
Abstract
The current study applied Holland’s RIASEC typology to develop a Physician Skills Inventory. We identified the transferable skills and abilities that are critical to effective performance in medicine and had 140 physicians in 25 different specialties rate the importance of those skills. Principal component analysis of their responses produced three major components that aligned with the RIASEC code of Investigative-Realistic-Social (IRS) for physicians. The investigative type fit with problem-solving skills, the realistic type fit with psychomotor skills, and the social type fit with counseling skills. The Physician Skills Inventory may be used in helping medical students profile their skills for further development or remediation and for matching their skills to the requirements of different specialties.
Many medical students experience difficulty choosing a medical specialty in which to practice. They often find themselves in need of accurate information about the qualifications and qualities of physicians in the specialties that they are considering (Richard et al., 2007). They need to understand the skills required to perform effectively as a physician and to be able to assess their level of skill in those important areas. At the same time, career counselors and medical school advisors need additional resources to assist those students with their career decision making. Until recently, most existing career guidance tools had been developed for use by high school and undergraduate college students and had not been successfully applied to helping medical students choose their medical specialty. Research over the past few decades has now been reported on the development of new measures to assess the interests and values of medical students (Hartung, Taber, & Richard, 2005; Richard, 2005), but work examining other traits and characteristics, such as skills, that are important to successful performance as a physician is limited. Thus, while ability and skill assessment are central topics in the psychology of individual differences, little attention has been focused on studying the transferable skills of medical students and physicians.
Transferable skills are not limited to any one academic discipline or knowledge area but are applicable to many occupations. They are universal and can be acquired in a variety of ways, whether on the job, in the classroom, working on projects and hobbies, or participating in sports. In medicine, transferable skills are defined in a number of ways, and generally include skills involved in evaluating evidence, information handling, problem solving, oral and written communication, computing, numeracy, psychomotor movement, and organizational management (McLachlan, 2000; Whittle & Murdoch-Eaton, 2001). Many students believe that transferable skills training is extremely important to their future careers, and in some areas of health care, researchers assert that training in transferable skills may even reduce medical errors (Birch et al., 2007). The United Kingdom has taken the lead in advocating the importance of identifying and developing transferable skills. In particular, the U.K. General Medical Council, in its publication “Tomorrows Doctors: Recommendations on Undergraduate Medical Education,” promoted the importance of training undergraduate medical students in transferable skills and encouraged more research on the topic (Grady, Gouldsborough, Sheader, & Speake, 2009; Mattick, Dennis, Bradley, & Bligh, 2008; Whittle & Murdoch-Eaton, 2001).
Research on the assessment and development of transferable skills has been conducted in a broad variety of populations (Mayall & Maze, 1985) and with students in specific occupational groups, including physiotherapy (Jones, McIntyre, & Naylor, 2010), nursing (Birch et al., 2007; Stephens-Lloyd, 2004), community and health sciences (Mpofu & Imalingat, 2006), and vocational rehabilitation (Darling, Growick, & Kontosh, 2002; Saxon & Roberts, 1983). Its importance also has been stressed in many other areas of higher education (Greenan, Humphreys, & McIlveen, 1997) as well as with PhD researchers (Alpay & Walsh, 2008; Bromley, Boran, & Myddelton, 2007). New measures are being developed to quantify the contribution of transferable skills to medical student performance (Mattick et al., 2008), yet there remains a need for more research on understanding the role of transferable skills in medicine and to develop methodologies that promote effective learning and transfer of skills to the work environment (Burke, Jones, & Doherty, 2005; Stephens-Lloyd, 2004).
Support for the training of transferable skills in curriculum redesign is slowly beginning to occur (Greenan et al., 1997; Jones et al., 2010; Mattick et al., 2008; McLachlan, 2000), and even in medical education there is a recognition that transferable skills actually are being applied, as in the case of problem-based learning (PBL) through which students use an interdisciplinary approach to solving patient problems (Goldsborough et al., 2009). Although these skills are demonstrated during PBL and other simulation-based training environments, they are not explicitly taught or measured, however, and dedicated time for practice and feedback to occur is not provided (Birch et al., 2007). With focused practice and attention to measurement and the provision of feedback, PBL courses could be an excellent venue for teaching and assessing transferable skills.
Recently research has been reported on the development of measures for assessing transferable skills among college students, many of which measure confidence in the ability to perform a number of skills (Alpay & Walsh, 2008; Bromley et al., 2007; Mayall & Maze, 1985; Mpofu & Imalingat, 2006; Whittle & Murdoch-Eaton, 2001). Results indicate that students generally feel confident in their skills, with some gender differences (Alpay & Walsh, 2008), and that transferable skills generally can be taught and improved. While there is growing agreement that basic, transferable skills are important to the performance of medical student, less is known specifically about the skills needed in the work of the successful physician. This study identified the skills critical for effective performance in a number of medical specialties and used the results to develop a self-report survey of transferable skills among medical students.
To construct the survey, we went beyond the typical procedures of having a small panel of experts identify the skills and group them into relevant categories without any empirical confirmation. None of the skills checklists that we could find used an empirical taxonomy to organize the skills. In each case, the skills were grouped a priori based on some commonsense framework. In our research, we wanted to link the framework to a theory of vocational behavior. After performing the usual steps in constructing a skills checklist, we attempted to determine empirically the relevant categories and link the resulting categories to Holland’s (1997) theory of vocational personality types. We used principal components analysis to organize the data and determine whether the skills could be conceptualized as having a clear latent structure and whether this structure resembled Holland’s typology. To gather the relevant data, we used a relatively large and diverse sample of practicing physicians rather than the typical small panel of occupational experts.
Method
Skills Identification
A 70-item skill analysis survey was developed to assess the importance and frequency of transferable skills pertaining to the practice of medicine. We constructed the initial skill list using three main sources of information. First, a list of skills and abilities were obtained from the U.S. Department of Labor’s Occupational Information Network (O*NET) classification system (O*NET Resource Center, 2000). O*NET replaced the long-standing dictionary of occupational titles and contains descriptions of job-oriented characteristics (e.g., work activities, work content, labor market information, and tasks) and worker-oriented characteristics (e.g., abilities, interests, values, work styles, skills, knowledge, experience, and education) that may be found in most occupations represented in the U.S. world of work. For the purpose of this research, only worker-oriented characteristics (basic skills, abilities, and cross-functional skills) were included. Second, a review of the medical specialty choice literature was conducted to identify skills important in the field of medicine (Double, 1998; Taylor, 1999; Whittle & Murdoch-Eaton, 2001). Finally, a generic skill list was obtained from the Careers in Medicine career planning system website developed by the Association of American Medical Colleges (2001). We consolidated these 3 skill lists to form a single list containing 70 skill items grouped into 6 categories (cognitive abilities, psychomotor abilities, basic and cross-functional skills, interpersonal and social skills, problem-solving skills, and resource management skills). Each skill in the final list was described by one or two sentences. Most of the skills were contained in the O*NET system and in those cases the descriptions were obtained from that system. For the remaining skills new descriptions were written. The list of skills and their descriptions were reviewed and refined by two physicians who worked in medical education and a medical school career counselor. And while most transferable skill surveys reported in the literature completed their research at this point, we took the additional step of empirically studying the skill list.
The resulting list of skills and their descriptions served as a skill analysis survey, which is available from the authors. Respondents rated each skill item for importance in the work that they performed on a typical day using a scale of 1 to 5 (1 = not important, 2 = of little importance, 3 = moderately important, 4 = very important, and 5 = extremely important). They also rated each item on the frequency with which they used that skill on a typical day using a scale from 1 to 5 (1 = never or rarely, 2 = seldom, 3 = sometimes, 4 = usually, and 5 = almost always or always).
Participants
The survey was distributed to clinical faculty members who, taken together, represented a diverse group of specialties and skills that comprise the contemporary practice of medicine. Participants were 164 clinical faculties at a community-based medical school in the Midwest. These physicians were especially knowledgeable about transferable skill requirements because they both teach and practice medicine. Participants had been practicing from 1 to 42 years, with a mean of 15.51 years. They represented 25 major specialties and subspecialties, including emergency medicine, family medicine, internal medicine, general surgery, obstetrics and gynecology, pediatrics, orthopedic surgery, pathology, psychiatry, urology, and diagnostic radiology. There were 122 (74%) males and 38 (23%) females who were engaged in a number of professional activities, such as hospital-based practice (57%), office-based practice (55%), teaching (28%), research (5%), and administration (10%; percentages do not total 100% because participants were allowed to indicate more than one activity). In addition to completing the survey, participants were asked to indicate their specialty, position title, years in practice, type of institution in which they were employed, major professional activity, and gender.
Results
There were 164 surveys returned from the following specialty groups: 61 in primary-care specialties; 32 in surgical specialties; 16 in technical specialties, and 52 in medical specialties. We discarded 24 surveys with missing responses, leaving a total of 140 usable surveys. Using participants’ skill ratings, we multiplied the importance score by the frequency score to compute a criticality score for each of the 70 skills.
Second, we explored the structure of the 70 criticality scores using principal components analysis with varimax rotation to organize the skills into uncorrelated components or groups. We selected principal components analysis because it is the simplest of the true eigenvector-based multivariate analyses and is commonly used for exploratory studies. The analysis initially produced 17 components with eigenvalues greater than 1.0. These 17 components accounted for 74% of the variance. However, many of the components contained only one or two items. Analysis of the eigenvalue scree plot indicated a large difference between the third and fourth components and a smaller drop after the seventh factor. Eigenvalues of components one through three were above 4.0 while components four through seven reported eigenvalues of 2.0–3.0. Based on inspection of the scree plot, we reran the principal components analysis to extract seven components. They accounted for 56% of the variance.
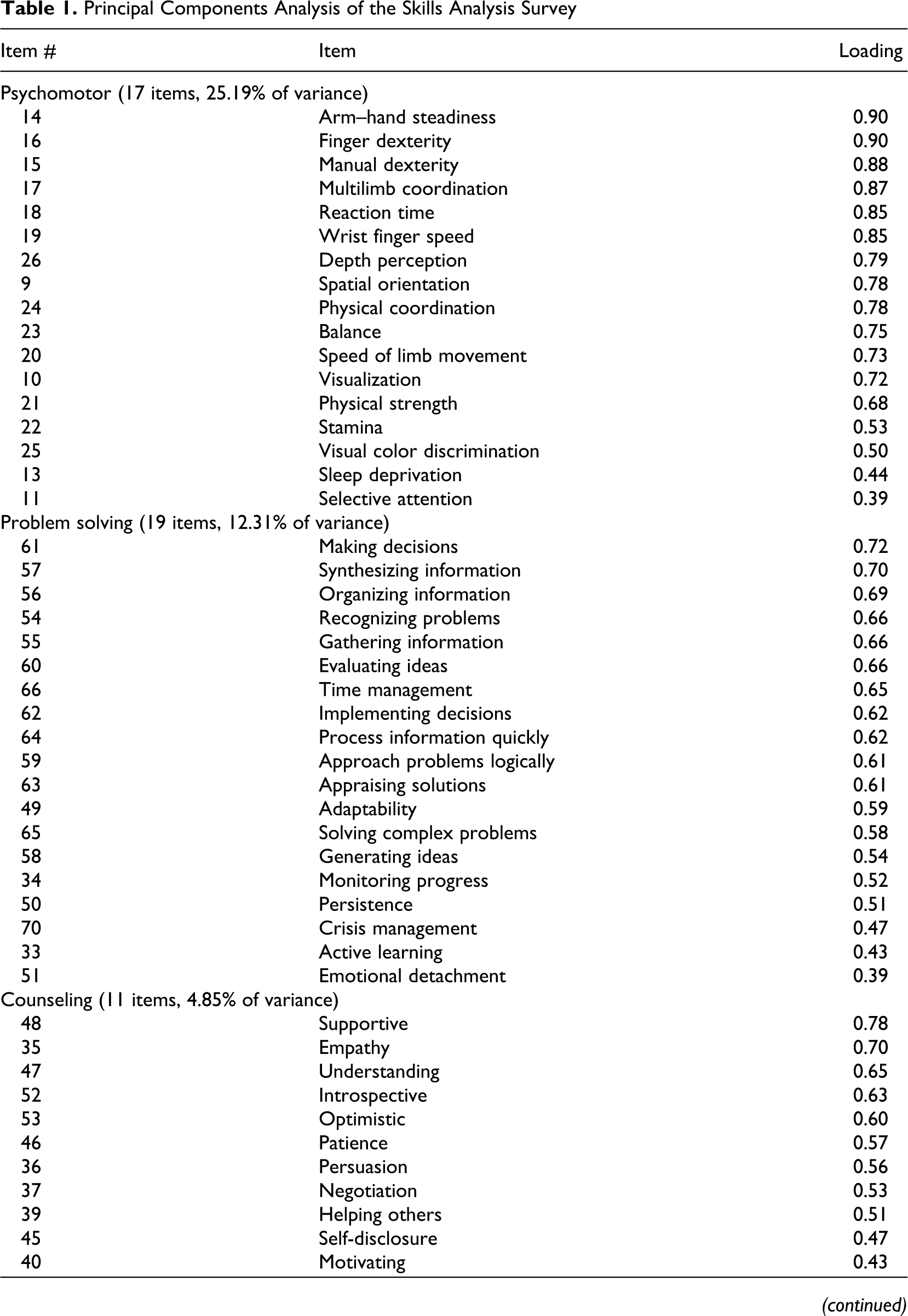
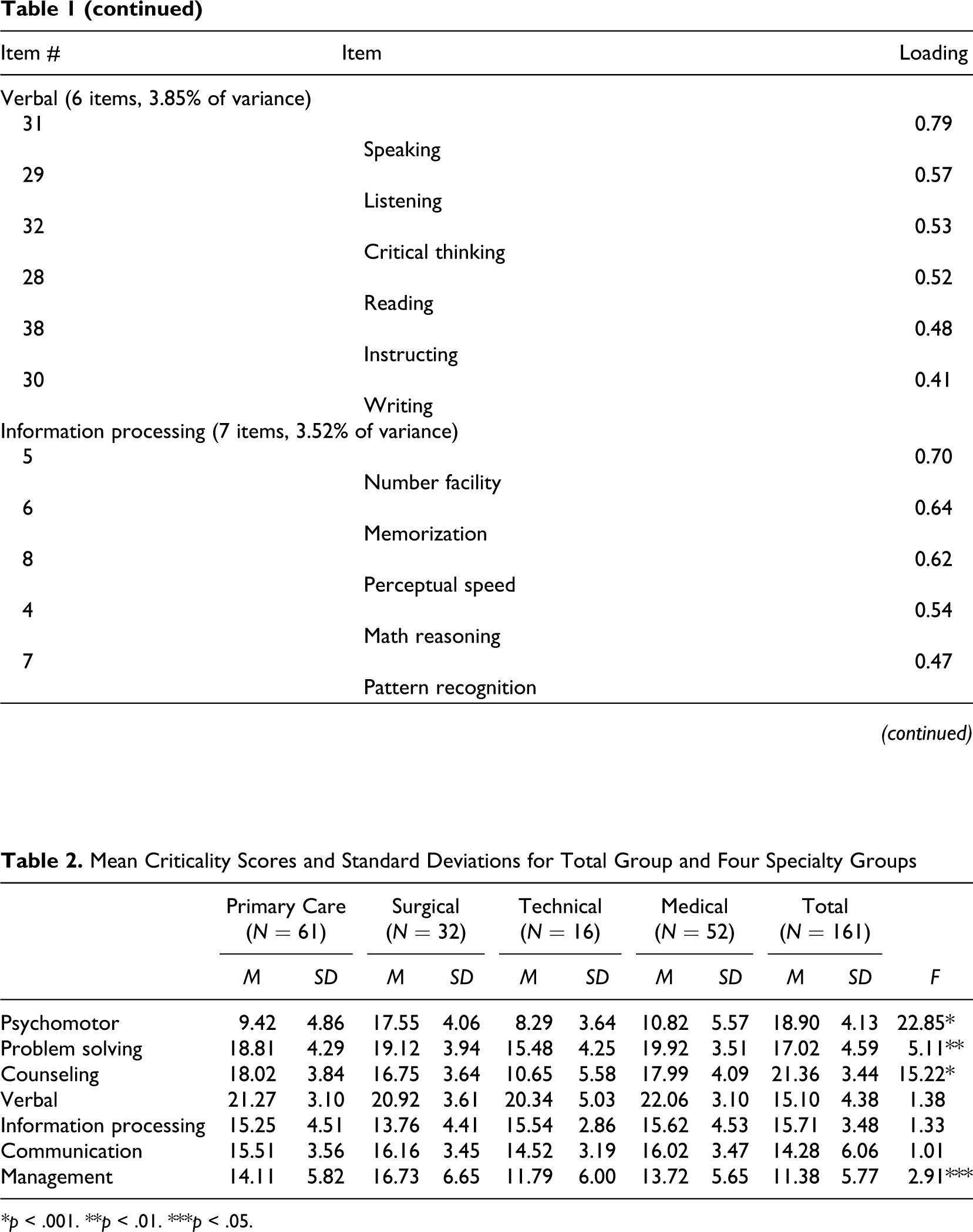
Among these 7 components, the first 3 major components contained 19, 17, and 11 items. The remaining 4 minor components contained 7, 7, 6, and 3 items. Table 1 presents the item loadings for each of these 7 components, which, upon review, seemed to correspond to the following skills: psychomotor (17 items, 25.19% of variance), problem solving (19 items, 12.31% of variance), counseling (11 items, 4.85% of variance), verbal (6 items, 3.85% of variance), information processing (7 items 3.52% of variance), communication (7 items, 3.02% of variance), and management (3 items, 2.91% of variance).
Principal Components Analysis of the Skills Analysis Survey
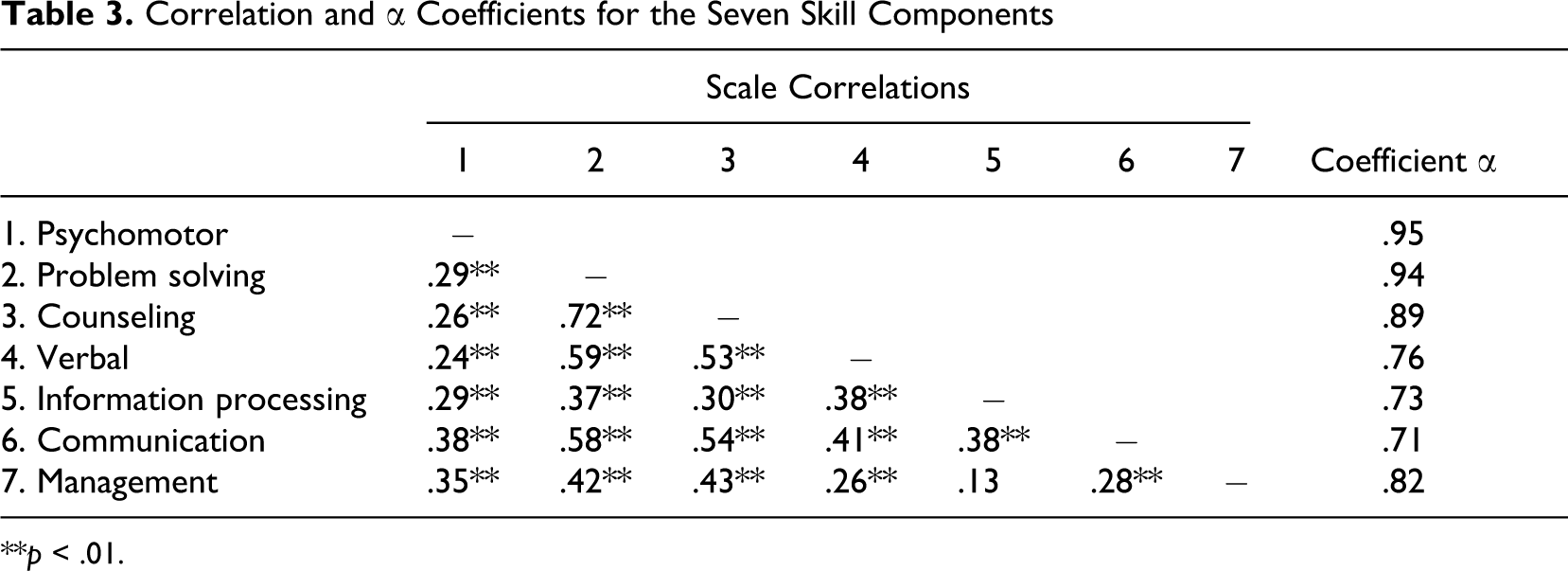
To examine the homogeneity of the skills in each of the components, we calculated Cronbach’s α coefficients: psychomotor = .95, counseling = .89, problem solving = .94, verbal = .76, information processing = .73, communication = .71, and management = .82. The coefficients were used to check the homogeneity of the items in each category, not to treat the groups of skills as if they were scale items in a psychometric inventory. We also examined the interrelationships between the seven categories using Pearson product–moment correlations for each category pair. These correlations appear in Table 2 . They were all significant with the exception of the correlation between the management and information skills factors. The magnitude of the correlations was moderate, with the strongest association occurring between problem solving and counseling skills (r = .72).
Mean Criticality Scores and Standard Deviations for Total Group and Four Specialty Groups
*p < .001.
**p < .01.
***p < .05.
Correlation and α Coefficients for the Seven Skill Components

**p < .01.
Mean criticality scores were then calculated for each of the seven components for all physicians and for each of the four specialty groups (see Table 2). Using these scores we conducted a post hoc analysis to examine skill rating differences across four groups of medical specialties. Although not the intent of the study, we looked for patterns in the data. We were cautious in interpreting the meaning of these patterns because they were not specified a priori and when one looks for something they are more likely to see it. Nevertheless, the results of the post hoc using multivariate analysis of variance ([MANOVA] as reported in Table 1) suggested that the surgical specialties seem to require greater psychomotor, problem-solving, and management skills. The technical specialties appear to require more verbal and less counseling, problem-solving, and psychomotor skills. Possibly, the technical specialties are defined better by highly specific skills, rather than generic transferable skills. The medical specialties appear to require slightly more counseling and slightly less psychomotor skills, but statistically significant differences were not found on the seven scales between the primary care and medicine specialties. While this may indicate support for combining these two groups of specialties into a single large group, their daily work involves significantly different activities and patient orientations. The likely reason for the lack of distinction between the two groups is that to enter any of the medical specialties, one must first complete training in internal medicine, which is considered a primary-care specialty by most medical specialty experts. Thus, while medical specialists may share common skill requirements with primary-care physicians, the services they provide differ substantially, thereby supporting the need to keep the two groups separate.
Discussion
Based on the results of the principal components analysis, we concluded that three major sets of transferable skill sets may define the practice of medicine among the four groups of specialties. They contained twice as many items as the four minor skill sets, had higher α coefficients, and the scree plot indicated that they may be a preferred interpretation of the data. The three major skill sets deal with psychomotor ability, problem solving, and counseling. Psychomotor skills consist of well-coordinated physical movements and precise manipulations. Sample items include arm–hand steadiness, finger dexterity, manual dexterity, reaction time, and multilimb coordination. These skills can be acquired and learned through repeated performance; practice makes perfect. Problem-solving skills consist of intellectual capacities to resolve novel, ill-defined problems in complex real-world settings. Sample items include gathering information, synthesizing information, evaluating ideas, making decisions, and implementing decisions. Counseling skills involve professional guidance using psychological methods and interview techniques to help patients work through their issues. Sample items are support, empathy, persuasion, understanding, and patience.
The three major skill sets for the practice of medicine coincide with three of the personality types in Holland’s theory of personality and work environments (Holland, 1997). Holland’s theory distinguishes six types: realistic, investigative, artistic, social, enterprising, and conventional. Holland classifies occupations by a vector of resemblance to these six types. According to his classification physicians resemble, in descending order, investigative, realistic, and social types (Gottfredson & Holland, 1996). This classification system utilizes a coding scheme based on the first letter of each of the six types. In this scheme, physicians would be classified as IRS.
There is a clear and coherent relationship between the three major skill sets and these three Holland types. Psychomotor skills, such as manual dexterity, physical coordination, and reaction time, are required for effective performance in realistic occupations. Problem-solving skills, such as gathering information, evaluating alternatives, and making decisions are required for effective performance in investigative occupations. Finally, counseling skills such as helping others, being supportive, and offering empathy are required for effective performance in social occupations. Based on our results, we think that all physicians need to develop the three skill sets. The investigative or problem-solving skills appear to be central to the work of all physicians, and of course it is the first letter in the IRS code. The realistic and social skill sets may be differentially used in particular medical specialties. Some specialties require more counseling skills, while others require psychomotor skills—the difference being accounted for by degree of involvement with people versus equipment. Thus, we think that the primary care and medical specialties may require more highly developed social and counseling skills (and might be coded ISR) and the technical and surgical specialties may require more highly developed realistic and psychomotor skills (and might be coded IRS).
To flesh out the vector of resemblance to the RIASEC types, we considered the correspondence of the four minor components to Holland’s theory of personality types. Certainly the management skill items fit well with Holland’s enterprising type and seem critical to effective performance for physicians who eventually work in public health or in administrative positions. The information processing skill set seems to fit with Holland’s conventional type because it includes attention to detail, perceptual speed, and pattern recognition. The communication skill set matches somewhat with Holland’s artistic type because it includes originality, creativity, and aesthetics. It would be interesting in further research to investigate the correlations between these six skill scales and scores for Holland’s six vocational personality types and work environments. The verbal scale seemed to represent basic or generic skills that are important in all six of Holland’s work environments.
Based on the principal component analysis and Holland’s (1997) theory of personality types, we decided to construct the physician skills inventory using just the 47 items from the 3 major components and naming the 3 sets of transferable skills for medicine as investigative skills, realistic skills, and psychosocial skills (see Appendix A). Each of the 47 items presents a skill and its description, and medical students are instructed to rate their competence for each skill on a scale from 1 (little or no skill) to 5 (exceptional skill). To provide students with insights into their skill strengths and weaknesses for the practice of medicine, their results are presented as their score for each item as well as the item mean score for each of the three skill sets. In addition to increasing self-awareness, the results are intended to help students improve their knowledge and understanding of the basic skills necessary for everyday practice of medicine. Students may also consider the balance of realistic skills versus social skills as they think about potential specialty choices.
Career counselors and medical school faculty may use the inventory to assist students identify and remediate skill deficiencies. Students must realize that cross-functional medical skills are developed capacities that, with practice, they may learn and master. For example, a student considering the specialty of psychiatry who scores low on the counseling skill set may still prepare to enter that specialty, yet would do well to seek opportunities to practice and improve her or his counseling skills. Most medical schools offer training to develop students’ capacity to respond empathically to patients. If students need to learn or develop this skill, they could seek additional training, tutoring, and practice. A similar path could be followed by a student with poorly developed psychomotor skills who is interested in surgery. For career counseling, we propose that advisors compare the results from the medical skills inventory to results from the Medical Specialty Preference Inventory, an interest inventory offered as part of the Association of American Medical Colleges (AAMC) Careers in Medicine Program (Richard, 2005), so that students may consider how well their specialty interests match their current skills, and if needed enact a skill-improvement plan. In short, the physician skills inventory should be viewed as prescriptive not diagnostic.
A number of limitations exist in this study. The results of the principal components analysis would have been more strongly supported with a larger pool of respondents. Statisticians recommend a minimum of four or five participants per item when conducting a principal components analysis, which would indicate approximately 280–350 participants needed for this analysis. Although the number of participants was small for sophisticated data analyses, collecting data to refine a skills checklist remains the strength of this study because it is a rare occurrence. Also because of the size of the sample, individual specialties could not be examined in the post hoc analysis, requiring us to group the specialties into the four specialty types (primary care, medical specialties, surgical specialties, and technical specialties). While this grouping is not unusual, it limits any analysis of individual specialty variations in skills. Future research should examine variations in skill requirements across specialties to provide students with an expanded ability to explore the skills required in desired specialties.
The physicians who participated in this study were regionally homogenous and generally represented only physicians working at community-based hospitals in the Midwest. The ability to generalize to other regions of the country and to other types of medical institutions, such as academic medical centers and private practice, may be limited. However, because the majority of physicians in the United States work in community settings, these results may be more representative of a larger portion of the physician population than might be expected. Finally, this study does not address knowledge obtained during the course of one’s educational program. It correctly assumes that the medical profession has sufficiently established the knowledge and learning required for success and assesses this knowledge by following well-established educational standards.
Our results support the initial development of a research edition of a self-report instrument that assesses medical students’ basic and cross-functional skills. With further research the ability to compare a student’s results to skills profiles of different specialties to determine those that fit, or match, the students’ skills could become a reality. Incorporating the physician skills inventory into a comprehensive career planning and decision-making system, such as the AAMC Careers in Medicine program, which offers additional self-assessment resources, can provide strong guidance and support in the process of matching one’s skills to the requirements of the work of a physician.
Footnotes
Appendix A
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.