
Abstract
End-of-life care is a form of unpaid care work that is primarily the responsibility of women and can affect their career development, employment, finances, and vocational success. This paper provides a review of the literature on the career and economic effects of providing unpaid end-of-life care for women caregivers. Illustrative reflections from women caregivers highlight challenging and positive aspects of providing end-of-life care. Challenges identified by the women caregivers included managing conflicting demands among work, home and caregiving as well as experiencing emotional strain, financial burden and economic instability. In addition, work schedules had to be altered and career trajectories were interrupted. Interestingly, caregivers reported receiving support from their employers and co-workers and few work-related benefits were used. Despite the many challenges in managing work and end-of-life care, many participants felt positively about their ability to provide a caring environment for a loved one at the time of their death. Recommendations for individual, familial, workplace, and societal changes related to unpaid end-of-life care will be provided.
The overwhelming amount of unpaid or underpaid care work done by women and girls (valued at over $10.8 trillion each year) contributes to global gender and economic inequality (Oxfam International, 2020). One type of unpaid work is end-of-life care, defined as caregiving that provides assistance to someone who is dying, typically in the last 6 to 12 months of life. The number of people providing end-of-life care in the United States is considerable and increasing given the aging population and the growing numbers of individuals who are dying at home (Cross & Warraich, 2019; MetLife Mature Market Institute, 2011). In 2011, 2.3 million people provided end-of-life assistance, and almost all (9 out of 10) were family members or unpaid caregivers (Ornstein et al., 2017). Women are much more likely than men to provide end-of-life care to family members—it is estimated that 61%–76% of end-of-life caregivers are women (Morgan et al., 2016; Ornstein et al., 2017; Washington et al., 2015).
The effects of end-of-life care are numerous and profound, spanning career, economic, physical and mental health, and relational domains. Women often experience negative consequences as a result of assisting those who are dying (Morgan et al., 2016; Washington et al., 2015). This paper will provide an overview of unpaid end-of-life care, propose several reasons for the high percentage of women engaged in this endeavor, describe the challenges and rewards associated with the provision of this care as indicated by a small sample of caregivers, and provide recommendations for how vocational psychologists can play a role in education, research, clinical interventions, and public policy related to women’s involvement in unpaid end-of-life care.
Vocational Psychology and Unpaid Care Work
Within vocational psychology, theorists have called for the transformation of our conceptualization of work and career (Blustein et al., 2004; Blustein, 2006, 2011; Richardson, 1993, 2012a, 2012b; Schultheiss, 2006, 2007). Specifically, Richardson advocated that the focus on work and career development be broadened to more holistically examine how lives are constructed. This reconceptualization acknowledges the salience of relationships and the importance of both paid and unpaid work. Often, unpaid care work is marginalized, devalued and not considered to be “work” (Richardson, 2012a). In Richardson’s narrative on this counseling for work and relationship perspective, four salient components of lives were identified including paid (market) work, unpaid care work (taking care of one’s personal needs, those of others and the community), personal relationships, and market work relationships.
Building on Giddens’ (1991) theory related to adaptations in self and identity and consistent with Super’s (1980) theory highlighting the importance of multiple life roles over the lifespan, Richardson (2012b) proposed that the way in which we construct our lives changes over time and in response to challenges and opportunities. The opportunity (or necessity) of providing end-of-life care could change the course of a life both relationally and vocationally. Furthermore, Richardson “goes beyond the interdependence of market work and relationships to focus on relationships themselves as social contexts through which people construct lives” (2012a, p. 203). The provision of end-of-life care (and the experience of the death of the individual for whom care was provided) likely would provide a powerful social context through which lives could be shaped, altered, and reimagined. Richardson (2012a) called for research on unpaid care work “as first and foremost” in the movement to encourage vocational psychology to embrace a work and relationship perspective. Several counseling psychologists have answered this call and begun to incorporate unpaid work in vocational theory and research (e.g., Blustein, 2011; Jung & Heppner, 2015; Jung & O’Brien, 2019; Schultheiss, 2009).
Overview of End-of-Life Care
One salient form of unpaid care that is rarely studied is end-of-life care. End-of-life care typically includes personal care (e.g., helping with meal preparation, eating, bathing, toileting, moving, symptom management), emotional/psychological support (e.g., assisting in saying goodbye and processing feelings related to dying or unfinished business), financial assistance (e.g., taking care of finances, being responsible for income), spiritual aid (e.g., supporting spiritual/faith practices, discussing spiritual beliefs about death), practical help (e.g., managing medications, appointments, transportation, grocery shopping, housework) and assistance with difficult decisions (e.g., deciding course of treatment, hospice involvement, palliative care, paid care, how to live the remaining time and how to die; National Institute on Aging, 2019). Women are much more likely than men to provide this type of care (Ornstein et al., 2017).
Factors Contributing to Women’s Overrepresentation in End-of-Life Care
It is interesting to posit what might be contributing to the pervasive gender disparity in the provision of unpaid end-of-life care—especially because research has demonstrated salient negative outcomes associated with this care (Ornstein et al., 2017). Some have suggested that because women live longer than men, they are more likely to provide caregiving at end-of-life. Other reasons stem from a sense of responsibility or because no one else is available to assist the terminally ill individual (Girgis et al., 2013).
It is important to note that gender role socialization likely contributes to the high percentage of women engaged in end-of-life caregiving. Women are expected to take care of and help others, and a key component of being a good daughter, spouse/partner, mother, sister or friend is taking care of those they love (Jung & O’Brien, 2019). Similarly, the belief that women are “natural caregivers” and have the innate skills to care for their loved ones also can contribute to women’s overrepresentation in this role (as men may be perceived as incompetent in the caregiving role). Interestingly, women who are perceived as natural caregivers may be less likely to receive support from others in providing end-of-life care (Washington et al., 2015). Furthermore, gender role socialization includes the expectation that relationships with others should be central for women (Kim et al., 2019). Consequently, when a family member is ill, the women in the family may have a closer relationship with that person and thus be more willing (and expected) to provide care and make sacrifices associated with this care (Kim et al., 2019).
What remains challenging is separating an individual woman’s desire to provide end-of-life care for someone from the societal expectations that may have been internalized regarding serving in this role. A key predictor of outcomes associated with end-of-life care is the degree to which individuals choose to engage in this assistance; understandably those who feel forced to provide care have less positive outcomes (Washington et al., 2015).
Vocational psychology also can enhance our understanding of the conscription of women in end-of-life caregiving roles. Given that women are concentrated in careers that involve caring for others (e.g., nurses, health care aids, teachers), this could translate to expectations that women in these or other care-taking roles provide caregiving for dying family members. Also, women often are employed in careers that underutilize their abilities so they can prioritize family—more women than men work within the home and care for children (Parker & Wang, 2013). Furthermore, women’s involvement in the labor force historically has been undervalued. A significant gender wage gap exists in the United States; women earn 18.4% less than men for comparable full-time work (i.e., 82 cents for every dollar earned by men; Hegewisch & Tesfaselassie, 2019). Family members, when deciding who will provide the care, may see women’s work as less valuable or more amenable to caretaking (either in addition to their job or at the expense of their position). It’s interesting (and discouraging) that some of the ongoing disparities in career choice, employment and income may contribute to women being overrepresented in the end-of-life caretaking role.
Career and Occupational Effects of End-of-Life Caregiving
Very little research exists on the vocational effects of unpaid end-of-life caregiving specifically. However, caregiving for those who are terminally ill has been shown to have considerable negative effects on career and occupational attainment and sustained employment (Fahle & McGarry, 2017). Career effects include reduced ability to work (i.e., needing to decrease work hours, take leave without pay or work from home, limit employment options, or accept low paid work; Girgis et al., 2013; Lahaie et al., 2012; Stajduhar et al., 2010).
Furthermore, women were more likely than men to leave their jobs rather than reduce their work hours (MetLife Mature Market Institute, 2011). Relatedly, more women than men retired early to provide care (Lahaie et al., 2012); one study found that women were five times more likely to retire early to care for spouses who were ill (compared to women who were not caregivers) while men who provided care were less likely to retire than non-caretaking men (Dentinger & Clarkberg, 2002). In addition, these modifications to one’s work might result in women being unable to progress within their career or being passed over for promotion (Girgis et al., 2013; Lahaie et al., 2012; Stajduhar et al., 2010).
Economic Effects of End-of-Life Caregiving
On average, the financial impact of unpaid caregiving is greater for women than men; women lose over $324,000 in wages and Social Security as a result of caring for aging parents (MetLife Mature Market Institute, 2011). Caring for terminally ill loved ones often results in diminished lifetime earnings (Fahle & McGarry, 2017) and/or reduced retirement savings (Girgis et al., 2013; Lahaie et al., 2012). In addition, caregiving can create financial burden through unexpected expenditures or debt due to expenses associated with treatment or care of the loved one (Girgis et al., 2013; Lahaie et al., 2012). Disturbingly, the negative financial effects of caregiving on women elevate the risk of living in poverty later in life (Fahle & McGarry, 2017; Wakabayashi & Donato, 2006). As Jung and O’Brien (2019) noted, unpaid work explains much of the gender gap in employment, salary and quality of position.
Prior to proceeding, it is important to address a pressing question related to the financial costs of unpaid end-of-life care for women. The overall financial costs of caregiving for women would be lower if those who provided caregiving were unemployed, inconsistently employed, or employed in low income positions. If those who are providing end-of-life care are employed (i.e., have “strong market attachments”), skilled and have the potential for good pay, benefits and retirement contributions, the financial costs of caregiving would be considerably higher. To address this question, Fahle and McGarry (2017) analyzed an existing 20-year data set of female caregivers of aging parents and found that caregivers were slightly more educated, more likely to be employed, and had higher earnings and higher levels of work experience than non-caregivers. They concluded that the negative effects on work associated with caregiving extend to after the provision of care. Also, a salient predictor of who provided care was the number of sisters in the family—women who had more sisters were less likely to provide care for aging parents, likely because a sister took on the role of caregiver.
In summary, research has found that women are disproportionally engaged in end-of-life care, partially as a result of gender role socialization and the devaluing of women’s involvement in the labor force. The provision of this care can have negative effects on career development and financial well-being. To enhance our overview of women’s involvement in unpaid end-of-life care, qualitative data were collected and analyzed to provide illustrative examples of the experiences of 12 women who managed caregiving while being employed. Of particular interest were the challenges and rewards associated with managing end-of-life care and work as well as the effects of providing end-of-life care on employment and finances.
Method
Participants
Participants were 12 White, heterosexual, employed women who provided care for someone at the end of their life within the past year (eight were currently providing care, four had provided care previously). They ranged in age from 29 to 58 years old (M = 38.5, SD = 9.03). Most were married or in a committed relationship (n = 8). All participants had completed some college with three having received a bachelor’s degree, four obtaining a master’s degree, and two receiving a doctoral or professional degree. Eleven participants were employed full-time and one worked part-time. All participants were in different occupations including chef, graphic designer, house cleaner, nurse manager, and associate professor. Their total household income varied from $20,000 to $39,999 (n = 4) to more than $100,000 (n = 3).
Most of the women provided care for their mothers (n = 7) or grandmothers (n = 2) with the remaining providing care for a father (n = 1), mother-in-law (n = 1), or father-in-law (n = 1). The average length of time providing care was 15.75 months (SD = 18.27). The caregivers reported very close relationships with the person for whom they provided care (M = 4.75, SD = .87). Most of the people receiving care had cancer (n = 7) while others had heart disease (n = 1), Alzheimer’s (n = 2), or other illnesses (n = 2). The majority chose to be in the role of caregiver (n = 7) and nine of the participants reported being willing to provide end-of-life care again in the future.
With regard to the use of work benefits (see Table 1), virtually all of the caregivers changed their work schedules to provide end-of-life care. Many worked different hours, arriving or leaving earlier or later than before and several reduced the number of hours that they worked. Impressively, most reported receiving support from their employer. Other work-related strategies like stopping work temporarily, working from home, changing jobs, or using Family Medical Leave Act were endorsed less frequently. None of the women in our sample retired early.
Means, Standard Deviations, Minimum and Maximum Values on the Likert-Response Items.

Procedure
After receipt of Institutional Review Board approval, participants were recruited through emails to personal contacts and community agencies for the bereaved, as well as online through blogs, message boards, listservs, and social networking sites. Our email advertisement/flyer asked, “Are you an employed woman who is providing (or has provided) unpaid care for someone who is at the end of their life (not a professional or paid caretaker) within the past year? Are you currently employed or were you employed at the time that you began to provide care for someone who was at the end of their life? We want to hear your voices.” A link to an online Qualtrics survey was included in the invitation to share their experiences.
After responding to questions assessing inclusion criteria (i.e., female, provide or provided unpaid care for someone at the end of their life within the past year, currently employed or employed at the time of giving end-of-life care), those who met the criteria were provided with an informed consent form. After indicating consent, participants received a survey consisting of four open-ended questions and several Likert scale items related to their experience of managing work and unpaid caregiving, as well as a demographics form. An optional open-ended question asked if there was anything more that they would like to share with the researchers.
As a small incentive, participants received a $20 Amazon.com gift card upon completion of the survey. No identifying information was collected on the main survey; those interested in receiving the gift card clicked on a link that took them to another survey where they provided their name and contact information.
Measures
Caregiving experiences
Participants were asked to respond to the following four open-ended questions: What are/were the challenging aspects of managing work and caregiving for someone at the end of their lives?; What are/were the rewarding aspects of managing work and caregiving for someone at the end of their lives?; How has/did providing care affected your employment/career/ professional or educational plans?; and How has/did providing care affected your finances/savings/retirement or retirement planning? These questions were developed by our research team (comprised of one professor, three graduate students, one post-baccalaureate researcher, and three undergraduate students) to obtain illustrative data from women who managed work and unpaid caregiving.
In addition, several items created by the research team asked participants to rate on a Likert scale the degree to which they used certain benefits while they were working and providing care. Specifically, items assessed the degree to which participants changed their schedule, worked different hours, received support from their employer, reduced their work hours, requested more vacation time, put less effort into their work, stopped work temporality, worked from home more often, changed jobs to have more flexibility, used benefits associated with the Family Medical Leave Act, and retired early.
Demographics
Participants indicated their age, gender, race/ethnicity, sexual orientation, relationship status, educational level, socio-economic status, employment status, occupation, relationship to the person for whom they are providing care and their illness, length of time providing care, and the degree to which the participants chose the caregiving role and would be open to providing caregiving again in the future.
Data Analyses
Directed content analysis was used to identify common themes in responses to the open-ended questions (Roberts, 2001). In this structured form of content analysis, existing research was used to inform initial coding themes or categories for the data (Hsieh & Shannon, 2005). First, guided by prior research and the literature, possible themes were generated by the research team. Next, teams of two reviewed responses to each question and created additional themes. There were a total of 87 possible themes (21 challenges, 13 rewards, 23 effects on employment/career/professional or educational plans, and 30 effects on finances/savings/retirement or retirement planning).
Two members independently coded the responses for each of the questions into themes. In cases where there was disagreement about the themes, the team members met to discuss the discrepancies and achieve consensus. After the coding process was completed, the professor reviewed the coding of every response. On a small number of responses, coders were asked to reconsider their coding decisions. The initial teams then met and decided on the final coding of the responses. Themes that were endorsed by at least 25% (n = 3) of the participants are reported in Table 2 as those with fewer responses did not represent the experiences of at least a quarter of the women who responded to our questionnaire. The entire coding spreadsheet (with a list of all themes and the data in each theme) is available from the first author.
Themes, Subthemes and Percentages of Endorsement.
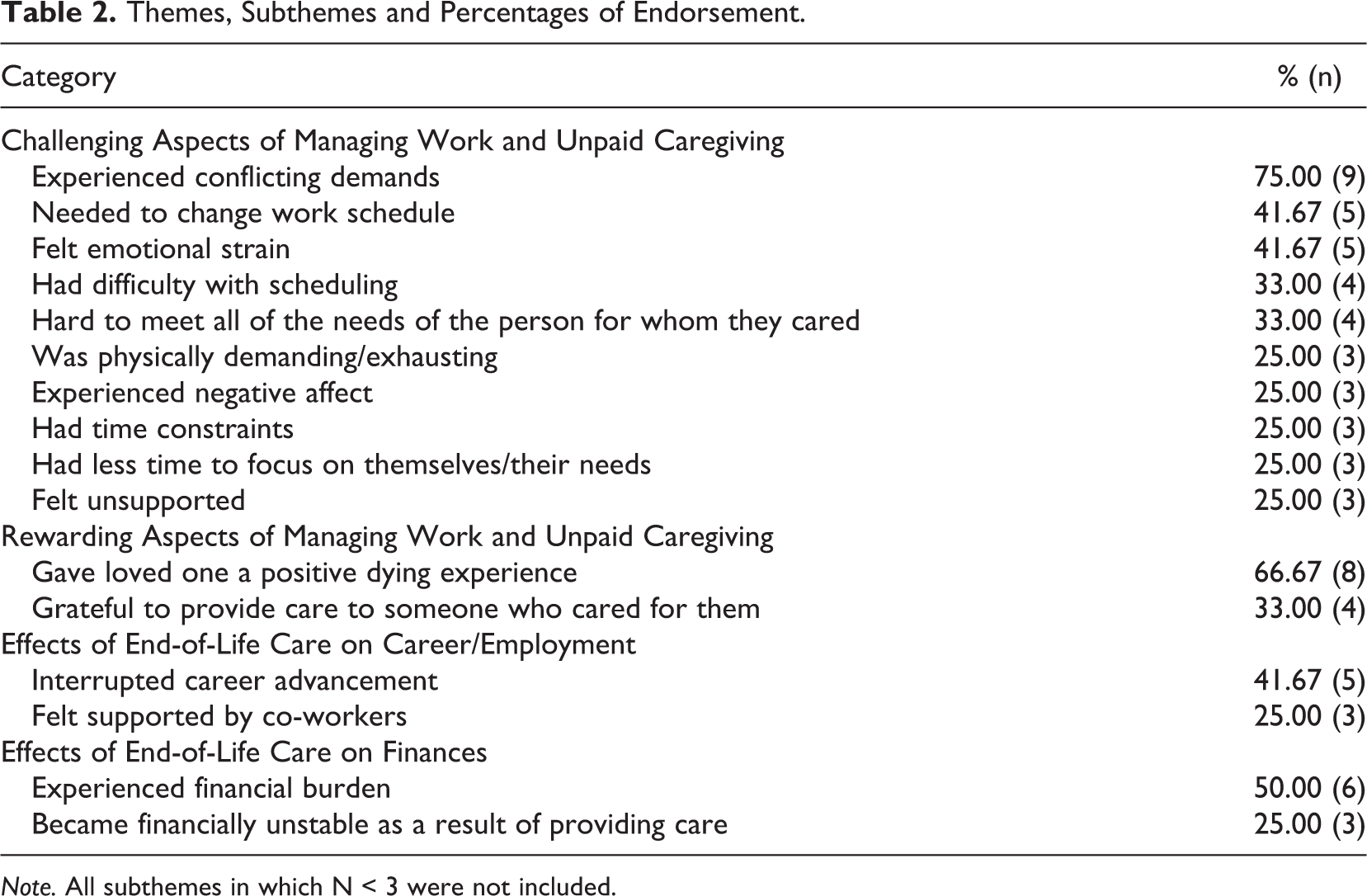
Note. All subthemes in which N < 3 were not included.
Results
Challenging Aspects of Managing Work and Caregiving Themes
Ten themes emerged related to challenging aspects of managing work and caregiving. Almost all of the participants (n = 9) experienced conflicting demands between caregiving and work. For example, one participant wrote: “Managing the many helpers/social workers, nurses, etc and unexpected disruptions as well as work life—along with my own family. The many hours spent on the phone looking at options for assistance, or having a stair lift company in the house for hours—takes away from the work I was supposed to be doing.” Another commented, “Ultimately, it is most challenging balancing everything—Family, work and care for my dad as well as attempting to make sure my mom does not over do as well. Changing your daily life to coordinate is a huge challenge.”
Several participants (n = 5) mentioned that they needed to change their work schedule, with participants noting, “I needed to be able to drop everything to go to her, leave early, go to work late” or “I try to trade days where possible so that I am not missing work as I have been out of PTO [paid time off] for quite some time and don’t get paid when I miss.”
Others reported that they had difficulty with scheduling (n = 4) “While she was in a care facility, daily visits, advocating for her, doctor appointments, and emergency room visits were all time we had to find to ensure her safety and health.” Relatedly, the caregivers indicated that they had time constraints (n = 3), i.e. “Time management was such a struggle.” Also, some of the women noted that they had less time to focus on themselves and their needs (n = 3); “Keeping up with self care—it was so easy to push exercise and meditation to the next day when my mom needed immediate help.”
Several participants (n = 5) also felt emotional strain as they managed work and caregiving: “There are many challenging aspects—I don’t think people take into consideration the mental toll it takes…The entire time I am at work I am scared, nervous and anxiety ridden because I am worrying how my mother is and I feel selfish for working because ultimately I should be at home but financially I have to. The mental anguish is the biggest challenge at least for myself.” Similarly, some caregivers indicated that they experienced negative affect (n = 3). For example, one participant wrote, “I would get emotional and aggressive in situations that shouldn’t have led to a reaction.”
Other emotions were shared as some of the caregivers felt unsupported (n = 3). Example responses included, “My husband and I did all the work and when it was all over, my FIL [father-in-law] and sister-in-law swooped in and acted like it wasn’t that big of a deal” and “I also found it very challenging to do this with no support from siblings and very little support from extended family members.”
For some of the caregivers, it was hard to meet all of the needs of the person for whom they were caring (n = 4), “…ensuring she gets all she needs” and “being available immediately when there are problems or when her doctors are visiting.” Understandably, the experience of caregiving was described as physically demanding/exhausting (n = 3): “I have never been spread so thin in my life. To care for a MIL [mother-in-law] while pregnant, then through six months postpartum is something I’m still recovering from.”
Rewarding Aspects of Managing Work and Caregiving Themes
When asked about the rewarding aspects of managing work and caregiving, two themes were found. First, numerous participants (n = 8) highlighted the meaningfulness of having gave their loved one a positive experience of dying, e.g. “Most rewarding was keeping a promise to my grandmother to keep her in her home as she wanted not with strangers and she was never alone. Family was with her every day.” Second, several participants (n = 3) indicated that they felt grateful to provide care for someone who cared for them, e.g. “And, I am so grateful for the opportunity to be able to return to her just the slightest amount of care that she afforded me throughout my life.”
Effects of End-of-Life Care on Career/Employment Themes
Two themes also emerged when participants reflected on how their career plans were affected by the provision of end-of-life care. First, several participants (n = 5) indicated that their career advancement was interrupted. For example, one participant wrote, “My grandmother was vegetative from Alzheimer’s and dementia and I took care of her for several years. While taking care of her I didn’t seek to advance my career or look for other opportunities.” The second theme was related to participants having felt supported by coworkers (n = 3). One participant wrote, “Luckily I felt my colleagues supported me being out of the office.”
Effects of End-of-Life Care on Finances
Finally, participants also noted that providing end-of-life care had an effect on their finances (two themes). About half of the women experienced financial burden (n = 6). One wrote, “Caring for a family member is expensive. In between medical supplies and taking unexpected time off.” Others reported that they became financially unstable as a result of providing care (n = 3), e.g. “It’s put a lot of the financial strain on him, I basically cover my student loans and food. But I plan to get my license soon because we cannot sustain the way we are heading.”
Discussion
In addition to providing an overview of unpaid end-of-life care, this paper highlighted the challenges and rewards experienced by 12 women who managed work and end-of-life care. Consistent with the recommendations of vocational psychologists (e.g., Blustein, 2006, 2011; Jung & O’Brien, 2019; Richardson, 2012a, 2012b; Schultheiss, 2009), unpaid end-of-life care should be considered work, relationships and relational experiences must be embedded in vocational theory, and changes are needed at the individual, family, workplace, and societal level to ensure that women are not unduly burdened by the provision of end-of-life care. Vocational psychologists have unique skills and expertise to address the challenges experienced by working women caregivers and thereby contribute to the advancement of education, research, clinical interventions, and public policy related to women’s involvement in unpaid end-of-life care.
Consistent with the literature, many caregivers experienced challenges in managing conflicting demands among work, home and caregiving. For example, it was difficult to schedule and find time for everything that needed to be done and it was virtually impossible to focus on the caregiver’s own needs. Furthermore, the physical and emotional strain and toll associated with caregiving was apparent, as the caregivers struggled with negative affect, feeling alone and unsupported by others, and had difficulty meeting all of the needs of the person for whom they cared. In addition, work schedules had to be altered and career trajectories were interrupted. The caregivers also experienced considerable financial burden and some reported becoming less financially stable due to the many expenses associated with caring for someone who was dying.
These findings were consistent with prior research as end-of-life care had negative ramifications for women’s vocational development with regard to ability to work traditional hours, career advancement, and emotional strain. Moreover, it is likely that the overrepresentation of women in this role (i.e., another form of unpaid work) explains some of the national gender gap in employment, salary and quality of position (Jung & O’Brien, 2019). This can happen in direct (i.e., not being able to apply for promotions) and indirect (i.e., being emotionally exhausted and unable to excel at work) ways. As long as society expects women to be largely responsible for end-of-life (and other forms of unpaid) care, inequities in the workplace will continue.
Despite the challenges inherent in managing work and end-of-life care, many caregivers reported positive aspects associated with assisting those who were dying including feeling positively about their ability to provide a caring environment for a loved one at the time of their death and being grateful for the opportunity to provide care for someone who had cared for them. This was consistent with prior research that identified experiencing personal growth, finding meaning and purpose, and enhancing the quality of end-of-life care as positive aspects of providing end-of-life care (Marino et al., 2017; Morgan et al., 2016). It is likely that for some people, accompanying someone who is dying could be a powerful way of being in relationship with another that could have a lasting impact on one’s self and identity. The experience of end-of-life caregiving may reflect what vocational psychologists call a transition in one's life trajectory that may be salient with regard to identity development (Elder & Shanahan, 2006; Richardson, 2012b). Moreover, the positive outcomes associated with caregiving were consistent with Blustein’s (2011) proposition that individuals may find meaning in their relationships and work experiences.
Notably, several themes found in prior studies were not replicated, e.g. developing new skills and strengthening relationships with the person who died (Schulz & Sherwood, 2008), and having better physical and cognitive functioning than non-caregivers (Trivedi et al., 2014). Furthermore, our finding that the caregivers received support from their employers and co-workers was not identified in prior research on end-of-life caregiving as some studies have described unsupportive work environments (Lahaie et al., 2012).
Interestingly, few work-related benefits were used, including those associated with the Family Medical Leave Act (FMLA). It is possible that the women in our sample were employed in organizations that did not have access to this benefit or that they might have had difficulty taking time off with no pay. Many caregivers in this sample and in prior research struggled with expenses associated with end-of-life care (McDermott et al., 2018)—not having an income may be untenable. The limitations to FMLA reflect societal undervaluing of end-of-life care as this benefit often fails to address the needs of employed women caregivers (e.g., 12 weeks may not be long enough for end-of-life care, strict guidelines exist regarding who can provide and receive the care, and the leave is unpaid; Ornstein et al., 2017).
Limitations
It is important to note that our paper and much of the published research did not examine race/ethnicity, socioeconomic status, sexual orientation, gender identity, relationship status, family composition, spiritual/religious/faith affiliation, immigration status, age, and other identity statuses of the women caregivers. The sample used to generate illustrative comments for this contribution was small and homogenous (i.e., comprised predominantly of heterosexual, educated, employed, resourced, White women), thus the findings cannot be generalized to others. It is likely that these identities and certainly the intersection of gender with other identity statuses plays a profound role in the experiences of caregivers at end-of-life.
For example, ethnic minority caregivers might experience racism as they try to advocate for their loved one – an experience that could add stress to their caregiving. One study found that Black and Hispanic workers were not able to take time off from work to take care of their family (26% and 23%, respectively; Horowitz et al., 2017). In addition, racial and ethnic minority individuals are less likely to be involved in end-of-life planning and more likely to die in hospitals as opposed to at home (Orlovic et al., 2019). Furthermore, ethnic minority individuals with low incomes reported using hospice care services less (Hughes & Vernon, 2019), which might result in additional physical, psychological, and financial burdens to the caregivers (Born et al., 2004).
Similarly, caregivers with few economic resources may encounter additional stressors related to affording needed medications, supplies or paid care. For example, the majority (93%) of low-wage workers have no access to paid family leave (Gupta et al., 2018). In addition, same-sex couples may face obstacles to receiving employer-sponsored unpaid medical leave benefits if they are not married. Single caregivers could struggle to provide care and work without the assistance of a partner/spouse. Also, caregivers whose primary language was not English could experience challenges in obtaining needed services of communicating with hospice or medical personnel (Giesbrecht et al., 2012). Those whose cultural mores differ from the majority culture could face challenges as they try to communicate about their cultural traditions regarding death and dying.
Recommendations for Clinical Practice and Education for Women Caregivers
Providing interventions for end-of-life caregivers could validate their experiences, promote psychological adjustment, and alleviate their burdens (Rabow et al., 2004). These interventions may be particularly salient for women as they adapt and respond to circumstances where they are asked/needed/required to care for someone who is dying (i.e., engaging in the co-construction of their lives; Richardson, 2012b). Examples of interventions include education, resource referrals, respite assistance, counseling, bereavement support, and career counseling. For example, psychologists and counselors might educate caregivers about the challenges of unpaid end-of-life caregiving (e.g., time demands, financial costs, emotional strain), provide information about managing work and care, and connect caregivers with local resources. In addition, some of the benefits that may be associated with end-of-life care could be discussed with caregivers. Also, counselors could assist caregivers in understanding how the provision of care could influence their identity development, work goals and construction of their lives. Telecounseling (e.g., Kwok et al., 2014) could reach those who are unable to leave their homes due to caregiving or geographical isolation. Providing multicomponent interventions in group settings also could be beneficial; a meta-analysis found that a combination of several interventions including education, support, psychotherapy, and respite lessened caregivers’ burden and improved well-being (Sörensen et al., 2002).
Moreover, connecting caregivers to community resources and other professionals could increase access to and use of helpful interventions. For example, referrals could be made to hospice organizations that offer respite services or caregiver support groups. In addition, working closely with other professionals who interact with caregivers, such as doctors, nurses, and social workers, could reduce barriers to the use of mental health services and physical health care (Hrovat et al., 2012). Caregivers might benefit from risk screening (pre-loss and post-loss). Finally, after the death of the person for whom they provided care, bereavement support could be helpful and career counseling could assist the caregiver in identifying future career/job possibilities and directions.
Recommendations for Workplace Changes related to Women Caregivers
Workplaces play a central role in reducing unfair and lasting burdens on women caregivers. Although the women in our small sample reported support from their employers and co-workers, many employed caregivers experience unsupportive workplace policies or cultures that further exacerbate their burden (Lahaie et al., 2012). Ideally, employers would provide flextime and telework, and allow short term leaves for employees. When possible, employees should be allowed to participate in meetings online instead of having to attend in person. Furthermore, many work places allocate specific paid time off for sick days, personal days, and vacation days. However, caregivers may benefit from having a shared paid time off policy, where they can pool their paid leave. Ensuring that their position and potential promotion were protected would enable employees to take limited time away from their job without concern that they would be jeopardizing their future career.
Recommendations for Research Related to Women Caregivers
Furthermore, there is clear need for further research on unpaid end-of-life caregivers. Specifically, investigating how intersecting identities (e.g., race/ethnicity, socioeconomic status, sexual orientation, and/or first-generation immigrant caregivers) affect the experiences of women caregivers would advance knowledge and inform interventions. Longitudinal studies are needed with diverse groups of caregivers to assess caregivers’ needs and the best strategies to support them as the illness progresses over time and after the death of the person for whom they provided care. It would be interesting to study the ways in which family members from diverse cultures make decisions about who provides end-of-life care. Interventions to reduce gender, racial/ethnic and economic disparities in end-of-life care could be created, implemented, and empirically evaluated.
In addition, large scale studies should examine the impact of unpaid end-of-life caregiving on the career development, personal and work relationships, financial earnings, and retirement savings of women. Studying how the social and relational context of end-of-life caregiving may play a role in women’s construction of their lives would contribute to our understanding of Richardson’s (2012a, 2012b) counseling for work and relationship perspective. Moreover, psychometrically sound measures should be developed to assess constructs of interest for this line of research. For example, an inventory identifying the salient challenges and rewards associated with end-of-life caregiving would be a contribution to the literature and to future research. Studying differences between those who wanted to provide care versus reluctant caregivers could contribute to our understanding of caregiving.
Recommendations for Societal Changes Related to Women Caregivers
At the individual level, ideally women would have options and be able to freely choose if they want to provide end-of-life care. At the familial level, responsibility for end-of-life care should be shared and this work should not be assigned based on gender. Gender role expectations should be changed so women are not expected to provide care but rather can make the choice to care for loved ones independent of societal expectations.
It is important to note that current gender role expectations are harmful to men as they may be perceived as incompetent to provide care. For some people under certain conditions and with resources (financial and other), providing end-of-life care to a loved one can be a positive and powerful life-changing experience. Some men may opt out or not be considered for these roles due to restrictive gender role expectations.
At a societal level, ensuring equal pay between women and men, paying caregivers for their work, and expanding the Family Medical Leave Act to address diverse caregiver situations (e.g., for individuals who have caregiving responsibilities for their adult children, domestic partners, as well as other non-kin individuals) and be less restrictive is needed. Unpaid care work should be valued as critical to the functioning of our society (Richardson, 2012a).
Finally, caregivers should be paid for the care that they provide to their loved ones or receive financial assistance to pay non-family members to provide end-of-life care. This would ensure that women could choose to provide the care or pay others, and thus not experience the deleterious effects of caregiving on their career and economic status.
To conclude, women who provide unpaid end-of-life care while employed experience both negative and positive outcomes related to career, relationships, health, and finances. Together, vocational psychologists can advocate for changes at the individual, familial, workplace and societal levels to ensure that women who provide end-of-life care are not unfairly burdened at this critical moment in the construction of their lives.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.