
Abstract
In this study, the authors focused on the context of physical disabilities (i.e., one’s age when a disability manifests and the severity with which it impacts major life activities) to better understand how disabilities influence vocational self-efficacies. Consistent with Social Cognitive Career Theory, age of onset moderated the relationship between disability severity and self-efficacies in the Realistic, Artistic, Social, and Conventional vocational domains. Specifically, disability severity had a strong, negative impact on self-efficacies for people who became physically disabled later in life. In contrast, the relationship between disability severity and self-efficacy was nonsignificant for people who became disabled in early childhood. These findings held across Holland’s Realistic, Investigative, Artistic, Social, Enterprising, and Conventional domains when controlling for a variety of other person inputs and domain-specific learning experiences.
Keywords
Much vocational research emphasizes the effects of person inputs, like gender and ethnicity, and background affordances, like social support networks, on career development. In particular, Lent, Brown, and Hackett’s (1994) Social Cognitive Career Theory (SCCT) describes the ways in which these personal factors impact people’s capacity to develop self-efficacies and make effective career choices. For example, recent research on SCCT has demonstrated that inputs such as gender (Williams & Subich, 2006), race and ethnicity (Fouad & Byars-Winston, 2005; Tokar, Thompson, Plaufcan, & Williams, 2007), sexual orientation (Fisher, Gushue, & Cerrone, 2011; Morrow, Gore, & Campbell, 1996), personality (Schaub & Tokar, 2005), and, more recently, socioeconomic status (SES; Diemer et al., 2010; Thompson & Dahling, 2010, 2012) all affect vocational processes.
In this study, we consider physical disabilities as a person input in SCCT. Within the vocational literature, disabilities have received less attention than other person inputs; a recent review by Foley-Nicpon and Lee (2012) indicated that less than 3% of the research published between 1990 and 2010 in major counseling psychology journals concerned disabilities. Further, of the 55 articles identified in their review, only 18 involved empirical analyses of quantitative or qualitative data. The limited existing research on disabilities has also generally focused on cognitive and learning disabilities to the exclusion of physical disabilities (e.g., Dipeolu, Reardon, Sampson, & Burkhead, 2002; Ochs & Roessler, 2004; Smith & Milson, 2011). As noted by Buist-Bouwman and colleagues (2006), physical disabilities pose different vocational challenges and warrant unique attention. For example, physical disabilities can introduce mobility restrictions and discrimination that may inhibit access to learning experiences and self-efficacies in a variety of performance domains, consistent with SCCT (Lent et al., 1994; Lindley, 2006; Szymanski, Enright, Hershenson, & Ettinger, 2003).
In addition, existing research on physical disabilities tends to focus on the effects of disability status by making between-group comparisons of people with a physical disability to people with other types of disabilities (e.g., Yanchak, Lease, & Strauser, 2005) or to people who do not have disabilities (e.g., Lusk & Cook, 2009; Luzzo, Hitchings, Retish, & Shoemaker, 1999). Focusing on between-group comparisons is problematic because this approach ignores contextual aspects of physical disabilities (e.g., their perceived severity and when they developed), which may explain important within-group variability in outcomes among the population of adults with physical disabilities (e.g., Moore, Konrad, Yang, Ng, & Doherty, 2011). For example, Noonan and colleagues conducted a qualitative study of highly achieving women who all possessed physical or sensory disabilities (Noonan et al., 2004). They found that their participants faced varying challenges and had different types of experiences that highlight the value of studying within-group differences among adults with physical disabilities. Accordingly, in this study we advance research on SCCT by examining how the contextual features of a disability yield different patterns of vocational self-efficacies among adults with a variety of physical disabilities.
Literature Review
Overview of Social Cognitive Career Theory
SCCT (Lent et al., 1994) is an extension of Bandura’s (1986) general Social Cognitive Theory to vocational processes. Bandura’s Social Cognitive Theory sought to explain the mutual interaction of human agency, behavioral choices, and environment. The theory assumes an adaptive, agentic model of human behavior in which individuals are capable of influencing and affecting their surroundings (Bandura, 1986, 2000). SCCT expands this to explore how people exercise their agency in the career development process (Lent, Brown, & Hackett, 2000; Lent et al., 1994). SCCT provides a framework for three important social cognitive functions that enable agency and guide an individual’s career development: self-efficacy beliefs, outcome expectations, and learning experiences. These three constructs interact in a continuous loop and inform individuals’ subsequent career decision making (Lent, 2005; Lent et al., 1994).
Bandura (1986) defined self-efficacy as “people’s judgments of their capabilities to organize and execute courses of action required to attain designated types of performance” (p. 391). Judgments about self-efficacy are dynamic and change depending on the performance domain in question. Self-efficacy has received extensive attention in the career development literature because it is regarded as the strongest determinant of vocational beliefs, decisions, and career-related goals (e.g., Chemers, Zurbriggen, Syed, Goza, & Bearman, 2011; Conklin, Dahling, & Garcia, 2013; Rogers & Creed, 2011). According to SCCT’s pathways, when pursuing a career path based on a strong sense of self-efficacy and positive outcome expectations, people form related interests and goals and then take actions to arrive at these objectives. SCCT posits that people assess their subsequent performance, which creates a feedback loop that continues to shape self-efficacy. As people learn about their capabilities and observe the outcomes of their behaviors, their self-efficacy judgments, interests, and goals change in a constantly dynamic, evolving process (Lent, 2005; Lent et al., 1994).
The choice model of SCCT also describes person inputs and affordances that influence vocational processes (Lent, 2005; Lent, Brown, Brenner et al. 2001; Lent, et al., 1994, 2000). Person inputs are enduring characteristics, such as race, gender, and disabilities, which shape the types of learning experiences that an individual is likely to experience. Learning experiences are further qualified by background affordances, such as opportunity structures and socialization. Person inputs also shape later contextual affordances (i.e., situational barriers and supports; Dahling & Thompson, 2010) that people might experience. For example, the person input of race influences the extent to which a person is likely to experience discriminatory treatment, which might dissuade interests and goals in the domain where discrimination was experienced.
Disabilities in Social Cognitive Career Theory
The effects of experiences with physical disabilities on self-efficacy are largely understudied as indicated by a recent review of the self-efficacy literature by Lindley (2006). These effects are important because they can inhibit individuals’ subsequent career choices and vocational development (Hutchinson, Versnel, Chin, & Munby, 2008). Lowered self-efficacy, regardless of why it occurs, poses a variety of problems for individuals; research and theory asserts that less self-efficacious individuals tend to be less determined and committed to goals, more apprehensive, receive less pleasure and reward from their experiences, have lower intrinsic interest, set less challenging goals for themselves, and exhibit lower performance on many different tasks (Bandura, 1986; Bouffard-Bouchard, Parent, & Larivee, 1991; Schunk, 1984). Thus, understanding the conditions under which physical disabilities can detract from self-efficacy in SCCT is particularly important to understanding a variety of distal outcomes.
This research question is increasingly important, given a critical need for vocational rehabilitation and counseling for physically disabled war veterans, particularly in the United States (Drebing et al., 2012). Advances in medical practices have saved the lives of many veterans wounded in combat, who subsequently need additional supports to readjust to civilian work with a disability (Hendricks & Amara, 2008). Changes in employment laws have also resulted in more research interest in the personnel practices of employers regarding disabled candidates and employees (e.g., Fraser, Ajzen, Johnson, Hebert, & Chan, 2011) and the employment barriers that disabled employees sometimes encounter (Feldman, 2004).
One contextual factor related to physical disabilities that is important to consider is the age at which the disability manifested (Moore et al., 2011). Moore et al. noted that many studies on disabilities either discard data from participants who became disabled as children or ignore this contextual factor in their data altogether. Results from their study of workers with disabilities demonstrated that age of onset (which was simply operationalized as a dichotomous variable distinguishing between childhood or adult onset) moderated the effects of several different types of cognitive and physical disabilities on life satisfaction and perceived discrimination. These findings suggest that more nuanced research attending to the context of physical disabilities is needed.
A second contextual factor that has received little research attention from vocational psychologists is the severity of a physical disability. We define the severity of a disability in terms of its perceived impact on major life functions, which include, but are not limited to, communication with others, self-care, and mobility (Peterson, 2005; Üstün, Kostanjsek, & Chatterji, 2010). Critically, people with the same medical diagnosis may vary considerably in the perceived severity of a particular disability, which should have important impacts on self-efficacy as predicted by SCCT. Taken together, these findings highlight the importance of considering age of disability onset and perceived disability severity in vocational research.
Hypothesis Development
Building on the limited research on the context of physical disabilities in SCCT, we hypothesize that the severity of a physical disability and the age of onset will interact to influence vocational self-efficacies. Specifically, we predict that individuals who are disabled later in life and who perceive their disabilities to be severe will experience the lowest levels of self-efficacy. This expectation is grounded in social cognitive theory (Bandura, 1986) and SCCT (Lent et al., 1994), which both describe a feedback mechanism between domain performance and domain self-efficacy. Consistent with these theories, self-efficacy should be low when people perceive that their ability to perform major life functions has been restricted relative to their previous abilities; adults with late-onset, severe disabilities may contrast their current abilities with their abilities prior to become disabled, leading to lower self-efficacy judgments. A similar proposition was offered by Lindley (2006) who stated that “acquired disabilities … may arrest or alter a career path already in motion; negative vocational experiences attributable to discrimination in the workplace and/or loss of abilities may erode existing self-efficacy beliefs” (pp. 153–154). In contrast, people who develop a disability in childhood do not have existing, well-formed efficacy judgments to serve as a standard of comparison. Accordingly, the perceived severity of a disability should not influence their self-efficacy judgments later in life as adults (Feldman, 2004; Lindley, 2006).
The specific self-efficacies that we examined are from Holland’s (1959, 1996) Realistic, Investigative, Artistic, Social, Enterprising, and Conventional (RIASEC) framework. Holland theorized that vocational learning experiences, self-efficacies, outcome expectations, and interests can be organized into six types: Realistic, Investigative, Artistic, Social, Enterprising, and Conventional. We focus on the RIASEC framework in this study because it captures the broadest range of occupational efficacies. Furthermore, this choice connects our study to past research that has examined RIASEC interests among adults with disabilities (Rohe & Krauss, 1998; Turner, Unkefer, Cichy, Peper, & Juang, 2011). These studies showed that individuals with disabilities differ somewhat in their occupational interests (e.g., having lower social interests; Rohe & Krauss, 1998), when compared to individuals without disabilities, and that many people with disabilities work in jobs that do not have a good match to their interest profiles (Turner et al., 2011). Our focus on RIASEC self-efficacies in this study may help explain some of these findings concerning RIASEC interests in previous work.
We hypothesize that age of onset and disability severity will have an interactive relationship with self-efficacies in the (a) Realistic, (b) Investigative, (c) Artistic, (d) Social, (e) Enterprising, and (f) Conventional areas, with the lowest self-efficacy reported when self-rated severity is high and the age of onset occurs later in life. To provide a strong test of these hypotheses, we control for other person inputs (gender, age, education level, and childhood SES) and RIASEC learning experiences in each analysis, consistent with SCCT.
Method
Participants
Participants consisted of 153 individuals with physical disabilities residing in the United States. The mean age was 38.89 (standard deviation [SD] = 13.73, range of 18–73), and women comprised 59.1% of the sample. The sample was 6.8% Hispanic or Latino/Latina. With respect to race, 88.6% of the participants identified as Caucasian, 4.5% as African American, 3.1% as Asian American, 3% as Native American or Alaskan, and 0.8% as members of other groups. When asked about their employment status, 21.2% of the participants reported working full time, 21.2% worked part time, and 57.6% were unemployed. Concerning their level of education, 42.4% of the participants reported obtaining less than an undergraduate degree (high school diploma/GED, and/or some college), while 44.7% had undergraduate degrees and 12.9% had graduate-level degrees. We asked the participants to estimate their SES today and when they were growing up; 0% described their current SES as upper class, 9.1% as upper middle class, 38.6% as middle class, 32.6% as lower middle class, and 19.7% as lower class. While they were growing up, 0.8% of the participants were upper class, 21.2% were upper middle class, 47% were middle class, 22.7% were lower middle class, and 8.3% were lower class.
We asked participants to describe their disabilities in an open-ended question, with a special emphasis on reporting any formal medical diagnoses. We rationally coded the resulting narrative descriptions into nine categories agreed upon by the authors, with 28.8% (n = 38) involving injuries or deformities of the spine or central nervous system (e.g., spinal muscular atrophy or spinal bifida), 17.4% (23) involving joint and connective tissue injuries or deformities (e.g., Ehlers-Danlos syndrome or severe osteoarthritis), 9.8% (13) involving paralysis and serious mobility restrictions (e.g., polio-related paralysis or paraplegia), 8.3% (11) involving amputation of a limb or appendage, 8.3% (11) with cardiovascular disorders or deformities (e.g., acute endocarditis or pulmonary hypertension), 7.6% (10) with chronic pain or fatigue disorders (e.g., fibromyalgia), 7.6% (10) with severe autoimmune and inflammatory disorders (e.g., lupus or multiple sclerosis), 6.1% (8) with sensory injuries or deformities (e.g., aniridia or deafness), and 6.1% (8) serious disorders of other organs and systems (e.g., kidney failure requiring dialysis or type 1 diabetes with mobility complications). We made these categorizations so that we could later ascertain whether specific types of disabilities were associated with higher or lower levels of our variables of interest.
Measures
Severity of Physical Disabilities
The 12-item version of the World Health Organization Disability Assessment Schedule II (WHODAS 2.0) was used to determine the severity of participants’ physical disabilities (Üstün et al., 2010; Üstün, Kostanjsek, & Chatterji, 2010). The WHODAS 2.0 was developed from a set of International Classification of Functioning, Disability and Health (ICF) items and is used to measure health and disability across cultures. The measure covers six major life domains that disabilities may impact: cognition (e.g., understanding others), mobility (e.g., being able to get around), self-care (e.g., unassisted hygiene and eating), getting along (e.g., interacting with other people), life activities (e.g., domestic responsibilities and work), and participation (e.g., joining in community activities). Respondents indicated their difficulty performing major life functions on a 5-point scale ranging from 1 (none) to 5 (extreme or cannot do). Sample questions include “Standing for long periods such as 30 minutes?” “Concentrating on doing something for ten minutes?” and “Maintaining a friendship?” Scale scores were computed by summing all responses with a possible score range of 12–60, where higher scores indicate more severe disabilities.
The WHODAS 2.0 can be administered with either a 12-item version, which we used, or a 36-item version that elaborates on the same six major life domains. We opted to use the 12-item version consistent with instructions in the WHODAS 2.0 manual, which reports that the 12-item version explains 81% of the variance of the 36-item version and is preferable when assessments of overall functioning are desired (Üstün et al., 2010, p. 16). Permission to use the WHODAS 2.0 was requested from the World Health Organization (WHO) consistent with instructions.
Validation research (Garin et al., 2010; Üstün, Kostanjsek et al., 2010) shows that the WHODAS 2.0 is moderately correlated with the Short Form-36 Health Survey that contains questions pertaining to similar criteria. Internal consistency was demonstrated to be .96 for the 36-item scale by Üstün, Kostanjsek, and Chatterji (2010). The study also provided evidence for the concurrent validity of the WHODAS 2.0 using the WHO Quality-of-Life measure, the London Handicap Scale, the Functional Independent Measure, and the Short Form Health Survey. The reliability found for the 12-item version in our study was α = .87.
Learning Experiences
The Learning Experience Questionnaire (LEQ) was used to measure participant’s RIASEC learning through performance accomplishments, vicarious learning, verbal persuasion, and physiological arousal (Schaub, 2004). The LEQ contains 20 items for each of the six RIASEC areas for a total of 120 items. Of the 20 items in each area, 5 inquire about performance accomplishments, 5 about vicarious learning, 5 about verbal persuasion, and 5 about physiological arousal. All items are reported on a 6-point Likert-type scale ranging from 1 (strongly disagree) to 6 (strongly agree). Sample items include “I have made simple car repairs” (realistic performance accomplishments), “In school, I saw teachers whom I admired work on science projects” (investigative vicarious learning), and “People whom I respect have encouraged me to play a musical instrument” (artistic verbal persuasion). Scores were computed for each RIASEC area by averaging the full set of 20 items, yielding a possible score between 1 and 6; higher scores indicate more learning experiences in the domain.
Internal consistency reliabilities for the LEQ scales have been shown to be more than .70 for all domains (Schaub, 2004; Schaub & Tokar, 2005; Thompson & Dahling, 2012; Tokar et al., 2007; Williams & Subich, 2006). Schaub and Tokar (2005) also found that LEQ scores are strong predictors of self-efficacy. The reliabilities found in this study were α = .89 for realistic learning, α = .88 for investigative, α = .78 for artistic, α = .85 for social, α = .88 for enterprising, and α = .81 for conventional.
Self-Efficacy
The Self-Efficacy Questionnaire (SEQ) was used to measure participants’ RIASEC self-efficacies (Lenox & Subich, 1994). The SEQ includes 5 items for each of the six RIASEC categories for a total of 30 items. Participants were asked to indicate their degree of confidence in completing various activities on a 10-point scale ranging from 1 (completely unsure) to 10 (completely sure). Examples of these activities include “helping people who are upset or troubled” (social), “using algebra to solve mathematical problems” (investigative), and “operating power tools such as a drill press or grinder or sewing machine” (realistic). Scores were computed for each RIASEC area by averaging the full set of 5 items, yielding a possible score between 1 and 10; higher scores indicate more self-efficacy in the domain.
Williams and Subich (2006) found reliabilities for the SEQ ranging from .60 to .90 for the RIASEC themes. Betz and Gwilliam (2002) also found correlations between the SEQ and similar scales ranging from .59 to .81. The reliabilities in this study were α = .87 for realistic self-efficacy, α = .90 for investigative, α = .87 for artistic, α = .88 for social, α = .90 for enterprising, and α = .89 for conventional.
Procedure
Participants were recruited using an online participant pool called Amazon Mechanical Turk (MTurk; http://www.mturk.com). MTurk was developed in 2005 by Amazon.com, Inc., to pair up volunteer “workers” with “employers” who require large groups of people to complete short computerized tasks for business or scholarly purposes. Participants in this study received 80 cents for a complete response to the survey; typical payments on MTurk range from US$.01 up to US$1.00 for a more time-consuming task (Buhrmester, Kwang, & Gosling, 2011). We recruited through MTurk because it allows access to a very wide set of potential respondents with special characteristics, such as physical disabilities, who would otherwise be difficult to sample; at present, over 500,000 people are registered MTurk workers and eligible participants in studies. Moreover, several recent studies (e.g., Buhrmester et al., 2011; Mason & Suri, 2012; Paolicci, Chandler, & Ipeirotis, 2010) have found that the demographic diversity of respondents on MTurk and the quality of data available through the system closely parallel or exceed those found with matched samples recruited in person. These studies also found that the measurements collected using MTurk show good reliability and factorial stability over time.
Eligible participants were restricted through screening filters to be U.S. residents, to have a physical disability, and to not have a complicating psychological, learning, or mental disability. We restricted access among adults with these complicating conditions so that we could isolate the relationships of physical disabilities with self-efficacies. To ensure that our data would be viable, we embedded several quality-control items in longer questionnaires to confirm that participants were carefully attending to the survey (e.g., “Please select ‘strongly disagree’ as the answer to this question”). Repeat IP addresses and MTurk worker identification numbers were blocked to prevent duplicate responses from the same person. In addition to the U.S. residency requirement, we screened participants on the basis of their self-rated comfort with the English language to remove data for any participants who may have misinterpreted the survey items. Participants who finished the survey unreasonably quickly (i.e., in less than five minutes) were also excluded, given a low likelihood that they could have feasibly read the items closely. Finally, participants who gave descriptions of their disability that were too vague to categorize (e.g. “skin”) or that did not qualify as physical disabilities (e.g. “OCD”) were dropped as well. Based on these checks, we excluded data from three participants who reported low English proficiency, eight who missed one or more of the quality-control questions, two who finished the survey too quickly, and eight whose disability descriptions were too vague or did not qualify. Thus, we had a final sample of 132 responses for hypothesis testing (86.5% of the original sample of 153 responses).
Results
We began our analysis by evaluating the sample to determine whether mean scores on the WHODAS 2.0, LEQ, or SEQ varied across the different disability groupings that we identified (e.g., spinal/central nervous system injuries vs. joint and connective tissue disorders). We conducted a one-way analysis of variance on these self-report measures using the disability category as our factor of interest. No significant mean differences emerged between any of the groups for any of the dependent variables, so we combined the full sample for all analyses that follow.
Table 1 reports correlations and descriptive statistics for demographic and self-report items. As shown in the table, disability severity (WHODAS 2.0 scores) is generally unrelated to either learning experiences or self-efficacy across RIASEC domains. However, other person inputs in the table, particularly gender and age, are related to several dimensions of learning experiences and self-efficacy, consistent with SCCT (Lent et al., 1994). Moreover, learning experiences in a particular RIASEC domain are strongly correlated with self-efficacy in that domain, consistent with previous research (e.g., Schaub & Tokar, 2005).
Means, Standard Deviations, and Correlations Between Measures.

Notes. Internal consistency estimates are reported on the diagonal. WHODAS = disability severity score; LE = learning experiences; SE = self-efficacy; R = Realistic; I = Investigative; A = Artistic; S = Social; E = Enterprising; C = Conventional. For gender, 1 = male and 2 = female. For education level, 1 = less than an undergraduate degree, 2 = undergraduate degree, and 3 = graduate degree.
* p < .05. ** p < .01.
We tested our hypotheses concerning the interactive effects of disability severity and age of onset on RIASEC self-efficacies using hierarchical moderated multiple regression. Following practices outlined by Aiken and West (1991), we mean centered both disability severity and age of onset prior to creating the interaction term. To provide a strong test of the hypothesis for each type of self-efficacy, we controlled for other person inputs in Step 1 (gender, age, childhood perceived SES, and education level) and learning experiences in the same domain in Step 2. We then entered the centered main effects of disability severity and age of onset in Step 3 and the interaction term in Step 4. Table 2 summarizes the results of these analyses for each RIASEC self-efficacy. As shown in this table, the interaction term had significant effects on self-efficacy in the Realistic, Artistic, Social, and Conventional domains and approached significance in the Enterprising domain (p = .06). Self-efficacy in the Investigative area was not predicted by the interaction. The effect sizes for the interaction terms ranged from 1% (enterprising) to 7% (artistic), which are quite strong for interactions (Frazier, Tix, & Barron, 2004). Overall, the full set of predictor variables explained between 43% (Social) and 67% (Artistic) of the variability in the self-efficacies, with learning experiences emerging as the strongest predictor in each analysis.
Results of Moderated Multiple Regression Analyses.

Notes. DVs = Dependent Variables; SES = socioeconomic status. For gender, 1 = male and 2 = female. For education level, 1 = less than an undergraduate degree, 2 = undergraduate degree, and 3 = graduate degree.
*p < .05. **p < .01. † p < .10.
We probed the significant interaction terms following Aiken and West (1991) by plotting the interaction at high and low levels of disability severity and age of onset (+1 SD and −1 SD, respectively). Because all of the interactions took a similar form, we present only the interaction for Social self-efficacy as an example (Figure 1). As shown in the figure, for participants whose disability manifested at an early age (−1 SD, or approximately 8.42 years old), the relationship between disability severity and Social self-efficacy is not statistically significant (simple slope t = −0.38, p = .70). However, for participants whose disability manifested later in life (+1 SD, or approximately 41.80 years old), the relationship between disability severity and Social self-efficacy is negative and significant (t = −3.91, p < .001). Similar findings were evident for the Realistic, Artistic, Enterprising, and Conventional domains, with participants who were disabled early in life exhibiting no significant differences in self-efficacy regardless of disability severity. In contrast, participants who were disabled later in life showed a moderate to strong, negative relationship between disability severity and self-efficacy. Thus, our hypotheses were supported with the exception of self-efficacy in the Investigative area.
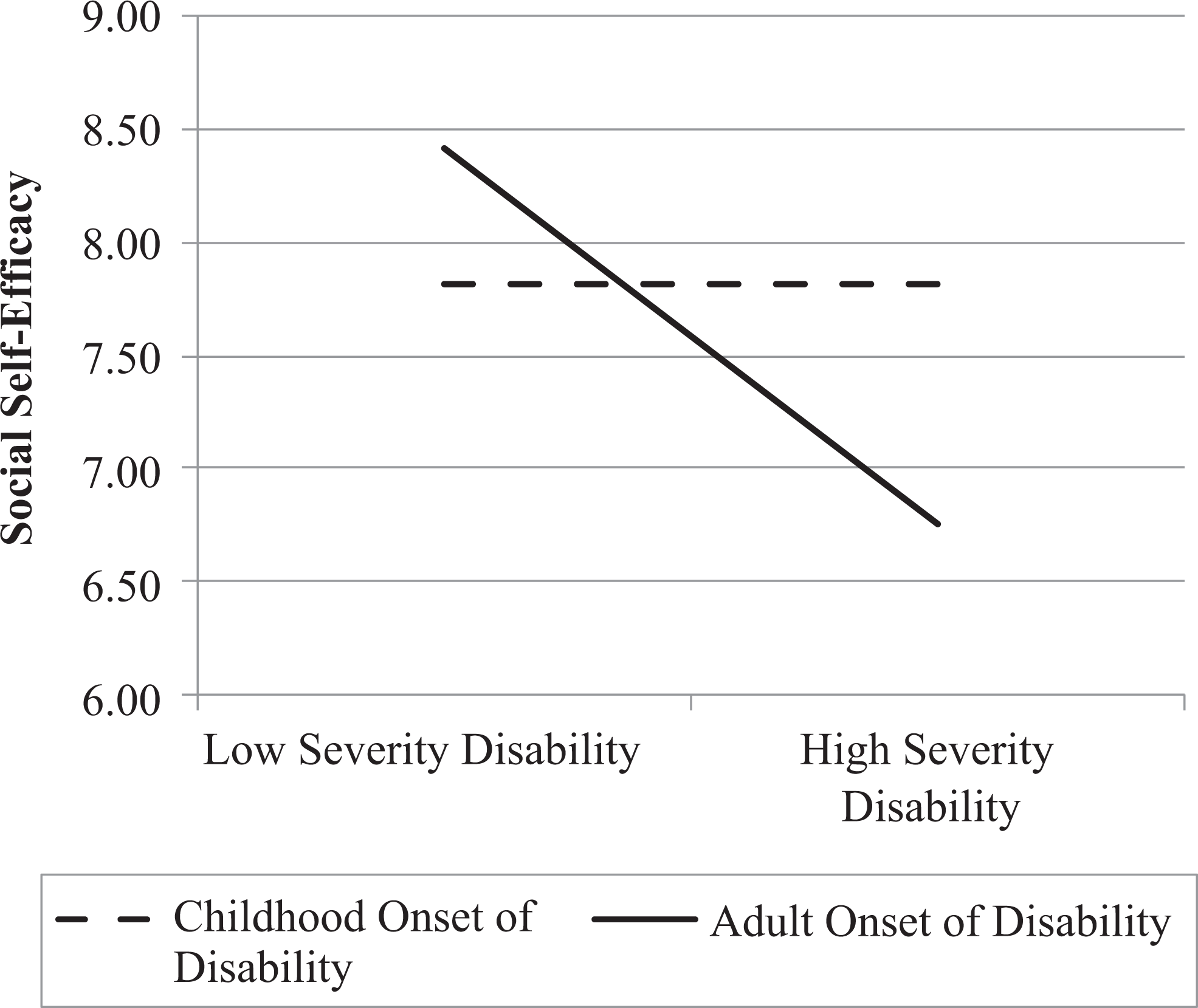
Interaction of severity of disability and age of disability onset predicting Social self-efficacy.
As an exploratory analysis, we tested the effects of the disability severity and age of onset interaction on learning experiences in each domain. We conducted this analysis consistent with SCCT (Lent et al., 1994) to determine whether learning experiences act as a mediator of the relationships between the disability severity and the age of onset interaction and self-efficacies. However, we found no significant effects for the interaction on learning experiences after controlling for the same set of person inputs (gender, age, childhood SES, and education level) and the centered main effects. Thus, learning experiences could not mediate this relationship. Overall, the results show that the disability severity and age of onset interaction affects RIASEC self-efficacies independent of vocational learning experiences.
Discussion
Physical disabilities are understudied in vocational psychology, and previous research has shown that the effects of disabilities on vocational processes are rarely straightforward (Foley-Nicpon & Lee, 2012; Lindley, 2006; Moore et al., 2011). By evaluating the context of a physical disability, we demonstrated that the interactive effects of disability severity and age of onset have significant relationships with self-efficacy in the Realistic, Artistic, Social, and Conventional domains and approached conventional significance in the Enterprising domain. These relationships remained significant when controlling for a variety of other person antecedents derived from SCCT. Learning experiences, which operated independently of this interaction, exhibited the strongest relationships with self-efficacies. In total, our full set of predictor variables explained as much as 67% of the variability in self-efficacy scores (Artistic). The only domain in which the physical disability variables did not have or approach significant relationships was for Investigative self-efficacy.
These findings are important because they demonstrate that self-rated disability severity does not have a detrimental relation with vocational self-efficacies among those individuals who become disabled early in life. Consistent with social cognitive processes, we suggest that individuals who become disabled in childhood form their occupational self-efficacies in light of their disability. In contrast, individuals who become disabled later in life show a steeply negative relationship between self-rated disability severity and self-efficacies. A key proposition of social cognitive theory (Bandura, 1986) and SCCT (Lent et al., 1994) is that perceptions of domain-specific performance generate a feedback mechanism that shapes subsequent self-efficacy judgments. Consequently, adults who perceive that their late-onset disability has negatively impacted their ability to perform major life functions should report lower levels of self-efficacy in most RIASEC domains, consistent with our results.
Curiously, the interaction of disability severity and onset age had a significant or marginal relationship with all vocational self-efficacies, with the exception of the Investigative domain. This null finding may have occurred because the Investigative domain generally concerns knowledge acquisition, intellectual pursuit, critical analysis, and academic talent. The Investigative items in the SEQ, which involve actions such as solving math problems or performing a science experiment, are primarily focused on mental tasks that can be performed alone and that require minimal physical mobility. In contrast, all of the other domains as measured in the SEQ require physical mobility and/or interaction with others (which may present opportunities for discrimination). Thus, within the context of the domain as measured by the SEQ, physical disabilities may be irrelevant to Investigative self-efficacy (Holland, 1996; Lenox & Subich, 1994). However, future research on Investigative self-efficacy with a variety of different instruments is needed to confirm this finding.
We also found that the severity and age of onset interaction affected self-efficacy directly, rather than through learning experiences. Although SCCT positions disabilities as person inputs that shape learning experiences directly and self-efficacy indirectly, we found that the disability interaction affected self-efficacy directly and independently of learning experiences. We offer that perhaps disabilities, especially those that occur in adulthood, operate more like contextual affordances in SCCT rather than lifelong background variables. More recent research on SCCT acknowledges that contextual affordances do have direct effects on self-efficacies beyond those of learning experiences (e.g., Lent et al., 2001), which is consistent with our results. Further research on physical disabilities that is grounded in SCCT is needed to elaborate on these processes; it is likely that different vocational processes unfold depending on when in the life span one experiences a physical disability.
Directions for Future Practice
Our study offers several new directions for researchers and career counselors. We encourage practitioners to be sensitive to the context of a disability when providing vocational counseling to individuals with physical disabilities. We are not alone in making this observation; previous studies have called for counselors to exhibit greater sensitivity to the impact of disabilities on career development and recreational activities (e.g., Devine & Koch, 2003; Yanchak et al., 2005). However, while past research has documented that disability status impacts vocational self-efficacies (e.g., Luzzo et al., 1999), researchers have generally ignored the variations in experiences within the population of individuals with physical disabilities. Our results show that differences such as the perceived severity of the disability and the point in the life span at which it occurred are not negligible details. One implication of our findings is that counselors need to inquire deeply about the context of a disability to better understand the ways in which it might, or might not, be relevant to vocational development in a particular career domain.
Measures such as the WHODAS 2.0 (Üstün et al., 2010) provide a means for counselors to assess information about the daily impact of a disability. Aside from the WHODAS 2.0, a review article by Eby, Johnson, and Russell (1998) summarized the characteristics of several other assessment tools for use with clients with disabilities that practicing counselors may find useful. We also suggest that frameworks developed in rehabilitation psychology, particularly the ICF, offer useful conceptualizations for gaining a meaningful understanding of the context of a physical disability as it is experienced by a particular client (Peterson, 2005). For more details, we refer interested readers to Peterson and Elliott’s (2008) review chapter on conceptualizations of disabilities for an overview of the ICF and its use by counseling psychologists. The insights gleaned from these more specific assessments of physical disabilities can supplement existing process models for working with clients having disabilities (e.g., Klein, Wheaton, & Wilson, 1997).
Limitations and Future Research Directions
Despite the contributions of this article, we have several limitations to acknowledge. First, our design was cross-sectional and our findings should be replicated with repeated-measures designs over time to track changes in self-efficacy among children and adults with disabilities. Self-efficacy is a dynamic construct that changes based on performance feedback (Lent, 2005), and although self-efficacy may drop significantly after the adult onset of a disability, it is possible that it might gradually recover as individuals learn to adapt. Moreover, the effects of a physical disability may wax and wane over time. Consequently, it may have been difficult for some participants to identify the precise point at which their disability manifested. Longitudinal research would allow for a better examination of the changing relationship between disability severity and self-efficacy.
Furthermore, there are many individual differences that might offset the impact of disability on self-efficacy judgments. Traits such as resilience or optimism may buffer against self-esteem losses, particularly among adults who experience late-onset disabilities. Conversely, individual differences such as a maximizing decision-making style could exacerbate self-esteem losses (Dahling & Thompson, 2013). We did not measure any personality traits in this study that could qualify our findings, but future studies could examine the impact of these traits on self-efficacy recovery.
Our data collection strategy through MTurk introduces other potential limitations. First, although our sample was quite diverse with respect to physical disability types, gender, education, and perceived SES, the sample lacked diversity in regard to race and ethnicity. Future studies with more diverse samples of adults with disabilities are desirable. Additionally, recruitment of online participants may restrict access to participants with certain types of disabilities. For example, potential participants from low SES backgrounds and with sensory disabilities, like blindness, may have lacked access to the necessary assistive technology to participate in this study. Outreach to low-SES participants is particularly critical, given that social status and financial resources are also important person inputs and background affordances in SCCT (Lent et al., 1994). It may also be the case that individuals with disabilities who use MTurk differ from the broader population of adults with disabilities in ways that we have not considered. Consequently, our findings should be replicated with samples recruited through other means.
Conclusion
The results of this study point to a critical need for more research on physical disabilities and vocational processes. Disabilities are experienced and processed differently by each individual, and a consideration of this context is important to further develop theory and recommendations for practice. Self-efficacy development is a lifelong process informed by ongoing performance and experiences with work; as our knowledge of the constructs that influence this process improves, so will our ability to guide and assist clients with disabilities.
Footnotes
Authors’ Note
All three authors contributed equally to this article.
Acknowledgments
The authors thank Mindi N. Thompson for her helpful feedback on a previous version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a MUSE grant from The College of New Jersey.