
Abstract
When individuals are in duress, they often neglect health habits. Research shows romantic partners often adopt similar health habits. This study sought to examine the relationship between health habits and current health status as couples endured the winter (2020–2021) peak of the SARS-CoV-2/COVID-19 pandemic. Mixed gender couples (N = 228) completed this ecological momentary assessment designed study over a 2-week period. Regression analysis tested the relationship between physical health status and health habits including healthy weekday eating, weekend emotional eating, exercise, sleep quality, troubled sleep, tobacco use, and alcohol use. Tobacco and alcohol use were not significant, and all other predictors were significant. Next, we tested actor partner effects between physical health status and health habits using the predictors that were significant in the regression model. Weekday healthy eating and sleep quality were related to physical health status for both men and women. Weekend emotional eating was related to health status for women. Exercise showed actor effects for women only and partner effects for men only. Sleep quality showed partner effects for men only. Surprisingly, our findings showed no potential regulatory effects for men regulating women's physical health status through their health habits. However, women's health habits were related to their male partners’ physical health status. This adds to the growing body of research showing a regulatory effect for women to men in different-gender relationships.
The SARS-CoV-2 (COVID-19) pandemic caused unexpected changes in our lives. Traversing new daily routines (e.g., working remotely and virtual school) caused significant stress for many. Changes may have been particularly hard for parents (Czeisler et al., 2021) who needed to learn how to keep themselves and their children safe during the pandemic. Parents are often reliant on others (i.e., childcare services, grandparents, and relatives) to share in the caregiving responsibility and for social support when parenting is challenging (e.g., respite, connections with friends, and advice from other parents). When these systems maintaining the family status quo are interrupted, as we saw early in the pandemic, the burden of increased childcare responsibilities (e.g., homeschooling and leaving the labor force) often becomes the responsibility of the mothers in mixed gender relationships (Collins et al., 2021) leading to gender disparities and worse health outcomes for mothers (Flor et al., 2022).
When under stress, individuals are more likely to neglect positive health behaviors. For example, stress is a barrier to exercise (Marashi et al., 2021) and sleep quality (Alotaibi et al., 2020) and individuals may turn to alcohol (Childs et al., 2011), tobacco (Torres & O'Dell, 2016), and poor diets (Richardson et al., 2015) to cope. When individuals face long-term stress and are coping with poor health habits, they are more likely to develop chronic health conditions.
Health habits such as healthy diet, sleep quality, regular exercise, limiting alcohol use, and eliminating tobacco use are some of the best options for preventing chronic disease (Liu et al., 2016; NASEM, 2017) and their importance increases with age. Middle age may be the time when poor health habits catch up with us (Linardakis et al., 2015).
Adhering to positive health habits can be challenging (Garner et al., 2017). Individuals may need an accountability partner to initiate or continue positive health habits. For many individuals, health habits are dictated by a romantic partner's support and adherence to healthy habits (Kiecolt-Glaser & Wilson, 2017). Couples adopt each other's health habits, and this may be related to couple dynamics (Brazeau & Lewis, 2021). Research has consistently demonstrated through statistics that romantic partners influence health (Kiecolt-Glaser & Wilson, 2017; Meyer et al., 2019; Young et al., 2019). Findings range from showing that when one partner reports better health their romantic partner will also show better physical health (Meyer et al., 2019) to partners influencing one another's health habits (Young et al., 2019). When one makes positive changes for their health, their partner is also likely to engage in these behaviors (Jackson et al., 2015). The purpose of this study was to examine the relationship between health habits and global physical health in couples (mostly middle-aged and parents) facing pandemic stress. We predicted, using the entire sample, poorer health habits (higher alcohol use, poor eating habits, less daily exercise, smoking, poor sleep quality, and troubled sleep) would be related to lower global physical health. We sought to identify if romantic partners influenced health habits and global physical health. We predicted one's own (actor effects) poorer health habits and one's partner's (partner effects) poorer health habits would be related to lower global physical health in both partners.
Methods
Participants
Couples (N = 228, n = 114) participated in this dyadic, longitudinal study examining how couples coped during the pandemic. Couples had been together for an average of 11.56 years (SD = 8.51, range 1–50 years). Participants ranged in age from 22 to 76 (M = 36.38, SD = 9.20). The sample was predominantly white (n = 146, 64%), followed by Black/African American (n = 32, 14%), Asian (n = 18, 8%), Latinx (n = 14, 7%), Multiracial (n = 10, 4%), and fewer than five individuals identified as another race or ethnicity. The sample was mostly heterosexual (n = 215, 94%) followed by bisexual or pansexual (n = 6, 3%) with fewer than five individuals identifying as another sexual orientation. The majority had a bachelor's degree or higher (n = 159, 63%). Most couples (n = 97/114, 85.8%) were married/civil union with the remaining couples identifying as cohabiting or a different type of relationship. Most couples had children (n = 96/114, 85%). Gender was almost evenly split (n = 115 women, n = 111 men), with the remaining participants identifying as another gender or not responding. Almost all individuals reported at least some pandemic stress (201/211, 95%).
Procedures
The study was approved by the internal review board of the researchers’ university. Data was collected during the fall/winter 2020–2021 pandemic peak of cases. Couples learned about the study from paid Facebooks advertisements targeting potential participants by age and relationship status, parenting groups, and newsletters (e.g., churches and universities). Flyers were posted in medical clinics and online to platforms for elementary schools, preschools, and parents’ social media groups. To participate, both partners needed to consent and to be: (1) aged 21 years or older, (2) cohabitating, and (3) able to respond to the survey in English. Potential participants contacted the PI via a research Facebook page (not any of the researchers’ personal Facebook pages) or emailed the PI to demonstrate an interest in the study. Individuals known to the PI were not actively recruited for the study. As this study was advertised online, we needed to ensure all respondents were real couples. The PI corresponded with all couples via email to share study information, gather phone numbers, and ensure email responses were consistent with a real person responding. A research associate called the couple to confirm eligibility and describe the study in detail and determine dates to complete the study. Couples selected days to complete four surveys including two surveys during the week and two over the weekend across a 2-week period. All couples were emailed the links on the chosen days and asked to complete their survey just before bedtime reflecting on their entire day. Daily surveys took approximately 10 to 15 min to complete. Couples were thanked with a gift card for their participation. If couples completed the full study, they received a $20 gift card.
Measures
Demographics
Demographics (e.g., age, gender, race, ethnicity, parental status, relationship status, income, and education) were collected via self-reported. Stress related to the pandemic was measured through one item asking about distress specific to the pandemic, “How distressing have you found the situation with COVID-19?”. Participants responded on a five-point Likert scale ranging from (1) little to no distress to (5) extremely distressing. Participants most frequently reported pandemic changes to be distressing (M = 3.27, mode = 3, n = 69), followed by very distressing (n = 54), somewhat distressing (n = 44), extremely distressing (n = 34), little to no distress (n = 10), with 17 individuals not responding.
Global Physical Health
We used the four-item Patient-Reported Outcomes Measurement Information System (PROMIS) Global Health (Hays et al., 2009) to measure overall physical health (e.g., pain, ability to engage in activities, fatigue, and perceived physical health). This instrument has sound psychometric properties (internal consistency 0.81; correlated with similar measure EuroQol-5D. r = .76; Hays et al., 2009).
Eating Habits
Eating habits were measured using two items that were included in the statistical models independently. Emotional eating was assessed using a seven-point Likert scale (1 = ‘strongly disagree’, 7 = ‘strongly agree’) to gauge the level of agreement with the statement “Today, I ate when I felt upset or angry.” Healthy eating was measured using the same response scale with the item, “Today, I ate healthy.”
Alcohol Use
Alcohol use was measured using one item that asked participants to indicate the number of alcoholic beverages they consumed in the past 24 h. Participants responded using a six-point Likert scale (1 = ‘0’, 6 = ‘5+’).
Tobacco Use
Tobacco use was assessed using one item, “Do you use tobacco products?”, with three response options: “yes, no, sometimes.”
Sleep
Sleep habits were measured using two items that were independently entered into the statistical models. Sleep quality was measured with the following question, “Overall, how would you rate your sleep quality?” Participants could respond using a five-point Likert scale ranging from terrible to excellent. Trouble sleeping was measuring using the statement, “Thinking about your sleep on an average night, I have trouble getting to sleep.” Participants responded to their level of agreement using a five-point Likert scale from never to always.
Exercise
Exercise habits were measured using the item, “Overall, how frequently do you exercise, at least, the recommended 150 min per week?” Participants responded on a six-point Likert scale from “never” to “always.”
Analytic Plan
Using SPSS 27, we sought to investigate what specific health habits were significant predictors of global physical health in the sample. We regressed daily alcohol use, eating habits, daily exercise, smoking status, sleep quality, and troubled sleep on global physical health.
Next, we used the significant predictors from the regression model (e.g., eating habits, exercise, and sleep) to measure individual and dyadic influences on health. Multiple Actor-Partner Interdependence Models (APIM; Kenny et al., 2006) were conducted to assess how individual male and female global health status (actor) as well as partner global health status were related to eating habits, exercise, and sleep. APIM models treated dyads as distinguishable based on gender and a two-intercept model approach was used to obtain actor-partner effects per level of the distinguishable variable. Only mixed gender couples were included in APIM models. Using the Lavaan program for R (Rosseel, 2012), APIM models were conducted via structural equation model with bootstrap and maximum likelihood estimation run. Analysis was completed online through a web-based program (Stas et al., 2018). No outliers were found in all the analyses. Gender effects were calculated simultaneously, controlling for nonindependence. Nine partial correlation effects were provided in these models including: (1) female intercept; (2) male intercept; (3) female actor effect (global physical health status on own eating habits, sleep, and exercise); (4) female partner effect (global physical health status on partner eating habits, sleep, and exercise); (5) male actor effect (global physical health status on own eating habits, sleep, and exercise); and (6) male partner effect (global physical health status on partner eating habits, sleep, and exercise). Beta coefficients are Z tests and standard errors were calculated to assess the relationship of actor and partner effects on global physical health status (Stas et al., 2018).
Results
Assumptions Check
Prior to executing a multiple regression analysis, data was checked for outliers, missing data, and violation of assumptions. One outlier was identified but included in the analysis as it was anticipated it would not impact the outcomes enough to change the model. We calculated means for daily scores. If the participant had at least one unit of data, we calculated a mean. Other missing data were not included in the analysis. Most assumptions were not violated (multicollinearity, sample size, and normality, linearity, and homogeneity of variance among the residual). Most variables had acceptable skewness and kurtosis except for alcohol usage which was positively skewed. Thus, we transformed the variable and because the transformation had a limited impact on the results, we used the original data.
Regression Analysis
A multiple regression analysis was conducted with global physical health as the dependent variable and emotional eating (weekend days, weekdays, and average), health eating (weekend days, weekdays, and average), alcohol use (weekend days, weekdays, and average), overall exercise, tobacco use, and overall sleep quality, and overall troubled sleep. The model demonstrated good fit (F(10, 194)= 8.45) with 30.3% of the variance explained by the model (R = 0.55, R2= .30, adjusted R2 = .27, p < .01). The significant independent variables were emotional eating on the weekend (unstandardized coefficient β1= −.07, p = .04), healthy weekday eating (β2 = 0.29, p = .007), exercise (β3 = 0.21, p = .022), troubled sleep (β4= −.36, p = .011), and sleep quality (β5 = 0.50, p = .005). Weekday emotional eating, weekend healthy eating, alcohol use, and tobacco use were not significant predictors.
Actor Partner Interdependence Models
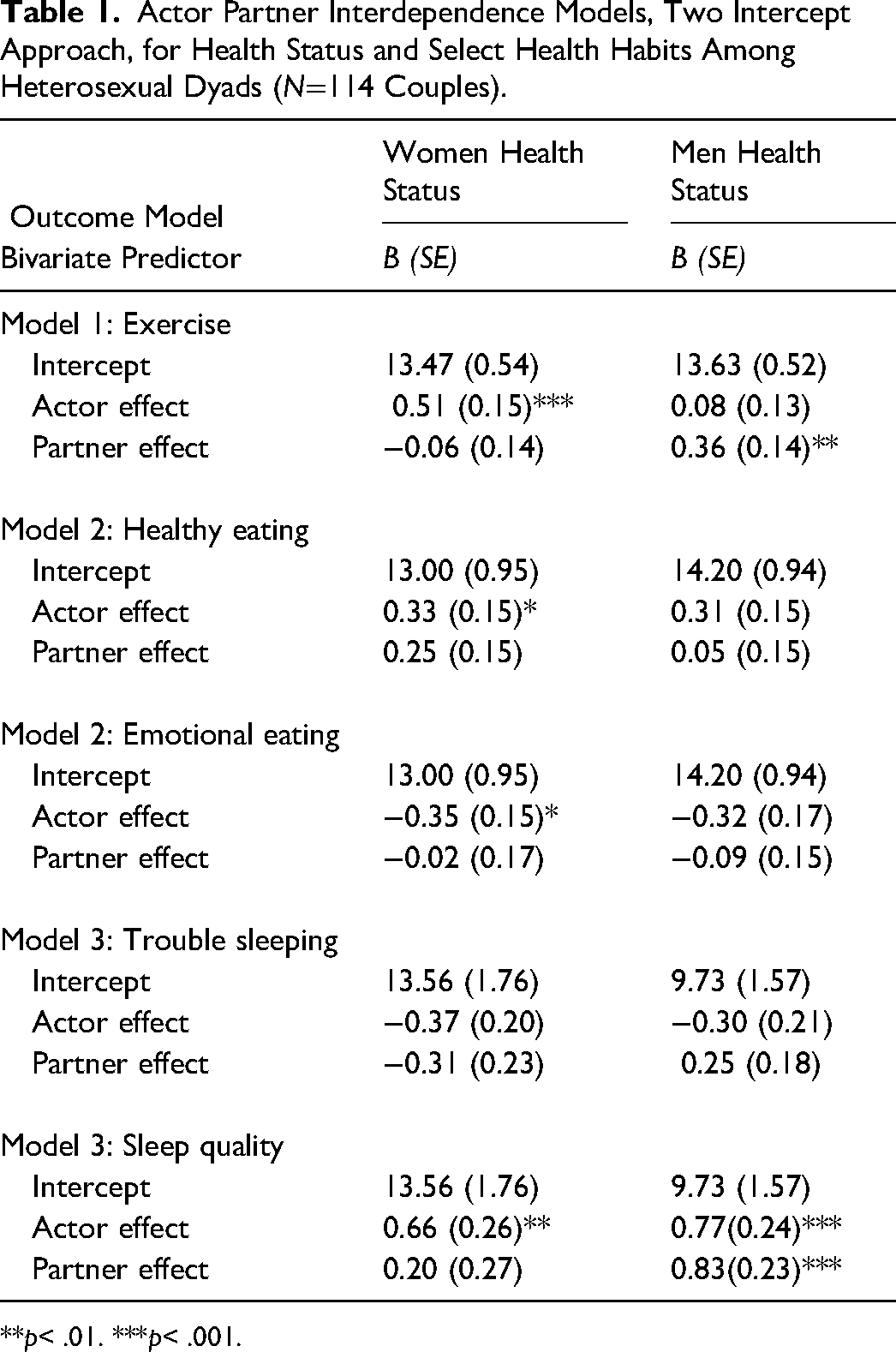
We conducted exploratory analysis to identify if the health habits significantly related to physical health status (i.e., weekend emotional eating, weekday healthy eating, exercise habits, sleep quality, and troubled sleep) exhibited actor/partner effects. We did observe significant or partially significant findings in the bivariate actor partner interdependence models examining exercise and global physical health (tests of distinguishability, χ2 (6) = 11.31, p = .08), the model examining emotional and healthy eating on global physical health (χ2 (10) = 16.75, p = .08), and the sleep quality and trouble sleeping on global physical (χ2 (10) = 17.02, p = .07) model (see Table 1).
Actor Partner Interdependence Models, Two Intercept Approach, for Health Status and Select Health Habits Among Heterosexual Dyads (N=114 Couples).
**p< .01. ***p< .001.
In the model testing exercise habits and global physical, actor-partner effects explained 10.4% of the variance women's scores and 6.7% of the variance for men. The results showed only actor effects (overall actor effects, .29, p = .02, 95% CI: .1, .48) for women (.51, p < .001, 95% CI: .23, 80) and only partner effects (overall partner effects .15, p = .13, 95% CI: −.04, .34) for men (.36, p = .011, 95% CI: .08, .64).
In the model testing emotional and healthy eating on global physical health actor effects explained 15.7% of the variance women's scores and 9.7% of the variance for men. The results showed actor effects (overall actor effects, .32, p = .002, 95% CI: .12, .52) for healthy eating during the week for women (.33, p = .027, 95% CI: .04, .61) and men (.31, p = .042, 95% CI: −.56, −.11). The results showed actor effects (overall actor effects, −.33, p = .003, 95% CI: .12, .52) for emotional eating on the weekends for women (−.35, p = .024, 95% CI: −.65, −.05) and no actor effects for men (−.19, p = .90, 95% CI: −.49, .43). No partner effects were observed for weekday healthy eating or weekend emotional eating on global physical health.
In the model testing trouble sleeping and overall sleep quality on global physical health, actor-partner effects explained 23.4% of the variance in women's scores and 29.7% of the variance for men. We found no main effects for gender for trouble sleeping. The results showed actor effects (overall actor effects β=.72, p < .00, 95% CI: .36, 1.07) for both men (.77, p = .001, 95% CI: .3, 1.25) and women (.66, p = .011, 95% CI: .15, 1.17) but only partner effects (overall partner effects .003, p = .003, 95% CI: 0.17, 0.86) for women to men for overall sleep quality (0.83, p < .001, 95% CI: .37, 1.29).
Discussion
We investigated the relationship between health habits (alcohol, smoking status, exercise, sleep, and diet) and global physical health in stressed couples (mostly middle-aged parents).
Our findings showed weekday healthy eating, weekend emotional eating, regular exercise, trouble sleeping, and sleep quality were related to current health status. While the literature documents these findings, our research links daily healthy habits to a period of high stress in a younger sample (mean age 36.38 years) than previous studies with samples aged 50 years and older (Li et al., 2020; Shan et al., 2020). We did not find alcohol or tobacco use was related to health status. This does not negate the research indicating alcohol (Kiiskinen et al., 2020) and tobacco use predicts health status (Daskalopoulou et al., 2018). Most of our sample used alcohol in moderation (4-day M = 1.59) and very few used tobacco (25/210). We suspect lack of variability explains our observations or because our sample was on average middle aged, possibly tobacco use length has not generated an observable impact on health status (NCI, 2019).
Our findings showed that eating habits were beneficial or harmful depending on when they occurred. Weekday healthy eating may give individuals the energy needed to manage stress associated with daily hassles. Women more frequently engaged in weekend emotional eating. Weekends are a time when many individuals decompress after the work week. Using emotional eating on the weekend could indicate duress remains elevated. Women experience more stress (Kowal et al., 2020) as the pandemic highlighted and created gender inequity (e.g., women managing homeschooling and more childcare, Alon et al., 2020). Women may be using food to cope as an effort to restore their mental health. The societal expectations for women's appearances (Schaefer et al., 2019), may explain why men did not show a relationship between emotional eating and health status. Women may internalize their eating habits more than men and feel worse when they eat unhealthy foods (Boswell & White, 2015). For example, women judging their food choices may lead to depressive symptoms (Boswell & White, 2015). No partner effects were observed for diet. This may show that couples are eating the same foods, thus, experiencing a similar boost in health status when they eat healthy.
As expected, regular exercise was associated with improved physical health status. Gender differences were observed. Unlike men, women's regular exercise was associated with better physical health. Women are more likely to exercise for appearance whereas men for enjoyment, perhaps explaining why women tend to exercise more frequently than men (Craft et al., 2014). Exercise is also used to manage stress and show concern for health. Our results showed when women exercised more, men were more likely to be healthier. Women may be including their partners in their exercise routines (e.g., walks together). Thus, romantic partners may share exercise habits (Perry et al., 2016).
Trouble falling asleep and sleep quality were related to physical health status. Both sleep patterns are barometers for mental health. As mental health is directly linked to health outcomes (Ohrnberger et al., 2017), our findings are expected. No main effects for gender were observed for trouble sleeping to physical health status. Sleep quality was shown to have both actor and partner effects. Both men and women when they had poorer sleep quality experienced worse physical health. When women reported poorer sleep quality, their male partners had poorer physical health. This may be simply explained by environmental exposure (i.e., both partners sleep in the same bed). However, like exercise, we demonstrated a pattern where women's health habits are related to men's physical health without a reciprocal outcome. Previous research (Meyer et al., 2019) demonstrated a similar association where women influence men's health, but men do not influence women's health. These findings could reflect women are more likely to receive support from others not just their romantic partner (McLaughlin et al., 2010). As our sample was mostly parents, our findings may replicate previous research demonstrating women's health linked to their children's wellbeing (Saxbe et al., 2014).
Limitations and Future Research
Our study had limitations. Our sample was not representative of the United States (e.g., race, ethnicity, alcohol, and tobacco use). We only captured a 2-week period and not every day during the pandemic. The pandemic is a unique time and a model of chronic stress. We do not know if conducting this study at another time would show the same outcomes. Finally, our measurements showed multiple concerns. Most of our constructs were measured with one-item which may not accurately encompass the construct. Our stress measure, a sample demographic, only inquired about pandemic distress not other stress types (e.g., work, financial). Additionally, our measures were both daily and long-term assessments. We chose to use long-term measurements for items that may need long-term exposure to affect the person (e.g., smoking; exercise, and sleep quality) and chose short-term measurements for items that may reflect emotional coping (e.g., eating habits and alcohol). The measurement inconsistency inhibits our ability to accurately determine temporal effects. For those items measured long term, we cannot determine if these factors changed since the onset of the pandemic. Additionally, our measures were self-reported, so we cannot determine the veracity of the reports. Finally, our couples were in monogamous, heterosexual relationships. We cannot determine how couples in same-sex or polyamorous relationships may influence health habits.
Our findings need to be replicated. Future research should seek to use more comprehensive instruments to measure health habits and health status (e.g., blood tests and blood pressure). Future research may want to examine the long-term impact of health habits and partner health status. We suspect partner influence may increase as couples age. Lastly, future research should include different types of couples and coupling to learn more about the association between health habits and health status in other types of romantic relationships.
Counseling Implications
Our findings support a holistic approach to counseling intervention. As our results show sleep, diet, and exercise are related to health status, counselors may want to promote health habits in counseling. A host of research supports sleep (Scott et al., 2021), exercise (Singh et al., 2023), and diet (Firth et al., 2020) improves mental health. Thorough assessments of health habits can identify what behaviors may be useful to target in counseling. It is not surprising that one's health habits would be related to health status, but our findings support romantic partners may impact health habits, and when health habits are engaged in long term, then the trajectory of one's health status. As such, couple interventions may be key to promoting health. While many counselors may already inquire about health habits, this approach is often neglected in the context of couples counseling.
When including health habits in couples counseling, counselors need to remember that many couples engage in similar health habits. Many couples eat regular meals together, they go for walks or other forms of exercise together, and often as couples are sharing a bed, they will have similar sleep habits. Using the dyad to support health is an organic approach using a framework that couples already employ.
Our research shows the unique role a female partner plays in influencing her male partner's health habits. This relationship could be utilized for the betterment of both partners. The research already shows health habits are beneficial for mental health, thus it is expected women will receive the benefits of engaging in health habits. If women regulate one's partner's health, then our findings offer empirical support for couples-based health interventions. For example, couples counselors can inquire if health is a concern. If health is a concern, then a systems-adapted orientation for changing health behaviors could be utilized. Motivational Interviewing and Stages of Change are frequently used in counseling. Couples counselors could examine readiness for change and intervene using dyadic motivational interviewing (see Starks et al., 2020) to help cultivate meaningful change across the couple. Targeting symptoms (e.g., ambivalence and motivation) at an interpersonal level could identify behaviors that may be stymieing couple progress. Couples counselors can use the system to eliminate impasses. If both partners acknowledge their role in improving their partner's life, goal achievement may be more easily obtained to create lasting dyadic change.
Conclusion
We demonstrated that health habits, when under chronic stress, are related to physical health among partnered individuals and that women's health habits, specifically exercise and sleep quality, helped bolster men's health status. These results add detail to our understanding of chronic stress and its impact on health habits through the examination of these associations during a time of uniquely high stress, the COVID-19 pandemic. The pandemic, as a chronic stress model, may be applied to other chronic stressors when similar emotions re-experienced by couples (e.g., health concern within one partner). Our results could be used to develop partner-based interventions to reduce stress and improve each partner's health habits with the hope of the relationship emerging from the stressful time in a healthier state.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.