
Abstract
Many clients drop out of therapy before reaching their goals; and research has yet to develop a thorough understanding of the factors that lead to dropout. Some have suggested that experiencing therapy as helpful or productive is key to therapy persistence. A small body of qualitative research has investigated client perspectives about things that happen during therapy sessions to produce change or therapy productiveness. The present study describes the process of developing and refining an instrument used to measure client perception of therapy productiveness in a sample of participants seeking therapy with a marriage and family therapist. Seventy-two participants engaged in therapy and completed the Productive Processes Inventory (PPI). Procedures used to establish reliability and validity are presented and discussed. Results of a principle components analysis revealed three factors. Results support the potential usefulness of the PPI as a measure of therapy productiveness.
Clients often drop out of therapy before reaching their goals (Bohart & Wade, 2013), while relational clients are particularly vulnerable to premature dropout (Hamilton, Moore, Crane, & Payne, 2011; Masi, Miller, & Olson, 2003). Clients who end treatment prematurely are less likely to experience therapy benefits and more likely to report dissatisfaction with treatment (Hamilton et al., 2011; Pekarik & Wierzbicki, 1986). Little is known about the in-session therapy processes that contribute to treatment persistence (Marchionda & Slesnick, 2013). The marriage and family therapist (MFT) field has yet to develop a thorough understanding of what makes therapy feel effective to clients (Davis & Piercy, 2007a, 2007b; Pinsof & Wynne, 2000), such that they persist in therapy. A small body of research on change processes or the in-session, emotional processes that clients identify as helping to produce change (Greenberg, James, & Conry, 1988, p. 6) has contributed to the explanation of how change occurs through the therapeutic process (Blow et al., 2009; Christensen, Russell, Miller, & Peterson, 1998; Helmeke & Sprenkle, 2000; Wark, 1994).
There have been four qualitative studies investigating clients’ perceptions of helpful change processes in couple and family therapy (Blow et al., 2009; Christensen et al., 1998; Helmeke & Sprenkle, 2000; Wark, 1994). In each of these studies, couple and family therapy clients were asked to describe the events that occurred in therapy sessions that they believe were most important in helping them change. Wark (1994) investigated clients’ accounts of the most critical events of therapy associated with change using critical incident technique. In a sample of five couples and five therapists, she found that clients’ positive views of therapy were associated with the therapists’ ability to provide routine and structure, ability to offer alternative perspectives, assume a directive or nondirective style when needed, and ability to focus on positives (Wark, 1994). Most notably, Wark’s (1994) findings are focused on therapeutic alliance variables and the therapists’ actions.
Christensen, Russell, Miller, and Peterson (1998) were influenced by Wark’s (1994) research of critical change incidents over the course of therapy and designed a qualitative investigation of 24 couple therapy clients and 9 therapists aimed to understand turning points over the course of therapy that left them thinking or feeling differently about the presenting problem. In contrast to Wark (1994), Christensen and colleagues’ (1998) study does not assume that therapeutic change occurs in few noteworthy events, rather change is assumed to occur as a subtle gradual process, sometimes even without significant markers. Christensen and colleagues found changes occurred in cognition, affect, and communication patterns. Five contextual factors, namely, safety, fairness, normalization, hope, and pacing, contributed to this perceived change. Similar to Wark’s (1994) findings, Christensen and colleagues’ (1998) findings related to what happened in therapy that brought about change are inextricably linked to things the therapist did to facilitate changes in cognition, affect, and communication.
Helmeke and Sprenkle (2000) were influenced by Wark’s (1994) and Christensen and colleagues’ (1998) studies of change processes and aimed to focus on specific change processes they called pivotal moments, as opposed to more general aspects of therapeutic change. Helmeke and Sprenkle (2000) asked three couples (six clients) and one therapist to identify pivotal moments in their therapy. Partners of different genders, therapists, and clients often identified different events as pivotal. Consistent with Wark’s (1994) and Christensen and colleagues’ (1998) findings, Helmeke and Sprenkle (2000) found support for things the therapist did that were identified as allowing a pivotal moment to occur. Pivotal moments were found to occur around discussions of the presenting problem and occur after a topic had been discussed repeatedly in sessions (repetition). Other findings related to pivotal moments were centered upon things that the therapist did to facilitate such moments, including use of illustration or metaphor, therapist characteristics, use of practical suggestions, positive reinforcement, willingness to offer alternative solutions, ability to be in tune with the moment, and ability to foster client trust (Helmeke & Sprenkle, 2000). Findings of this study and preceding studies continually find that the therapist is inextricably linked to change processes.
Although methodologically and conceptually rigorous, the small body of research of change processes has not been replicated in several years, warranting new research aimed to continue and expand this research. A notable limitation of these qualitative studies is that they do not identify an outcome that is impacted by these change processes and the importance of this research is not clear to its consumers (Greenberg & Pinsof, 1986; Helmeke & Sprenkle, 2000). One way to expand on change processes research is to clarify the language used to identify those processes and to establish their contribution to successful therapy outcomes.
While studies use terms such as “helpful,” “critical,” and “pivotal” interchangeably, we propose that productive may be a more accurate and specific way to identify and describe these processes. Productive is defined as giving rise to a significant event or result (10th ed.; Merriam-Webster’s Collegiate Dictionary, 1993). Change processes can be defined as productive when they are identified as the process (the event, behavior, cognition, or action) that contributed to moving toward the therapeutic goal. This conceptualization of productive change processes is more specific than helpful, critical, or pivotal change processes because it connects the productive change process to bringing about a therapeutic goal. The definition of productive change processes is inextricably linked with clients’ perceived progress toward their therapeutic goals.
Clients determine whether they persist in therapy; therefore, the client perspective is critical to investigating persistence (Horvath & Symonds, 1991). Through effect size comparison, Horvath and Symonds (1991) found that client-reported outcome is a better predictor of outcome than therapist-reported outcome and while observer report was found to be the least reliable predictor. Client self-report is useful for assessing client perceptions (Oka & Whiting, 2013). These previous findings justify the importance of using client report as the data source in the present study.
Purpose
The purpose of the present study is to develop and refine an instrument to quantitatively measure therapy productiveness. We report the results of a secondary data analysis, in which we reanalyze data collected for the purpose of understanding client perception of therapy productiveness. The development procedures for the Productive Processes Inventory (PPI) including procedures to ensure reliability and validity are presented and discussed. We discuss the results of a principle components analysis (PCA), followed by the process and rationale for refinements we have made to the PPI. The research question that guided the development of this instrument was, what components of the PPI (PPI) account for the most variance in client perception of therapy productiveness?
Method
Sample
The present data analysis was conducted as part of a larger study of productive change processes and client retention. We sampled adults (over age 18) who are current clients of MFTs being seen in a general therapy clinic. A convenience sample of 72 (N = 72) participants was recruited from community- and university-based therapy centers between October 1, 2014, and February 20, 2015. All university-based therapy centers are Commission on Accreditation in Marriage and Family Therapy Education–accredited training programs.
Potential participants were informed of the study and the requirements through recruitment posters and flyers displayed in therapy center waiting rooms. Recruitment flyers contained the Internet link to the survey and stated that participation is confidential and there are no consequences for choosing not to participate. The recruitment flyer also advertised an incentive, a US$5 Amazon© gift card.
The Internet-based survey was administered using the survey portal, QuestionPro©. A concern about using web-based surveys is the potential for sampling bias. Using the Internet for survey research limits the participants to those who have access to computers and the Internet. Given the increasing and widespread availability of the Internet, this was not enough of a concern to warrant using paper-and-pencil methods. An Internet-based survey allowed for data collection from participants in a way that was less intrusive to the therapeutic process and more confidential than completing the survey in the therapy centers. Further, collecting information about participant perception of therapy productiveness using a web-based method provided increased anonymity, which was important for participants to feel comfortable to disclose positive, and less-than-positive perceptions of therapy. This decision resulted from observations made during the qualitative phase of the larger study, during which it became apparent that participants who had less-than-positive perceptions of their therapist were reluctant to disclose.
The first page of the web-based survey was the study consent form, which participants were required to sign before continuing to the survey. The gift card was given directly through the survey platform, QuestionPro, and no identifying data were gathered in order to give the US$5 Amazon gift card. Sixteen potential participants viewed the survey but did not answer any questions.
Measures
Intended retention
Participants’ intentions toward the future of therapy are measured using an item written for the purpose of the present study. The first item asks participants to choose the response that best described how they feel about continuing therapy. Response categories are as follows: 1 = I will stop therapy because I have made my desired change, 2 = I will continue coming to therapy because I am making good progress toward change, 3 = I continue coming to therapy but I am not making progress toward change, 4 = I will stop therapy because I am not making progress toward change, and 5 = none of these apply to me. Responses 2 and 3 are modified from the Termination Status Form (TSF; Adams, Piercy, & Jurich, 1991). Responses 1 and 2 are considered positive intentions to remain in treatment, indicating that the participant has made the desired changes or will remain in therapy until making the desired changes. The later two responses are considered negative intentions to remain in treatment, as they indicate lack of perceived progress because of therapy. For the purpose of conducting a binary logistic regression analysis, Responses 1 and 2 were coded as intention to stay in therapy = 1, while Responses 3 and 4 were coded as intention to drop out of therapy = 0. These response categories intentionally include indicators of participants’ perceived therapeutic progress. As previously described, for the present study, retention is defined as intention to remain in therapy until participants have made progress toward attaining their goals. Premature dropout is defined as intention to end therapy before participants have met their goals (made progress toward change).
Productiveness
This instrument was designed specifically for the present study to quantitatively measure clients’ perceptions of the productiveness of change processes. The root question was “therapy is most productive for me when.” Likert-type response categories are 1 = does not apply, 2 = not productive, 3 = somewhat unproductive, 4 = somewhat productive, and 5 = very productive. A neutral response category is intentionally not included, as we aimed to encourage participants to make a decision between productive or unproductive responses (Dillman, 2007). The instructions stated that the “does not apply” response should be used when the given change process did not occur. An example of an item is “our therapist helps us clarify our therapy goals.” A score of 2 or 3 indicated change processes were unproductive and a score of 4 or 5 indicated change processes were productive. A higher overall score indicates higher perceived productiveness.
Design procedures for the PPI
The purpose of the PPI is to measure clients’ perception of how productive change processes impacted their decision to continue therapy. To develop the PPI, the first author reviewed and analyzed qualitative findings of studies of helpful and pivotal change processes in couple and family therapy for common or recurring themes. Studies were reviewed by Blow and colleagues (2009), Christensen and colleagues, (1998) Helmeke and Sprenkle (2000) and Wark (1994). Reoccurring themes, those found in two or more study results, were flagged for use in construct development. Once the researcher identified reoccurring themes, the researcher determined that these themes could be collapsed into four constructs that could be used to classify all results. Initial hypothesized constructs were therapeutic alliance factors, process factors, locus of control, and therapeutic time frame factors. Items were then created that are aimed to operationalize and measure the constructs identified. Items intended to measure the same construct were written in several different ways. Multiple versions of each item were included in the initial item pool.
We used the following procedures to ensure face, content, and construct validity. Obtaining feedback from both laypersons and experts supported validity. Expert reviewers were a university professor and a doctoral candidate in marriage and family therapy who have designed measurements and conducted independent research. Expert reviewers are familiar with the topic area. Layperson reviewers are seven adults intended to represent individuals who may seek services in a community mental health clinic.
Face validity refers to the degree to which the PPI looks like it is appropriate for measuring what it intends to measure. Having the words productive change processes and “staying in therapy” in the title addresses face validity. Both expert reviewers reported the PPI looks like it measures perceived productiveness of change processes and the decision to stay in therapy. Both expert reviewers reported that the PPI looks like it measures productive change processes. Further, all seven layperson reviewers agreed that the PPI looks like its purpose is to measure productive change process and the decision to stay in therapy.
Content validity refers to the extent to which the PPI truly represents the abstract construct of therapy productiveness (Pedhazur & Schmelkin, 1991). To address content validity, we operationalized constructs represented in the extant literature into variables through writing items. A strong connection to existing literature is an important step in demonstrating content validity (Pedhazur & Schmelkin, 1991). The therapy processes identified in each item as well as the language used to talk about these change processes are directly from the findings of qualitative studies on productive change processes (e.g., Christensen et al., 1998; Blow et al., 2009; Helmeke & Sprenkle, 2000; Wark, 1994). We asked two experts in MFT to assess content validity. To assess content validity, we created a spreadsheet, in which column 1 contained the construct and appropriate citation from the literature; in the second column, the item intended to measure that construct. In column 3, we asked reviewers to indicate their assessment of the degree to which the item represents the construct. Resulting from the expert review, we reworded 1 item that the expert believed did not accurately reflect the intended construct and removed 1 item that was determined to be qualitatively different than the others. Further, we solicited feedback on item clarity and length from past or current therapy clients. Reviewers were asked to comment on content validity and face validity and overall felt that the items assessed content and face validity.
Demographic Data
The mean age of participants was 34 years old, SD = 14.24, a range of 18–77 years. Sixty-nine percent of participants (n = 50) were White, 3% (n = 2) were native Hawaiian, 6% (n = 4) were Middle Eastern, 10% (n = 7) were Black, 7% (n = 5) were Hispanic, 3% (n = 2) were Asian, and 3% (n = 2) identified as mixed race. Sixty-three percent (65%, n = 47) of participants were female, while 32% (n = 23) were male, and one participant identified as transgender. Thirty-two percent (32%) of participants were single, while 51% were either in a committed relationship, living with their partner or married, and 10% of participants were divorced.
Fifty-one percent of participants had attended more than nine therapy sessions, while 28% attended between one and four sessions and 21% attended between five and eight sessions. Sixty-four percent of participants (n = 46) were clients of individual therapy, while 24% (n = 17) were in couple therapy and 12% (n = 9) were in family therapy. This variation may mirror the reality of a community-based treatment clinic, where the majority of clients present for individual therapy. Collecting data on therapy dosage using a categorical variable with three levels posed advantages and disadvantages. A disadvantage is the lost nuance, as the third level of this variable has a wide range. However, using three answer categories posed the advantage of allowing us to collect information about participants’ stage in therapy in a way that resulted in minimal missing data.
Each item of the PPI describes a change process identified in the extant literature, which participants must rate along a Likert-type scale ranging from not productive to very productive. Measures of central tendency, means, standard deviations, sample size, and range are presented for each item of the PPI in Table 1.
Productive Change Processes Inventory (PPI) Measures of Central Tendency.
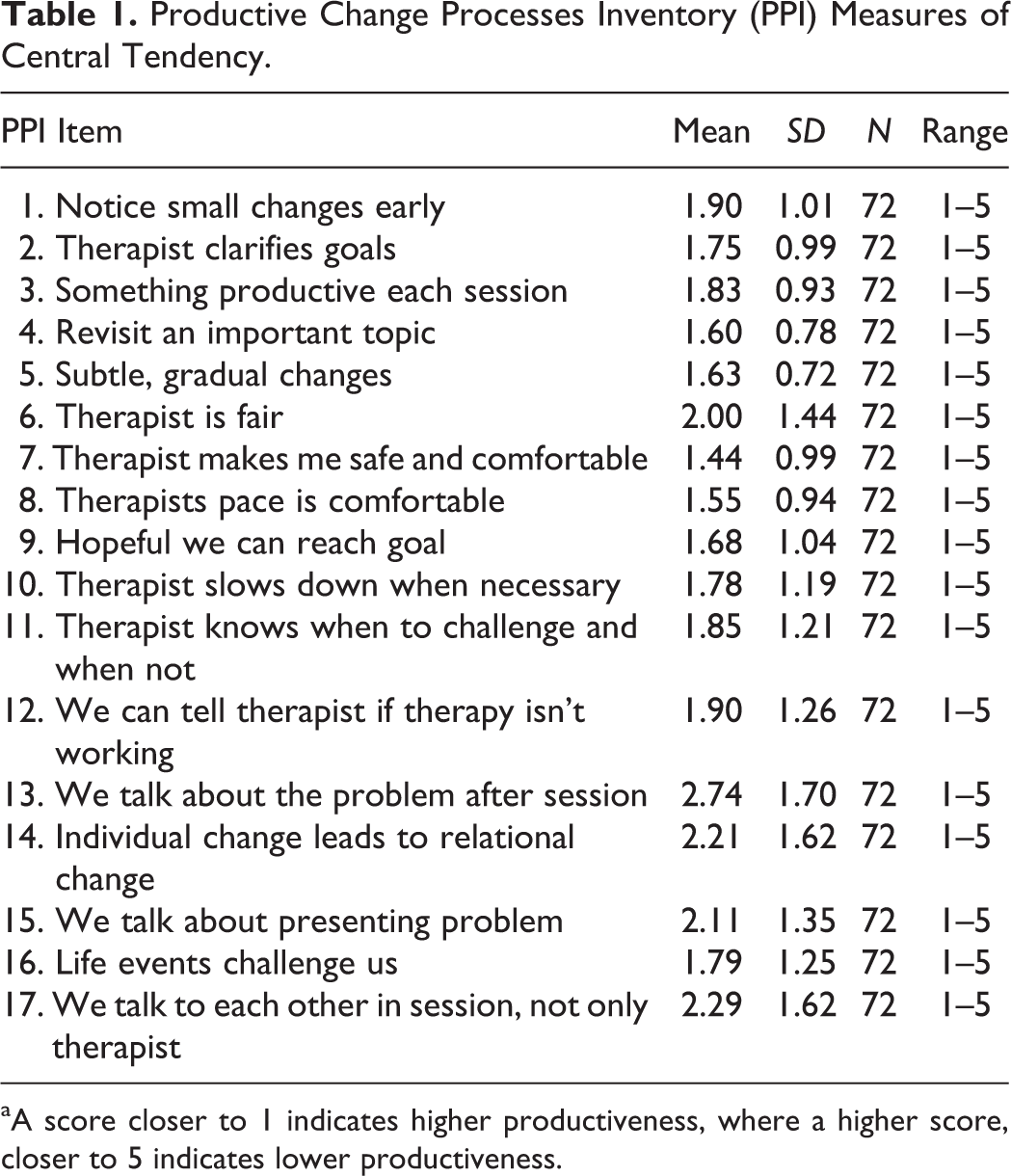
aA score closer to 1 indicates higher productiveness, where a higher score, closer to 5 indicates lower productiveness.
PCA
PCA is a useful data reduction technique for reducing a large number of factors down to a smaller number of components that describe the relationships among observed variables or to test the underlying process (Tabachnick & Fidell, 2013). PCA is particularly suited for use as an exploratory analysis to support construct validity by showing the components being measured by items (Tabachnick & Fidell, 2013). Three components were extracted, based on eigenvalues, and consistent with scree plot results. Tabachnick and Fidell (2013) recommend using varimax rotation when the solution is hypothesized to be orthogonal and when the goal is to simplify the number of factors by maximizing variance of the loadings within factors and across variables (Tabachnick & Fidell, 2013). Kaiser–Meyer–Olkin’s measure of sampling adequacy was conducted, and sampling adequacy was determined to be .769 with 16 variables and 72 participants. A score over .4 is generally accepted as adequate, indicating the present sample is acceptable for PCA (Tabachnick &Fidell, 2013). Bartlett’s test of sphericity was conducted to determine whether there is at least one meaningful correlation among the data set. Bartlett’s test of sphericity, χ2(120) = 653.57, p < .001, indicates these data were adequate to conduct PCA. Three components are evident in these data, as three components have an eigenvalue greater than 1, indicating that this component structure fits these data. Component loadings are presented in Table 2. The three components explained 60.83% of overall variance. Component 1, “productive relational processes,” accounted for 30.04% of variance in therapy productiveness, while Component 2, “productive therapist processes,” accounted for 13.83% of variance in productiveness. Component 3, “recognizing change markers,” accounted for 8.95% of the variance in productiveness.
Factor Loadings for the Original Version of the PPI.
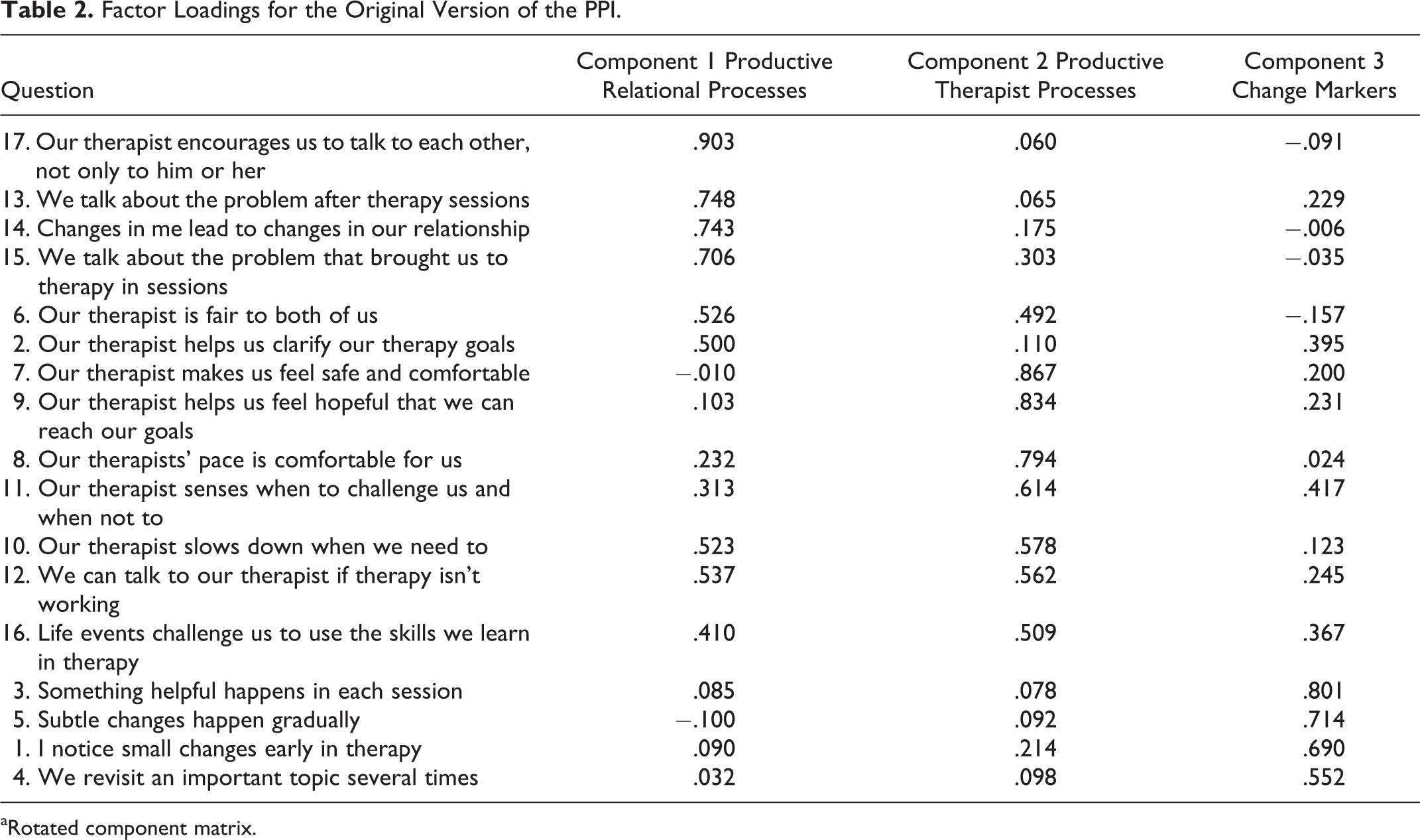
aRotated component matrix.
Reliability Analysis of the PPI
Reliability of the PPI was measured using internal consistency reliability, Cronbach’s α (Pedhazur & Schmelkin, 1991). Internal consistency reliability was used because it is most sensitive to the degree to which items on a measure are representative of the domain of the construct being measured and yields the highest reliability estimate of all methods (Pedhauzur & Smelkin, 1991). We applied the standard cutoff score for acceptable reliability of .70 (Nunnally, 1978). Cronbach’s α was .89, indicating high internal consistency reliability, as α = .7 is a generally accepted cutoff score (Nunally, 1978). Item 4, “we revisit an important topic several times,” was removed from the scale, as it did not contribute to reliably measuring the intended construct. All other items in the scale contributed to increasing internal consistency reliability of the PPI.
Revisions to the PPI
In this section of the article, we discuss our rationale for revisions made to the PPI. When revising the PPI, we examined each item’s performance to determine which items contributed strongly to measuring therapy productiveness. We removed Item 10, “our therapist slows down when we need to.” Upon examination of this item, the wording of this item may be unclear to participants. Participants may not understand what was meant by the term “slow down” without the researchers’ ability to further explain. This item did not load strongly onto any of the three components extracted in the PCA, leading us to conclude that this item is problematic.
We removed Item 16, “life events challenge us to use the skills we learn in therapy.” This item is more about events that are external to therapy and less about therapy productiveness. This item might lie outside of the scope of therapy productiveness, which focuses on in-session therapy processes. Additionally, this item did not load strongly on any component.
Revised PPI
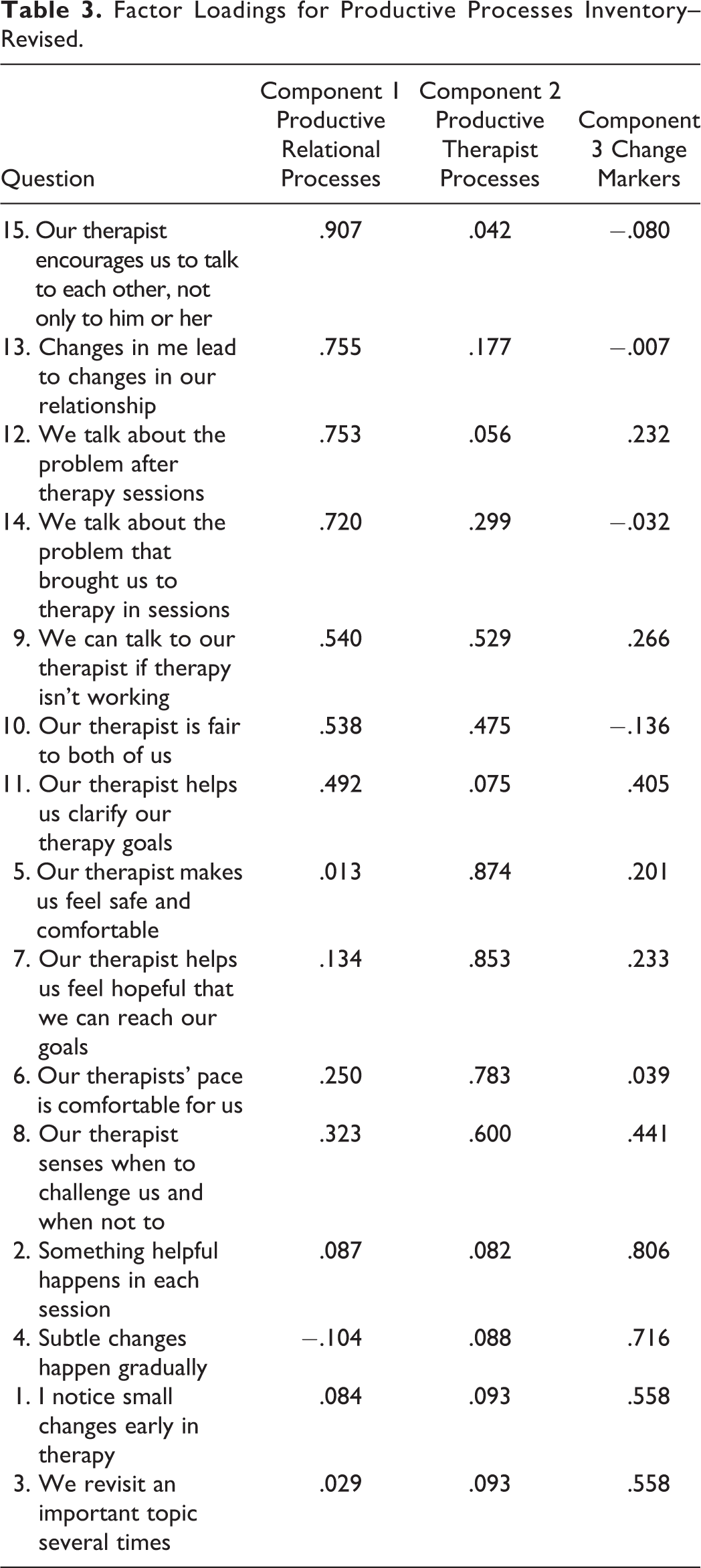
We conducted an additional PCA on the revised version of the PPI, or the PPI-R. The revised PPI (presented in Table 3) contains 15 items and yielded a Cronbach’s α of .863, indicating high internal consistency reliability. Kaiser–Meyer–Olkin’s measure of sampling adequacy showed sampling adequacy of .724 with 15 variables and 72 participants. Bartlett’s test of sphericity was conducted to determine whether there is at least one meaningful correlation among the data set. Bartlett’s test of sphericity, χ2(105) = 535.08, p < .001, indicates these data were adequate to conduct PCA. The three components explained 61.49% of overall variance. Component 1, productive relational processes, accounted for 35.87% of variance in productiveness, while productive therapist processes accounted for 15.53% of variance and recognizing change markers accounted for 10.08% of variance in productiveness.
Factor Loadings for Productive Processes Inventory–Revised.
Predictive Validity
Productiveness, as measured by the PPI-R, significantly predicted membership to the categories of intended therapy persistence or intended therapy dropout in a binary logistic regression analysis, b = −.944 (exp)B = .389, df = 1, p = .019, CI [.176, .859]). Further, productiveness significantly predicted the strength of the therapeutic alliance as measured by the Working Alliance Inventory – Short Form (WAI-SF) (Hatcher & Gillaspy, 2006) B = .458, t = 3.90, p < .001. Productiveness explained a significant proportion of variance in therapeutic alliance, R 2 = .17, F = 15.22, df = 1, 70, p < .001. The ability of the PPI-R to predict intended retention and the strength of the therapeutic alliance begins to support predictive validity.
Discussion
The present study described the procedures used to develop and refine a measurement instrument used to assess client perception of therapy productiveness with a sample of individual, couple, and family therapy clients. Results support the PPI-R as a potentially useful measure of therapy productiveness. This analysis revealed three components of the PPI-R: (1) productive relational processes, (2) productive therapist processes, and (3) change markers. The first component, productive relational processes, accounted for the most variance in therapy productiveness. The items that loaded onto this component all describe relationship processes between the participant and other members of the therapy treatment system. Although our sample contained participants in individual therapy as well as relational therapy, the component describing relational therapy processes accounted for the most variance. This result indicates that a large proportion of the variance in therapy productiveness is attributed to relational therapy processes. The second component, productive therapist processes, describes therapy processes that are imitated. These items include processes identified in previous studies of helpful therapy process such as building a strong therapeutic alliance (Christensen et al., 1998), engendering hope (Wark, 1994), pacing (Christensen et al., 1998), and facilitating helpful moments (Helmeke & Sprenkle, 2000). Four items loaded onto the final component, “change markers” that described how participants knew that therapy was productive. For example, 1 item “something helpful happens in each session,” indicates that when participants recognized that something helpful happened in each session, they concluded that therapy was productive.
High internal consistency reliability shows that the items measure the same construct, an important component of a viable measure. A PCA provides information about the factor structure of the PPI with a sample of individuals in therapy with a MFT. While the PPI-R yielded the same three-factor structure as the original PPI, there are key differences between the original version of the PPI and the PPI-R. Component loadings are all slightly higher in the PPI-R than in the original version. Since the items load strongly onto the revised components, it suggests that the items are now more accurately measuring those components. Eigenvalues show that the PPI-R accounts for a slightly higher percentage of overall variance than the original version.
Implications
The MFT field endeavors to understand what makes therapy feel effective to clients (Davis & Piercy, 2007a, 2007b; Pinsof & Wynne, 2000) and to understand the factors that contribute to therapy persistence or therapy dropout (Marchionda & Slesnick, 2013). The present results are consistent with Helmeke and Sprenkle’s (2000) findings, showing that therapy clients are able to identify productive or pivotal therapy moments. Productiveness may be an important, yet overlooked process variable that could be helpful in identifying the factors that contribute to therapy persistence.
While the construct of therapy productiveness possesses conceptual overlaps with the concept of therapeutic alliance, it is fundamentally distinct. Where therapeutic alliance scales measure perception of agreement between client and therapist along the domains of bond, task, and goal (Hatcher & Gillaspy, 2006), productiveness is centered on the client perspective. An area of overlap among productiveness and alliance is the therapist. Many productive elements of therapy involve the therapist, which makes conceptual sense, as researchers have asserted that the therapist is synonymous with the therapy (Blow, Sprenkle & Davis, 2007). In productiveness research, we do not aim to measure the strength of the relationship between client and therapist; rather, we aim to measure how productive the client perceives the therapy events facilitated by his or her therapist.
Several areas of couple and family therapy research would benefit from including and measuring therapy productiveness. For example, when testing new models or interventions, it would be beneficial to include and measure client perception of productiveness. Managed care companies are continually interested in efficacious treatment. Research that investigates client perception of productiveness may be of interest to managed care companies seeking to understand productive change elements of therapy treatment.
Limitations and Future Research
Slightly more than half of participants (64%) in the present study were in individual therapy, although with an MFT. This sample may have impacted the factor structure. The subscale, Productive Relational Processes, may have accounted for more variance in a sample comprised of participants in couple or family therapy. The PPI-R should be tested further using larger samples of participants in relational therapy. Additional studies of therapy productiveness using the PPI-R would be useful in further legitimizing it as a viable measurement instrument of therapy productiveness. Further refinement and testing, perhaps using a confirmatory factor analysis, would be an important way to advance this research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.