
Abstract
Background
Primary breast lymphomas are rare neoplasms, the majority of which are of B cell origin. Anaplastic large cell lymphoma of the breast is most commonly associated with breast implants; however, implant-unrelated tumors have also been reported. This case report describes a young patient diagnosed with primary anaplastic lymphoma kinase (ALK)-negative breast anaplastic large cell lymphoma in the absence of any history of breast implantation.
Case Report
A 26-year-old woman presented with right breast pain and a palpable mass that had persisted for 3 months. Radiological evaluation revealed a complex cystic lesion suspicious for malignancy. Histopathological examination of the core biopsy specimen demonstrated diffuse neoplastic infiltration composed of large atypical cells with marked nuclear pleomorphism and increased mitotic activity. Immunohistochemical analysis showed strong CD30 positivity and focal epithelial membrane antigen expression, while ALK, keratin AE1/AE3, CD20, and Epstein–Barr virus (EBV) were negative. Following breast-conserving surgery, the final diagnosis was ALK-negative anaplastic large cell lymphoma.
Conclusion
This report highlights that the development of anaplastic large cell lymphoma in the breast is not exclusively dependent on the presence of an implant and may occur in patients without any history of breast implantation. Given the nonspecific clinical and radiological findings, anaplastic large cell lymphoma should be considered in the differential diagnosis of breast masses, particularly those associated with cystic changes or chronic inflammatory processes. Definitive diagnosis requires thorough histopathological and immunophenotypic evaluation.
Keywords
Introduction
Breast lymphomas, which are clinically categorized as primary or secondary, represent rare neoplasms of the breast. Secondary breast lymphomas refer to lymphomas originating outside the breast that subsequently involve the breast, accounting for approximately 17% of all breast metastases. 1 Primary breast lymphoma was first described in 1972 and defined according to several diagnostic criteria, including the presence of adequate histopathological material regardless of ipsilateral axillary lymph node involvement, a close association between lymphoma infiltration and breast parenchyma, the absence of systemic lymphoma at the time of diagnosis, and no prior history of extramammary lymphoma. Over time, however, these criteria have been interpreted more flexibly, and clinical presentation with a breast mass or related symptoms, together with the absence of a previous lymphoma diagnosis, has been considered sufficient for diagnosis, even if distant involvement is detected during staging.2–4
Primary breast lymphomas are exceedingly rare and account for approximately 0.04–0.7% of all malignant breast lesions.2–4 According to the World Health Organization classification of breast tumors, breast lymphomas are categorized into five main subtypes: extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma), follicular lymphoma, diffuse large B cell lymphoma, Burkitt lymphoma, and breast implant-associated anaplastic large cell lymphoma. 5 Diffuse large B cell lymphoma represents the most common subtype, whereas T cell lymphomas account for fewer than 10% of all primary breast lymphomas. The reported incidence of anaplastic large cell lymphoma is approximately 8.1 per 100 million women annually. Although anaplastic large cell lymphoma is extremely rare, it shows a strong association with breast implants, and implant-unrelated anaplastic large cell lymphoma involving the breast has only rarely been reported in the literature.6–8
In this report, we describe a young patient with primary anaplastic lymphoma kinase (ALK)-negative anaplastic large cell lymphoma of the breast, without a history of breast implantation, and discuss the clinicopathological features in the context of the existing literature.
Case Report
A 26-year-old woman presented to the clinic with pain, tenderness, and a palpable mass in the right breast that had persisted for 3 months. The patient had no known medical history or prior surgical procedures. On physical examination, a soft, well-circumscribed mass measuring approximately 3 × 2 cm was detected in the upper middle quadrant of the right breast, and no axillary lymphadenopathy was observed. Contrast-enhanced magnetic resonance imaging and breast ultrasonography revealed a complex cystic mass measuring approximately 7.6 × 6 cm in the central portion of the right breast, extending toward the upper and lower quadrants (Figure 1). The findings were considered suspicious for malignancy, and histopathological verification was recommended.
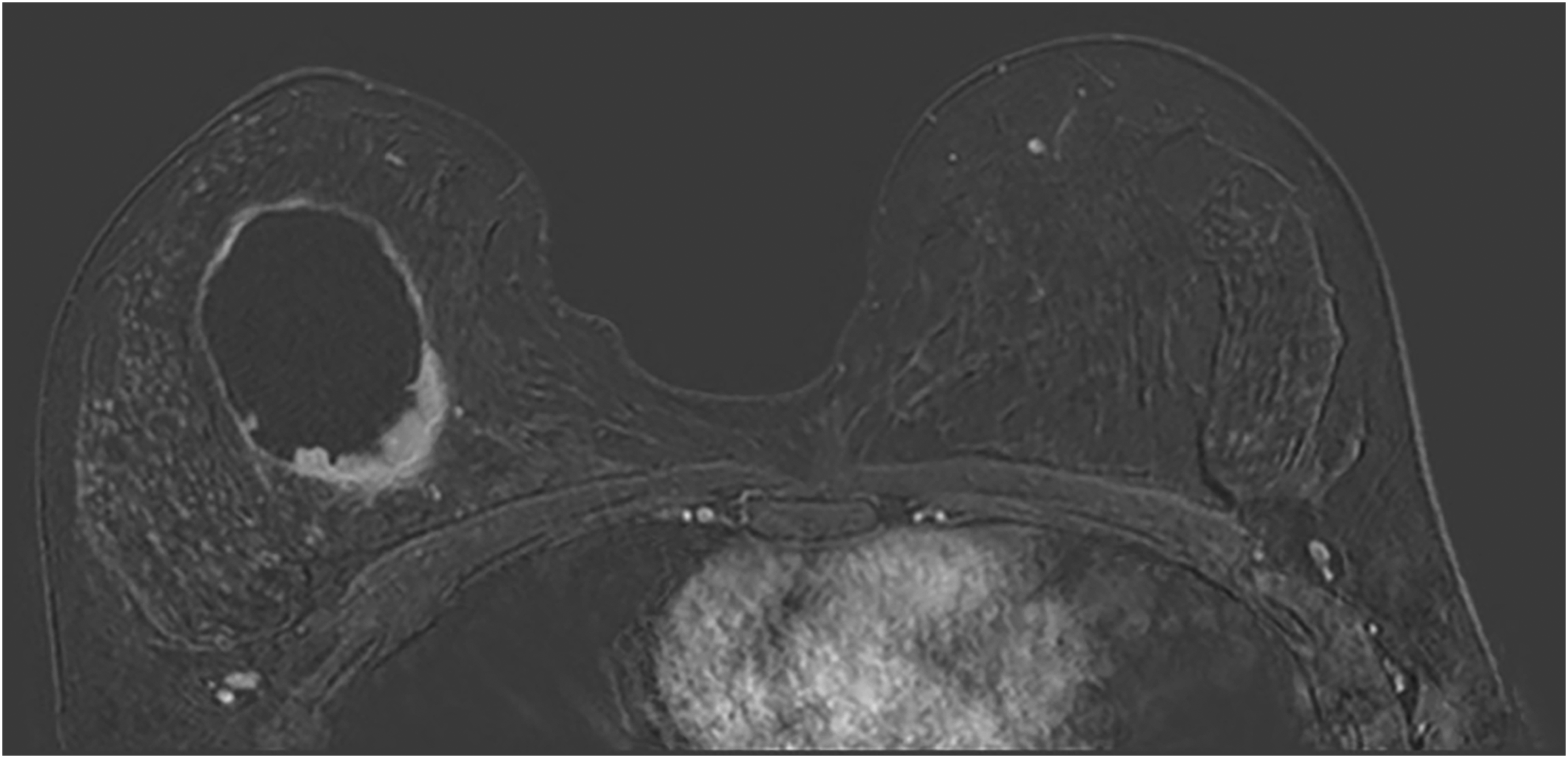
Contrast-enhanced breast MRI showing a large complex cystic lesion in the right breast with mural nodularity and irregular wall thickening, suspicious for malignancy (BI-RADS 4A).
Microscopic examination of the core needle biopsy specimen revealed a neoplastic lesion composed of atypical cells with large vesicular nuclei, some showing prominent nucleoli, eosinophilic cytoplasm, and increased mitotic activity. The immunohistochemical studies demonstrated strong CD30 expression, with focal immunoreactivity for epithelial membrane antigen (EMA) and CD43, whereas keratin AE1/AE3, CD20, CD79a, keratin 7, GATA3, and ALK were negative (Figure 2). Based on the biopsy findings, wire-guided breast-conserving surgery and sentinel lymph node biopsy were planned.
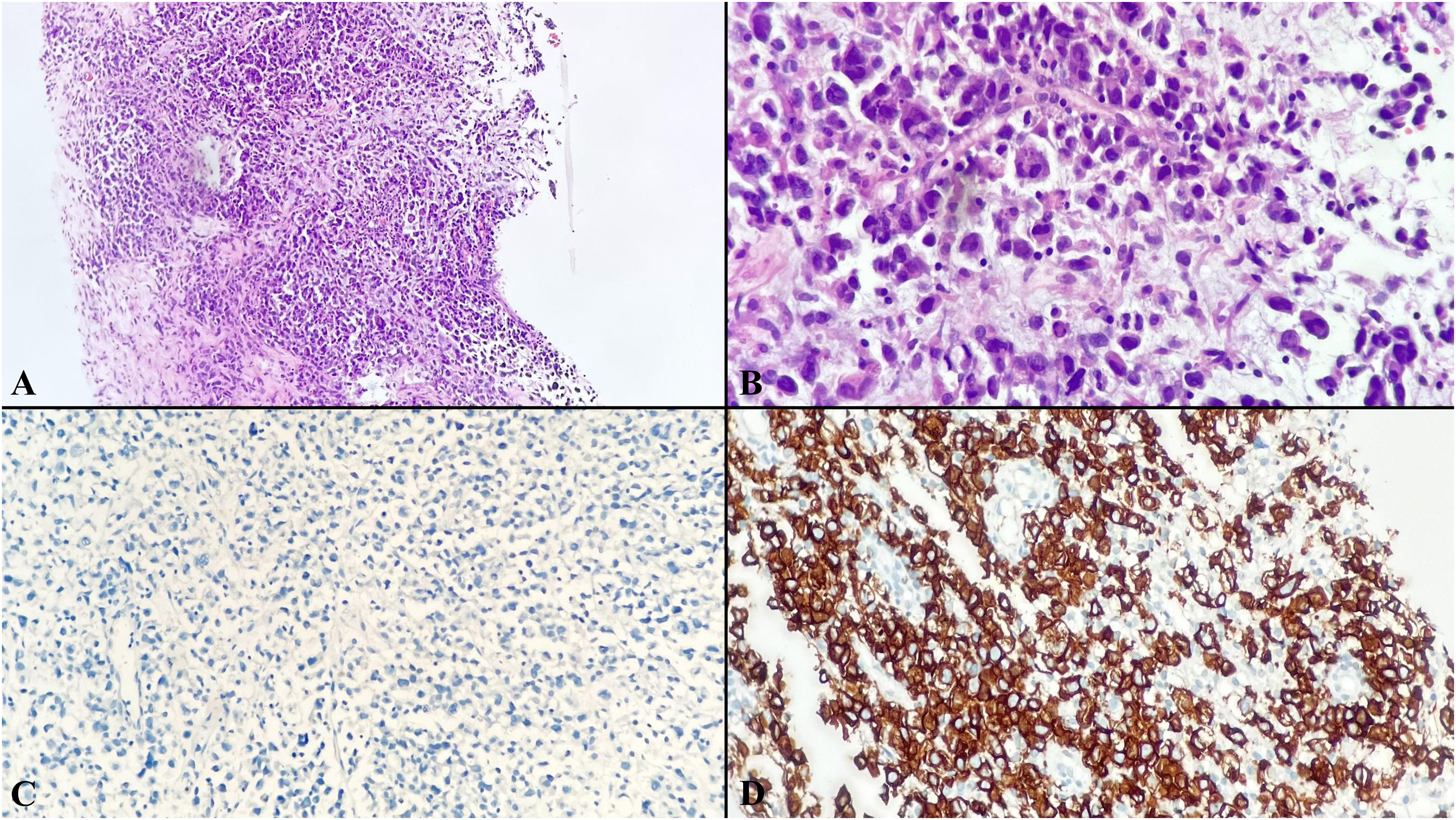
Tru-cut biopsy specimen from a patient of breast anaplastic large cell lymphoma. Diffuse infiltration of atypical lymphoid cells with abundant cytoplasm within the breast stroma (A, ×100). Large anaplastic tumor cells showing marked nuclear pleomorphism and vesicular chromatin (B, ×400). Tumor cells showing no immunoreactivity for keratin AE1/AE3 (C, ×200). Strong positivity for CD30 in tumor cells (D, ×200).
Macroscopic examination of the lumpectomy specimen revealed a firm gray-white lesion measuring 8 × 7.5 × 3 cm, containing a cystic area measuring approximately 6 × 4 cm. Microscopic evaluation demonstrated a neoplastic lesion measuring 3.5 × 1.6 cm composed of atypical cells with prominent nucleoli, some displaying horseshoe- or kidney-shaped nuclei, coarse chromatin, and eosinophilic cytoplasm. Mitotic activity was high in the tumor. Extensive areas of necrosis were present in the central portion of the tumor, along with a large cystic component consistent with the macroscopic findings. While most of the cystic areas lacked an epithelial lining, focal areas showed lining epithelium composed of cells with abundant eosinophilic cytoplasm and prominent nucleoli, exhibiting metaplastic changes. A dense mononuclear inflammatory infiltrate was observed around the cyst, with neoplastic cells in close proximity. Although normal breast ducts were not identified within the tumor, ductal structures were present in the surrounding tissue, accompanied by periductal mononuclear inflammatory infiltration (Figure 3). Immunohistochemical analysis showed strong CD30 expression, with immunoreactivity for EMA (focal), CD43 (diffuse), CD4 (focal), CD5 (focal), CD7 (focal), and while keratin AE1/AE3, CD20, CD15, Epstein–Barr virus (EBV), PAX5, and ALK were negative (Figure 4).
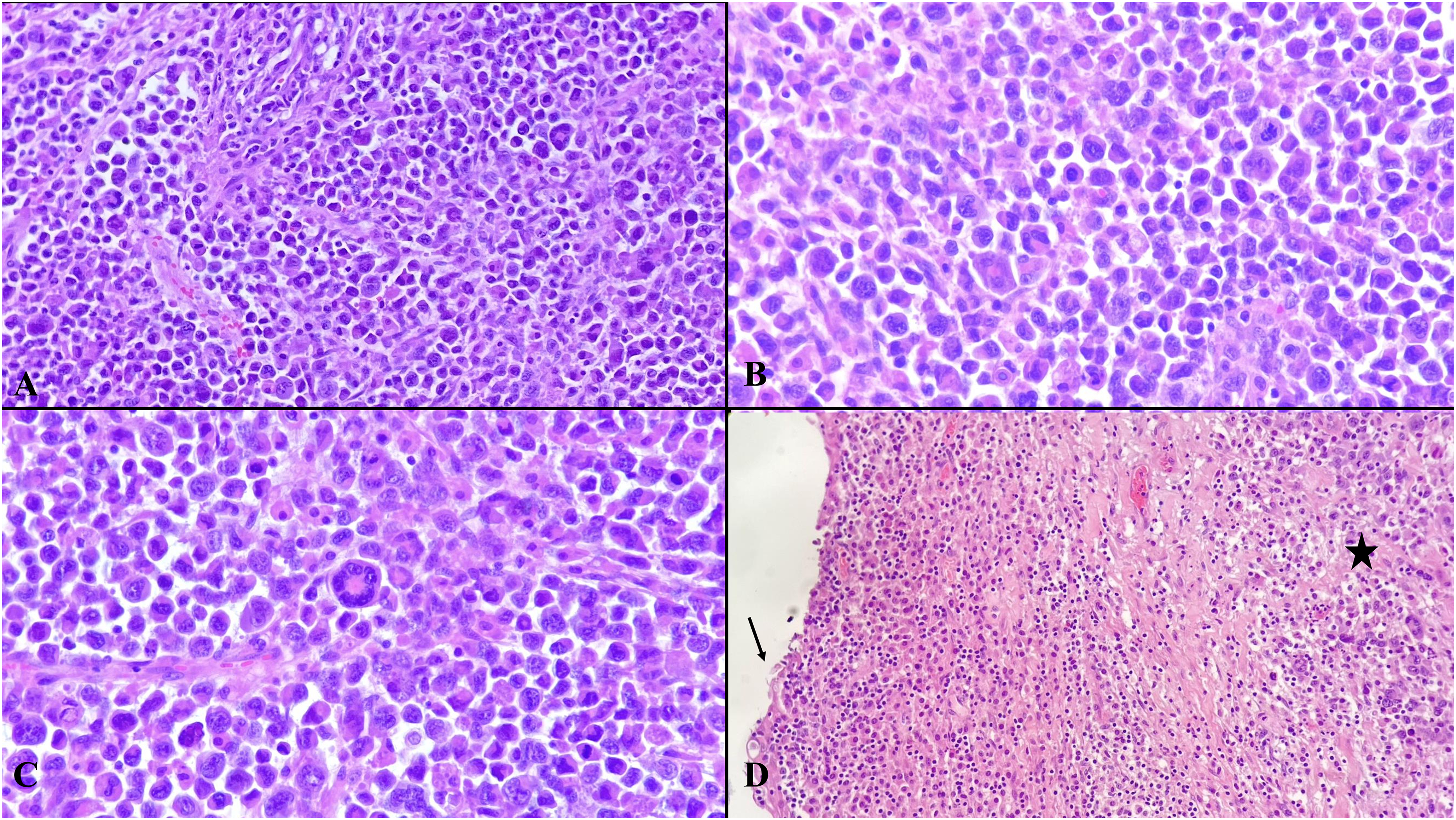
Resection specimen from a patient of breast anaplastic large cell lymphoma. Proliferation of atypical lymphoid cells with a diffuse infiltrative growth pattern in the breast stroma (A, ×100). Large anaplastic tumor cells with abundant cytoplasm, pleomorphic appearance, irregular nuclear contours, coarse chromatin, and occasional prominent nucleoli (B, ×200). Large neoplastic cells with folded or multilobed nuclei, corresponding to hallmark cells, horseshoe cells, or embryo cells (C, ×400). The arrow indicates cyst lining epithelium with metaplastic changes, while the asterisk highlights neoplastic cells (D, ×100).

Focal immunoreactivity for CD5 in tumor cells (A, ×200). CD4 immunopositivity in tumor cells (B, ×200). Tumor cells showing focal cytoplasmic EMA immunoreactivity (C, ×200). No immunoreactivity for ALK is observed in tumor cells (D, ×200).
Based on histomorphological and immunohistochemical findings, the diagnosis of ALK-negative anaplastic large cell lymphoma was established. Following the identification of ALK negativity, further evaluation was performed at an external center using fluorescence in situ hybridization (FISH) for EBV and DUSP22 rearrangements; no evidence of translocation, copy number gain, or deletion was identified in the tumor. The patient was staged as IV-A according to the Ann Arbor staging system and treated with a brentuximab vedotin-combined cyclophosphamide, doxorubicin, and prednisone regimen for a total of eight cycles. The patient has been under follow-up for 13 months, is alive, and continues to receive treatment.
Discussion
The majority of primary breast lymphomas exhibit a B cell phenotype, whereas T cell lymphomas are exceedingly rare. Among T cell lymphomas of the breast, the most frequently encountered subtype is anaplastic large cell lymphoma, which demonstrates CD30 expression and is classified into ALK-positive and ALK-negative subtypes. Most anaplastic large cell lymphomas involving the breast are associated with breast implants. 9
Breast implant-associated anaplastic large cell lymphoma was first described in 1997 and was subsequently included as a provisional entity in the 2016 WHO classification. 10 Proposed risk factors include chronic inflammation and immune response induced by the breast implant, prolonged immune stimulation, subclinical bacterial infections, and genetic predisposition. 11 However, the etiology of implant-unrelated anaplastic large cell lymphoma remains unclear. Mulligan et al reported an ALK-negative anaplastic large cell lymphoma associated with a cyst in a patient without a history of breast prosthesis, suggesting a potential role for implant-independent chronic inflammatory processes. 12 Our findings similarly support this hypothesis, as no prosthesis was present, although a cystic component with an associated chronic inflammatory cell infiltrate was observed adjacent to the tumor.
Studies on implant-unrelated breast anaplastic large cell lymphoma remain limited in the literature. In a study by Lazzeri et al, 27 patients with implant-unrelated breast anaplastic large cell lymphoma were reported. Among these, 10 were ALK-negative, 11 were ALK-positive, and ALK status was unknown in six patients. The age of the patients ranged from 13 to 92 years (mean: 42.5 ± 22.3 years), and 92.6% were female patients. 13 The present patient was a 26-year-old woman at the time of diagnosis.
Clinically, primary breast lymphomas most commonly present with a painless palpable breast mass, similar to breast carcinomas. While implant-associated primary breast anaplastic large cell lymphoma involves both breasts with similar frequency, other primary breast lymphomas more commonly affect the right breast.2,14 In the present patient, the lesion was located in the right breast, and no pathological findings were detected in the left breast during clinicoradiological follow-up. Radiologically, breast lymphomas are typically detected as irregular masses with indistinct margins. Radiological findings alone are insufficient to reliably differentiate breast lymphomas from breast carcinomas. 15 In the present patient, the lesion was evaluated using mammography, ultrasonography, contrast-enhanced magnetic resonance imaging, and the complex cystic mass was interpreted as BI-RADS category 4A.
Macroscopic findings may vary depending on the presence of a distinct mass lesion. In situations, particularly breast implant-associated anaplastic large cell lymphoma, where no macroscopic mass lesion is identified, the tissue should first be adequately fixed and the surgical margins appropriately inked. Subsequently, it is recommended that 12 tissue samples be obtained from six directions, including sections from the surface facing the implant. 16 Evans et al reported that in patients with breast implant-associated anaplastic large cell lymphoma, invasive diagnostic procedures had been performed between 6 months and 4 years prior to the final diagnosis. These procedures included capsule sampling, capsule incision, partial excision, implant replacement, or fluid aspiration, yet none of these procedures initially yielded a lymphoma diagnosis, highlighting the critical importance of adequate sampling. 17
Breast implant-associated anaplastic large cell lymphoma is typically identified along the inner surface of the capsule and is often associated with peri-implant effusion, and is characterized by large anaplastic cells showing marked pleomorphism. Tumor cells generally have abundant cytoplasm and irregular horseshoe-shaped nuclei, and necrosis and karyorrhexis may be observed. Immunophenotypically, strong and diffuse CD30 positivity is characteristic, and loss of pan-T cell antigens is frequently observed. ALK immunohistochemical evaluation is mandatory, and tumors are categorized as ALK-positive or ALK-negative according to the expression status. These tumors frequently show clonal rearrangements of T cell receptor genes. Mutations in genes involved in the JAK/STAT pathway (eg, STAT3, JAK1, and JAK3), as well as DNMT3A and TP53, have been reported, particularly in breast implant-associated anaplastic large cell lymphoma. In contrast, DUSP22 and TP63 rearrangements define distinct molecular subsets of ALK-negative anaplastic large cell lymphoma. Reactive inflammation, other high-grade lymphomas, and non-lymphoid malignancies should be considered in the differential diagnosis due to overlapping morphological features. 18 In the limited number of implant-unrelated tumors reported in the literature, the histomorphological features of anaplastic large cell lymphoma appear similar to those of implant-associated tumors. In the study by Lazzeri et al, ALK negativity was reported in 10 of 21 patients with known ALK status. 13 In the present patient, following the identification of ALK negativity, further evaluation for EBV and DUSP22 rearrangements was performed. EBV was not detected. No evidence of DUSP22 rearrangement, copy number gain, or deletion was identified. In this context, the findings argue against the DUSP22-rearranged subgroup and support classification within the so-called “triple-negative” ALK-negative ALCL category. We acknowledge that additional molecular analyses, including evaluation for TP63 rearrangements and JAK/STAT pathway alterations, would further clarify the pathogenesis of this rare implant-unrelated entity.
This report represents one of the examples demonstrating that the development of anaplastic large cell lymphoma in the breast is not exclusively dependent on the presence of breast implants and may rarely occur in patients without a history of implantation. Because clinical and radiological findings are non-specific, anaplastic large cell lymphoma should be considered a rare but important differential diagnosis, particularly in patients presenting with newly developed pain, swelling, or a solid mass, especially in the presence of cysts or a history of surgical intervention. The definitive diagnosis should rely on adequate histopathological and immunophenotypic evaluation obtained through core needle biopsy or surgical excision.
Footnotes
Ethical Approval
Ethics approval for the case report, dated April 8, 2026, and numbered 2026/214-7/25, was obtained from the local Clinical Research Ethics Committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.