
Abstract
Parental perspectives on childhood disability shape the healthcare experiences and well-being of children and families. Understanding the perspectives of immigrant and refugee parents is essential for providing culturally safe and responsive services, supports, interventions, and plans of care. This integrative review examined how immigrant and refugee parents living in Canada and the United States understand and make meaning of their children's disabilities. A systematic search of seven databases identified 23 studies (22 qualitative, 1 mixed methods) published between 2001 and 2024. Data were analyzed thematically using a lifeworld fractions framework, encompassing selfhood, society, embodiment, temporality, spatiality, project, discourse, and moodedness. Parents drew on multiple cultural and religious frameworks—often blending biomedical, traditional, and spiritual explanations—to interpret their children's disabilities and guide caregiving. Across studies, parents described challenges with language, stigma, and navigating fragmented service systems, yet also expressed resilience, faith, and hope for their children's futures. A lifeworld approach highlights how meanings of disability are embedded in everyday experiences and cultural contexts. This perspective offers healthcare and education professionals a holistic framework for assessment and support, encouraging attention to parents’ lived realities, values, and cultural worldviews to promote equity and trust in care relationships.
Introduction
Globally, approximately 93 million children (5%), experience moderate or severe disability (WHO, 2015). In Canada and the United States, childhood disability rates are 3.7% and 4.3% respectively, with cognitive disability being the most common condition, with one-third of those having two or more disabilities (Miller et al., 2013; Statistics Canada, 2008; Young, 2021). Worldwide prevalence rates of developmental disabilities vary from 2.42% to 17.8% (Marquis et al., 2018; Miller et al., 2013; WHO, 2011; Zablotsky et al., 2019). Children with disabilities—encompassing developmental, intellectual and physical disabilities, chronic medical conditions, and mental health disorders—often experience co-occurring disabilities, mental health and medical conditions; this can increase their risk of psychological dysfunction and can lead to higher rates of mental health service utilization (American Psychological Association, 2013; British Columbia Ministry of Health, 2007). Family caregivers of children with disabilities are also at risk of psychological distress and mental health problems (Marquis et al., 2020).
Immigrants make up 21% of the population of Canada and 15% of the United States (Pison, 2019). In 2020, there were 82.4 million refugees worldwide (42% were children) (UNHCR, 2021). Refugees are individuals who have been forcefully displaced from “their country of origin for reasons of feared persecution, conflict, generalized violence, or other circumstances that have seriously disturbed public order and, as a result, require international protection” (United Nations, n.d.). Immigrants, on the other hand, are individuals who have moved to a new country, irrespective of the reason for migration or legal status (United Nations, n.d.). In 2019, 27,500 refugees settled in the United States and 30,100 in Canada (the highest worldwide) (Statistics Canada, 2017a; UNHCR, 2021). In Canada, 37.5% of children have at least one foreign-born parent and 25% in the United States do (FIFCFS, 2021; Statistics Canada, 2017a, 2017b). Immigrant and refugee—“newcomer”—parents of children with disabilities face particular barriers to securing essential support for their children with disabilities and special health care needs, including: language; financial resources; health and education system complexity; social isolation; racism and discrimination (Bešić & Hochgatterer, 2020; Brassart et al., 2017; Choe et al., 2024; Honey-Arcement, 2016; Jennings et al., 2014; Minhas et al., 2017; Rivard et al., 2019; Zechella & Raval, 2016).
Cultural perceptions between newcomer families and the host country's majority play a role in the diagnosis of disabilities and intervention, which may contribute to barriers and delays in receiving health care and education services for their children with developmental disability (Brassart et al., 2017; Kibria & Becerra, 2021; Minhas et al., 2017; Rivard et al., 2019). Examples include conflicting cultural views on disability and medicine, diagnostic tools biased toward Western norms causing misdiagnosis or delays, overlooking trauma and spirituality, differing beliefs on gender interactions, and gendered caregiving roles. Additional issues include reluctance to question authorities or share challenges, varying perspectives on healthcare as a basic right, stigma around disabilities and mental health, differing parental roles in disability care, and alternative explanatory models of childhood disability and its treatment (Brassart et al., 2017; Honey-Arcement, 2016; Jennings et al., 2014; Minhas et al., 2017; Rivard et al., 2019; Zechella & Raval, 2016).
Service fragmentation in host countries intensifies these barriers for families of children with developmental disabilities, underscoring the need for individualized, culturally attuned approaches. Providers in healthcare, education, and social services must understand newcomer parents’ experiences, cultural beliefs, and values—such as etiology, treatment, and parental roles—and directly ask about terms for disability, causality, priorities, and treatment expectations (Bešić & Hochgatterer, 2020; Brassart et al., 2017; Minhas et al., 2017; Zechella & Raval, 2016). Studies have indicated the potential value of support groups for parents to camaraderie with other newcomers (Bešić & Hochgatterer, 2020; Honey-Arcement, 2016). At the same time, it is essential to avoid treating newcomers as a homogenous group, and thus an individualized approach is required for service providers to provide culturally appropriate support to parents of children with disabilities (Brassart et al., 2017; Jennings et al., 2014; Minhas et al., 2017; Zechella & Raval, 2016). To provide effective health services, it is essential to understand the mosaic of meanings that newcomer parents ascribe to their experiences of raising and providing care for their children with disabilities. Understanding these perspectives is also essential for advancing health equity and dismantling systemic barriers within care systems.
Significant knowledge gaps still exist on how these parents deal with difficulties presented by raising children with disabilities, despite the expanding body of research on newcomer families (Bešić & Hochgatterer, 2020; Brassart et al., 2017; Honey-Arcement, 2016; Jennings et al., 2014; Minhas et al., 2017; Rivard et al., 2019; Zechella & Raval, 2016). There is a lack of research on how newcomer parents draw on cultural frames of reference from their home countries and the host society to adapt to these challenges. There is a need to synthesize the literature on how these parents construct, conceptualize, assign, and negotiate these meanings across intersecting worldviews. Applying a holistic phenomenological lens to explore the everyday, embodied, and relational dimensions of these experiences across cultural contexts has the potential to inform culturally responsive practice.
The aim of this integrative review was to synthesize existing research on the meaning-making of childhood disability among newcomer parents, focusing on how newcomer parents navigate and integrate cultural frames of reference from their countries of origin and settlement. Such understandings are essential for practices and policies that promote inclusivity and equity in social services, education, and health. By exploring this intersection, the study seeks to identify patterns using Ashworth's (2016) lifeworld approach as a guide to inform culturally responsive practices and highlight opportunities for improved support.
Methods
To examine how newcomer parents make meaning of childhood disability, we employed an integrative review design, allowing for the inclusion of studies with diverse methodological approaches in the published literature. We followed guidance from Toronto and Remington (2020) and Whittemore and Knafl (2005) on conducting an integrative review, which involves synthesizing empirical studies to gain a comprehensive understanding of the phenomenon, through a systematic search, data analysis and interpretation. The review process is reported in accordance with PRISMA guidelines (Page et al., 2021), adapted for integrative review methodology. A search of seven electronic databases relevant to health, nursing, culture, rehabilitation, and social sciences (Academic Search Complete, Anthropology Plus, CINAHL, MEDLINE, PsychINFO, SCOPUS, and Sociological Abstracts) for papers published from January 2001 to December 2024 yielded 618 records (see Figure 1). Search terms were developed iteratively and combined using Boolean operators. Core search concepts included [refugees OR immigrant] AND [children with disabilities OR disabled children], with database-specific headings applied where available. A hand search of reference lists of articles included after full-text reviewed yielded no additional articles for inclusion.

PRISMA flow diagram.
Studies were included if they met the following criteria: focused on parents or primary caregivers of children with disabilities; examined how disability was understood, interpreted, or given meaning, either explicitly or implicitly; included immigrant and/or refugee families; used qualitative, quantitative, mixed-methods, or review approaches with extractable findings that substantively explored the meaning of childhood disability and incorporated newcomer parents’ experiences and viewpoints; and were published in English (for feasibility). Studies were excluded if they: did not address parental perspectives or meaning-making processes (e.g., focused exclusively on professional, policy, or service outcomes without parental narratives); were not peer-reviewed publications or doctoral-level dissertations; examined settlement outside Canada or the United States; or were not published in English.
Titles and abstracts of all records identified through the database search were screened against the inclusion criteria (A.C.), with secondary screening of non-obvious cases conducted by a second reviewer (E.M.). Duplicate records were removed. Word processing and spreadsheet software were employed for data management. Full-text screening was then conducted to determine final eligibility (A.C. and E.M.). Discrepancies were resolved through discussion until consensus was reached. Methodological quality was appraised to support interpretive rigor rather than to exclude studies on the basis of design. Each included study was assessed for relevance of findings to the research question. A data extraction matrix was piloted and refined (A.C., E.M.) which focused on study characteristics (author, year, country, participant characteristics, disability type, and methodology) and relevant findings (A.C.), and the extracted findings were read repeatedly to identify patterns of meaning across studies (A.C., E.M.). Data were analyzed using a deductive, inductive, and interpretive thematic synthesis. Initial codes were generated and iteratively refined through constant comparison, allowing similarities and differences across cultural, social, and contextual settings to be examined. Appraisal emphasized conceptual and interpretive contribution rather than methodological scoring. Themes were refined through team discussion to ensure coherence, depth, and analytic transparency (E.M., A.C., O.G.) and a final synthesis and interpretation (E.M., A.C., J.G., S.A., O.G.) reflecting in vivo and theoretical relevance.
Data analysis and interpretation were informed by Ashworth's (2016) description of the lifeworld—the total subjective experience of a phenomenon, comprising interrelated aspects of meaning. Drawing on phenomenological philosophy and psychology, Ashworth described eight interpenetrating fractions of the lifeworld: selfhood, society, embodiment, temporality, spatiality, project, discourse, and moodedness. Each fraction is intrinsically tied to human experience. Incorporating these dimensions in the integrative review process enhances the richness and contextual depth of the qualitative data analysis, regardless of the study's specific focus. To further interpret sociality, spatiality, temporality, and project, we drew on Mattingly's (2014) notion of the moral laboratories and the good life, which illustrates how parents of children with serious chronic conditions engage in ethical projects of care as they strive to transform their shifting social and physical surroundings so their children can flourish and thrive.
Results
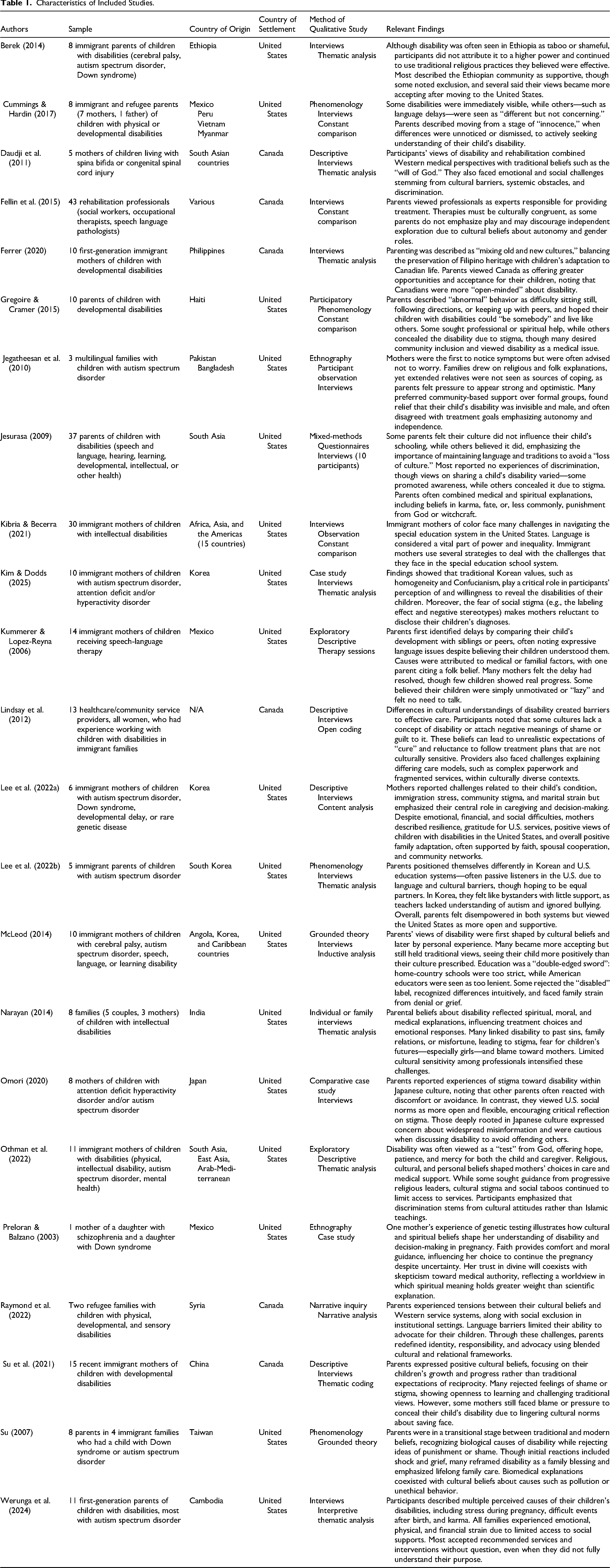
Of the 23 studies reviewed, 22 used qualitative designs and 1 employed mixed methods; seven were doctoral dissertations. Studies were conducted in Canada (n = 6) and the United States (n = 17), with participants originating from many countries, primarily from the Global South, including regions across South, Southeast, and East Asia, the Arab–Mediterranean, Africa, and Latin America (see Table 1). Analysis of the 23 included studies and initial coding generated 59 codes which were regrouped into 16 themes and 35 subthemes according to Ashworth's (2016) eight aspects of the lifeworld (see Table 2). These illuminate how parents construct meaning and respond to childhood disability within intersecting cultural and structural contexts.
Characteristics of Included Studies.
Integrative Review Lifeworld Aspects, Fractions, Themes, and Subthemes.

Temporality
Temporality concerns the starting point of an experience, its conclusion, and how it is bound with past experiences (Ashworth, 2016). Parents’ understandings of childhood disability are often shaped by perceived causes and anticipated trajectories. Included in this lifeworld fraction are themes of parents’ understanding of causes of disability (natural, supernatural), relative permanence and curability of disability (disability as temporary), and their visions of a better future for the child and themselves (barriers to education and marriage, ongoing need for support). In several studies, parents described the cause of their child's disability as genetic, biological, natural and rooted in the body, including medical events, reported physician's neglect, premature birth, seizures, family history or heredity (Berek, 2014; Gregoire & Cramer, 2015; Jesurasa, 2009; Kummerer & Lopez-Reyna, 2006; Othman et al., 2022).
Across several studies, parents also made reference to beliefs that supernatural influences had caused their children's disabilities (e.g., Berek, 2014; Daudji et al., 2011; Gregoire & Cramer, 2015; Kummerer & Lopez-Reyna, 2006; Narayan, 2014; Othman et al., 2022; Preloran & Balzano, 2003). While some spoke of a curse (Berek, 2014) or a folk belief (e.g., cutting of hair too early) (Kummerer & Lopez-Reyna, 2006). Most understandings were related to religious beliefs that disability came from God. Parents stated that disability was the will of God, and some believed they had been gifted or specially chosen to care for a child with a disability (Daudji et al., 2011; Narayan, 2014). In some cases, child disability was reportedly viewed as a result of sins committed in the past or a past life (Narayan, 2014; Werunga et al., 2024). Some parents were aware of supernatural beliefs, but did not hold them personally (Berek, 2014; Su, 2007).
Some studies noted that newcomer parents saw disability as temporary and curable, particularly by medical intervention in the settlement country (Daudji et al., 2011; Lindsay et al., 2012). When envisioning the future, some parents described disability as a barrier to accessing education, employment and marriage, particularly for girls with disabilities, due to discrimination (Daudji et al., 2011), even impacting a non-disabled sibling's prospects (Su, 2007). Parents in several studies anticipated an ongoing need for support for their child, describing concern for their children's future, including worries and pessimism about their ability to succeed, dependency on others, and capacity to care for themselves if the caregiving parent died (Gregoire & Cramer, 2015; Kibria & Becerra, 2021; McLeod, 2014; Narayan, 2014; Othman et al., 2022).
Selfhood
Selfhood concerns social identity and a person's sense of agency, presence and voice in a situation (Ashworth, 2016). Themes related to parents’ social identity, agency, and presence encompass challenges such as language barriers, lack of understanding of their child's diagnosis and treatment, and a deference to authority, characterized by reluctance to question or challenge healthcare professionals, who are perceived as experts (Cummings & Hardin, 2017; Ferrer, 2020; Gregoire & Cramer, 2015; Lindsay et al., 2012; Narayan, 2014; Raymond et al., 2022).
Language difficulties impact immigrant parents' social identity and sense of agency. According to Ashworth (2016), agency refers to a person's ability to act intentionally and influence their environment. For newcomer parents, language difficulties can significantly impact their lifeworld by constraining their ability to fully engage with their new social environment. Language barriers and absence of translation and interpretation services for newcomer parents of children with complex needs limit their access to information and ability to collaborate with service providers (Raymond et al., 2022). Medical jargon and diagnostic language made it particularly difficult for newcomer parents when communicating with their healthcare providers (Cummings & Hardin, 2017; Lindsay et al., 2012). This often prevented parents from engaging fully in their child's health care and education, leading to dissatisfaction with care, and miscommunication (Gregoire & Cramer, 2015; Jegatheesan et al., 2010; Kibria & Becerra, 2021). Some newcomer parents could not fully participate in the process of the childhood disability diagnosis and support planning and did not fully grasp the diagnosis or the services (Gregoire & Cramer, 2015; Jegatheesan et al., 2010; Werunga et al., 2024). The lack of clear and complete understanding of the child's diagnosis undermines the parent's agency in the situation.
Some healthcare and education professionals reported that newcomer parents saw them as experts who are not to be judged or questioned, even though the professionals wanted to place the expertise back in the hands of the parents (Cummings & Hardin, 2017; Fellin et al., 2015; Lindsay et al., 2012). Some parents described avoiding complaining about the services their children received, citing a sense of obligation to accept the care they were given, and possibly due to respect for authority (Berek, 2014). Lee et al. (2022a) noted that most parents felt unknowledgeable and assumed the position of listeners and receivers due to language and cultural differences. Another study maintained that immigrant mothers tended to minimize conflicts with their children's special education school system to avoid retribution (Kibria & Becerra, 2021).
Sociality
Sociality concerns how others are implicated in an experience, and how a situation affects relations with others (Ashworth, 2016). For newcomer parents, the meaning of childhood disability centered on interpersonal influences, social interactions, and connections, with key themes including relational aspects (disability and siblings, family ties), ethnic community support, social perceptions (respect, normality), and stigma (family blame, hiding children with disabilities). Childhood disability was impacted by family members and the social environment. In many studies, child's disability was often contextualized by their siblings, who served as a comparator, a source of socialization for the child with a disability, and a source of support for parents (Gregoire & Cramer, 2015; Kummerer & Lopez-Reyna, 2006; Su, 2007). Siblings were sometimes considered in the disabled child's plan of care by health professionals (Fellin et al., 2015; Lindsay et al., 2012). Parents often spoke of the need to seek emotional and practical support from other family members and community members, particularly during times of overwhelm (Daudji et al., 2011; Gregoire & Cramer, 2015; Omori, 2020).
In some cases, a lack of family support was felt deeply (Ferrer, 2020). For some parents, seeking support from others was a matter of honor, to be kept secret or within the family to avoid shame from outsiders or diminished social standing (Ferrer, 2020; McLeod, 2014). Some parents chose to avoid rather than seek familial support and rely on unrelated supporters (Ferrer, 2020), at times to prevent older family members from worry (Jegatheesan et al., 2010). Sometimes parents reported they relied on networking. For example, parents in Jegatheesan et al. (2010) reported networking within their own ethnic community to find information and support for their children (Berek, 2014; Jegatheesan et al., 2010).
The word “normal” was often used by parents both to describe their children's behavior, particularly when assessing their ability to function independently within the household, as well as in comparison to children with more significant impairments (Gregoire & Cramer, 2015). In some cases, perceived normality—difference but not concerning—led to a delay in diagnosis (Cummings & Hardin, 2017; Lee et al., 2022b), at times because the norms of parents’ home cultures were often more relaxed and allowed for more diversity (Jegatheesan et al., 2010; Kummerer & Lopez-Reyna, 2006).
Some parents emphasized they expected their children to be seen as respectful, demonstrating proper comportment and appropriate behavior (towards Elders, in religious settings), and this could be a struggle (Ferrer, 2020; Omori, 2020; Othman et al., 2022). Several studies noted that parents were blamed and isolated for their children's disabilities, and for keeping the child (Berek, 2014; Daudji et al., 2011) and others described the need to hide or otherwise justify a child's behavior or disability, by not disclosing the diagnosis, or keeping the child from public spaces, fearful of displays of disability (e.g., difficult behaviors), to preserve reputation and avoid shame and rejection (Berek, 2014; Gregoire & Cramer, 2015; Jesurasa, 2009; Narayan, 2014; Othman et al., 2022; Su et al., 2021). The stigma associated with children's disability often caused significant distress for parents as well (Daudji et al., 2011).
Spatiality
Spatiality concerns a person's picture of the geography of the places they need to go to and act within the social norms of, affected by the situation (Ashworth, 2016). With regards to physical and social spaces, both geography and social norms, features of spatiality were implicated in the meanings of childhood disability for newcomer parents. Physical space did not arise as a theme in the literature reviewed, while social spaces and norms figured largely. Newcomer parents noted that government support in their settlement country, including laws, funding, programs, and policies that protect the rights of people with disabilities (Berek, 2014; Daudji et al., 2011; Ferrer, 2020; Su et al., 2021). The themes under this fraction focus on cultural influences and norms related to having a child with a disability such as mixing cultures, cultural versus individual, cultural clashes, and rejecting cultures. Parents in several studies expressed the tendency to mix, blend, or simultaneously hold Western and non-Western or traditional beliefs around disability and rehabilitation, and child-rearing practices.
Often parents were willing to take several approaches to care simultaneously, using both Western and non-Western forms of medicine, believing in the effectiveness of both biomedical interventions offered by professionals and also in spiritual healing and prayer (Berek, 2014). Thus, these forms of culturally-sanctioned treatment are not mutually exclusive. In some studies, acculturation was found to impact parents’ beliefs, as they slowly adopt Western beliefs and become more accepting of mainstream understandings of disability, this was specifically evident among younger generations (e.g., Daudji et al., 2011; Othman et al., 2022).
Participants in several studies described how their cultural understandings of disability were overturned by the individual lived experience of caring for a child with a disability (e.g., McLeod, 2014). Nevertheless, several studies examined times when Western and home cultures were placed at odds with each other, such as parents holding different perspectives than professionals, related to educational interventions, speaking multiple languages, and the expectation of parental involvement in children's education (e.g., Jegatheesan et al., 2010; Omori 2020). Cultural clashes sometimes led to parents choosing to reject and distance themselves from their home cultures (Omori, 2020; Su, 2007). For example, a parent in Berek (2014) described how they began to distance themselves from their ethnic community because of the stigma their daughter experienced.
Embodiment
Embodiment concerns how the situation relates to feelings about one's own body, including gender, “disabilities,” and emotions (Ashworth, 2016). The way one's body is related to the experience is typically a significant thread in first-person accounts of disability. Newcomer parents’ descriptions of embodiment in relation to childhood disability focused on gender, disability and emotion. Themes included blaming the mother and collective suffering. In several studies, mothers reported being blamed for giving birth to a child with a disability. They were implicated biologically and ethically, and in terms of gestational health and behavior, as well as genetic links as causes of child disability (e.g., Narayan, 2014; Su, 2007; Su et al., 2021).
The mother's stress during immigration and gestational diabetes were sometimes reported as connected to disability (e.g., Jegatheesan et al., 2010; Narayan, 2014). While not necessarily the cause, the mother's body was still blamed for the child's disability. Newcomer mothers’ behaviors before or during pregnancy were sometimes blamed for children's disabilities; these varied from taking medication, traveling, and past sins, or religious non-adherence (Jegatheesan et al., 2010; Narayan, 2014; Preloran & Balzano, 2003). Children's disabilities were sometimes attributed to genetics, especially when a child inherited a disability that their mother also had (e.g., Narayan, 2014).
Studies also highlighted the negative impact of stigma on the health of the newcomer parents of children with disabilities. We refer to this as “collective suffering” to emphasize how parents “took on” the suffering their children were experiencing. Authors described how sometimes mothers need to assuage their children's suffering, to protect them from further suffering, which was at times emotionally distressing and led to health deterioration for newcomer parents (Daudji et al., 2011; Ferrer, 2020; Gregoire & Cramer, 2015).
Moodedness
Moodedness concerns the feeling-tone and atmosphere of a situation or experience (Ashworth, 2016). Closely related to embodiment, the affective aspect—or facet of moodedness—of childhood disability experience for newcomer parents is represented by the themes of initial reactions and hope in participant reports. Parents often expressed disbelief and anxiety upon hearing their child's diagnosis, stating that the label was inappropriate or not serious (e.g., Berek, 2014; Daudji et al., 2011; Kim & Dodds, 2025; Lee et al., 2022b). Other common emotions included hurt, pain, confusion, hopelessness, shock, grief, depression, and anxiety (Berek, 2014; Gregoire & Cramer, 2015; Jegatheesan et al., 2010; McLeod, 2014; Narayan, 2014; Othman et al., 2022; Preloran & Balzano, 2003; Su, 2007; Su et al., 2021).
Although initial reactions to a child's diagnosis tended to be negative, parents often described hope for the future as a significant aspect of their experiences, the sources of which were both biomedical and traditional interventions, and support from family and disability specialists (e.g., Daudji et al., 2011; Narayan, 2014). Hope was often framed in the hope of attaining “normalcy” or hoping that a child's disability would “resolve” (Daudji et al., 2011). Together, these emotions illustrate how parents’ affective experiences are intertwined with faith, stigma, and hope.
Discourse
Discourse describes the organized ways that cultural forms, language, symbols, and communication techniques convey and mold meaning in a certain social or cultural setting (Ashworth, 2016). In this theme, language both expresses and shapes the meaning of disability. Newcomer parent reports of childhood disability were shaped by different discourses of disability, particularly the ways used for classifying disability. The themes in this lifeworld facet included rejection of labeling, mental versus physical, and disability as a problem.
In the diagnostic process, some parents were uncomfortable with terms and labels used. They were particularly concerned about the implications of illness, deficit and disorder. Some parents rejected both the words and the diagnosis itself (e.g., Berek, 2014; Daudji et al., 2011; Lindsay et al., 2012). In some of the reviewed studies, mental disability was conceptualized as more severe and troubling than physical disability, and carrying greater stigma (e.g., Othman et al., 2022). In contrast, one study found that newcomer parents often expressed gratitude that their children's disabilities were not physically apparent, implying that visibility, not physicality, was their main concern (Jegatheesan et al., 2010).
In general, much of the discourse around children's disabilities in the studies of newcomer parents was built on the view that disability is a problem or a difficulty that one encounters, entailing challenges in occupational and social functioning, stigma, and unwanted visibility (e.g., Gregoire & Cramer, 2015; McLeod, 2014; Narayan, 2014). Language of disability discourse appears restrictive to newcomer parents. Terms like mental disability or diagnostic labels may reflect a clash between their lifeworld (cultural and personal values) and the imposed medical discourse. This mismatch shapes their emotional and cognitive experience of navigating the diagnosis and treatment process.
Project
Project concerns how a situation relates to the person's ability to carry out the activities they are committed to and which they regard as central (Ashworth, 2016). A substantial facet of the lifeworlds of newcomer parents of children with disabilities was that of project. Two primary activities stood out and were considered central to their experiences: coping (strengths of the child, purposefully, not hiding faith) and treatment (goals of treatment, negative views of Western treatment, traditional treatment, prayer).
Many studies noted how parents coped with the stigma and difficulties of raising a child with a disability. Parents in several studies emphasized the importance of focusing on their child's strengths as a coping mechanism and wished that schools and cultural beliefs would adopt a similar approach (e.g., Berek, 2014; Daudji et al., 2011; Preloran & Balzano, 2003). Parents in several studies spoke of the active choice to not hide a child's disability—even to share about it—as a strategy for accessing support and encouraging acceptance for disabilities at large and lessening taboo (e.g., Berek, 2014; Gregoire & Cramer, 2015; Jesurasa, 2009; Omori, 2020). Some parents noted that actively hiding their child's disability took too much effort (Omori, 2020; Su et al., 2021). A frequently noted coping mechanism for parents was faith which provided comfort and peace, through religious social structures and both emotional and practical support (Berek, 2014; Cummings & Hardin, 2017; Daudji et al., 2011; Gregoire & Cramer, 2015; Narayan, 2014; Othman et al., 2022; Preloran & Balzano, 2003).
Another aspect of this realm was general and specific treatment goals of newcomer parents for their children with disabilities. Some parents wanted their children to be cured or completely healed (Berek, 2014; Gregoire & Cramer, 2015; Lindsay et al., 2012; McLeod, 2014; Narayan, 2014). Sometimes Western professionals’ treatment goals (e.g., to speak only English at home, to be independent at tasks) were at odds with the parent's goals (Fellin et al., 2015; Jegatheesan et al., 2010; Jesurasa, 2009).
The difference between clinician and parental goals for treatment was sometimes based on underlying philosophy; mothers in Jegatheesan et al. (2010), for example, did not understand the concept of play-based language intervention or increasing autonomy, and thus struggled to put such forms of treatment into place. In several studies, parents described negative views of Western treatment and goals of treatment they perceived were “pampering” their children, and could prevent them from reaching their potentials (Berek, 2014; Gregoire & Cramer, 2015; Kummerer & Lopez-Reyna, 2006; McLeod, 2014). Other parents felt that pampering or nurturing was an important way to treat one's child (e.g., Ferrer, 2020). Some studies reported newcomer parents generally disagreed with or mistrusted Western treatment, such as speech therapy and complex diagnostic processes (e.g., Berek, 2014).
Parents in several studies described actively looking for traditional, non-Western treatments (e.g., holy water, folk treatments, consulting Elders, prayer) for their children, with the proportional significance of each approach varying among individuals (e.g., Berek, 2014; Jegatheesn et al., 2010). Prayer was a frequently cited avenue for newcomer parents to cope with or treat childhood disabilities (Berek, 2014; Daudji et al., 2011; Gregoire & Cramer, 2015; Narayan, 2014).
Across 23 studies, eight interconnected lifeworld aspects illuminated how immigrant and refugee parents understand and respond to childhood disability. Common threads included faith-based interpretations of causality, the negotiation of stigma and language barriers, and blending of cultural and biomedical frameworks. Across all lifeworld aspects, parents’ experiences reflected both struggle and adaptation. The interplay of cultural frameworks, social relationships, and personal agency reveals how newcomer parents reconstruct meanings of disability through lived experience. These patterns reveal how meaning-making is relational, adaptive, and situated within parents’ everyday efforts to ensure their children's well-being.
Discussion
This integrative review synthesized 23 studies to identify how newcomer parents in Canada and the United States understand and experience childhood disability. Using Ashworth's (2016) lifeworld framework, we organized the data according to eight aspects of experience, revealing how parents navigate and integrate multiple cultural, religious, and biomedical worldviews. We were interested in how newcomer parents weave meanings from the cultural frames of reference from their home country and country of settlement to adapt to their experiences of childhood disability. The studies reported on experiences of immigrants and refugees from diverse cultures and countries of origin. Themes and subthemes within the fractions noted commonalities and differences in their experiences. Across diverse cultural contexts, a consistent pattern emerged: parents construct meaning through both continuity and transformation of their home and host cultural values as they care for their children. They drew on ideas and approaches to childhood disability from both mainstream and traditional sources.
The causes of disability, social experiences, and chosen interventions—which roughly align with past, present, and future features of experience—were predominant themes across the fractions. We can further understand newcomer parents’ experiences by referring to Mattingly's (2014) proposal that parents of children with chronic conditions embark on an ethical project of creating a good life for their children in which they flourish and thrive, an “unexpected and unwanted project of becoming” (p. 5). Mattingly asserts these are moral projects that involve influencing their social surroundings and constructing communities of care. Health, education, and rehabilitation professionals can frame newcomer parents’ use of a medley of explanations for disability and treatments as a strategy for understanding and responding to their children's needs. The project of parenting and caring for a child with unique qualities and impairments necessitates drawing on what may seem like contradictory ideas and varied supports. Studies have shown that parents of children with disabilities across diverse contexts draw on a combination of cultural, social, traditional, spiritual, religious, and biomedical beliefs and practices as they seek to explain and manage childhood disability (Cologon, 2016; Jalil et al., 2025; Landry et al., 2015; Thomas, 2024). By taking a lifeworld approach to assessment, professionals can better understand and appreciate how newcomer parents make sense of and give meaning to their experiences, as they draw on diverse discourses, to cope with the impact that childhood disability has on their sense of self, social location, and purpose.
Previous reviews have advanced understanding of immigrant and refugee families’ experiences raising children with disabilities. Most have emphasized structural barriers, cultural competence, or service-use frameworks to describe stressors, adaptation, or systemic inequities (e.g., Bhayana & Bhayana, 2018; Khanlou et al., 2015; McKay, 2019), rather than parents’ interpretations of disability through moral, spiritual, religious and cultural frames. Recent work by Imanpour et al. (2025) described Afghan and Iranian immigrant fathers’ feelings of disorientation and loss when navigating autism services, describing how cultural and systemic barriers hinder equal access. Their findings are like our review's observation that newcomer parents experience disruption and moral tension as they reconcile home and host cultural expectations of disability and care. However, whereas Imanpour et al. frame these challenges largely in terms of service access and equity, the lifeworld approach applied in this review reveals how such experiences are also moral and existential, reflecting parents’ efforts to sustain identity, belonging, and hope across intersecting cultural worlds. Using Ashworth's (2016) lifeworld framework, we illuminate how newcomer parents actively construct meaning across intersecting cultural and biomedical worlds in their everyday care practices. Through this lens, parents' varied and sometimes contradictory beliefs emerge not as inconsistencies but as adaptive strategies for sustaining identity, belonging, and hope within plural cultural contexts.
While family-centered care models promoted by professional associations emphasize partnership with diverse children, youth, and their families—inclusive of those with disabilities—a lifeworld approach deepens these concepts by situating parents’ understandings within their intrapersonal and sociocultural contexts. For example, the Canadian Paediatric Society practice point advises providers to “assess each patient's understanding of their health condition, it's causes and potential treatments” (Ladha et al., 2018, p. 66). Similarly, the American Academy of Pediatrics (2012) policy states providers should “unequivocally convey respect for families’ unique insights into and understanding of their child's behavior and needs [and] actively seek out their observations” (p. 399). These guidelines oblige professionals to seek to understand the perspectives of families; however, they do not explicate how to thoroughly and holistically conduct that assessment, and how to reconcile a parent's mosaic of understandings of disability (e.g., causality, project) in the context of a complete lifeworld of experience.
Clinical guidance for working with newcomer families often frames cultural difference instrumentally—approaching it as a set of barriers or variables to manage—rather than as an embodied and existential experience. Recent scholarship emphasizes the importance of developing assessment and intervention approaches that are both culturally and contextually responsive and that actively engage families. For example, autism spectrum disorder diagnostic tools are needed that reflect sensitivity to families’ cultural, religious, and linguistic backgrounds are essential for ensuring service accessibility, and meaningful parental involvement during assessment enables professionals to interpret a child's behaviors within the family's cultural frame of reference (Davenport et al., 2018; de Leeuw et al., 2020; Papoudi et al., 2021). Building on this, family-centered and culturally engaged disability assessment approaches informed by the lifeworld perspective can deepen professionals’ understanding of how newcomer families make sense of disability, honoring their unique values and ontologies, and avoid a homogenizing approach. Future research could explore operationalizing the lifeworld fractions into assessment tools.
Ashworth's (2016) lifeworld fraction framework has been used in disability research. For example, Andrews et al. (2019), Hebblewhite et al. (2020), and Redmore (2024) demonstrated the potential of Ashworth's (2016) lifeworld fractions as a methodological and analytical framework for inclusive, qualitative inquiry to understand the experiences of adults who live with autism spectrum disorder, intellectual disabilities, and profound learning disabilities. Their work illustrates how a lifeworld perspective can capture lived experience in contexts of disability. To our knowledge, no prior study has applied Ashworth's lifeworld fractions to the experiences of newcomer parents raising children with disabilities or suggested the use of this framework as a potential assessment tool for populations or families.
Limitations
This integrative review was limited to published, English-language studies conducted in Canada and the United States, which may restrict the transferability of findings to other settlement contexts and linguistic communities. The reviewed literature did not address the experiences of Canadians and Americans migrating to the global south. Gray literature, community reports, and unpublished studies were not included, potentially omitting valuable community-based or practice-oriented insights. Investigation of childhood disability experiences and meanings from the perspectives of children and youth themselves is needed. The analysis relied on the interpretations of primary authors rather than reanalysis of original data, which may have constrained the depth of lifeworld exploration across diverse cultural settings. Furthermore, most included studies focused on mothers, leaving fathers’ and extended family members’ perspectives underrepresented. Experiences of different immigration pathways (e.g., refugees vs. economic immigrants) and intersecting social positions such as socioeconomic status, education, or religion were rarely distinguished. Finally, while the lifeworld framework provided a rich lens for synthesis, some aspects—particularly spatiality and physical embodiment—were less developed in the included studies and warrant further empirical exploration.
Conclusion
This integrative review used Ashworth's (2016) lifeworld framework to examine how immigrant and refugee parents conceptualize and respond to childhood disability in Canada and the United States. The findings show that parents draw on multiple cultural, religious, and biomedical frameworks to interpret their children's disabilities, navigating between worlds of meaning while striving to ensure their children's well-being. Experiences of language barriers, stigma, and fragmented systems coexist with expressions of faith, resilience, and hope. The reviewed studies of newcomers to Canada and the United States reported that biomedical and traditional beliefs about childhood disability can be both complementary and contradictory. This can lead to a complex variety of challenges for parents within themselves, their families and the health care and rehabilitation systems. By illuminating how parents construct meaning across intersecting lifeworlds, this study extends understandings of cultural safety and family-centered care. The lifeworld fractions framework offers providers a tool for holistic assessment and dialogue that values parents’ lived realities, cultural knowledge, and moral agency. Integrating this approach into health, education, and social service systems can foster more equitable and responsive care relationships by prioritizing parents’ lived experience and empowering families in their child's care. Future research should explore how the lifeworld perspective can be operationalized in practice—through co-designed assessment tools, training for practitioners, and policy frameworks that recognize every family's way of making sense of disability holds insight essential to improving systems of care.
Footnotes
Author Contributions
Conceputalization, methodology and supervision: EM, JG, SA. Formal analysis, investigation, writing (original draft, review, and editing): EM, JG, AC, SA, OG.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.