric or psychological treatment in the past 2 years, had any current problems with alcohol or drug use, were incarcerated, had any current concerns of domestic abuse, or had any immediate plans to terminate the relationship. If eligible, couples were randomly assigned to the treatment or control group using an online random number generator.
One of the 19 couples initially enrolled in the control group withdrew from the study prior to the first assessment and two others did not complete the final assessments. Two of the 18 couples in the treatment group dropped out during the course of the study. The first stopped attending counseling sessions, and the other couple did not complete the final assessments. Therefore, the control group consisted of 16 couples (n = 32) and the treatment group consisted of 14 couples (n = 28). Participants who did not meet the inclusion criteria were notified of their status and referred to appropriate psychological services when necessary (e.g., when they reported active domestic abuse) or requested by the prospective participant.
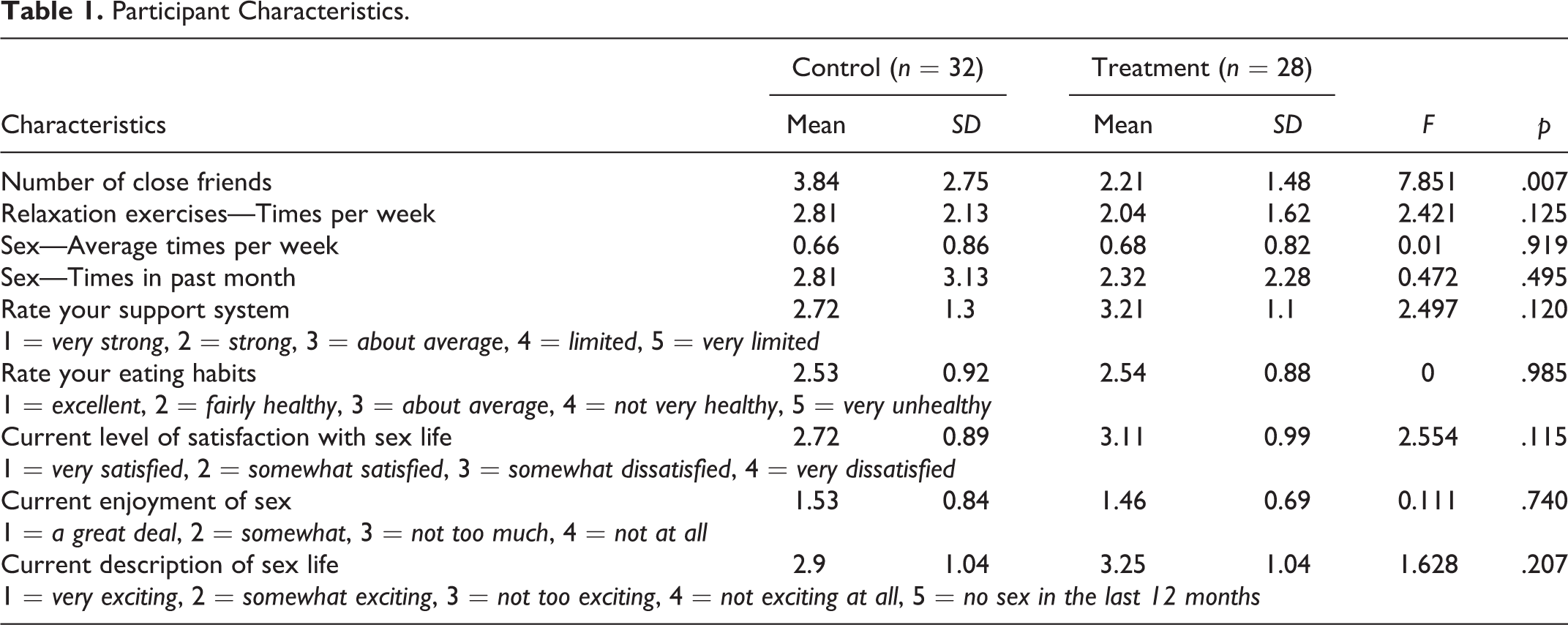
The majority of participants (64%) were in the 30- to 50-year-old range and the mean age for the sample was 45 years. The vast majority of participants were Caucasian (81%) and African American (17%), and individuals of Asian descent (2%) were represented to a lesser extent. Many of the couples (30%) had been together for 5–10 years prior to the research study, and the length of the participant relationships ranged from 2–45 years. The sample was highly educated with only 5% not having completed any college credits; 37% of the sample finished graduate or professional degree programs. Seventeen percent of the sample reported household income between 0 and 59,000; another 30% reported income between 60,000 and 100,000. An additional 41% of participants reported having income between 100,000 and 199,000 and a final 12% reported income over 200,000. Thirty percent of the participants had engaged in couple therapy during the past 5 years, and 22% had engaged in either individual or group therapy. With regard to religion, most participants identified as Christian (52.5%), two individuals as Jewish (3.4%), and the remaining participants (44.1%) listed themselves in the following categories: spiritual but not religious (25.4%), nonreligious/secular (6.8%), Atheist (5.1%), and Agnostic (6.8%). Beyond the traditional demographic data, the initial questionnaire also included seeking information about participants’ previous involvement in therapy, sexual satisfaction levels, and individual wellness practices (e.g., support systems, stress management, nutrition, etc.). See Table 1 for an overview of additional participant responses.
Participant Characteristics.
Procedures
Couples in the treatment group were assigned to an imago therapist in their geographical area and made a commitment to complete twelve 90-min treatment sessions at no cost to the clients. Couples were given 18 weeks to complete the 12 sessions; however, the time between sessions could not exceed 2 weeks. The therapists were all licensed in their respective fields (e.g., counseling, social work, and psychology) and had achieved the highest levels of IRT training and certification. They each videotaped all sessions and completed a brief checklist after each session to indicate the particular IRT interventions that were utilized during that meeting. Treatment integrity was determined through a process of reactive observation (Bernard, 2012) by a team of expert imago therapists. Along with one of the researchers, this group of therapists developed a scoring method and worked through a number of iterations of this method in an effort to increase interrater reliability prior to it being put to use.
The control group engaged in a 12-week bibliotherapy exercise and was assessed on the same schedule as participants in the intervention group. At the end of the study, these participants were offered free admission to a Getting the Love You Want Workshop in their geographic area. This intensive, 2-day couples relationship education session has been shown to promote short-term, positive communication behaviors as well as marital satisfaction (Schmidt, Luquet, & Gehlert, 2016). Both control and treatment participants completed assessment measures at the beginning (T 1), middle (T 2), and end (T 3) of their participation.
Measures
The interpersonal reactivity index (IRI; Davis, 1980, 1983, 1996) assesses dispositional empathy in social situations and is the most widely researched and multidimensional assessment of empathy available (Cliffordson, 2002; Nomura & Akai, 2012). The IRI is unique in that it assesses both the cognitive and affective aspects of empathy. The instrument contains the four orthogonal 7-item subscales of Perspective Taking (PT), Empathic Concern (EC), Personal Distress (PD), and Fantasy (FS). The IRI is a self-report instrument scored on a Likert-type scale ranging from 0 (doesn’t describe me at all) to 4 (describes me very well). PT represents the everyday tendency to adopt the psychological viewpoint of others (e.g., “I sometimes try to understand my friends better by imagining how things look from their perspective”). The EC subscale measures the propensity to experience sympathy and compassion for those who are less fortunate (e.g., “I often have tender, concerned feelings for people less fortunate than me”). The PD subscale assesses the tendency to experience distress and discomfort in response to extreme distress in others (e.g., “Being in a tense emotional situation scares me”). The FS subscale measures the propensity to imagine oneself in fictional situations (e.g., “When I am reading an interesting story or novel, I imagine how I would feel if the events in the story were happening to me”). Utilizing a normative sample, internal consistency reliabilities of the four subscales ranged from .70 to .82 (Davis, 1980; Pulos, Elison, & Lennon, 2004). Test–retest reliabilities ranged from .62 to .71 over a 2-month period (Davis, 1980).
The subscales of the IRI were originally evaluated individually and particular importance was placed on the PT and EC subscales because they were hypothesized to reflect the most advanced levels of empathy. Over time, however, researchers have utilized combinations of subscales in order to evaluate more complex aspects of empathy. For instance, because the PT and EC subscales are the most representative of multidimensional empathy in mature adults (including both the cognitive and affective elements), these are often combined when evaluating adults in order to achieve a total empathy score (Greason & Cashwell, 2009).
Others have argued that the IRI subscales contribute differentially to the construct of empathy with EC as the primary affective component, which is supported by cognitive components captured by PT and FS (Cliffordson, 2001, 2002; Fernández, Dufey, & Kramp, 2015; Hawk et al., 2013; Pulos et al., 2004). Pulos, Elison, and Lennon (2004) utilized a Schmid–Leiman orthogonalization and did not find any relationship between the PD items and the general empathy factor. This provided further support for the idea that empathy and PD are separate constructs (Eisenberg & Fabes, 1998; Lennon & Eisenberg, 1987). Therefore, Pulos et al. (2004) argued that the summing of the EC, PT, and FS subscales captured a second-order factor structure that corresponds directly to the more traditional notion of empathy. In the present study, we utilized this approach in quantifying empathy for our analyses.
Results
PT (α = .85), EC (α = .83), and FS (α = .76) subscales were combined into a total empathy score (α = .87) that was used for all analyses. Mean scores for the control and experimental groups at all three time points are given in Table 2. First, a repeated measures multivariate analysis of variance (MANOVA) was performed on the total empathy score for each participant group. This analysis showed that there was a significant interaction between time and condition, F(2, 116) = 4.95, p < .01; Wilks’ Λ = .95, and partial η2 = .044. Paired samples t-tests showed that the treatment group made significant increases from T
1 (
Individual Mean and SD Empathy Values.

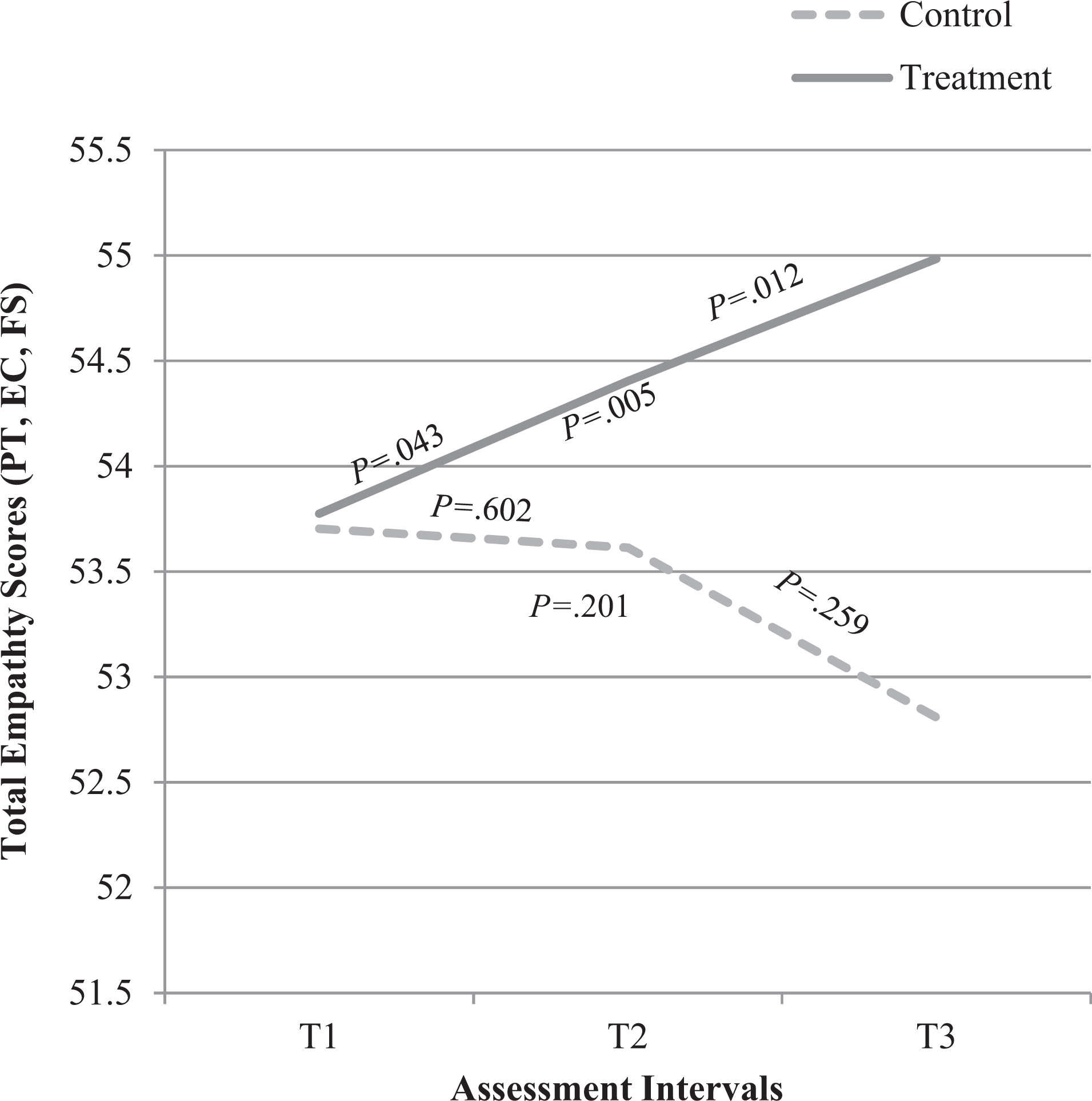
Empathy over time.
We next sought to test our hypothesis regarding clinically significant change. Clinical significance describes whether or not the treatment effect has a noticeable practical impact on the participants (i.e., change from a mean score in the abnormal range to one within the normal range). Jacobson and Truax (1991) describe three methods for evaluating clinical significance, two of which require the use of mean score data from a functional (i.e., healthy) population. Because data from functional individuals are not available for the IRI, we utilized Jacobson and Truax’s method that does not require those data. In this approach, an individual is understood to experience clinically significant change when their posttreatment score falls “outside the range of the dysfunctional population, where range is defined as extending to two standard deviations beyond (in the direction of functionality) the mean for that population” (p. 13). The mean IRI score for females is 58.38 (SD = 4.65), and therefore, the “functional” range is from 49.08 to 67.68. For males, the mean IRI total score is 51.55, and therefore, the functional range is from 41.87 to 61.23. At Time 1, both the male and female mean scores from this sample fell within this functional range. Hence, we were unable to test this hypothesis because our participants entered the study with functional levels of empathy that could not be improved from a clinical perspective.
Considering the differences in IRI scores between genders at T
1 (females:
A Pearson product-moment correlation coefficient was computed to assess the relationship between participant empathy scores and all items from the background questionnaire. There was a correlation between empathy scores and participant spirituality/religion responses (r = .302, n = 59, p = .02). When analyzed by gender, there was a correlation between male empathy scores and times per week practicing relaxation techniques (r = .389, n = 30, p = .034) and sexual enjoyment (r = .424, n = 30, p = .019). There was also a correlation between female empathy scores and spirituality/religion responses (r = .441, n = 29, p = .017). There was no correlation between empathy scores and marital satisfaction (r = .101, n = 60, p = .444).
Discussion
This study is focused specifically on empathy development; however, we also know that this course of IRT also has a significant positive impact on relational satisfaction as measured by the marital adjustment test (Gehlert, Schmidt, Giegerich, & Luquet, 2016). The most important findings from this study were that a course of 12 sessions of IRT with a highly trained imago therapist has the potential to make a statistically significant and positive impact on an individual’s empathy. Participants in the treatment group showed a steady increase in their empathy scores over the course of treatment, making significant progress at each assessment point. These results indicate that the focus on empathy in couples counseling, and in IRT in particular, does affect the individual in important ways that are in addition to empirically proven increases in marital satisfaction. When analyzed by gender, we found that the treatment had a greater impact on male total empathy scores than female scores.
While the sample showed significant improvement in empathy, that improvement does not appear to be reflective of clinically significant change due to the fact that the participants’ empathy scores were in the functional range at the beginning of treatment. The fact that participant empathy levels were in the normal range likely minimized the potential for greater advancement in empathy scores. Additionally, it has been argued that empathy is a rather stable personality trait; therefore, it is difficult to modify without multilayered interventions (Quince, Parker, Wood, & Benson, 2011). While the 12 sessions of IRT were helpful to these couples, additional treatment could have enhanced the gains experienced by participants.
With regard to available data on the IRI, we do not know how an increase in empathy will impact one’s functioning in life or with his or her romantic partner. Further understanding of how an increase or decrease in empathy scores impacts behavior would help both practitioners and researchers in their work. Additionally, the IRI measures empathy at the level of individual functioning (i.e., empathic tendencies in a general social context) and not in a relational context. The IRI for couples (IRI-C; Péloquin & Lafontaine, 2010) is an adapted version of the IRI that seeks to specifically assess empathy expressed within a romantic relationship. We did not use the IRI-C in the present study because it was relatively new and untested at the commencement of our research. Future researchers should consider using this instrument, as it may better assess the impact of empathy-focused interventions on romantic relationships.
Researchers focused on empathy in couples therapy, and IRT in particular, might benefit from further refining their empirical approach toward enhancing empathy. Such refinement would include the specific types of empathy that treatment assumes to impact and the explicit interventions meant to influence those types of empathy. For instance, IRT has a number of precise intervention techniques that are taught and practiced with couples. The effect that one intervention has over another regarding empathy development, however, cannot be known unless interventions are more precisely examined. A research study focused on a particular set of techniques could help identify the specific impacts that such techniques and interventions have on client empathy scores.
There are important limitations to this study that should be considered. First, while the sample size in this research was average for couples research, there was a lack of diverse representation of individuals, making it challenging to try and generalize to non-Caucasians. Second, as alluded to above, it would be helpful in future studies to have a more specific means for evaluating the types of interventions utilized by the therapists during each session. This information would allow the researchers to evaluate those couples that focused a great deal on empathy development and, therefore, should show greater gains in empathy scores. Additionally, the researchers did not screen for participant empathy in order to evaluate pretreatment functional/dysfunctional levels; this would have enabled the researchers to evaluate clinical change. Lastly, this research lacked posttreatment follow-up data that could shed light on the long-term impact of the changes that were made.
Given the need for an expanded body of research exploring the efficacy of IRT as a form of couples therapy, this research serves to establish a necessary path toward further empirical investigations of this approach. It is, of course, vital that future investigators seek to replicate this research with more diverse sample populations and a variety of therapists. The findings reported in this study, however, give credence to the impact of IRT on participant empathy levels and begin to shed light on the potential benefits of using this approach to promote positive relational change within romantic relationships.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.