
Abstract
To explore the relationships between complex trauma, family cohesion, family environment, resiliency, and depression, the authors employed hierarchical multiple regression and mediation analysis were employed with a sample of 485 young adults. The sample consisted of three groups of participants based on the amount of trauma experienced, those who reported 1–3 trauma experiences, those who reported 3 or more trauma experiences, and those who did not report trauma. Analyses indicated that despite complex trauma experiences, families were still able to cultivate strong family environment and family cohesion, which enhanced resilience in individuals and in turn reduced depression symptoms. Future research, as well as important implications for family counseling with the aim of enhancing family resilience and decreasing depression symptoms, especially as a trauma response, are discussed.
Trauma is an experience which follows the intolerable responses of heightened stress, emotional distress, and physical pain (Arnold & Fisch, 2013). A person's exposure to trauma can impact their social, cognitive, spiritual, and emotional wellness. Specifically, we focused on complex trauma which is chronic, ongoing traumas which have a higher likelihood to impact child development (Arnold & Fisch, 2013; Vergano et al., 2015). Complex trauma tends to occur within the family system such as child abuse, child maltreatment, the witnessing of intimate partner violence in the home, parental/caregiver substance abuse, parental/caregiver mental health struggles or suicidal ideation in the home, separation or divorce of parents/caregivers, parentification, medical challenges, parent/caregiver incarceration, general absence of a parent/caregiver, and community violence (Arnold & Fisch, 2013; Vergano et al., 2015). Foreman (2018) found counselors’ caseloads have a prevalence of trauma, while counselors are also highly likely to experience vicarious traumatization. Therefore, the topic of trauma is of high interest to family counselors.
The chronic nature of complex trauma is correlated to various physical and mental health issues. Physically, complex trauma reactions trigger a release of cortisol in the body which increases inflammation and has been correlated to autoimmune disorders, issues with the endocrine system, lung disease, heart disease, and liver disease (Lopes et al., 2020). Typically, physical ailments are a stressor for individuals they can worsen at unpredictable times. Furthermore, those who are physically ill may feel isolated if they need to take time at home to recover, or if they do not know others with similar ailments as they have. Considering the emotional toll these physical ailments have on humans, they have been linked to mental health challenges such as anxiety and depression (Ohrnberger et al., 2017). Delving further into the mental health impacts of complex trauma, those who experienced neglect or sexual abuse during childhood were more likely to have a depressive disorder and partake in violent acts of conduct as adolescents (Lee et al., 2012). One sample of young adult women who experienced complex trauma during childhood were found to have correlated symptoms of depression in young adulthood in comparison to those who did not experience complex trauma (Chapman et al., 2004). These findings suggest the need for more focus on symptoms of depression as a trauma response in the counseling literature. Our study aims to better address how depression symptoms may be impacted by resilience and the family system.
Despite significant findings focused on negative life outcomes resulting from trauma, resilience is still possible (Rosenberg et al., 2014). Resilience occurs when an individual acclimates to their environment after adverse events (Ungar et al., 2013). For example, acclimating post-event can consist of a person recalling previous success they had during a trying time, which enhances their confidence during future adversity (Connor & Davidson, 2003). One aim of our study was to understand the impact complex trauma during childhood can have on young adults as it pertains to the depression, resilience, and the family system.
Depression, Mental Health, and Complex Trauma
Depression was one of the main variables assessed in our study. Depression was defined as either a trauma response or a mental health disorder in which people lose interest in previously enjoyed activities, feel hopeless and helpless, experience sadness, fatigue, may lack self-esteem, can appear indecisive or have difficulty making decisions, feel chronically lonely, may experience a change in sleep patterns, and may have bouts of suicidal ideation (American Psychiatric Association, 2013). Multiple studies have found that college students may experience complex trauma at high rates which can lead to a negative impact on a person's mental health (Carey et al., 2018, Frazier et al., 2009). For example, a sample of young adult women's experiences of complex trauma during childhood were correlated to symptoms of depression in young adulthood in comparison to those who did not experience complex trauma (Chapman et al., 2004). Carey and colleagues (2018) also found that 28% of participants reported at least one sexual abuse prior to college entry. These participants reported elevated symptoms of anxiety and depression frequently, with at least 1 in 8 students reported symptoms of depression that surpassed clinical thresholds (Carey et al., 2018). These results present the case for the prevalence of complex trauma prior to young adulthood. It is important to understand complex trauma outcomes as repeated exposure to trauma throughout an individual's lifetime increases their risk for experiencing symptoms of distress, including depression (Frazier et al., 2009).
We aimed to understand if any relationship existed between depression symptoms, resilience, family environment, and family cohesion despite complex trauma during childhood. Previous studies that did not account for protective factors found complex trauma can increase risk for experiencing symptoms of distress, including depression (Frazier et al., 2009). Considering individual's risk for mental health concerns post complex trauma, specifically depression (Frazier et al., 2009), it was of particular interest to investigate which protective factors bolster resilience in young adults, including family environment and cohesion, and whether they mitigate the impact of depressive symptoms after enduring complex trauma. The focus on depression is imperative in the counseling literature considering it is highly prevalent in the United States (SAMHSA, 2014), and can be a trauma response (Vitriol et al., 2014). A better understanding of the relationship between depression and resilience can assist counselors with more effectively decreasing depression symptoms in clients while enhancing client resilience.
Resilience
Clients who display more resiliency, (e.g., holding hopeful attitudes about the future, utilizing a support system, and having a personal understanding of the meaning of life) learn how to receive help via the surrounding resources to persevere during or after traumatic events (Ungar et al., 2013). Such resources consist of family support, neighbors, general community, and schools (Ungar et al., 2013). Werner (1992) cultivated a list of factors that build children and adolescents into resilient adults; (1) adults encouraging children and adolescents to socially interact with each other; (2) optimistic worldview, faith, responsibilities, and goals; (3) Caregivers or Parents who model prosocial behaviors; (4) Caregivers or Parents who enhance self-esteem of children and adolescents; and, (5) Caregivers or Parents who are resilient and trustworthy in the eyes of the child/adolescent.
Previous research has led to conclusions that people are still able to demonstrate resiliency after trauma experiences (McGloin & Widom, 2001; Masten & Wright, 2010). Haverfield and Theiss (2016) found families who addressed trauma experiences occurring in the family had higher resilience levels and reduced depression symptoms in comparison to families who avoided acknowledging trauma. The ability to address trauma experienced within a family system could be due to family cohesion, as the families may have the tools to effectively communicate and higher comfort levels with each other to address difficult topics. Robbins et al. (2018) found that aspects of family environment, namely levels of attachment-related maternal avoidance and paternal anxiety negatively predicted resilience in their sample. This showed how young adults may exhibit greater or lesser resilience in the aftermath of enduring stressful life events dependent on their level of attachment to their parent/caregiver during childhood. This secure attachment can lead to emotion regulation, trust of others, and security in one's family system, and positive coping skills (Lindblad-Goldberg & Northey, 2013), all of which are signs of resiliency. Family counselors recognize that a portion of strengthening family resilience is enhancing attachment in the family system (Walsh, 2016). Secure attachments lead to comfort, trust, and commitment to the family system. These families are better able to problem-solve, and more easily access resources and coping skills to adapt to their changed life experience as a result of the trauma or crises, which is a sign of family resilience (Walsh, 2016).
Resilience, Depression, and the Family System
The family resilience literature (Walsh, 2016) recognizes that resilience is possible in children and adolescents who experience complex trauma. Siriwardhana et al. (2014) found the presence of familial support and other social supports were found to decrease likelihood of severe depression in young adults who experienced complex trauma during childhood. Findings such as these present the case for our study focused on the relationship between family and resilience that we hypothesized would decrease depression symptoms.
Resilience can also reduce depressive symptoms that an individual experiences as a result of enduring complex trauma. Individuals who are resilient are more likely to seek out social support, community support, are flexible, and can regulate their emotions during adversity, so that a more resilient individual who experiences depressive symptoms will be better able to partake in self-care activities that can reduce symptoms (Rosenberg et al., 2014).
When there is a lack of familial or parental support, children may experience psychosis and other moderate to severe mental health symptoms (Masten & Tellegen, 2012). We investigated why the relationship between family, resilience, and depression exists, which is the underlying reasoning that the family environment and family cohesion variables were essential to assess. In previous literature where mental health and resilience are main constructs, they appear to be a related, but they lack the variables to better describe why a relationship may exist. This is seen in a sample of youth who endured complex trauma, where a strong correlation existed between the number of disorders youth were diagnosed with such as depression, PTSD and substance use, and the number of traumas experienced (Rosenberg et al., 2014). Rosenberg et al. (2014) found a strong relationship between trauma and mental health diagnoses, as youth who reported the average number of traumas in the entire sample (N = 5.4) had seven times the likelihood of screening for depression. Youth who experienced complex trauma were at a greater risk for experiencing depressive symptoms and ultimately a diagnosis of depression. Yet, Rosenberg et al. (2014) did find resiliency is still possible in young adulthood to mitigate the effects of complex trauma on mental health symptoms. Considering these findings, we assessed the specific levels of depression in comparison to resilience levels. Our aim was to understand if resilience was a mediator between the relationship of family environment and depression as well as family cohesion and depression, as we recognized a gap in the research to more fully explain why resilience was possible.
Family Environment and Cohesion: The Protective Factors to Decrease Depression
The family system can provide the supports that consist of cohesion, religion, culture, values, independence, conflict, organization, orientation, control and expressiveness (Moos & Moos, 2009). Family cohesion is an important component when considering the overall environment within a family and is identified through empathy, connection, encouragement, compassion, and caring for each other's wellbeing (Moos & Moos, 2009). When a positive force, family systems can lead to resilience in children and adolescents leading to resilient adults (McClure et al., 2008). Family cohesion has been linked to resiliency where high levels of family cohesion are associated with children's self-confidence and self-efficacy in the home which translates to school and community settings (DiClemente et al., 2018). Family cohesion has been found to enhance the quantity and quality of protective factors present in a children and adolescent's lives leading to more resiliency as they age into young adults (McClure et al., 2008; Simpson, 2010).
Protective factors cultivated in the family system that may lead to resiliency consist of collaboration with others, belongingness, and self-restraint, which McClure et al. (2008) found were still able to be cultivated in families despite complex trauma exposure. Family cohesion is correlated to enhanced bonds within a family, providing children with the security of belonging in a group. Family cohesion can also lead to children being adaptable, stronger communicators, healthy boundary setters, and able to seek out healthy relationships (Uruk et al., 2007). In households where such cohesion exists, children and adolescents are comfortable with expressing their feelings enhancing resiliency. Zhao et al. (2015) found the presence of strong family cohesion was correlated to lower depression in children. Family cohesion was also correlated to some of the components of resilience such as ability to adapt. Children who did not perceive any family cohesion in their family system reported higher levels of depression and more intense feelings of loneliness. These findings further support the focus of the present study to continue investigating the role family environment and family cohesion have in resilience levels and depression symptomatology.
Purpose of Study
Our first purpose for the present study was to assess the relationships between the constructs, complex trauma, family environment, family cohesion, resilience, and depression. We assessed whether the construct resilience impacts the depression in young adults who experienced complex trauma. We also investigated if the relationship between family environment or family cohesion and depression was mediated by resilience levels. Our study was different than the majority of the complex trauma literature, as we measured a wide range of complex traumas rather than honing in on a specific type of complex trauma. It is imperative that the counseling research on complex trauma is; (1) Focused on a wider range of complex trauma since all are prevalent in client caseloads and; (2) more strengths focused so family counselors have a better idea which client characteristics should be highlighted to promote client resilience. Considering correlations exist between complex trauma and depression (Dworkin et al., 2017), we incorporated the variable depression alongside the variables, family environment, family cohesion, and resilience to understand if there are possible positive mental health outcomes.
Research questions proposed in the present study were:
Research Question 1: Does family environment and resiliency predict depression after controlling for complex trauma exposure?
Research Question 2: Does family cohesion and resiliency predict depression after controlling for complex trauma exposure?
Research Question 3: Is resilience a mediator for the correlation between family environment and depression?
Research Question 4: Is resilience a mediator for the correlation between family cohesion and depression?
Method
Participants and Procedures
The sample consisted of 485 participants ages 18–35 (M = 25 years) with 84.7% of the sample female (n = 410) and 14.3% male (n = 69). Participants also identified as non-binary (n = 3) and agender (n = 2). Regarding race and ethnic identity, 78.4% were White (n = 315), 8% were Asian (n = 32), 7.0% were Hispanic/Latinx (n = 28), 4.2% were Black/African American (n = 17), .5% were Native American (n = 2), and .2% were Pacific Islander (n = 1). Of these demographics, 7.2% (n = 35) participants identified with multiple race/ethnicities. Following approval from our University's Institutional Review Board (IRB), young adults were recruited via various Facebook groups, Twitter posts, Reddit feeds, email Listservs, and classroom talks. A wide range of recruitment techniques was important to obtain a diverse sample.
Instruments
Participants then completed the survey online via Qualtrics that included a demographics questionnaire, ACE Questionnaire (Felitti et al., 1998), Patient Health Questionnaire-9 (PHQ-9; Spitzer et al., 1999), Connor-Davidson Resilience Scale (CDRISC; Connor & Davidson, 2003), and Family Environment Scale (FES; Moos & Moos, 2009).
Demographics Questionnaire
A 13-item questionnaire in place to assess sociodemographic variables, knowledge of trauma, quantity of family members, and changes in family over time. Participants were able to select a response or insert their own response as needed. Participants were also given the option to skip questions.
Complex Trauma
The 10-item ACE Questionnaire (Felitti et al., 1998) measured previous experiences of complex trauma prior to the age of 18, and measured the quantity of these experiences. Participants answered “yes”, “no”, or “prefer not to answer” for each item. An example of an item is, “Did you often feel that … No one in your family loved you or thought you were important or special? or Your family didn't look out for each other, feel close to each other, or support each other?” When participants respond, “yes” one point is added to their final score. The questionnaire has a high internal consistency (Cronbach alpha = .95), a strong test-retest reliability, and strong construct validity (Poole, et al., 2016). While coding the data, scores were re-coded into three categories which consisted of (1) no trauma; a score of 0; (2) low exposure; score 1–3 (3) high exposure; a score of 4–10. The rationale for these categories was due to the findings that complex trauma has stronger effects on those whose score is 4 or higher. The no risk group was used as a reference group since they did not experience complex trauma.
Depression
The Patient Health Questionnaire 9 (PHQ-9; Spitzer et al., 1999), a 10-item scale in Likert format assessed symptoms and severity of depression over a period of two weeks, following the DSM-5 (American Psychiatric Association, 2013; Spitzer et al., 1999). There were five possible score outcomes for participants which consist of; severe depression = 20–27, moderately severe depression = 15–19, moderate depression = 10–14, mild depression = 5–9, and no depression = 0–4. Overall, the PHQ-9 exhibited strong reliability with a Cronbach alpha (.89). The PHQ-9 also has strong construct validity and test-retest reliability (Kocalevent et al., 2013), as well as high criterion validity (Lowe et al., 2004).
Resilience
The Connor-Davidson Resilience Scale (CD-RISC; Connor & Davidson, 2003) a 25-item measure, assessed resilience after complex trauma experiences. Resilience was measured by participant's ability to cope with negative scenarios, meaning of life, ability to take care of oneself, and humor in reasonable circumstances (Connor & Davidson, 2003). Higher scores are associated with high resilience levels. The CDRISC (Connor & Davidson, 2003) has a high internal consistency (Cronbach alpha = .89). When utilized with an adult population who was considered high stress, the test-retest reliability was .68 (Connor & Davidson, 2003; Wu et al., 2018).
Family Environment and Cohesion
The Family Environment Scale (FES; Moos & Moos, 2009), a 90-item questionnaire, which retroactively assessed family environment in the areas of; communication within the family system, activities, religious experiences, disputes, and violence. Participants answered each question with either “true”, “false”, and “prefer not to say”. The various subscales consisted of cohesion, conflict, expressiveness, achievement orientation, independence, intellectual-cultural orientation, moral-religious emphasis, active-recreational orientation, control, and organization. When analyzing data, we focused on the entire FES as well as the cohesion subscale. The test-retest reliability for the FES was .68–.86, and internal consistency ranging .61–.78 (Lucey & Lam, 2012; Moos & Moos, 1994). When used with a sample who experienced alcoholism in a family system, there was strong convergent validity (Sanford et al., 1999). Regarding various cultures, when utilized with a sample of African American and Latino youth the Cronbach alpha was slightly less than .70 (Groenenberg et al., 2013). Meanwhile, when used with a sample of Mexican American adults, Cronbach alpha was .61–.78, with the cohesion subscale was stronger with a Cronbach alpha of .78 (Negy & Snyder, 2006).
Internal Consistency of Instruments
Cronbach alphas were calculated as .89 for the PHQ-9 (Spitzer, Kroenke & Williams, 1999); .74 for the ACE questionnaire; and .92 for the CDRISC (Connor & Davidson, 2003). The Cronbach alpha for the entire FES (Moos & Moos, 2009) was .40 however, the family cohesion subscale Cronbach alpha was .80. We assessed high internal consistency existed with these instruments considering a Cronbach alpha of .70 or more is appropriate (Taber, 2018).
Procedures
Inclusion criteria required young adults to be ages 18–35 (Jackson et al., 2012; Logan et al., 2016). Participants completed the survey online, which started with an overview of the study, informed consent, as well as a trigger warning that trauma questions would be asked. Participants were reminded that their participation was voluntary and they were free to quit their participation in the survey at any moment. Crisis resources were listed following the trigger warning as well. Once participants finished the survey, they were led to the debriefing form.
Data Analysis
Participant data of individuals who were not ages 18–35 were removed from the dataset for analysis. Other participant data removed consisted of those who did not complete the survey, only completed the demographic questionnaire, or did not complete a significant portion of the survey to achieve scores for each construct, which would skew the data when analyzed (Graham, 2012). Histogram distributions and boxplots were also utilized to assess if outliers were present. This investigation led to one participant's results being removed from the final dataset, as this participant did not complete the family environment portion of the survey, meaning there was no score for that section.
The demographic variables were evaluated via means, standard deviation, range, and frequencies. To understand the strength and direction of correlations, Pearson coefficients were employed (see Table 1). To assess the relationship between (1) family environment, resilience, and depression and (2) family cohesion, resilience, and depression with complex trauma as the control variable in both models, hierarchical multiple regression was implemented. Prior to analyzing the data via hierarchical multiple regression, various assumptions were checked such as; normality, linearity, independence, homoscedasticity, and residual distribution (Tabachnick & Fidell, 2007). We followed specific steps for hierarchical multiple regression analysis which were; (1) Complex trauma as grouping variable (model 1); (2) model 2 consisted of the addition of either family environment or family cohesion; (3) Resilience was inputted into model 3; (4) The p value (<.05), F, R2, Δ R2 were assessed during each step. Statistical significance was considered numbers less than .05. The change in R2 was also examined during each step in the model.
Intercorrelations for Main Variables.
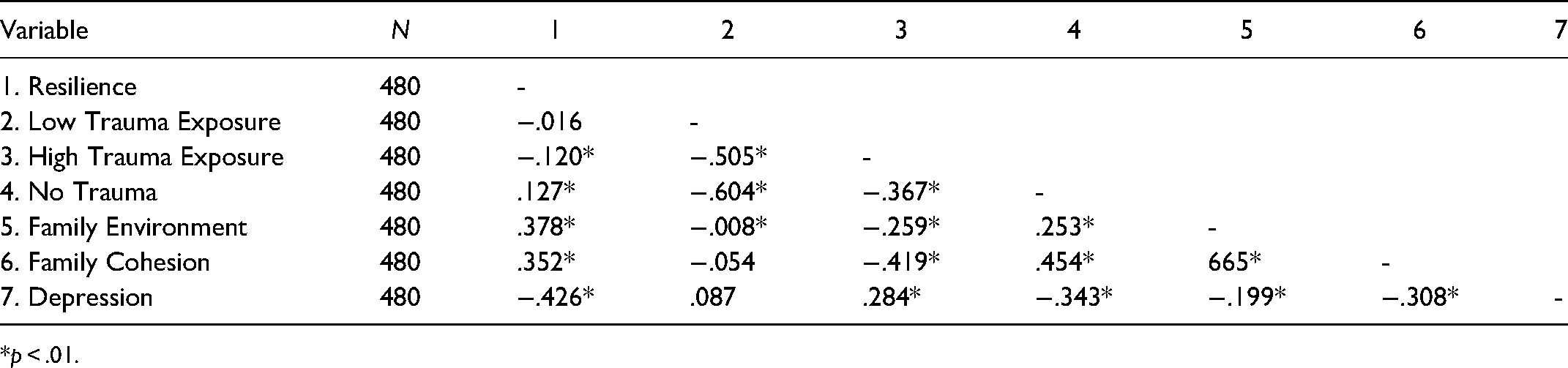
*p < .01.
Results
Main variables intercorrelations are found on Table 1. The variable correlations ranged from −.016 to .665. The correlations did not exceed .70, therefore no threat to multicollinearity existed (Tabachnick & Fidell, 2007). The means of the main variables were: complex trauma 2.17 (SD = 2.3), family environment (M = 49.8, SD = 10.2), family cohesion (M = 5.7, SD = 2.7), resilience (M = 7.4, SD = 16), and depression (M = 7.4, SD = 5.7). The construct, complex trauma exposure was created in three groups. Group one experienced a low exposure of trauma, which was quantified as the experience of 1–3 types of traumatic experiences (N = 219, M = 1.9). The next group was a high exposure of complex trauma, which was the experience of 4–10 types of complex trauma (N = 113, M = 5.5). The third group consisted of participants that did not experience trauma (N = 147, M = 0).
Research Question 1
A hierarchical multiple regression with three models was utilized to examine if family environment and resilience predicted depression. Model one was focused on the complex trauma construct with low trauma exposure and high trauma exposure being inputted into model one. The reference group, no trauma exposure was also inputted into the model. The variable, complex trauma accounted for 16% of the variance in depression (R2 = .155, Δ R2 = .159, F (2,479) = 45.051, p < .000). The variable, family environment was added to model two, which accounted for.02% additional variance in depression (R2 = .170, Δ R2 = .016, F (2,479) = 33.737, p < .001). Resilience was added to model three, accounting for an extra 14% of variance in depression (R2 = .312, Δ R2 = .142, F (2,479) = 55.306, p < .000). In model three, resilience removed the statistical significance of family environment, suggesting a direct relationship between family environment and resilience (higher family environment score correlated to higher resilience score). These findings suggest, family environment may be correlated to high resilience levels which can lead to low or no depression symptoms, defined as a score of 0–4 on the PHQ-9 (Spitzer et al., 1999).
Research Question 2
Another hierarchical multiple regression was employed to examine if family cohesion and resiliency predict depression. All three trauma groups were added to model one, with the participants who experienced no trauma as the reference group. In model one, 16% of the variance was accounted for by the variables (R2 = .155, Δ R2 = .159, F (2,479) = 45.051, p < .000). Family cohesion was added to model two, and accounted for an additional.03% of the variance for depression (R2 = .170, Δ R2 = .025, F (2,479) = 35.794, p < .001). These results demonstrate less trauma experiences may predict stronger family cohesion. When resilience was added to model three, it accounted for another 13% of the variance for depression (R2 = .312, Δ R2 = .133, F (2,479) = 55.247, p < .001) the addition of resilience variable removed the significance of family cohesion. The results demonstrate, high family cohesion is correlated to high resilience levels which are correlated to low or no depression. As expected, the findings were similar to those found for research question 1.
Research Question 3
In order to properly run a mediation model via hierarchical multiple regression, four steps were followed to establish that a mediation existed prior to re-running the analyses in SPSS. First, we assured all independent variables (complex trauma, family environment) had a statistically significant relationship amongst each other as well as the dependent variable, depression, this condition was met. The second step consisted of assuring family environment (independent variable) had a statistically significant relationship with resilience, which was the mediator. This condition was also met. Third, we investigated if a statistically significant relationship existed between resilience (mediator) and depression (dependent variable), which it did. Fourth, we were to analyze if the relationship between the independent variable (family environment) and the dependent variable (depression) was either erased or reduced significantly. In this case, the relationship no longer existed suggesting a mediation.
Once all conditions were met, we conducted the mediation analysis again via three steps using SPSS. In the first step of the mediation model, a relationship existed between complex trauma and depression and was statistically significant (R2 = .155, Δ R2 = .159, F (2,479) = 45.051, p < .000). In step two, family environment was added to the model, and the relationship between family environment and depression was statistically significant (R2 = .170, Δ R2 = .016, F (2,479) = 33.737, p < .001). When the mediator in step three, resilience was added and family environment lost statistical significance and no longer predicted depression (β = .034, t(479) = .792, p = .429), suggesting resilience is a mediator between family environment and depression (Table 2).
Hierarchical Multiple Regression: Relationship of Complex Trauma Exposure, Family Environment, and Resiliency to Depression (N = 479).
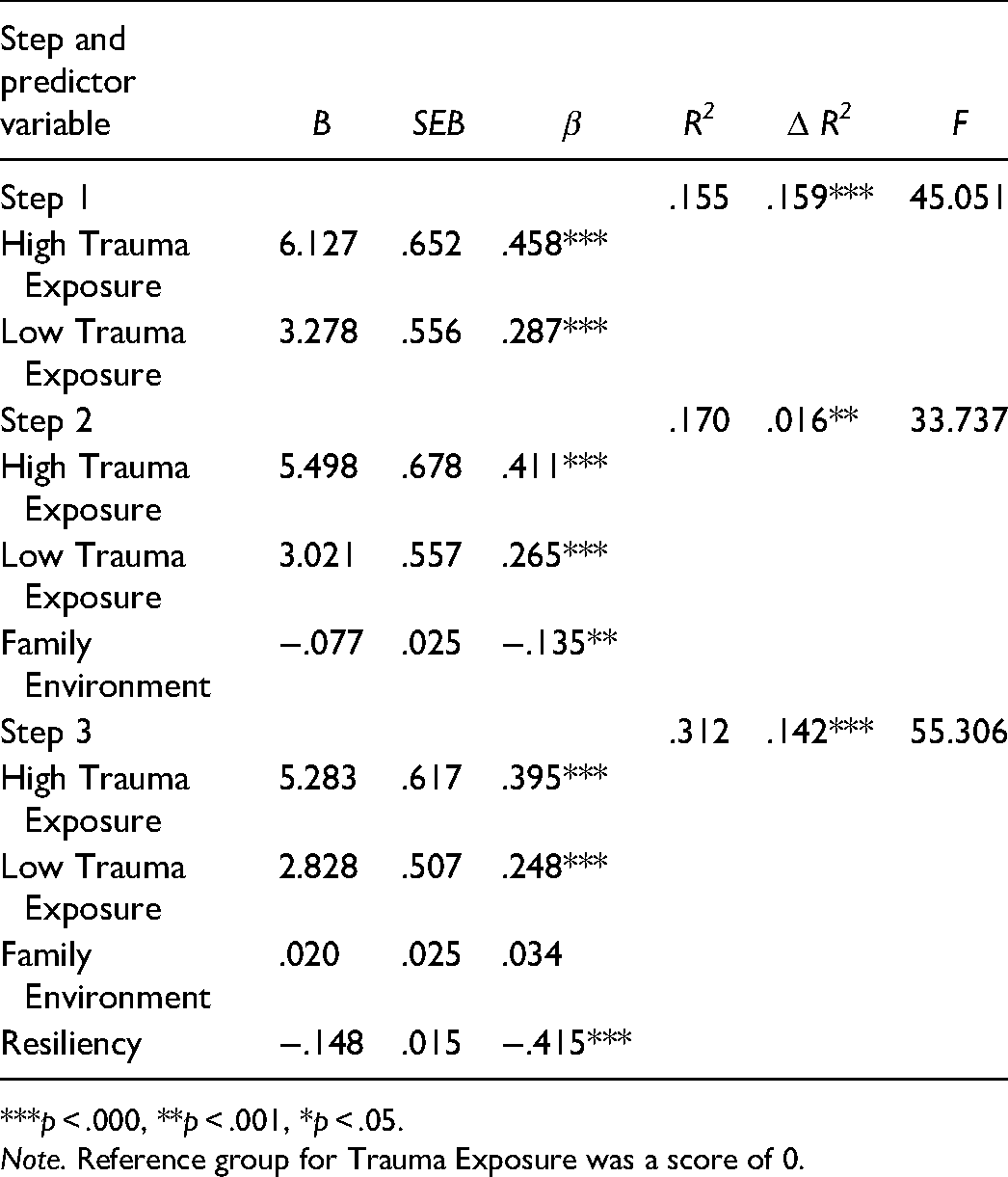
***p < .000, **p < .001, *p < .05.
Note. Reference group for Trauma Exposure was a score of 0.
Research Question 4
The same steps were repeated for question four however, a subscale of family environment, family cohesion was inputted into the model rather than the all-encompassing variable, family environment. First, we assessed all independent variables (complex trauma, family cohesion) has a statistically significant relationship amongst each other as well as the dependent variable, depression, this condition was met. The second step consisted of assuring family cohesion (independent variable) had a statistically significant relationship with resilience, which was the mediator. This condition was met. Third, we investigated if a statistically significant relationship existed between resilience (mediator) and depression (dependent variable), which it did. Fourth, we were to analyze if the relationship between the independent variable (family environment) and the dependent variable (depression) was either erased or reduced significantly. In this case, the relationship no longer existed, suggesting mediation.
Once all conditions were met, we conducted the mediation analysis again via three steps in SPSS. In step one, a statistically significant relationship existed between complex trauma and depression (R2 = .155, Δ R2 = .159, F (2,479) = 45.051, p < .000). In step two, the regression relationship between family cohesion and Depression was also statistically significant (R2 = .170, Δ R2 = .025, F (2,479) = 35.794, p < .001), meaning family cohesion is a predictor of Depression (β = −.186, t(479) = −3.833, p = .000). In step three, when the mediator, resilience, was added to the model, it removed the statistically significant relationship between family cohesion and depression (β = −.069, t(479) = −.683, p = .495). This suggests, resilience was a mediator for the relationship between family cohesion and depression (Table 3).
Hierarchical Multiple Regression: Relationship of Complex Trauma Exposure, Family Cohesion, and Resiliency to Depression (N = 479).
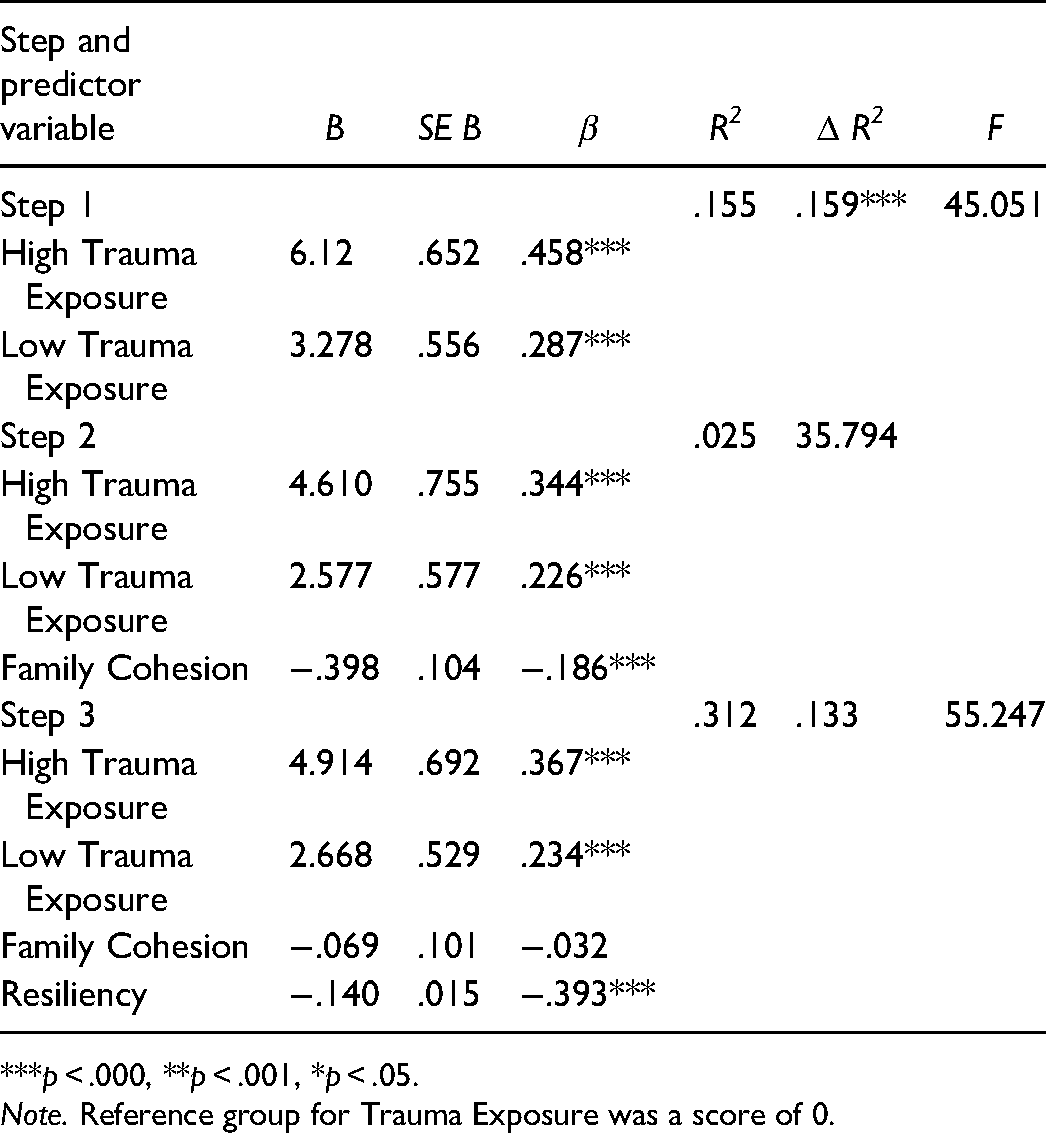
***p < .000, **p < .001, *p < .05.
Note. Reference group for Trauma Exposure was a score of 0.
Discussion
We aimed to advance the trauma research by focusing on factors that can enhance possibilities for resilience such as family environment and family cohesion despite complex trauma experiences. We also investigated how resilience might decrease depression. The results demonstrate that resilience is possible despite complex trauma exposures. Another main finding was that depression was lower in those with higher resiliency. The variable resilience was found to be a mediator between; (1) family environment and depression and; (2) family cohesion and depression. Our results led to more clarity regarding why people may display resilience and have less severe depression responses to trauma in comparison to previous research (Dworkin et al., 2017). We found family cohesion and family resilience were statistically significant in enhancing resiliency in individuals despite previous trauma exposure.
Lee et al. (2018) hypothesized resilience may be a mediator between trauma and depression (Lee et al., 2018), but his study did not include a family variable. The current findings expand the possibilities that resilience is a mediator between family environment, cohesion and depression, thereby identifying family assessment, support, and counseling as a means to enhance client resiliency and lower depression severity.
Considering depression can be a trauma response, a goal of ours was to analyze the variable depression to see how the severity of depression changes in response to the other variables, including trauma exposure, family environment, family cohesion, and resiliency. Dennison et al. (2016) found a statistically significant correlation between trauma exposure and depression (Dennison et al., 2016), which is aligned with the findings of the present study as complex trauma and depression were correlated prior to the addition of the other variables. Our study adds to the mental health counseling literature, by demonstrating that strong family environment or strong family cohesion may lead to resiliency that may decrease depression. These findings may be explained by the relationship between loneliness and positive family environments, as the presence of family is associated with lower levels of loneliness (Skopp et al., 2011). Meanwhile, higher levels of loneliness is associated with a lack of family support, and loneliness is one of the prominent depression symptoms (American Psychiatric Association, 2013).
Our findings demonstrate that despite complex trauma experiences and depression symptomatology, families are still able to cultivate strong family environments and family cohesion and maintain resiliency. Masten & Reed (2002) also found family as a force correlated with resiliency. Considering a lack of family cohesion and environment is correlated to the likelihood of an individual's experience of severe depression in adolescence (Eisman et al., 2015), our findings can be interpreted as insight into how counselors can utilize the family to decrease depression by using the family in counseling sessions during childhood and adolescence in a trauma informed, resilience focused manner.
Implications for Family Counselors
Considering our findings that family can positively impact outcomes pertaining to resiliency and depression, family counselors should utilize the family system in counseling sessions. Strengthening the family system by increasing protective factors helps to build resilience of individuals. The family resilience method can be utilized to enhance the likelihood of individual resiliency and other positive client outcomes. Family counselors who build resilience in their clients are able to prioritize understanding the relationships, boundaries, culture, and spirituality found in the family system as a means to understand first, the strengths and next the areas for improvement or negative cycles of interaction in the family system (Walsh, 2016).
To build child-client resiliency, family counselors can learn about the deficits in the family system and reframe or relabel the ways in which family members label a particular situation, or family member in the family system. For example, a family that experiences complex trauma in the form of interpersonal partner violence may label the identified client, typically a child or adolescent as “bad” since the child does not “comply” with the uncertain environment in their home. Family counselors should note the negative labels placed on identified clients and reframe by explaining to the family that the child is responding to the intimate partner violence in the home, and a behavioral response is expected in children (Bremner, 2006; Mersky et al., 2013).
Family counselors can utilize the family resilience approach. This approach is strengths-based, which is important for resilience building and strengthening family systems (Walsh, 2016). Treating depressive symptoms from a strengths-based approach may improve young adults’ resiliency thus reducing the negative pathological outcomes associated with complex trauma (Authors, 2021), and depression in particular. Counselors working with young adults who endured trauma may choose to include the family in sessions to lessen the risk of the client developing depressive symptoms (Courtois, 2004).
Trauma and depression were two important variables in our study especially as they relate to resilience. Interpersonal Psychotherapy (IPT) (Ellis et al., 2018) is another approach that counselors use to enhance resilience in clients who are experiencing trauma and depression. Aspects of IPT may be particularly useful since counselors can highlight the relationships in an individuals’ lives and their roles across multiple systems. For example, the family counselor may ask about boundaries constructed in the family system and assess the ways in which those boundaries (Teybur & McClure, 2011) help or hinder a client as they move forward in other relationships or systems such as their place of employment. This portion of IPT can enhance client resilience as it pertains to enhancing self-efficacy, more secure attachment, and greater self-awareness.
IPT delves into shame as a response to previous trauma exposure, and shame is also tied to depression symptomatology (American Psychiatric Association, 2013). Following the IPT approach, family counselors may ask clients about the ways in which family members responded to their feelings of sadness or some other feeling a client struggles to convey in the counseling relationship. Further investigation of the client's response will lead to joining between the counselor and client, and a space where the client can share their emotions without shame, which builds resilience and can lead to healing from depressive symptoms (Teybur & McClure, 2011). This exercise can enhance family cohesion as they can gain a better understanding of each other and strengthen communication moving forward. Furthermore, this use of an IPT approach empowers clients to take control of how they conceptualize their depression symptoms and take the next steps towards wellness (Kress et al., 2019).
Limitations
Our study contributed to the trauma and resilience literature in the mental health counseling. However, multiple limitations are still present. First, those who were willing to participate may be more likely to have overcome previous trauma and felt comfortable enough to share their experiences as a result. There were many attempts to diversify the sample regarding age range, ethnicity, education status, and socioeconomic status. Part of the attempt consisted of participant recruitment outside of college settings utilizing social media groups instead of solely recruiting in college classrooms. Despite this attempt, 50% of the participants were college students. A majority of the sample were white and female as well. Furthermore, considering the study was a self-report survey study, it can only be assumed that participants were absolutely truthful in their responses. However, stigma and shame could sway participant responses. Lastly, causation cannot be deemed considering the study is correlational. Some people do not perceive depression as an emotional response, rather they are more in tune with the physical symptoms of depression (Dailey et al., 2014), participants who quantify depression more physically may not be accounted for in the data.
Future Research
A larger variety of constructs that may promote resilience after trauma exposure should be assessed, in future studies. Further investigation of family variables and family relationships may enhance the literature considering that we found statistically significant relationships between family environment, cohesion, depression, and resilience. Research focused on the counseling process of families who experienced trauma is needed to understand how to better prevent negative impacts of trauma. Such studies will assist counselors in the pursuit of providing higher quality care for children, adolescents, and families. Additional research on other counseling approaches for depression as a trauma response such as IPT would be beneficial, especially considering IPT tends to only be taught in advanced graduate courses or solely at the doctoral level depending on the program.
Conclusion
A gap that exists in the counseling literature is the lack of strengths-based research with resiliency outcomes as it pertains to trauma experiences. Our findings provide a better understanding of positive outcomes in clients who experience trauma. Meaning, clients can experience trauma and also display resilience. Furthermore, higher levels of resilience levels can decrease depression symptomatology. Therefore, we suggest family counselors place a high importance on the family system. Despite the chaotic experience of trauma, there is still hope for a positive family environment and cohesion. Thus, family counselors should aim to fortify family systems when working with families impacted by trauma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.