
Abstract
Aims
Primary effusion lymphoma (PEL) is an aggressive, human herpesvirus 8 (HHV8)-associated large B-cell lymphoma characterised by malignant effusions in serous cavities (classic PEL). However, a subset of tumours may present exclusively as solid masses, referred to as extracavitary primary effusion lymphoma (EC-PEL). Despite the high regional prevalence of human immunodeficiency virus (HIV) and Kaposi sarcoma-associated virus /HHV8, PEL is likely under-reported in Sub-Saharan Africa. This study reports on the clinicopathologic features and differential diagnoses of EC-PEL.
Methods
A retrospective review of biopsies with a diagnosis of PEL from 2010 to 2019 was performed. Seven patients met the 2024 WHO criteria for PEL. Clinical information was collected and histopathological and immunohistochemical features were reviewed independently.
Results
Seven patients with a median age of 38 years (range, 25-51 years) were identified. Most patients were men (86%), and all were Black African. Five patients (71%) were living with HIV, with CD4 + counts ranging from 137 to 348 cells/µL. Tumour sites were lymph nodes, stomach, maxillary sinus, and soft tissue. All tumours showed diffuse sheets of plasmablastic or immunoblastic cells. Immunohistochemistry showed expression of plasma-cell markers (VS38C, CD138), lacked pan B-cell markers (CD20 and PAX5), and had high proliferative indices (Ki-67: 90-95%). All tumours were positive for HHV8 (LANA-1) and EBER in situ hybridisation was positive in 86%.
Conclusion
Extracavitary PEL in Sub-Saharan Africa exhibits the characteristic clinicopathologic profile described globally and remains strongly associated with HIV-related immunosuppression. Improved recognition of this rare but aggressive lymphoma can be achieved with increased awareness of the diagnosis and improved access to HHV8 immunohistochemistry.
Keywords
Introduction
Primary effusion lymphoma (PEL) is an aggressive large B-cell non-Hodgkin lymphoma that typically exhibits as lymphomatous effusions within the pleural, peritoneal, or pericardial cavities, with no detectable solid tumour mass.1,2 PEL primarily occurs in young to middle-aged male adults with advanced immunodeficiency, predominantly induced by human immunodeficiency virus (HIV) infection. 3 The lymphoma has also been observed in elderly and immunodeficient patients including solid organ transplant recipients, among others. PEL is universally associated with human herpesvirus 8/ Kaposi sarcoma-associated herpesvirus (HHV8/KSHV) infection which plays a role lymphomagenesis by encoding latent proteins that induce cell proliferation and inhibit apoptosis.1,4,5
An extracavitary solid variant termed extracavitary primary effusion lymphoma (EC-PEL), presents as nodal or extranodal solid masses in the absence of serous effusions.6–10 Although initially described as a secondary manifestation of conventional PEL, EC-PEL is now recognised as a distinct clinicopathologic variant. This differs from classic PEL in its clinical presentation and may present significant diagnostic challenges due to its solid, mass-forming growth patterns.1,6,7
Morphologically, EC-PEL demonstrates diffuse proliferation of large atypical lymphoid cells with immunoblastic, plasmablastic, or anaplastic features.1,11 The tumour cells typically lack pan B-cell markers and instead express markers of terminal B-cell/plasmablastic differentiation.4,12 Demonstration of HHV8 infection by nuclear staining for latent nuclear antigen-1 (LANA-1) is critical for diagnosis. 1 Epstein-Barr virus (EBV) co-infection is common, although its pathogenetic role remains uncertain and remains the subject of ongoing investigation.4,13–15 EBV-negative PELs usually occur in elderly HIV-negative patients from HHV8-endemic areas such as the Mediterranean.16,17
EC-PEL follows an aggressive clinical course and a poor prognosis, with a reported median survival typically less than six months despite chemotherapy.6,18 Extracavitary presentations are diagnostically challenging as the absence of serous effusion and lack of pan-B-cell marker expression can lead to misdiagnosis as plasmablastic lymphoma (PBL), anaplastic large cell lymphoma (ALCL), or poorly differentiated carcinoma, especial in small biopsies.
Despite the high prevalence of HIV and HHV8 infections in Sub-Saharan Africa, published data on EC-PEL from the region remains limited.17,19 Given its diagnostic complexity and aggressive behaviour, further clinicopathologic characterisation in endemic settings is warranted.
In this study, we describe a case series of EC-PEL diagnosed at our institution highlighting clinicopathologic features, diagnostic pitfalls, and differential diagnoses in a high HIV/HHV8 prevalence setting.
Materials and Methods
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Biomedical Research Ethics Committee of the University of KwaZulu-Natal (BREC Ref No. BE00001933/20).
Study Design and Population
This was a laboratory-based retrospective study conducted within the National Health Laboratory Service (NHLS), Durban, South Africa. A purposive sampling strategy was employed to identify all patients diagnosed and coded as PEL between 1 January 2010 and 31 December 2019.
Records were retrieved from the NHLS Corporate Data Warehouse using SNOMED-coded searches and keyword searches for ‘primary effusion lymphoma’. All retrieved specimens were reviewed to confirm diagnostic accuracy.
The diagnosis of EC-PEL was established according to the criteria outlined in the 5th edition of the World Health Organization Classification of Haematolymphoid Tumours (2024). 1 EC-PEL is defined as a KSHV/HHV8-positive large B-cell lymphoma presenting as a solid nodal or extranodal mass in the absence of a concurrent serous effusion. Morphologically, the tumour demonstrates a diffuse proliferation of large atypical lymphoid cells with immunoblastic, plasmablastic, or anaplastic features. Immunophenotypically, the neoplastic cells typically lack pan-B-cell markers and exhibit a post-germinal centre/plasmablastic phenotype, expressing markers such as CD38, CD138, MUM1/IRF4, and epithelial membrane antigen. Demonstration of KSHV/HHV8 infection by immunohistochemical (IHC) detection of LANA-1 is required for diagnosis. EBV infection may be present but is not required.
Ten patients with PEL were identified during the study period. Two patients represented classic PEL, clinically presenting as serous-effusion-based disease (pleural and peritoneal fluid) without a discrete mass and were excluded from further analysis. On histopathological and immunophenotypic review, one tumour was reclassified as KSHV/HHV8-positive diffuse large B-cell lymphoma (DLBCL). This tumour demonstrated cytoplasmic IgM expression with lambda light-chain restriction and was therefore excluded. Seven patients met diagnostic criteria for EC-PEL and constituted the final study cohort.
Clinical Data Collection
Limited clinical information, including age, sex, HIV status, CD4 count, viral load, anatomical site, presence of serous effusions, and the presence of concurrent Kaposi sarcoma or Castleman disease were extracted from the patient records.
The absence of a concurrent serous effusion at diagnosis was confirmed through review of available clinical records, radiologic imaging reports (including chest radiographs and/or computed tomography scans), and laboratory cytology records within the NHLS database. Tumours were classified as extracavitary only if there was no documented pleural, peritoneal, or pericardial effusion at the time of diagnosis and no cytologic evidence of effusion-based lymphoma involvement.
Histopathological and Immunohistochemistry and In Situ Hybridisation
Archived haematoxylin and eosin (H&E)-stained sections and corresponding IHC slides were retrieved. Where necessary, formalin-fixed paraffin embeded (FFPE) tissue blocks were recut at 3 µm for additional stainining. All tumours were independently reviewed by two Anatomical Pathologists (AM and GN) both with experience in haematopathology, using Olympus BX43 microscopes (Olympus, Tokyo, Japan). Whenever a discrepancy occurred, both pathologists re-examined the slides to reach a consensus.
The following stains were reviewed: H&E, CD45, CD3, CD20, MUM1, VS38c, CD138, HHV8 (LANA-1), ALK-1, IgM and Ki-67. EBV was assessed using EBER in situ hybridisation (EBER-ISH).
Immunohistochemistry
IHC staining was performed on the Ventana Benchmark Ultra automated platform (Ventana Medical Systems, Tucson, AZ, USA) according to the manufacturer's protocols. Primary antibodies, clones, dilutions, controls, and suppliers are summarised in Table 1. Appropriate external positive controls were included with each staining run.
Primary Antibodies and In Situ Hybridisation Probes Utilised in This Study.
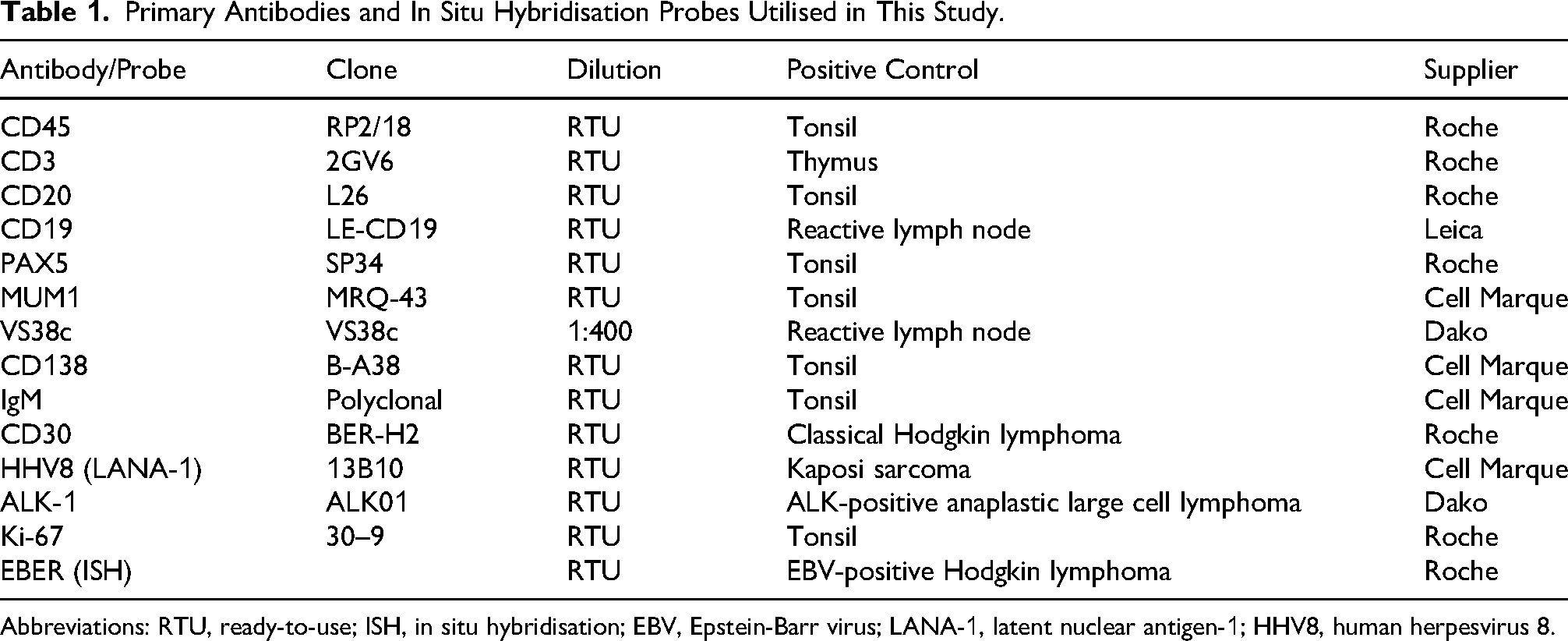
Abbreviations: RTU, ready-to-use; ISH, in situ hybridisation; EBV, Epstein-Barr virus; LANA-1, latent nuclear antigen-1; HHV8, human herpesvirus 8.
IgM immunohistochemistry was not performed at initial diagnosis in all tumours. During study review, IgM staining was performed on all available tumours to further evaluate B-cell differentiation.
For interpretation:
HHV8 (LANA-1) was considered positive when unequivocal nuclear staining was present in tumour cells. All other markers were considered positive when >30% of tumour cells demonstrated specific staining of appropriate cellular localisation. Ki-67 was recorded as a proliferation index (percentage of positive tumour nuclei).
Molecular Cytogenetics
Digital images of fluorescence in situ hybridisation (FISH) analysis were reviewed. FISH analysis was performed with Vysis LSI dual colour, break-apart rearrangement probes (Abbott Molecular, Des Plaines, IL), and was carried out on 4-mm-thick FFPE tissue sections following manufacturer's guidelines.
Molecular analysis for immunoglobulin heavy-chain somatic hypermutation status was not available at our institution during the study period and was therefore not performed.
Assessment for Associated HHV8-Related Disorders
Where available, prior or concurrent histopathologic specimens from the same patients were reviewed for evidence of Kaposi sarcoma, multicentric Castleman disease, or other HHV8-associated lymphoproliferative disorders.
Statistical Analysis
Descriptive statistics were used to summarise clinicopathological variables. Continuous variables were reported as medians and ranges, and categorical variables as frequencies and percentages. Given the small sample size, no inferential statistical comparisons were performed.
Results
Clinical Characteristics
Seven patients of EC-PEL were diagnosed during the study period. The clinical features are summarised in Table 2. The median age at which individuals were diagnosed was 38 years (range, 25 and 51 years). All the patients in the study cohort were black Africans with a significant male patient predominance (male-to-female patient ratio of 6:1).
Clinical Characteristics of Patients Diagnosed with Primary Effusion Lymphoma.
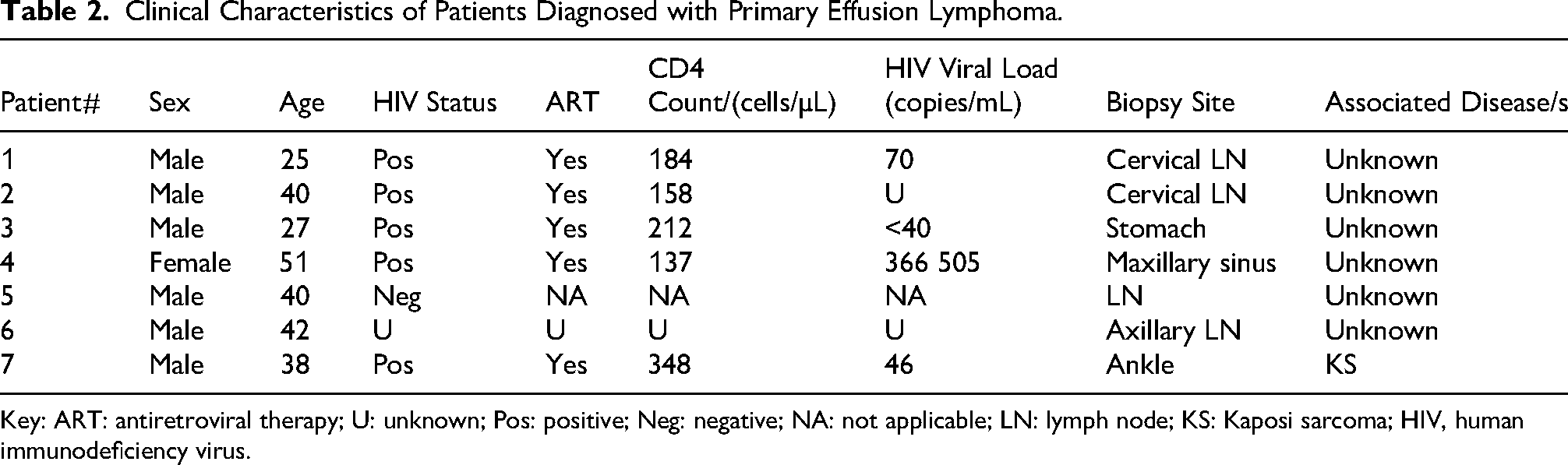
Key: ART: antiretroviral therapy; U: unknown; Pos: positive; Neg: negative; NA: not applicable; LN: lymph node; KS: Kaposi sarcoma; HIV, human immunodeficiency virus.
Lymph node involvement occurred most commonly in cervical and axillary regions, while extranodal presentations affected the stomach, maxillary sinus, and soft tissue of the ankle. One patient hadco-existing Kaposi sarcoma. None of the patients had any prior diagnosis of Castleman disease or KSHV/HHV8-positive germinotropic lymphoproliferative disorder.
Of the seven patients enrolled, five (71%) were living with HIV, one (14%) was HIV-negative and one (14%) had an unknown HIV status. The CD4 cell counts were available for five patients and were uniformly low, ranging from 137 to 348 cells/µL, consistent with advanced immunosuppression. HIV viral load data were available for four of the five patients living with HIV and demonstrated marked heterogeneity, ranging from undetectable levels to high-level viremia.
Microscopic Features
All the neoplasms showed a diffuse proliferation of large atypical lymphoid cells with plasmablastic and/or immunoblastic morphology (Figure 1A & B). The tumour cells demonstrated eosinophilic cytoplasm, round to oval nuclei with irregular nuclear outlines and prominent nucleoli. A brisk mitotic activity was evident in all tumours (Figure 1C&D), in keeping with the highly proliferative nature of PEL. Background small mature lymphocytes were present to varying degrees (Figure 1C&D).
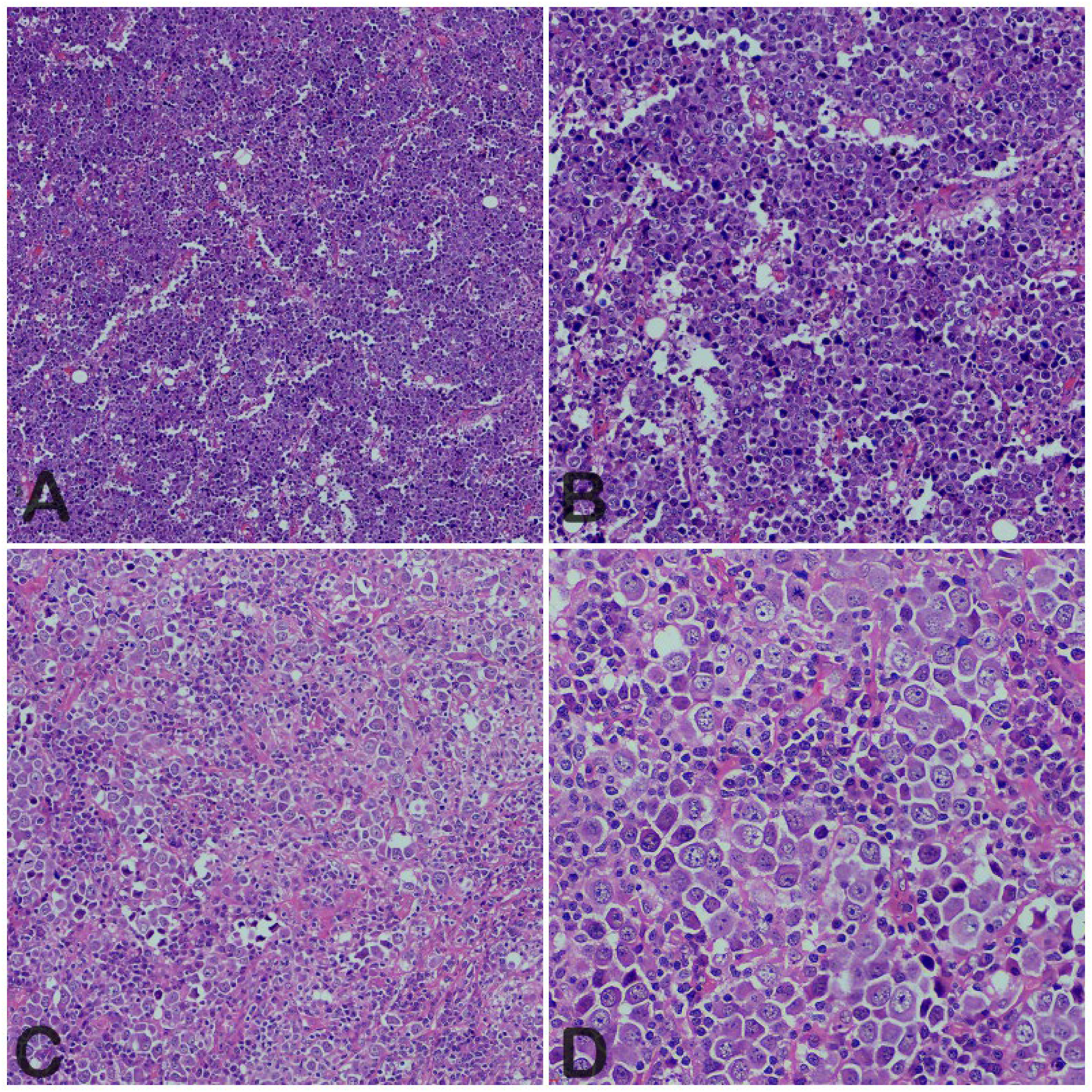
Haematoxylin and eosin (H&E)-stained sections demonstrating the histomorphology of extracavitary primary effusion lymphoma (PEL). (A, 10×; B, 20×) Low and intermediate power views showing diffuse sheets of neoplastic cells with markedly variable cytologic appearances, including immunoblastic, plasmablastic, and anaplastic features. (C, 20×; D, 40×) Intermediate and higher power views highlighting the pleomorphic tumour cell population, with large cells exhibiting prominent nucleoli and abundant cytoplasm with scattered small lymphocytes in the background. Mitotic activity is evident.
Immunohistochemical Findings
The IHC results are summarised in Table 3. All the tumours showed robust and diffuse expression of plasma cell-associated markers (VS38C and CD138) and MUM1 (Figure 2A and 2B), confirming terminal B-cell differentiation. CD45 expression was retained in 29% of the tumours and when present was weak and focal. CD20, CD19 and PAX5 were all negative, and none of the tumours showed ALK-1 immunopositivity. Aberrant T-cell-associated marker expression was demonstrated in two tumours.

Immunophenotype of extracavitary primary effusion lymphoma (x40) (A) VS38c: strong cytoplasmic positivity highlighting plasmablastic differentiation. (B) MUM1: Diffuse nuclear staining consistent with post-germinal centre/terminal B-cell phenotype. (C) HHV-8 (LANA-1): Distinct nuclear positivity confirming HHV-8 infection. (D) EBER In Situ Hybridization (ISH): Strong nuclear positivity indicating Epstein-Barr virus association. LANA-1, latent nuclear antigen-1; HHV-8, human herpesvirus 8.
Immunohistochemical Profiling of Primary Effusion Lymphomas.
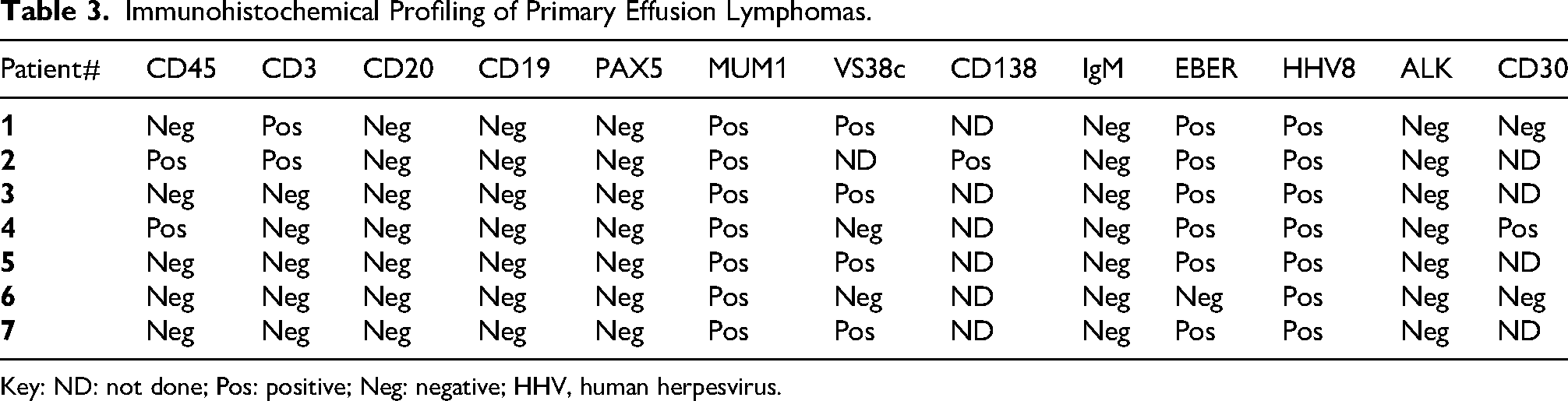
Key: ND: not done; Pos: positive; Neg: negative; HHV, human herpesvirus.
The Ki-67 proliferation index was markedly high in all the tumours ranging from 90% to 95%. Nuclear expression of HHV8 LANA-1 was observed in all seven tumours, confirming the diagnosis of extracavitary PEL (Figure 2C) EBER-ISH was positive in 6 of 7 tumours (86%), while one tumour was EBV-negative (Figure 2D). The EBER-negative tumour showed loss of pan B-cell markers (CD19, CD20 and PAX5). The neoplastic cells expressed MUM1/IRF4, consistent with terminal B-cell differentiation, and lacked cytoplasmic IgM expression (Figure 2B).
FISH assays using break-apart probes for BCL2, BCL6, and MYC revealed no gene rearrangements
All seven tumours exhibited cytomorphologic features that, alongside the distinctive immunophenotypic profile of plasma-cell marker expression, absence of pan-B-cell markers, and universal HHV8 LANA-1 positivity, confirmed diagnosis of EC-PEL.
Discussion
This study represents one of the few dedicated reviews of EC-PEL from Sub-Saharan Africa, a region with a high prevalence of HIV and HHV8 infection but relatively few documented patients with this lymphoma. Consistent with global observations, our series demonstrates that EC-PEL remains a rare but distinctly aggressive lymphoma, predominantly affecting immunocompromised individuals and showing characteristic morphological and immunophenotypic features.
Demographic and Clinical Characteristics
The median age of 38 years in our cohort closely resembles age distributions found previously for HIV-associated PEL, which is generally from the third to fifth decades of life. 1 A strong male patient predominance (6:1) is also consistent with established epidemiological trends in both classical and extracavitary forms as well. 3 Our cohort included only black Africans, corresponding to the demographic profile of the population area served by our institution.
The predominance of patients living with HIV, many of whom demonstrated reduced CD4-positive T-cell counts, reinforces the central role of severe immunosuppression in the pathogenesis of PEL. In this cohort, CD4 counts ranged from 137 to 348 cells/µL (Table 1), which is substantially below the normal adult reference range of approximately 500-1500 cells/µL.20,21 These values fall within the range typically reported for PEL, although some studies have described even more profound CD4 depletion, particularly in patients with classic effusion-only disease. 12 The presence of coexistent HHV8-associated disorders, such as Kaposi sarcoma, is consistent with the well-established clinical association between PEL and other HHV8-driven diseases.1,6
Extracavitary involvement in our cohort included lymph nodes, stomach, sinuses, and soft tissue. These sites are consistent with the spectrum of previously reported extracavitary presentations, which frequently involve lymph nodes and extranodal mucosal or soft tissue sites.7,11,22,23 Notably, all the patients in our cohort did not have concurrent effusions at diagnosis, highlighting the ability of PEL to present purely as a solid mass, an important diagnostic consideration in settings with high rates of HIV-associated lymphoproliferative disorders.
Morphological and Immunophenotypic Characteristics
All the tumours showed the hallmark features of PEL with large plasmablastic or immunoblastic cells, prominent nucleoli, and high mitotic activity. These features closely resemble those described in the literature for both classical and extracavitary forms.2,7 The presence of background small lymphocytes in some tumours has also been reported and may reflect associated inflammatory or reactive processes.
The immunophenotype in our patients was typical and supportive of PEL. All tumours expressed terminal B-cell differentiation markers (CD138, VS38c, and MUM1), with absence of conventional B-cell markers such as CD20, findings that align with early descriptions of PEL as a lymphoma driven toward plasmablastic differentiation. 4 Aberrant or absent expression of B-cell markers contributes to one of the major diagnostic challenges, given that this pattern overlaps with PBL and Kaposi sarcoma-associated virus (KSV)/HHV8+ DLBCL.
HHV8 positivity, confirmed by LANA-1 staining, was universal in our cohort, fulfilling the WHO 2024 diagnostic requirement and supporting HHV8's central role in tumorigenesis.1,5 EBV co-infection was detected in 86% of tumours, similar to many earlier reports, though slightly higher than some recent series.6,24 EBV-negative PELs are most frequently reported in elderly, HIV-negative patients from HHV8-endemic regions; however, with only one EBV-negative tumour in our cohort, no broader conclusions can be drawn. 25
The high proliferative index (90-95%) observed across all tumours further reflects the aggressive biological behaviour of PEL. Elevated proliferation indices are a well-recognized feature of this lymphoma and correlate with poor clinical outcomes. 11
Differential Diagnosis
A comprehensive list of differential diagnoses is summarised in Table 4. Owing to its non-specific histomorphology and frequent loss of conventional B-cell markers, extracavitary PEL presents a broad differential diagnosis, particularly when occurring at solid sites.
Comprehensive Clinical, Histopathological and Molecular Features to Aid Differential Diagnosis.
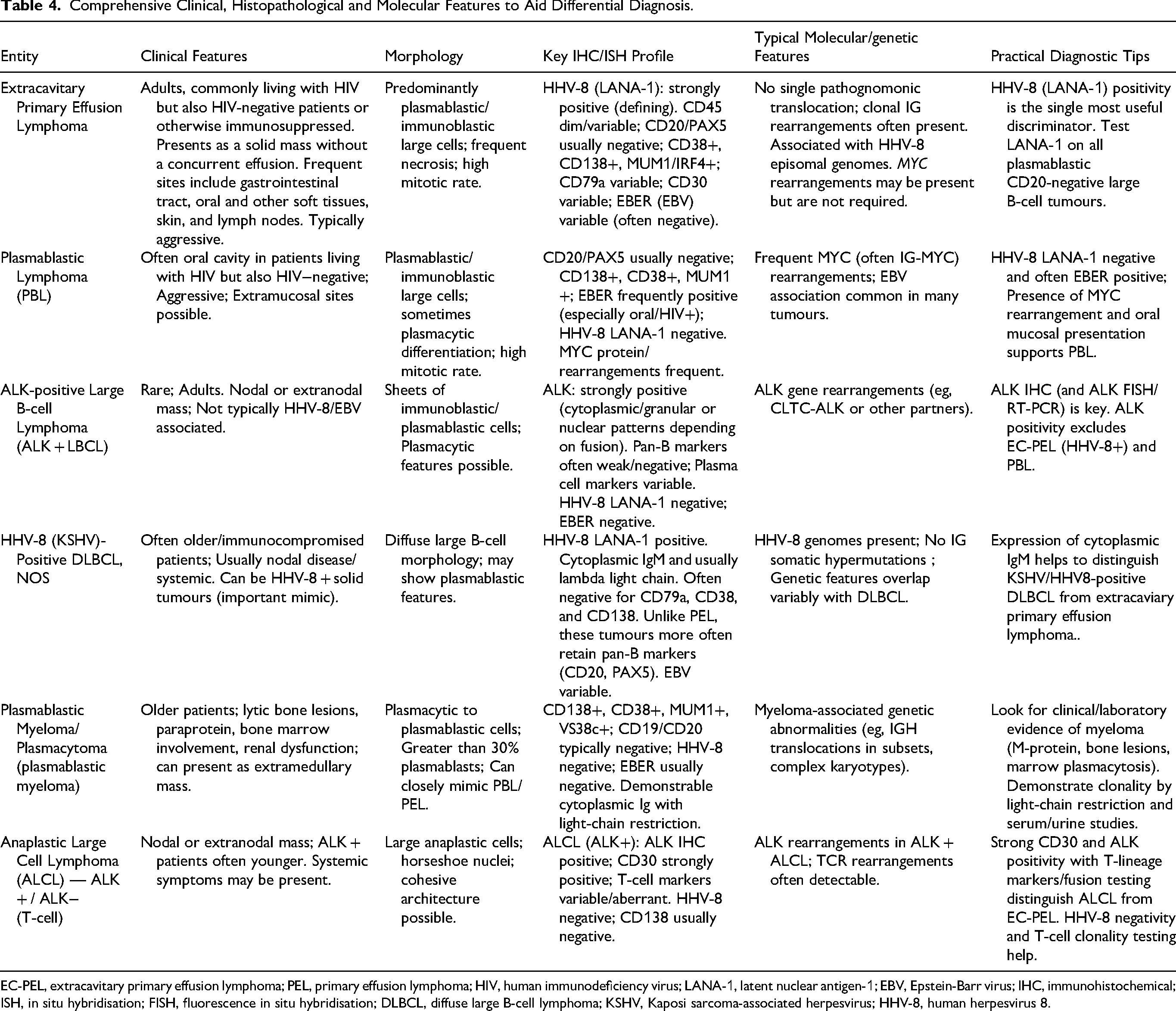
EC-PEL, extracavitary primary effusion lymphoma; PEL, primary effusion lymphoma; HIV, human immunodeficiency virus; LANA-1, latent nuclear antigen-1; EBV, Epstein-Barr virus; IHC, immunohistochemical; ISH, in situ hybridisation; FISH, fluorescence in situ hybridisation; DLBCL, diffuse large B-cell lymphoma; KSHV, Kaposi sarcoma-associated herpesvirus; HHV-8, human herpesvirus 8.
Among the important diagnostic mimics is KSHV/ HHV8+ DLBCL, which can also be seen in patients living with HIV (or otherwise immunosuppressed). Interestingly, partial expression of B-cell-associated antigens can be observed in EC-PEL, overlapping with the immunophenotype of HHV8+ DLBCL. However, HHV8+ DLBCL generally lacks plasmablastic differentiation, is usually EBER-negative, and demonstrates strong cytoplasmic IgM expression with light-chain restriction, which differs markedly from the typical and supportive IgM negativity of PEL.26,27 Therefore, a strong cytoplasmic IgM expression in a solid mass supports the diagnosis of HHV8+ DLBCL over EC-PEL. In addition, HHV8+ DLBCL is often associated with multicentric Castleman disease. 18 In the present study, one patient initially suspected to represent EC-PEL was reclassified as HHV8+ DLBCL based on retained immunoglobulin expression and light-chain restriction, underscoring the importance of comprehensive immunophenotypic evaluation.
PBL also shows significant overlap with EC-PEL, particularly in patients living with HIV. Both entities share plasmablastic morphology, expression of plasma cell-associated markers, and frequent EBV positivity. However, PBL is characteristically negative for HHV8, making LANA-1 immunostaining essential for definitive distinction.1,28–30 The universal HHV8 positivity observed in our cohort effectively excluded PBL.
ALK-positive large B-cell lymphoma (ALK + LBCL) is an important differential diagnosis of extracavitary PEL due to its plasmablastic morphology and frequent loss of conventional B-cell markers.31,32 Morphologically, it shows sheets of large immunoblasts or plasmablasts that may closely resemble EC-PEL at solid sites. 33
Immunophenotypically, the defining feature for this entity is cytoplasmic ALK expression resulting from ALK gene rearrangements, a finding not seen in EC-PEL. In addition, ALK + LBCL is negative for KSHV/HHV8 and EBER, in contrast to the universal HHV8 positivity of EC-PEL. 32 Therefore, the demonstration of ALK expression and absence of HHV8 effectively supports ALK + LBCL over EC-PEL in the appropriate morphologic context.
ALCL can also be considered in the differential diagnosis, especially if marked anaplasia is noted. Clinically, ALCL typically occurs in a younger, HIV-seronegative patient population, in contrast to EC-PEL. 34 Immunophenotypically, ALCL characteristically demonstrates diffuse CD30 expression and may show ALK positivity, neither of which was identified in this series.35,36 The absence of KSHV/HHV8 infection in ALCL also provides an important distinguishing feature and thus effectively excludes this entity. 1
To summarise, proper classification of extracavitary PEL takes careful convergence of morphologic and immunophenotypic data. HHV8 positivity is the most significant distinguishing feature, in line with common loss of B-cell markers, plasmablastic differentiation, and cytoplasmic IgM absence. This differentiation is especially relevant in limited-resource regions where overlapping traits may lead to the misclassification of and under-recognition of an unusual entity.
Significance in a Sub-Saharan African Context
Despite the high prevalence of HIV infection and endemic KSHV/HHV8 in Sub-Saharan Africa, documented patients with PEL from the region remain disproportionately few.17,19 This discrepancy likely reflects significant under-recognition and underdiagnosis rather than true rarity. HIV-associated lymphomas constitute a substantial proportion of haematolymphoid malignancies in the region, yet diagnostic subtyping is frequently constrained by limited access to advanced immunophenotyping and ancillary molecular techniques. In many centres, lymphoma classification is based primarily on morphology and a restricted IHC panel, which may not include essential markers such as HHV8 LANA-1, EBER-ISH, or cytoplasmic immunoglobulin markers required for accurate distinction of EC-PEL from its mimics.37,38 Our results highlight the need for more diagnostic awareness and access to fundamental immunophenotypic biomarkers in the region.
Resource limitations in pathology services across Sub-Saharan Africa have been well documented, including shortages of reagents, inconsistent antibody availability, limited technical expertise, and prolonged turnaround times for specialised testing.37,38 These constraints directly impact the accurate classification of aggressive B-cell lymphomas, particularly entities such as PEL that characteristically lack conventional B-cell marker expression (eg, CD20) and require virus-directed immunohistochemistry for definitive diagnosis. In this context, tumours may be misclassified as ‘high-grade non-Hodgkin lymphoma’, ‘plasmablastic lymphoma’, or ‘diffuse large B-cell lymphoma, NOS’, thereby obscuring the true burden of disease.37,38
Diagnostic capacity constraints were evident in the present cohort. Although 10 neoplasms were initially identified as PEL during the study period, two patients with classic PEL were only definitively diagnosed following pleural and peritoneal tissue biopsies, despite effusion cytology initially being reported as malignant lymphoma. The lack of optimised IHC protocols for cytology cell block material significantly limits the ability to establish a definitive diagnosis of classic PEL on effusion samples alone. In many regional laboratories, cell block preparation and validation of viral markers on cytology specimens are not routinely standardised, creating an additional diagnostic barrier.
Moreover, one tumour initially classified as PEL was subsequently reclassified as HHV8+ DLBCL following the later availability of cytoplasmic IgM immunostaining. This reclassification underscores the critical importance of extended immunophenotyping, particularly in distinguishing HHV8-associated lymphoproliferative disorders that share overlapping morphologic and immunophenotypic features. Without access to cytoplasmic immunoglobulin stains and light-chain assessment, misclassification is likely, which has implications for prognostication and therapeutic decision-making.
The identification of extracavitary (solid) disease in this series further emphasises the need for heightened diagnostic awareness. In HIV-endemic settings, atypical nodal or extranodal masses in immunocompromised patients may be attributed to more common entities such as DLBCL or PBL, especially when effusions are absent. However, extracavitary PEL is increasingly recognised and may represent a significant but underdiagnosed component of HIV-associated lymphomas. 1 Routine inclusion of HHV8 LANA-1 immunostaining in the evaluation of plasmablastic or CD20-negative large B-cell lymphomas in patients living with HIV may therefore substantially improve diagnostic accuracy in the region.
Collectively, these findings highlight the urgent need to strengthen haematopathology diagnostic systems in Sub-Saharan Africa through improved access to essential IHC markers, optimisation of cytology-based lymphoma workup, regional referral pathways for specialised testing, and continued training in HIV-associated lymphoma classification. Strengthening diagnostic infrastructure will improve the accuracy of disease burden estimates and enable timely and appropriate patient referral for clinical management, while supporting epidemiologic surveillance of HHV8-associated lymphoproliferative disorders in high-prevalence settings.
Limitations
This study is limited to small data generation that is indicative of the exceptional rarity of PEL, especially extracavitary PEL. In some patients, clinical data was incomplete and some patients had missing HIV-related laboratory parameters, further limiting the depth of clinical correlation. Efforts to retrieve follow-up data were not successful, and as a result, treatment and outcomes analysis were impossible. These gaps emphasize the importance of strengthening a multidisciplinary team approach to better manage these patients and improve their outcomes.
Conclusion
This study demonstrates that extracavitary PEL in Sub-Saharan Africa has comparable clinical, morphological, and immunophenotypic features to others in the world, and is strongly associated with HIV, HHV8 infection, and advanced immunosuppression. HHV8 LANA-1 and IgM are still essential for diagnosis especially to differentiate PEL from morphologic mimics including PBL and KSHV/HHV8-positive DLBCL. In this way, improving access to diagnostic immunohistochemistry and increasing regional awareness may lead to a more accurate and timely diagnosis, thereby contributing to better characterisation of this aggressive lymphoma in Sub-Saharan Africa.
Footnotes
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Biomedical Research Ethics Committee of the University of KwaZulu-Natal (BREC Ref No. BE00001933/20).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.