
Abstract
Substance abuse in parents is damaging to their children and the family system as a whole. If family treatment is paired with substance abuse treatment for the parents, children have the possibility of having better attachment with their parents and thus increase general functioning skills and overall family well-being. This study examined the impact of Whole Family Theraplay as an effective play therapy treatment with mothers in recovery from substance abuse and their children with attachment issues in an inpatient substance abuse rehabilitation facility. Scores indicated that women/mothers had reduced symptoms of distress and improved their mental health functioning. Their children demonstrated improved interpersonal relationships, reduced interpersonal distress, and improvement in overall mental health functioning. The implications of this study were that by implementing Whole Family Theraplay, in addition to individual and group counseling in substance abuse treatment, subjects showed demonstrated improvement in attachment relationships and mental health outcomes.
Substance use disorders (SUDs) have a tremendous impact on a societal, individual, and familial level. It is estimated that US$42.1 billion will be spent in 2020 trying to combat the many negative effects of SUDs (Substance Abuse and Mental Health Administration, 2014). Multiple theories, treatment approaches, and countless research have aimed at helping individuals recover from SUDs. Additionally, and more recently, there are growing investments in familial or systemic approaches to tackling the issues that nonaddict family members face when a loved one struggles with a SUD (Lander et al., 2013). However, most of these approaches are aimed at reducing negative childhood outcomes. Rarely, the focus has been on how to help the adult addict (who is a parent) improve their relationship with their child.
Parenting, or the quality of the relationship between the parent and the child, has lifelong impact on child development. Researchers conclusively find that substance abuse has a negative impact on parenting (e.g., Mayes & Truman, 2002). In fact, children with SUD parents experience poorer academic functioning; behavioral, emotional, and social problems; and less secure attachment patterns (Solis et al., 2012). The latter can be particularly detrimental in development as attachment style can be the difference between successful adaptation and functioning and the inability to cope, deal with stressful situations, or even form meaningful healthy relationships (Bowlby, 1969). As attachment is a key developmental concept in childhood, it would be important to understand not just how it is negatively impacted but also how it can be repaired.
Traditional approaches in the treatment of SUDs have focused more on individual pathology and not as much on systemic pathology. The effects of substance abuse are far more reaching and impactful than just the individual. Even if substance abuse treatment is successful for the individual, there remains the need to heal their impacted relationships in the system. Whole Family Theraplay, a systemic and attachment-based therapy approach, is a potential option for healing the systemic effects of SUDs on parent–child relationships (Booth & Jernberg, 2009; Weir et al., 2013). The purpose of this study was to investigate Whole Family Theraplay as an approach that could be particularly effective with repairing attachment bonds between children and a parent who struggles with substance abuse.
Literature
Substance abuse by parents can have damaging effects on their children (Dandona, 2016; Straussner & Baggerly, 2015). Some of the potential impacts parental substance abuse can have on their children include increased risks of child abuse and neglect, anxiety, depression, psychosomatic illnesses, regressive behaviors (e.g., thumb-sucking, enuresis, and infantile behavior), phobias, low self-esteem, social isolation, and eventual substance abuse of their own (Dandona, 2016). Impacts to children of substance-abusing parents should be viewed in a systemic context where issues pertaining to attachment, trauma, and interactions with institutional systems (educational, health, and social services) are often cyclical parts of the children’s tumultuous lives (Kaplan-Sanoff, 1996).
Treatment modalities for such families vary from motivational interviewing, harm reduction, and cognitive behavioral approaches (Straussner, 2014) to foster care and multifamily group therapy (Wong et al., 2019). Additionally, several previous studies have shown that both family therapy and play therapy are treatment modalities that have established histories of demonstrated effectiveness (Bratton et al., 2005; Carr, 2000a, 2000b; Charles, 2001; Cottrell & Boston, 2002; Crane & Hafen, 2002; Gil, 1994; Holder, 2008; Larner, 2004; Murphy Jones & Landreth, 2002; Pinsoff & Wynne, 1995; Sprenkle, 2002; Wettig et al., 2011). Among play therapy models, Theraplay® has a demonstrated record of effectiveness as an evidenced-based practice (Booth & Winstead, 2016; Tucker & Smith-Adcock, 2017). This study posits that Whole Family Theraplay (Weir et al., 2013)—an integration of Theraplay with family systems models—can be effectively utilized to improve both individual and family systemic functioning among mothers in an inpatient recovery program for substance abuse and their children. With its roots in developmental psychology and attachment theory, and with accumulating evidence from neurobiology, Theraplay gives a therapist a strong position from which to grow and families a way to connect with closer attachment patterns. Theraplay has found its way around the world and is practiced in 40 countries including the United States, Canada, Finland, Ireland, the United Kingdom, Turkey, and South Korea (Myrow, 2016).
Data that include participants of multiple ethnicities and remain valid across various cultures are especially important in today’s literature. Research reported by Kim and Nahm (2008) states that although play may be ubiquitous among human beings, parental involvement in children’s play varies historically across cultures. These various cultural norms need to be accounted for in order for us to demonstrate that Theraplay is effective with people of diverse cultural backgrounds and also show that a culture’s own traditional forms of play and interactions can blend well with the widely accepted values of a healthy parent–child relationship. Kim and Nahm (2008) noted that therapists found it easy to introduce new concepts and programs by observing games and activities that were already popular with their clients. Practitioners in Korea who sought to adapt many of the activities provided during their training found that the process was easier than expected because preexisting forms of traditional play activities fit many of the dimensions and were analogous to the originally suggested activities. For therapists who work with culturally diverse populations, Kim and Nahm (2008) suggest collaborating with parents to understand better how one might introduce play therapy, in general as a treatment option or in terms of specific activities. Many times, the transition can be smoother than one anticipates if close attention is paid to already existing family games that are familiar.
“Theraplay is a counseling approach that uses elements of play therapy to help children build better attachment relationships with others through attachment-based play” (Simeone-Russell, 2011). Theraplay was developed by Ann Jernberg in 1971. “Theraplay is an active, playful, short-term (about 12-week period of therapy sessions) treatment method that uses attachment-based play to create better relationships between parents and their children” (Booth & Koller, 1998, p. 308). Theraplay integrates interpersonal theories of human development, object relations theory, and the attachment theories of Bowlby and Ainsworth (Booth & Lindaman, 2000). The interaction provides healing emotional experiences that create secure attachment, that is, sensitive attunement to the child, contingent responsiveness, warmth and nurturance, mutually enjoyable interactions, dyadic regulation of emotion at a preverbal level, and stress-reducing physical contact. When participating with a parent in Theraplay, the child sees themselves as special and capable, the parent as trustworthy, and the world as safe and joyful. This shift results in a positive behavior change and generalized to other relationships and situations (Robison et al., 2009). The four key dimensions to building such healthy attachments through play are structure, engagement, nurturing, and challenge. Weir et al. (2013) best describe each dimension given here: Structure: The goal of structure is to assure the child that the parent is in charge and the child is safe with them being in charge. Structure helps children listen to and follow directions, providing them with a sense of security because they know they are being protected and guided. As children are regulated in a caring but structured manner, their ability to co-regulate their emotions will increase. Engagement: The goal of engagement is to connect with the child in a very intense and personal way, allowing the child to know that surprises can be fun and safe. Engagement involves paying attention to the child, making good eye contact, being upbeat, being playful, and communicating that the child is of worth through the adult’s attunement with the child. Often attunement begets affect regulation. Nurture: The goal of nurture is to produce an environment for the child that is caring, calming, and predictable; this gives the child a feeling of comfort and stability. This dimension (along with the other three dimensions) assists a child with affect regulation by meeting the child’s emotional needs at their level of development. Nurturance provides opportunities for tenderness, parent-child affection, and healing. Challenge: The goal of challenge is to give a child a challenge, but not to make that challenge undoable; this promotes a child’s self-esteem and promotes feelings of competence. As adults and children face and overcome challenges together, such cooperation enhances attachment. Also, as children experience some minimal frustration in facing and overcoming challenges, their frustration tolerance will grow and their affect regulation will increase.
A variety of studies suggest that Theraplay has been a successful and well-rounded mode of treatment for a wide array of different types of children with special needs and other disorders. According to Hiles Howard et al. (2018), their findings lend support to the validity and usefulness of Theraplay as an intervention for special-needs children. Activities in Theraplay provided opportunities for success while teaching the child how to manage feelings of anxiety or frustration. Their findings also found that Theraplay interventions improved interaction tasks between parents and children with autism. This is because Theraplay is based on the belief that a playful, interactive experience can help to improve parental attunement and sensitivity as well as a child’s affect regulation. Theraplay focuses on the nonverbal aspects of child communication and uses playful interactions as the medium for intervention. Siu (2014) mentions research on school-based play therapy has shown to have potential in reducing internalizing and externalizing behavior, increasing self-concept, improving social skills, increasing academic achievements and skills, decreasing attention deficit hyperactivity disorder symptoms, and reducing aggressive and disruptive behavior. Aspects of joint attention were also improved because of Theraplay research done by Hiles Howard et al. (2018). They discovered joint attention improves when parents are able to synchronize their behavior to their children. The children’s gains in consensual eye gazing, proximity, and responsiveness demonstrate that Theraplay can help improve some aspects of joint attention. Tucker et al. (2017) found their Sunshine Circle model of Theraplay to be a very promising intervention, especially for early childhood classrooms with large numbers of children experiencing toxic stress.
Children with internalizing problems tend to keep things to themselves and are less verbal in talking about their problems. Siu (2009) found the positive attention given to children through Theraplay could help to create a perception in children that they are lovable and valued, and in turn, this sense of feeling important may be an essential element in building children’s general self-esteem. There is no universal mental health treatment that works equally and universally for every single individual. Children require alternative methods to talk therapy. This may be further evident when the child has a complication related to communication. Behavioral treatment models are often seen as the solution to this problem, but they do not address the way children naturally interact in the same way Theraplay is capable. For a child who lacks a history of healthy attachments, this relationship may serve as the child’s first model of a secure and healthy attachment relationship (Simeone-Russell, 2011). Approaches like behaviorism and other similar treatment models make practical and effective use of systems of rewards and punishments, praise and redirection, clear expectations, inducements, incentives, and consequences to modify the child’s behavior and effect desired changes. These popular approaches work well with children without attachment disorders, but generally, behavioral approaches to treatment of attachment-disordered children may actually exacerbate their behavioral acting out. Some of the children do not fully grasp the reward portions of behavioral approaches and disproportionately focus on the punishment aspects of behaviorism (Weir et al., 2013). Attachment-disordered children often cognitively distort behavioral punishments in a relational context rather than a goal-achieving context. For example, an adopted or foster child with reactive attachment disorder who receives a consequence for misbehavior is more likely to think, “I hate my (foster) mom” instead of thinking “I shouldn’t have done that” in response to their consequence. Because children with reactive attachment disorder have difficulties with relationships, problem-solving, and responses to discipline (Hughes, 1997, 2007; Weir, 2011), Theraplay is able to coexist and fill in the gaps of these treatment models. Work by Friend (2012) demonstrates that these therapies have the potential to be easily incorporated alongside the existing theories and skills of many therapists working in the family therapy field.
Thus, our central research question is: Can Whole Family Theraplay be successfully utilized as an effective play therapy treatment with mothers in recovery from substance abuse and their children with attachment issues in an inpatient substance abuse rehabilitation facility?
Method
Sample
The sample consisted of 175 total participants, which included 78 mothers and 97 children. The children’s ages ranged from 2 days old to 11 years old, with a mean of 3.17 years old (SD = 2.755). Mothers’ ages ranged from 19 to 45 years old, with the parents averaging 28.3 years old (SD = 5.813), suggesting that the families were fairly young, for the most part; it should be noted that 28 mothers did not report their age. In terms of the gender of the participants, there were 78 mothers, 29 children reported as female (total 107 females), and 50 children reported as male. The remaining 18 participants (children) did not specify their gender. Twelve women reported being married, 35 women reported cohabiting together prior to their inpatient placement, and the remaining 31 mothers did not specify their relational status. In terms of ethnicity, 14 (8%) participants reported being African American, 33 (19%) reported being Caucasian or White, 5 (3%) reported being Hmong, 1 (.01%) reported being Filipino, 44 (25%) reported being Hispanic or Latino, 13 (7%) specified being Mexican and 15 (9%) reported multiple ethnicities, and 50 (29%) did not report their ethnicity, which suggests a very ethnically diverse sample.
In terms of socioeconomic status, these women are among the most impoverished in the United States. The annual income for the total sample averaged US$4,064.46. Of those who reported having an income prior to placement (22 mothers), their average annual income was US$9,395.27. The remaining 56 families reported having either no income or relying solely on state welfare and food stamps. One-hundred percent of the families in the sample are well below the federal poverty level. This region was ranked the absolute lowest in the nation in 2008 on the American Human Development Index by the Social Science Research Council (2013)’s “Measure of America” (Doyle, 2008). This index combines data on education, health, and income. Over the last decade, since it was ranked the lowest in the nation, the region continues to remain among the lowest rankings (among the bottom five or less) in the nation indicating a community where significant poverty, disparity, and poor health and educational attainment dominate perpetually.
Recruitment of Participants
As part of the intake process, women with children placed in the residential facility with them were offered free weekly Theraplay sessions in addition to their standard individual and group therapy sessions regarding substance abuse. For those women whose children were not placed in the facility but had weekly visitation in the facility with their children, weekly Theraplay sessions were offered in addition to their individual and group therapy. Subjects were free to accept or decline to participate, and no financial costs or compensation was offered.
Training and Supervision
The lead author of this study was designated as a “university-based Theraplay researcher” by the Theraplay Institute in Chicago, IL, and was one of the developers of the Whole Family Theraplay integrative model. After years of associating with the Theraplay Institute and training students for prior research studies involving Whole Family Theraplay, the lead author was granted permission to proceed with this study on behalf of the Theraplay Institute and provide supervision and training to the therapist-trainees providing the sessions in the facility. The therapist-trainees were all graduate students earning their master’s degree in counseling and were placed in the facility as part of their fieldwork curriculum.
Instruments and Study Design
The design of this study was a pretest/posttest quasi-experimental design using three key instruments: the McMaster Family Assessment Device (FAD), the Outcome Questionnaire-45 (OQ), and the Youth Outcome Questionnaire 2.01 (Y-OQ). The FAD was implemented to measure the family’s overall systemic functioning. It has seven subscales: Problem-Solving, Communication, Roles, Affective Responsiveness, Affective Involvement, Behavior Control, and General Functioning. The OQ was implemented to measure the parents’ outcomes through treatment on three subscales: Symptom Distress, Interpersonal Relations, and Social Role. The Y-OQ was implemented to measure the outcomes for the children. It has six subscales: Intrapersonal Distress, Somatic, Interpersonal Relations, Critical Items, Social Problem, and Behavior Dysfunction.
Reliability and validity scores for the FAD, OQ, and Y-OQ are all acceptable or high. The FAD subscales’ reliability scores (as measured by Cronbach’s α) range from .72 to .90 (Epstein et al., 1983; Miller et al., 1985). The OQ was reported to have a Cronbach’s α score of .93, with the subscales ranging from .70 to .93 (Ellsworth et al., 2006; Lambert & Finch, 1999; Wells et al., 1996), and the internal consistency reliability scores of the Y-OQ range from .74 to .93 for the subscales (Wells et al., 1996), with a very high total scale estimate of .97 (Wells et al., 1999). Additionally, various forms of validity testing have been thoroughly conducted on each of these three instruments, and all were found to be valid at acceptable or high levels (Ellsworth et al., 2006; Epstein et al., 1983; Lambert & Finch, 1999; Miller et al., 1985; Wells et al., 1996, 1999).
Families completed the assessment instruments prior to commencing the Whole Family Theraplay treatment sessions, at 1-month intervals during their stay in the facility, and again at the conclusion of the treatment. Mothers were to complete one FAD for their family, one OQ for themselves, and one Y-OQ for each child in their family. In all cases, the mothers completed the assessments, but the student-trainees were available to assist where needed. Therapist-student-trainees were responsible for the collection of the assessment instruments prior to commencing Theraplay treatment, at 1-month intervals while placed in the facility, and at termination of treatment.
After completing the pretest assessment data sets, families engaged in a modified version of the Marshak Interaction Method (MIM) simplified and adapted to just five tasks to accommodate larger families. The modified MIM assessment was only utilized in the first session of treatment as a clinical diagnostic tool to determine the attachment themes, strengths, weaknesses, and patterns in the adoptive families. Afterward, the family received 12–15 weekly sessions of Whole Family Theraplay with a wide variety of treatment games and activities based on what was learned from the Whole Family Theraplay’s modified MIM throughout a 16-week semester and then completed the assessment instruments upon termination.
Analysis
Pretest and posttest responses on the assessment instruments were compared utilizing t tests to examine statistically significant improvement between pretest and posttest scores. The current study went beyond collecting data from two time points, and instead, we collected responses before treatment (pretest, Time 1) and at five different time points after treatment commenced (posttest, Times 2, 3, 4, and 5). Each time period was 1 month apart from one another. In some cases, mothers in rehabilitation did not complete all five time periods (5 months) due to relapse, dismissal from the residential program, or other factors. The data were consistently available through Times 1, 2, and 3, but only available for Times 4 and 5 for those that remained in the residential facility throughout their specified course of treatment. Thus, the Results section of this study will utilize Times 1–3 as the common reporting of the data but also include significant results from Times 4 and 5 where available.
In our analysis of the FAD, we considered all seven subscales (Problem-Solving, Communication, Roles, Affective Responsiveness, Affective Involvement, Behavior Control, and General Functioning) as well as overall total scores on the FAD. The FAD served as a systemic measure of the family system. As mentioned earlier, one FAD was filled out by the mother for the whole family, which means that the scores were based off of her perspective of the family’s systemic functioning.
We performed t-test comparisons on the OQ for each parent of Time 1–5. We examined the change over time at both the subscale level (Symptom Distress, Interpersonal Relations, and Social Role) and the overall total OQ score. The OQ was used to measure the impact Whole Family Theraplay sessions had on the parents. Each parent filled out their own OQ.
Finally, we examined t-test comparisons of Time 1–5 for each child on the Y-OQ. The Y-OQ has six subscales (Intrapersonal Distress, Somatic, Interpersonal Relations, Critical Items, Social Problem, and Behavior Dysfunction). We ran t tests for each subscale and the overall total score on the Y-OQ from the data from Time 1–5. Instead of targeting a specific identified patient, we sought to determine how all children in the family system fared; thus, the Y-OQ scores for all children were examined.
Results
This study analyzed t-test comparisons for pretest and posttest scores on the FAD, OQ, and Y-OQ at five different time points to see whether there were favorable improvements in these areas among the family participants. Of the 95 total t-test comparisons analyzed, 10 were found to be statistically significant in all three of the measures. In order to conserve space and for consistency, only comparisons between Times 1 and 3 (as well as significant results from other time points) are displayed in the tables included. Additionally, it is fairly common in these types of studies to see that families tend to have nonsignificant results (and in some cases worse scores) in the second time point but improved results in the third time point and beyond (Weir et al., 2013), which was the case in this study.
These findings suggest that family systemic functioning showed improvement after Whole Family Theraplay treatment, specifically that there was a statistically significant change in pretest and posttest scores at Time 3 in the FADRoles at the p ≤ .037 level, FADGeneral Functioning at the p ≤ .013 level, and the FADTotal Score at the p ≤ .019 level and interestingly, FADRoles at the p ≤ .037 level again at Time 5, as seen in Table 1. The FAD Family Roles subscale is composed of items measuring family roles on a 4-point Likert-type scale on how much respondents agree or disagree with statements such as “We make sure members meet their family responsibilities,” “We discuss who is to do household jobs,” and “If people are asked to do something, they need reminding.” The FAD General Functioning subscale is composed of items measuring general functioning on a 4-point Likert-type scale on how much respondents agree or disagree with statements such as “In time of crisis we can turn to each other for support,” “We can express feelings to each other,” and “We feel accepted for what we are.” The FADTotal Score is measured by combining all of the subscales in the instrument. The findings indicate the Whole Family Theraplay treatment improved clarity on family roles both at Times 3 and 5, general family functioning at Time 3, and family systemic functioning in terms of the total score at Time 3.
Paired t-Test Findings Between Times 1 and 3 (Unless Specified): Family Assessment Device (FAD)—Total Score and Subscale Scores Results.

a t Test between Times 1 and 5.
*p ≤ .05.
The mothers who participated in this treatment were also assessed using the OQ. The results from pretest and posttests between Times 1 and 3 (along with a couple of statistically significant subscales from Time 4) are presented in Table 2. The results from the OQ indicate that adult parents showed statistically significant improvement in their symptom distress at Time 3 (p ≤ .031) and in their overall functioning (OQ Total) at Time 3 (p ≤ .036) and at Time 4 (p ≤ .039). The Symptom Distress subscale is composed of items measuring general symptoms like feeling anxious, unhappiness, headaches, trouble sleeping, and other indicators of mental and emotional distress on a 5-point Likert-type scale ranging from never to almost always. Sample items from this subscale include “I feel no interest in things,” “I have thoughts of ending my life,” “After heavy drinking, I need a drink the next morning to get going,” and “I feel nervous.” The OQ total combines all of the subscales (Symptom Distress, Interpersonal Relations, and Social Role) and is a good measure of an individual adult’s overall social and emotional functioning. The results from the study indicate that the mothers were able to benefit personally from treatment even though the Whole Family Theraplay is a systemic form of play therapy treatment.
Paired t-Test Findings Between Times 1 and 3 (Unless Specified): Outcome Questionnaire (OQ; Adults/Parents)—Total Score and Subscale Scores Results.
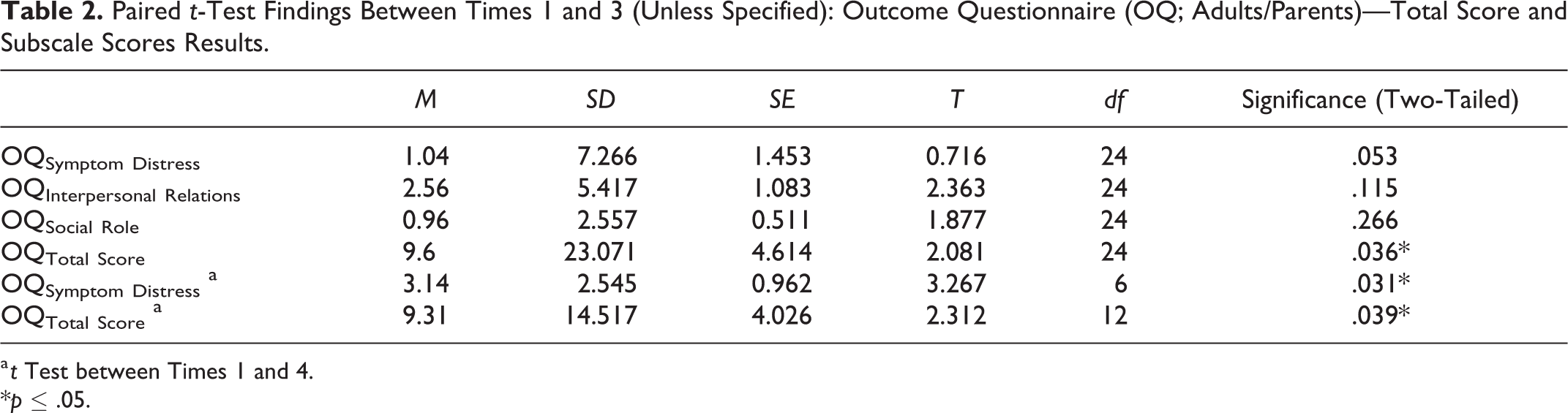
a t Test between Times 1 and 4.
*p ≤ .05.
The results presented in Table 3 from the Y-OQ indicate that Whole Family Theraplay treatments made a statistically significant improvement in interpersonal relations (p ≤ .027) and in the Y-OQ total score (p ≤ .048) at Time 3 and in intrapersonal distress (p ≤ .017) at Time 5. The Interpersonal Relations subscale of the Y-OQ consists of items measuring the quality of relationships with family, adults, and/or peers on a 5-point Likert-type scale ranging from never to almost always. A sample from this subscale reads, “Enjoys relationships with family and friends.” The Intrapersonal Distress subscale consists of items measuring the amount of personal distress a child has in their life, and the same 5-point Likert-type scale is used as in other subscales. A sample from this subscale reads, “Appears sad or unhappy.” The Y-OQ total score is a summation of all subscales that reflects the total functioning and well-being in the child’s life. These results suggest that the children benefited from receiving Whole Family Theraplay treatment at Times 3 and 5.
Paired t-Test Findings Between Times 1 and 3 (Unless Specified): Youth–Outcome Questionnaire (Y-OQ; Children)—Total Score and Subscale Scores Results.
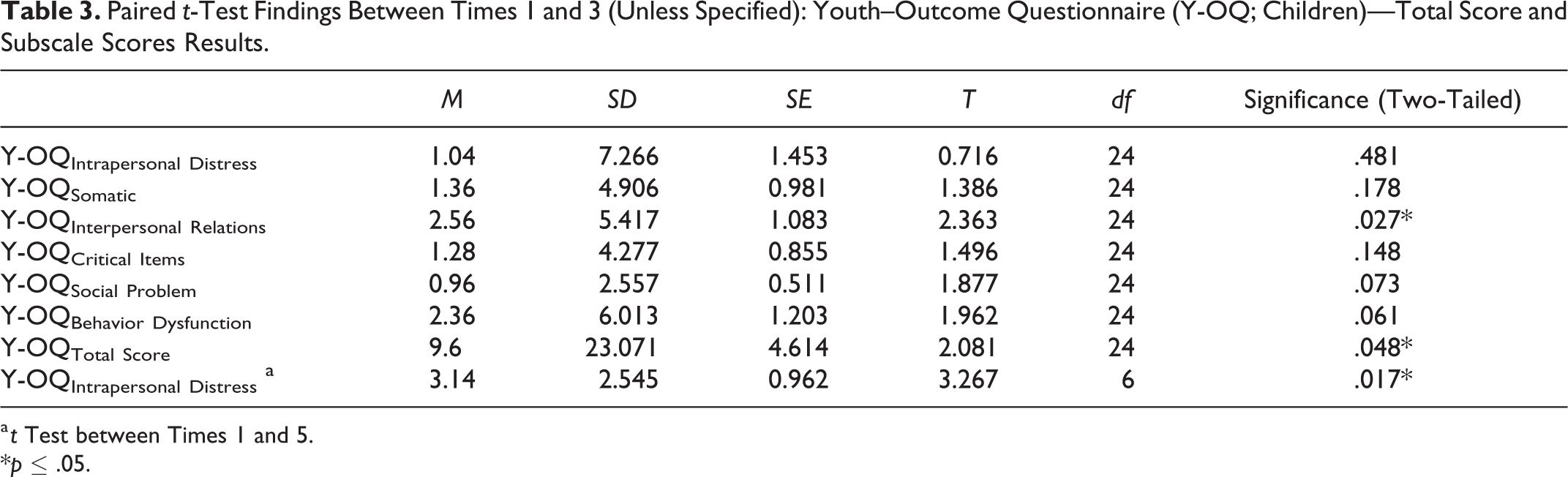
a t Test between Times 1 and 5.
*p ≤ .05.
Discussion
This study demonstrates that Whole Family Theraplay can have a significant, beneficial impact on women in recovery treatment for substance abuse and their children. Specifically, short-term application of Whole Family Theraplay treatment benefits women/mothers by reducing their symptom distress and improving their overall mental health functioning. Their children develop better interpersonal relationships, reduce intrapersonal distress, and improve their overall mental health functioning as a result of their involvement in Whole Family Theraplay treatment. Additionally, the family system, as a whole, appears to benefit in terms of having healthier roles in their family, increased general functioning skills, and overall family well-being as a result of engaging in short-term Whole Family Theraplay treatment.
What adds to the significance of this study is that these benefits for women, children, and their family systems are found in some of the most marginalized elements of our society. The high levels of diversity and the overwhelming poverty levels of these families did not deter significant improvements in these crucial areas of their lives. Building better attachments in all families leads to better individual and systemic social–emotional and mental health, but it is perhaps even more crucial in families where substance abuse, poverty, and oppressive societal racial barriers have caused much heartache and sorrow. Families in these difficult circumstances learned to have fun, connect, find joy, and function better. Such intangibles may be more significant to substance abuse recovery than previously considered.
It is also possible that the women’s improving sobriety as a result of their individual and group therapy substance abuse treatment was also a positive confounding factor that may also be partially responsible for some of the individual and family improvement scores. Indeed, we hope that it was. Yet, it may also be true that the Whole Family Theraplay treatment may have contributed to their recovery as well. We can hypothesize that as they felt more attached to their children, the women had increased motivation to excel in their recovery process. Future studies may be conducted to further explore the potentially recursive relationships between enhanced family health due to play therapy and substance abuse recovery outcomes.
The limitations of this study include the following: While most participants remained in treatment for the Time 1–3 assessment periods (allowing at least 12 weeks of Whole Family Theraplay treatment), not all participants completed the full 5 months (as indicated by Times 4 and 5 results). Some participants left the residential facility after the Time 3 period for a variety of reasons (loss of insurance funding, relapse, planned reunifications with family members, dismissal from the residence for violations of rules, voluntary departures, etc.). Thus, while it is evident that those that did remain to be assessed in Times 4 and 5 significantly benefited from further treatment, we do not have data on those participants who left the study after Time 3 and cannot determine the sustainability of their improvements. Another limitation of this study is that we were not able to engage in follow-up assessments once the mothers and children returned to their home environments. Thus, we cannot predict the lasting effects of Whole Family Theraplay outside their stay in the residential facility. Future studies could involve local caseworkers to attempt to obtain assessment data after the mothers and children have left the residential facility to ascertain whether the Whole Family Theraplay treatment had lasting effects in their home environments.
Conclusion
It is our conclusion that Whole Family Theraplay utilized in treatment for women in substance abuse residential facilities and their children benefited in significant ways in this study. Uniquely, mothers were found to have a decrease in symptom distress, and children were found to have improved interpersonal relationships and reduced intrapersonal distress. Most importantly, using Whole Family Therapy on a short-term basis was found to have statistically significant benefits in their overall mental health functioning for both women/mothers and their children. Where deemed appropriate, residential facilities treating women for SUDs may consider adding Whole Family Theraplay as outlined in this study as part of the treatment process.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.