
Abstract
This study extended research on Psychology of Working Theory (PWT) by examining the connection of decent work to work fulfillment and general well-being in 346 predominantly U.S. adult workers diagnosed with Chiari malformation (CM), a chronic health condition involving a structural malformation affecting the posterior region and base of the skull, and commonly presenting with chronic head and neck pain and related physical (e.g., fatigue) and psychological (e.g., anxiety, depression) complications. Participants completed an online survey containing measures of PWT’s outcomes of decent work constructs as well as the domain-specific marginalization constructs of condition severity and workplace limitations. Results of structural equation modeling analyses supported 12 of 19 hypotheses. Decent work directly and positively predicted survival, social contribution, and self-determination needs; social contribution and self-determination needs directly and positively predicted work fulfillment; survival and self-determination needs directly and positively predicted general well-being; decent work indirectly (via social contribution and self-determination needs) and positively predicted work fulfillment and indirectly (via survival and self-determination needs) and positively predicted general well-being; and condition severity directly and negatively predicted general well-being. Consistent with PWT, attaining decent work contributes to meeting needs for survival, social contribution, and self-determination, which in turn contributes to greater work fulfillment and general well-being in workers with CM.
Introduction
An estimated 60% of U.S. adults has one or more chronic health conditions, or conditions that persist for one year or longer, limit daily activities, and/or frequently require ongoing medical attention (Centers for Disease Control and Prevention, 2019). Previous estimates suggest that 68% of U.S. workers experience one or more chronic physical (e.g., high blood pressure, diabetes), mental health (i.e., depression), or pain conditions (Witters & Agrawal, 2011). As the U.S. workforce continues to age and chronic disease management evolves, this percentage likely will increase (Koch et al., 2013; McGonagle & Barnes-Farrell, 2014) as will our need to better understand chronic health barriers to productive work and the factors improving vocational productivity and satisfaction. In the present study, we consider variables influencing work-related behaviors among individuals diagnosed with Chiari malformation, a typically congenital condition yielding acute and chronic health effects. Utilizing the framework provided by the Psychology of Working Theory (PWT; Duffy et al., 2016), we attempt to broaden our understanding of worker outcomes among those with health conditions associated with this singular diagnosis, but with the potential for diverse impacts to work performance.
In general, workers with chronic health conditions and chronic pain often face a number of unique challenges at work, including managing symptoms of their condition(s), reduced work ability, extended absenteeism and presenteeism (i.e., working while ill or injured), and fear of discrimination from coworkers and supervisors (Beatty & Joffe, 2006; McGonagle et al., 2014, 2016, 2016; Munir et al., 2007). These unique challenges, in turn, can adversely affect workers’ experience of important work outcomes such as job satisfaction, job performance, and coworker relationships (Issa et al., 2012; McGonagle et al., 2016; Siu et al., 2013; Varekamp & van Dijk, 2010). In addition to their adverse effects on people’s work lives, chronic health conditions increase the risk of experiencing psychological distress (e.g., depression) and lower the likelihood of experiencing subjective well-being (Bishop et al., 2015; Helgeson & Zajdel, 2017; Jensen & Turk, 2014).
Given the significant impact of chronic health conditions on people’s workplace experiences and general well-being, it is important to identify factors that may affect the attainment of desirable work outcomes (e.g., job satisfaction) and general well-being in individuals with these conditions. Studies have revealed a number of such factors, including condition severity and functional limitations (i.e., impaired ability to perform meaningful daily activities) resulting from the chronic health condition(s) (Bishop et al., 2015; Helgeson & Zajdel, 2017; Siu et al., 2013). For example, workers with chronic health conditions who experienced more severe symptoms and/or greater work-related limitations (e.g., difficulty concentrating on work) reported significantly lower levels of job satisfaction (Bishop et al., 2015; Roessler & Rumrill, 1998; Siu et al., 2013). In a similar vein, individuals with chronic health conditions reported higher levels of well-being (e.g., life satisfaction, lower psychological distress) when they experienced less symptom severity (or fewer symptoms) (Huber et al., 2008; Ryan et al., 2007; Yaghmaian & Smedema, 2019) and fewer functional limitations (Huber et al., 2008; Munir et al., 2007; Yaghmaian & Smedema, 2019).
The current study sought to extend current understanding of the factors affecting the experience of work fulfillment (i.e., meaningful and satisfying work) and general well-being in workers experiencing one or more chronic health conditions associated with a diagnosis of Chiari malformation (CM) – an often congenital condition impacting brainstem anatomy, characterized by various sensory (e.g., pain, dizziness), movement, and psychological (e.g., depression, anxiety, executive function) symptoms (Fischbein et al., 2015; Meeker et al., 2015). In the sections that follow, we present the theoretical framework in which we ground our research (i.e., Psychology of Working Theory [PWT; Duffy et al., 2016]) and summarize relevant PWT-based research evidence. Subsequently, we describe the physical features, symptoms, and work-related impact of those with CM, thus providing a rationale for testing a model of factors promoting general well-being and fulfilling work in this sample of workers with CM and chronic health conditions.
Psychology of Working Theory
Although scholars have begun to identify factors affecting the work outcomes (e.g., job satisfaction) and general well-being of individuals with chronic health conditions, the extant literature is somewhat fragmented because it is not grounded in a clearly articulated and empirically supported theoretical framework. One particularly promising theory for understanding the work lives and general well-being of individuals with chronic health conditions (including CM) is the recently published Psychology of Working Theory (PWT; Duffy et al., 2016). Compared to other influential career development theories (e.g., Holland’s [1997] theory, Social Cognitive Career Theory [Lent et al., 1994]), PWT shines greater light on the notion that career choice and adjustment are volitional activities. Rather, PWT recognizes that contextual barriers—notably, economic constraints and experiences of marginalization—figure prominently in individuals’ attempt to secure decent work (i.e., work that provides a safe work environment, adequate compensation, access to health care, allowance for adequate rest and free time, and values that align with one’s personal and social values).
More specifically, PWT posits that individuals who have greater access to economic resources and fewer experiences of marginalization will be more likely to perceive career decision-making capability (i.e., work volition) and coping resources for career-related challenges (i.e., career adaptability), thus facilitating their likelihood of attaining decent work. PWT further posits that individuals who can secure decent work will be more likely to experience work fulfillment (i.e., satisfying and meaningful work) and overall well-being via the satisfaction of basic survival (e.g., providing for one’s family), social contribution (i.e., benefiting others through work), and self-determination (i.e., feeling autonomous, competent, and socially connected at work) needs. (See Figure 1 for a depiction of the outcomes portion of PWT, which is the focus of the current study.) Hypothesized structural model.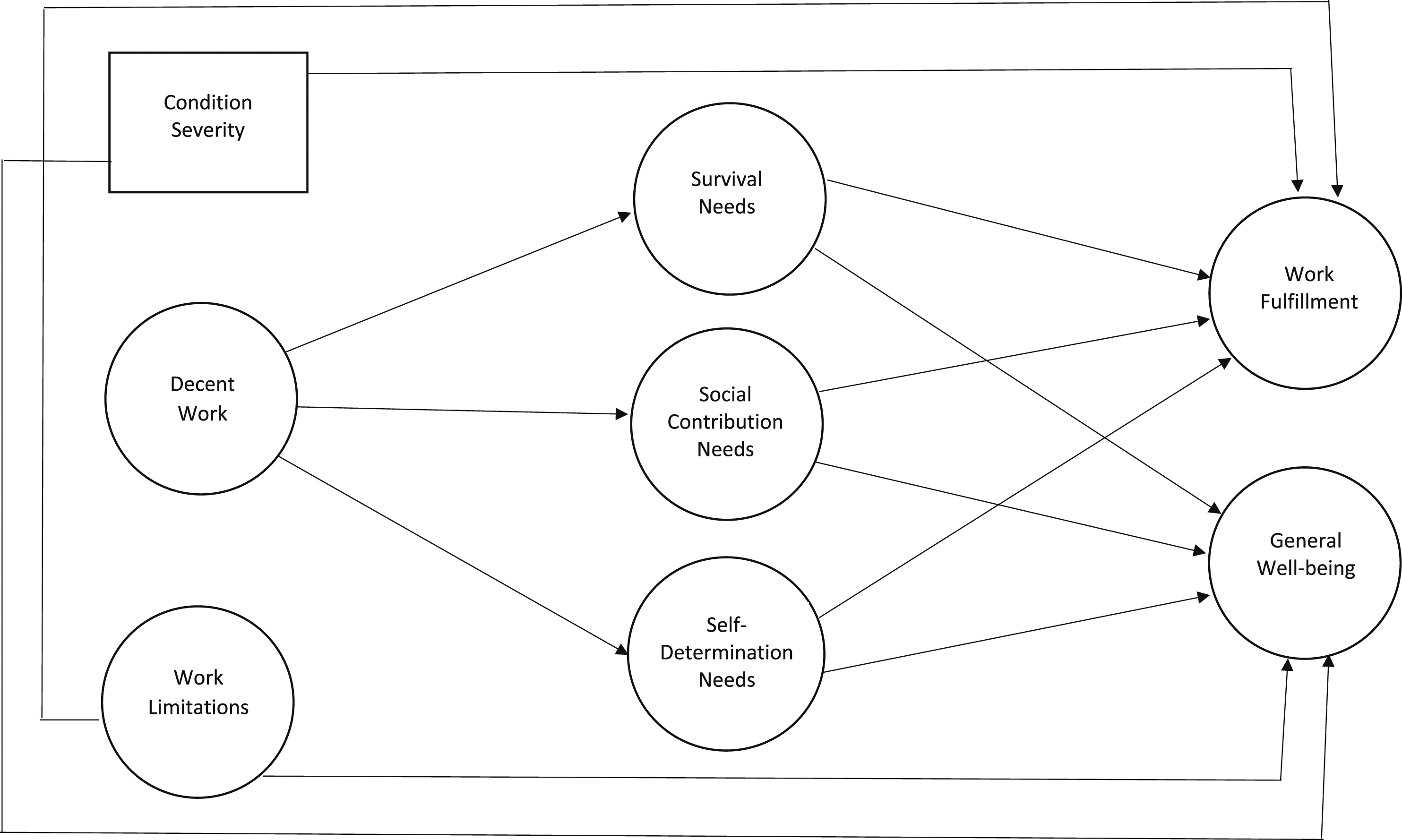
Since its recent publication, PWT has received considerable empirical support, most of which has focused on the posited predictors of decent work. Indeed, a recent review by Duffy et al. (2023) found that almost 100 empirical studies have been published to date using the theory. The majority of these studies focused on variables predicting decent work across a wide array of populations, mainly with working adults with some type of marginalized status (e.g., Autin, Herdt, et al., 2022; Autin, Williams, et al., 2022; England et al., 2020; Williams et al., 2023). These studies generally demonstrated that experiences of economic constraints and marginalization negatively predicted decent work attainment, and that these relations were often mediated by work volition. Specifically, a partial reason why these structural factors impeded the attainment of decent work was because of limiting choice in one’s career decision making. Most relevant to the current study, Tokar and Kaut (2018) demonstrated support for PWT’s posited predictors of decent work in a sample of 320 workers diagnosed with CM and other chronic health conditions. They found significant negative associations of economic constraints and ableist marginalization with decent work and work volition, a significant negative relation between economic constraints and career adaptability, and a significant positive relation between career adaptability and decent work.
A smaller, but still substantial group of studies have focused on outcomes of attaining decent work. Recent studies also have demonstrated support for PWT’s posited outcomes of decent work. Studies have consistently demonstrated across a variety of samples that decent work attainment is linked to meeting the three work-related needs proposed within PWT (survival, social contribution, and self-determination; Duffy et al., 2019, 2021; Kim et al., 2021; Seol et al., 2023). Other studies have focused on the links between decent work and more distal work outcomes, such as job satisfaction, meaningful work, turnover intentions, and mental and physical health. These studies have also shown strong links between experiencing one’s work as decent and being satisfied and stable in one’s job; it appears that decent work also links to stronger levels of general and physical mental health (Allan, Tebbe, et al., 2019; Duffy et al., 2021; Huang et al., 2022; Kim & Kim, 2022; Wan & Duffy, 2022).
The two most pertinent studies in relation to the present study are those by Duffy et al. (2019) and Seol et al. (2023). Duffy et al. (2019) tested the direct and indirect (via survival, social contribution, and self-determination need satisfaction) effects of securing decent work on physical and mental health in a sample of adult workers earning less than $50,000 annually. Consistent with PWT, Duffy et al. (2019) found that decent work directly and positively predicted satisfaction of survival needs, social contribution needs, self-determination needs, and physical health; satisfaction of all three needs directly and positively predicted mental health; and survival need satisfaction directly and positively predicted physical health. Furthermore, satisfaction of all three needs fully mediated the relation between decent work and mental health, whereas survival need satisfaction partially mediated the relation between decent work and physical health. Seol et al. (2023) tested a similar model, examining how decent work predicts PTSD and post traumatic growth as mediated by the three PWT need satisfaction constructs with a sample of midshipmen in the Republic of Korea Naval Academy. Using a time lagged design, they also found decent work to predict each need and for survival needs to significantly mediate the relation to PTSD and social contribution/self-determination needs to significantly mediate the relation to post traumatic growth.
Collectively, the extant empirical evidence strongly supports PWT for understanding predictors and outcomes of securing decent work in diverse samples of working adults. Namely, evidence across dozens of studies suggests that structural experiences of economic constraints and marginalization often limit decent work attainment due to limitations on work choice. For those who do attain decent work, they are likely to view their jobs as satisfying and meaningful and experience higher levels of mental and physical health, in part due to that work meeting needs for survival, social contribution, and self-determination. In the current study, we sought to extend the budding literature on the applicability of the outcomes (of decent work) portion of PWT by testing it in a sample of workers with one (i.e., Chiari malformation) or more chronic health conditions.
Chiari Malformation
In the current study, we tested the applicability of PWT’s outcomes of decent work in a sample of workers diagnosed with Chiari malformation (CM), a condition involving a structural malformation affecting the posterior region and base of the skull. Technically, CM is diagnosed upon radiological evaluation (e.g., magnetic resonance imaging) revealing portions of the cerebellum (i.e., cerebellar tonsils) descending abnormally into the transitional region between the medulla of the lower brainstem and upper segments of the spinal cord – a condition referred to as tonsillar ectopia (Heffez et al., 2020). Anatomically, the structural malformation to the posterior region of the skull typically reduces the available space occupied by the cerebellum (i.e., posterior cranial fossa), thereby exerting pressure on the cerebellar tonsils forcing them into the opening at the base of the skull (i.e., foramen magnum).
This malformation is most often congenital in nature, but to a much lesser extent can also be acquired following trauma (Speer et al., 2003). Prevalence estimates have varied in the literature, ranging from 1/18,000 to 1/1,000 (see Meeker et al., 2015; Sadler et al., 2020; Speer et al., 2003) and even as high as 1/100 (Sadler et al., 2020). Although the exact prevalence is unknown, it is estimated that approximately 200,000 Americans have a CM diagnosis (Fischbein et al., 2015). Certainly, advances in neuroimaging have facilitated the identification of individuals with CM, although it is recognized that many individuals can remain asymptomatic until adulthood (Leu, 2015; see also Morris et al., 2009). The condition appears to be of greater incidence among women, with women being represented to a noticeably higher degree in recent studies of CM patients (i.e., 72–93% women; Garcia et al., 2019; Killeen et al., 2015; Meeker et al., 2015).
Functionally, the resulting impact on brainstem and spinal cord anatomy can yield a number of symptoms (Haddad et al., 2018; Heffez et al., 2020; Landbridge et al., 2017; Shaffer et al., 2011; see also Pettorini et al., 2010) most commonly including chronic pain, headache (i.e., upon coughing, or migraine), fatigue, and sensory-motor disturbances typically affecting regions of the head, neck, and extremities (Haddad et al., 2018; paresthesia – tingling sensations; see Landbridge et al., 2017). As expected, cerebellar symptoms can be observed as well, which might include progressive ataxia (i.e., impaired balance or coordination) and unsteady gait (Leu, 2015). Apart from sensory and motor implications, increased levels of anxiety and depression have also been observed in CM (Fischbein et al., 2015; Garcia et al., 2019), as well as cognitive and executive function issues (Garcia et al., 2018; Houston et al., 2019; Rogers et al., 2018; Yilmaz et al., 2022).
Given the structural impact of CM and the potential for widespread physical, affective, and cognitive symptoms, it stands to reason that individuals with this diagnosis might experience varying degrees of functional decrements encroaching on work-related skills and performance. Indeed, recent studies of CM have revealed the adverse effects of this condition on activities of daily living (Meeker et al., 2015), including common activities of work engagement (e.g., extended sitting or standing, repetitive movements, bending down, concentrating, reading) (Tokar & Kaut, 2020). The majority of workers with CM also experience shifts in their career identity and goals, diminished work ability, and reduced levels of job satisfaction as a result of their condition (Tokar & Kaut, 2020). Furthermore, because they frequently encounter ableist marginalization, economic constraints, and other contextual barriers, workers with CM may be less likely than others to secure decent work (Tokar & Kaut, 2018). Preliminary evidence also suggests that individuals (including workers) with CM are less likely to experience general well-being (i.e., quality of life) than those in the general population (Fischbein et al., 2015; Sixt, et al., 2009). In sum, the available empirical evidence suggests that workers with CM are likely to face myriad challenges and barriers at work, which in turn decrease their likelihood of experiencing decent and fulfilling work and general well-being.
Applying PWT’s Outcomes of Decent Work to Workers with CM
In this study, we examined PWT’s proposed outcomes of decent work (i.e., work fulfillment and general well-being) in workers with CM, the majority of whom had been diagnosed with one or more additional chronic health conditions including connective tissue/joint disorder (i.e., Ehlers-Danlos syndrome), hypothyroidism, and syringomyelia (i.e., cyst formation within the spinal cord). Although PWT does not explicitly recognize all the factors potentially affecting the work fulfillment and general well-being of those with CM and other chronic health conditions (e.g., illness severity, work limitations), it nevertheless may be an ideal framework for capturing their work lives—including outcomes of decent work—for several reasons.
First, although PWT is useful for understanding the work lives of all workers, it was developed “with a particular aspiration to capture constructs salient to those traditionally left out of vocational theories—namely, marginalized populations” (Allan, Tebbe, et al., 2019, p. 409). As noted earlier, workers with chronic health conditions (including CM) face numerous barriers to securing decent work and experiencing work fulfillment and well-being (Beatty & Joffe, 2006; McGonagle et al., 2016; Tokar & Kaut, 2018). Second, preliminary evidence showed strong support for the applicability of the predictors-of-decent-work portion of the PWT to workers diagnosed with CM and other chronic health conditions (Tokar & Kaut, 2018); therefore, it is reasonable to suspect that the outcomes-of-decent-work portion of PWT may be similarly applicable. Finally, the authors of PWT acknowledged that in their effort to balance parsimony with inclusivity, the model might exclude important predictor variables (Duffy et al., 2016). Thus, important predictors other than those specified in the original PWT may contribute to decent work, work fulfillment, and general well-being. As an example, England et al. (2020) expanded PWT’s original model by investigating the potential role of workplace climate in employed women’s attainment of decent work. England et al. (2020) found support for a model that included workplace climate as a positive predictor of both decent work and work volition.
In a manner similar to England et al. (2020), we sought to expand the outcomes portion of the PWT model by including the additional variables of condition severity and work limitations as potential predictors of work fulfillment and general well-being. We chose to include these variables in our model because previous research has related them to indicators of work fulfillment (e.g., job satisfaction) and general well-being in individuals with chronic health conditions. Indeed, these constructs tap well into the proposition within PWT that experiences of marginalization serve to predict downstream experiences in the workplace. In the original PWT model, marginalization experiences were intended to be measured as those occurring across the lifespan, whereas in the current study we focus on specific experiences of marginalization within the workplace that may be prevalent with our sample. This approach – which does deviate from the original PWT model – was recommended as an appropriate extension in the recent Duffy et al. (2023) review article. Namely, they encouraged authors to extend the model in theory consistent ways to better study specific populations. By adding in these domain specific marginalization constructs, we are better able to capture the wide array of workplace experiences that contribute to work fulfillment and well-being.
Factors Fostering Work Fulfillment and General Well Being
Consistent with PWT (Duffy et al., 2016) and more recent work by Allan and colleagues (Allan, Owens, et al., 2019), we conceptualized fulfilling work as “a holistic and complete sense of well-being and flourishing in the work context” (Allan, Owens, et al., 2019, p. 269) that incorporates job satisfaction, meaningful work, and work engagement. (Note that Allan, Owens, et al., 2019, also included workplace positive emotions in their conceptualization). Empirical studies have demonstrated significant associations of individual (e.g., personality traits, abilities), organizational (e.g., workplace relationships), and societal (e.g., access to decent work) factors with job satisfaction (Dodd et al., 2019; Gonzalez-Mulé et al., 2017; Judge & Bono, 2001; Mérida-López et el., 2019), meaningful work (see Lysova et al., 2019), and work engagement (Caesens et al., 2014; Langelaan, et al., 2006; McIlveen et al., 2020) in samples of workers of unknown health status. Concerning workers with chronic health conditions specifically, previous research has suggested that condition severity and self-perceived work limitations (conceptualized herein as individual-level factors) relate negatively to job satisfaction, a key component of work fulfillment (Bishop et al., 2015; Roessler & Rumrill, 1998; Siu et al., 2013). Given their demonstrated relevance to at least one major component of work fulfillment (i.e., job satisfaction) in workers with chronic health conditions, we included condition severity and work limitations as predictors of work fulfillment in our hypothesized model (see Figure 1).
Also consistent with PWT (Duffy et al., 2016), we conceptualized general mental well-being as the experience of happiness or life satisfaction. Past research on individuals with chronic health conditions has demonstrated that less symptom severity and fewer functional limitations are associated with higher levels of general well-being (Huber et al., 2008; Ryan et al., 2007; Yaghmaian & Smedema, 2019). Therefore, we included condition severity and work limitations as predictors of general well-being in our hypothesized model (see Figure 1).
Purpose and Hypotheses
The purpose of this study is to extend research on PWT by testing the proposition that the attainment of decent work positively predicts work fulfillment and general well-being through the satisfaction of survival, social contribution, and self-determination needs in workers with CM and other chronic health conditions. Based on the propositions of PWT (Duffy et al., 2016) and previous empirical research reviewed above, we hypothesize that decent work relates positively to survival, social contribution, and self-determination need satisfaction (Hypotheses 1–3); survival, social contribution, and self-determination need satisfaction relate positively to work fulfillment (Hypotheses 4–6) and general well-being (Hypotheses 7–9); decent work relates positively and indirectly (via survival, social contribution, and self-determination need satisfaction) to work fulfillment (Hypotheses 10–12) and general well-being (Hypotheses 13–15); and condition severity and work limitations relate negatively to work fulfillment (Hypotheses 16–17) and general well-being (Hypotheses 18–19). By including in our model two additional variables that, although not specified in PWT, have been linked empirically to indicators of work fulfillment and general well-being in workers with chronic health conditions, we provide a particularly rigorous test of PWT’s propositions regarding outcomes of decent work.
Method
Participants and Procedure
Participants were 346 employed adults (313 women, 30 men, 1 transgender, 2 indicating some other gender) diagnosed with CM; 54.9% had been diagnosed with at least one additional chronic health condition, the most common of which included Ehlers-Danlos Syndrome, hypothyroidism, syringomelia, degenerative disk disease, and arthritis. Participants’ ages ranged from 18 to 63 years (M = 37.48 years, SD = 9.46 years). The majority (88.7%) of participants identified ethnically as White/European American, with 4.0% multiethnic, 3.6% Latinx, 2.6% Black/African American, .6% American Indian/Alaskan Native, and .3% Asian/Asian American. In terms of geographic location, 93.9% of participants for whom data were available were living in the United States, with 4.1% living in Australia, .8% in the United Kingdom, .4% in Ireland, .4% in Belgium, and .4% in Portugal. The majority (92.2%) identified as heterosexual, with 4.3% bisexual, 1.7% lesbian, .9% some other sexual orientation, and .3% gay. In terms of social class, 50.0% identified as middle class, 34.1% as working class, 10.1% as upper middle class, and 5.8% as lower class. The majority (66.8%) of participants were employed full-time outside the home, with 21.7% employed part-time outside the home, 6.4% self-employed part-time at home, and 3.2% self-employed full-time at home. The mean number of hours worked per week was 33.88 (SD = 12.44). The most frequently reported occupations were nursing/patient care (7.2%), management/supervision (6.6%), retail sales and merchandising (4.0%), teaching (3.8%), and accounting (2.6%). Regarding highest level of education completed, 31.5% indicated associate’s degree or trade school, 26.0% high school graduate, 21.4% bachelor’s degree, 16.5% master’s degree, 2.9% doctorate degree, and 1.7% some high school.
We recruited participants in two ways. First, we sent an email invitation containing the survey link to 648 individuals from the Chiari 1000 registry (an online database established through the Chiari research consortium at the University of Akron specifically for the collection of behavioral and anatomical information from individuals diagnosed with CM) who had previously expressed interest in participating in future studies. These individuals were invited to participate in an online study of the career development experiences of individuals with CM. Second, a brief description of the study with a link to the online survey was posted on the Conquer Chiari website. Participants who met the inclusion criteria (i.e., ≥ 18 years of age and currently employed) provided informed consent and then completed an online survey containing the measures described below via the Qualtrics internet-based survey platform. In addition to bot detection and other data protection settings built into the Qualtrics platform, participants were asked to respond to several specific qualitative items (e.g., current occupation, chronic health conditions besides CM) and informed that they had the opportunity to be included in a raffle to win one of ten $50 Visa gift cards. Qualitative questions and randomized participant incentives such as raffles are recommended strategies to reduce the likelihood of internet bots and other “mischievous respondents” (Griffin et al., 2022, p. 2841) and ensure data integrity. Upon completion of the survey, participants were debriefed and offered the opportunity to enter the raffle. A total of 443 participants began the survey; however, 91 cases were excluded because they did not meet the inclusion criterion of currently being employed. Another six cases were dropped because they failed to complete any of the measures included in the major analyses, resulting in a final usable sample of 346.
Instruments
Condition Severity
Consistent with previous studies assessing condition severity in individuals diagnosed with CM (e.g., Meeker et al., 2015), participants indicated the severity of their CM condition by responding to one item (“How would you rate the current severity of your Chiari malformation symptoms?”) on a 3-point Likert-type scale (1 = mild, 3 = severe).
Work Limitations
We defined functional limitations at the workplace (i.e., work limitations) as the extent to which participants’ CM symptoms or treatment interfered with their ability to perform essential work-related activities during the past month. We consulted previously developed measures of functional limitations (e.g., Work Limitations Scale [Lerner et al., 2001]); however, we believed it necessary to develop a functional limitations survey that would suitably reflect the often unique physical symptomology experienced by individuals with CM -- particularly if their symptoms were limited to head and neck movements/posturing, thus affecting a more limited range of work-related behaviors. The goal was to survey functional skills across a diverse range of physical and cognitive work-related tasks, thereby hoping to gain some degree of completeness (precision) in assessing the types of activities that could be overlooked yet of particular importance to someone with these types of symptoms. Based on existing measures and the current research regarding the symptoms and experiences of individuals with CM, the first and third authors rationally developed 31 items capturing work-related activities requiring physical, cognitive/mental, interpersonal/emotional, and task-related demands in workers with CM. Items developed to capture work-related difficulties stressing a particular demand (e.g., repetitive movements, extended standing) were combined to form rationally derived subscales ostensibly reflecting a given functional domain (e.g., physical); however, all 31 items were specifically intended to reflect the overarching functional limitations construct.
Participants used a Likert-type scale (1 = not at all; 2 = yes, somewhat; 3 = yes, to a great extent) to indicate the degree to which they had experienced problems meeting the job demands of 31 different work-related activities within the past month due to their CM condition. Items captured activities requiring physical (e.g., extended standing, reaching for objects), cognitive/mental (e.g., sustained concentration, recalling important information), interpersonal/emotional (e.g., managing irritability resulting from symptoms, balancing work and home life), and task-related (completing work tasks on time, writing) demands. Item ratings for each subscale were averaged, with higher scores indicating higher levels of each work limitations domain. Cronbach alpha coefficients for the four subscales ranged from .78 to .89 (item-subscale total correlations ranged from .35 to .81, mdn = .59), and the total scale alpha was .95 (item-total correlations ranged from .60 to .75, mdn = .71). Validity support was demonstrated through strong positive correlations (ranging from .58–.75) with a measure of chronic pain interference at work.
Decent Work
Decent work was assessed with the Decent Work Scale (DWS; Duffy et al., 2017), a 15-item self-report measure scored for five 3-item subscales: (a) safe working conditions, (b) access to health care, (c) adequate compensation, (d) free time and rest, and (e) complementary values. Participants used a 7-point Likert scale (1 = strongly disagree; 7 = strongly agree) to indicate the extent to which they agreed with each statement. Sample items include “I feel emotionally safe interacting with people at work” (safe working conditions), “I have a good healthcare plan at work” (access to health care), “I am rewarded adequately for my work” (adequate compensation), “I have free time during the work week” (free time and rest), and “The values of my organization match my family values” (complementary values). Item ratings for each subscale are summed, with higher scores indicating higher levels of each decent work dimension. Duffy et al. (2017) reported Cronbach alpha coefficients for DWS subscales ranging from .79 (safe working conditions) to .97 (access to healthcare) in a sample of 589 working adults and demonstrated evidence of predictive validity through anticipated correlations with job satisfaction, work meaning, and withdrawal intentions. Cronbach alpha coefficients for the current sample were as follows: safe working conditions (.82), access to health care, (.98), adequate compensation (.84), free time and rest (.87), complementary values (.96), and decent work total (.84).
Survival Need Satisfaction
According to PWT (Duffy et al., 2016), “survival needs comprise access to basic resources such as food and shelter as well as the ability to provide for oneself and family” (Duffy et al., 2019, p. 385). Based on this definition, we developed three items to measure survival need satisfaction through work: “My job enables me to provide for my family,” “My job provides a steady income,” and “I struggle to make ends meet on my salary” (reverse-scored). Participants used a 7-point Likert scale (1 = strongly disagree, 7 = strongly agree) to indicate the extent to which they agreed with each statement. Items were averaged, with higher scores indicating higher levels of survival need satisfaction. The alpha coefficient for the current sample was .77, item-total correlations ranged from .52 to .72, and inter-item correlations ranged from .39 to .65. Preliminary validity evidence was demonstrated by an expected relation with the Job Descriptive Index (Balzer et al., 1997) pay subscale.
Social Contribution Need Satisfaction
Guided by PWT (Duffy et al., 2016) as well as Autin et al.’s (2019) observation that “social contribution needs reflect the need to connect to the broader society, feel a part of one’s community, connected to something larger than oneself” (p. 198), we measured satisfaction of social contribution needs using two items developed for this study: “My work enables me to connect with others in my community” and “My work provides the opportunity to benefit the lives of others.” Participants used a 7-point Likert scale (1 = strongly disagree, 7 = strongly agree) to indicate the extent to which they agreed with each statement. Items were averaged, with higher scores indicating higher levels of social contribution need satisfaction. The two items correlated .55, and the Cronbach alpha coefficient was .71.
Self-Determination Need Satisfaction
Self-determination need satisfaction at work was assessed with the Basic Psychological Need Satisfaction at Work scale (BPNS-W; Deci et al., 2001), a 21-item self-report measure developed to assess the satisfaction of basic psychological needs (i.e., autonomy, competence, relatedness) at work. Participants used a 7-point Likert scale (1 = not at all true, 7 = very true) to indicate how true each statement was for them at work. Sample items include “I am free to express my ideas and opinions on the job” (autonomy), “Most days I feel a sense of accomplishment from working” (competence), and “I get along with people at work” (relatedness). Item ratings for each subscale are averaged, with higher scores corresponding to more perceived need satisfaction. Autin et al. (2019) reported subscale alpha coefficients ranging from .74 to .86 in a sample of 476 employed adults and found support for the measure’s convergent validity via strong positive relations with corresponding self-determination need subscales of the Work Need Satisfaction Scale. Cronbach alpha coefficients for the current sample were as follows: autonomy (.81), competence, (.77), and relatedness (.90).
Job Satisfaction
We measured job satisfaction with Judge et al.’s (1998) 5-item adaptation of Brayfield and Rothe’s (1951) measure of overall job satisfaction. Participants used a 7-point Likert scale (1 = strongly disagree, 7 = strongly agree) to rate the extent to which they agreed with each statement (e.g., “I feel fairly well satisfied with my present job”). Item ratings are averaged, with higher scores indicating higher levels of job satisfaction. Judge et al. (1998) reported a Cronbach alpha coefficient of .88 for the adapted measure in a sample of 222 university employees and demonstrated evidence of its validity via correlations approaching unity with a composite measure of job satisfaction. The Cronbach alpha coefficient for the current sample was .91.
Work Engagement
Work engagement was assessed with the 9-item Utrecht Work Engagement Scale (UWES-9; Schaufeli et al., 2006). The UWES-9 can be scored for three work engagement dimensions (vigor, dedication, and absorption) as well as for total work engagement. Participants rated how frequently they experienced each statement using a 7-point Likert scale (0 = never, 6 = always/every day). Sample items include “At my work, I feel bursting with energy” (vigor), “I am enthusiastic about my job” (dedication), and “I am immersed in my work” (absorption). Item ratings are averaged, with higher scores indicating higher levels of work engagement. Schaufeli et al. (2006) reported a Cronbach alpha coefficient of .92 for the UWES-9 total scale in a sample of 14,521 workers from 10 different countries and demonstrated evidence of validity via inverse correlations with burnout. The Cronbach alpha coefficient for the current sample was .92.
Meaningful Work
The experience of meaningful work was assessed with the 10-item Work as Meaning Inventory (WAMI; Steger et al., 2012). The WAMI is scored for three dimensions of meaningful work (positive meaning, meaning making through work, and greater good motivations) as well as total meaningful work. Participants used a 7-point Likert scale (1 = strongly disagree; 7 = strongly agree) to indicate the extent to which they agreed with each statement. Sample items include “I have found a meaningful career” (positive meaning), “My work helps me better understand myself” (meaning making through work), and “I know my work makes a positive difference in the world” (greater good motivations). Item ratings were averaged, with higher scores indicating higher levels of meaningful work. Steger et al. (2012) reported the following Cronbach alpha coefficients for WAMI subscale and total scale scores in a sample of 370 university employees: positive meaning (α = .89; current α = .93); meaning making through work (α = .82; current α = .92); greater good motivations (α = .83; current α = .84); and total scale (α = .93; current α = .95). In addition, WAMI subscale scores have been found to correlate as expected with job and life satisfaction, career commitment, and withdrawal intentions (Steger et al., 2012).
General Well-Being
We used the 5-item Satisfaction with Life Scale (SWLS; Diener et al., 1985) to measure the degree to which participants were generally satisfied with their lives. The SWLS asks respondents to use a 7-point Likert scale (1 = strongly disagree, 7 = strongly agree) to indicate their agreement with statements (e.g., “In most ways my life is close to my ideal”) regarding satisfaction with one’s life. Item ratings were averaged, with higher scores indicating higher levels of life satisfaction. Diener et al. (1985) reported a Cronbach alpha coefficient of .87 for the SWLS in a sample of 176 college students and demonstrated evidence of its validity via anticipated correlations with other measures of subjective well-being. The Cronbach alpha coefficient for the current sample was .88.
Results
Preliminary Analyses
Means, standard deviations, internal consistencies, and intercorrelations of all variables.

Note. Limitations = Work-Related Functional Limitations. Survival = Survival Needs. Social Contribution = Social Contribution Needs. Autonomy = Autonomy Needs. Competence = Competence Needs. Relatedness = Relatedness Needs. Correlations in bold are significant at p < .05.
All of the 346 usable cases contained at least one missing item-level data point, and the overall rate of missing data was 16.67%. Results of Little’s (1988) Missing Completely at Random (MCAR) test suggested that missingness was not systematically related to any of the study variables, χ2 (df = 188) = 193.34, p = .38. Missing data were handled using Full Information Maximum Likelihood (FIML) model estimation, a method that uses all available data to generate unbiased parameter estimates and standard errors (Schlomer et al., 2010).
Measurement Model
Prior to testing the hypothesized structural model (see Figure 1), we performed a confirmatory factor analysis (CFA) to evaluate the goodness of fit of the indicator variables and their corresponding latent factors as well as the factor correlations. For the hypothesized measurement and structural models, we created seven latent variables. We used the four work limitations subscales as indicators of the latent work limitations construct; the three BPNS-W subscales as indicators of the latent self-determination need satisfaction construct; and the Job Satisfaction, Work Engagement, and Meaningful Work scales as indictors of the latent work fulfillment construct. We used the survival need satisfaction, social contribution need satisfaction, and SWLS items as indicators of survival need satisfaction, social contribution need satisfaction, and general well-being latent variables, respectively. Based on previous research demonstrating that a bifactor structure best fits the DWS items (Douglass et al., 2017; Duffy et al., 2017), we used the 15 DWS items as indicators of a general decent work factor as well as specific decent work factors corresponding to the five DWS subscales. That is, DWS item responses were allowed to load on both a general decent work construct and a specific decent work construct (e.g., safe working conditions) that was orthogonal to the general latent construct. Given that we were interested in the ability of the general decent work construct to predict the outcome variables, the covariances of the specific decent work factors with the other constructs of interest were constrained to zero in the measurement model, and the specific decent work factors were not included as predictors in the hypothesized structural model. Finally, symptom severity was included as a single manifest variable.
We used M-Plus Version 8.1 (Muthén & Muthén, 1998-2018) with ML estimation procedures to evaluate the hypothesized measurement and structural models. Model fit was evaluated using the χ2 goodness-of-fit test, comparative fit index (CFI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). CFI values close to .95, RMSEA values ≤.06, and SRMR values ≤.08 indicate a good fit (Kline, 2016). CFA results revealed that the measurement model fit the data well, χ2 (552, N = 346) = 1060.24, p < .001, CFI = .94, RMSEA = .052, 90% CI [.047, .056], SRMR = .063. All factor loadings were significant (p < .001), ranging from .28 to .63 for the decent work factor, .80 to .91 for work limitations, .64 to .87 for survival needs, .59 to .95 for social contribution needs, .74 to .86 for self-determination needs, .81 to .92 for work fulfillment, and .60 to .90 for general well-being. (Note that the relatively lower decent work factor loadings are based on a bifactor model, which implies that DWS item responses are influenced by both a general decent work factor and a specific decent work factor that is orthogonal to the general factor and other specific factors).
Structural Model
The hypothesized structural model (see Figure 1) included direct paths from decent work to survival, social contribution, and self-determination need satisfaction; and from condition severity, work limitations, survival need satisfaction, social contribution need satisfaction, and self-determination need satisfaction to work fulfillment and general well-being. The model also included correlations between condition severity, work limitations, and decent work, and between the two outcome variables. The structural model provided a good fit to the data, χ2 (560, N = 346) = 1078.36, p < .001, CFI = .94, RMSEA = .052, 90% CI [.047, .056], SRMR = .063. Figure 2 depicts the standardized parameter estimates for the hypothesized structural model. As hypothesized, decent work had significant (p < .001) and positive direct effects on survival (Hypothesis 1), social contribution (Hypothesis 2), and self-determination need satisfaction (Hypothesis 3); social contribution (Hypothesis 5) and self-determination need satisfaction (Hypothesis 6) had significant (p < .001) and positive direct effects on work fulfillment; survival (Hypothesis 7) and self-determination need satisfaction (Hypothesis 9) had significant (p < .01) and positive direct effects on general well-being; and condition severity had a significant (p < .01) negative direct effect on general well-being (Hypothesis 18). Contrary to our hypotheses, direct paths from survival need satisfaction (Hypothesis 4), condition severity (Hypothesis 16), and work limitations (Hypothesis 17) to work fulfillment, as well as paths from social contribution needs (Hypothesis 8) and work limitations (Hypothesis 19) to general well-being, were not significant. The variables explained 77% of the variance in work fulfillment and 35% in general well-being. Standardized parameter estimates for the hypothesized structural model.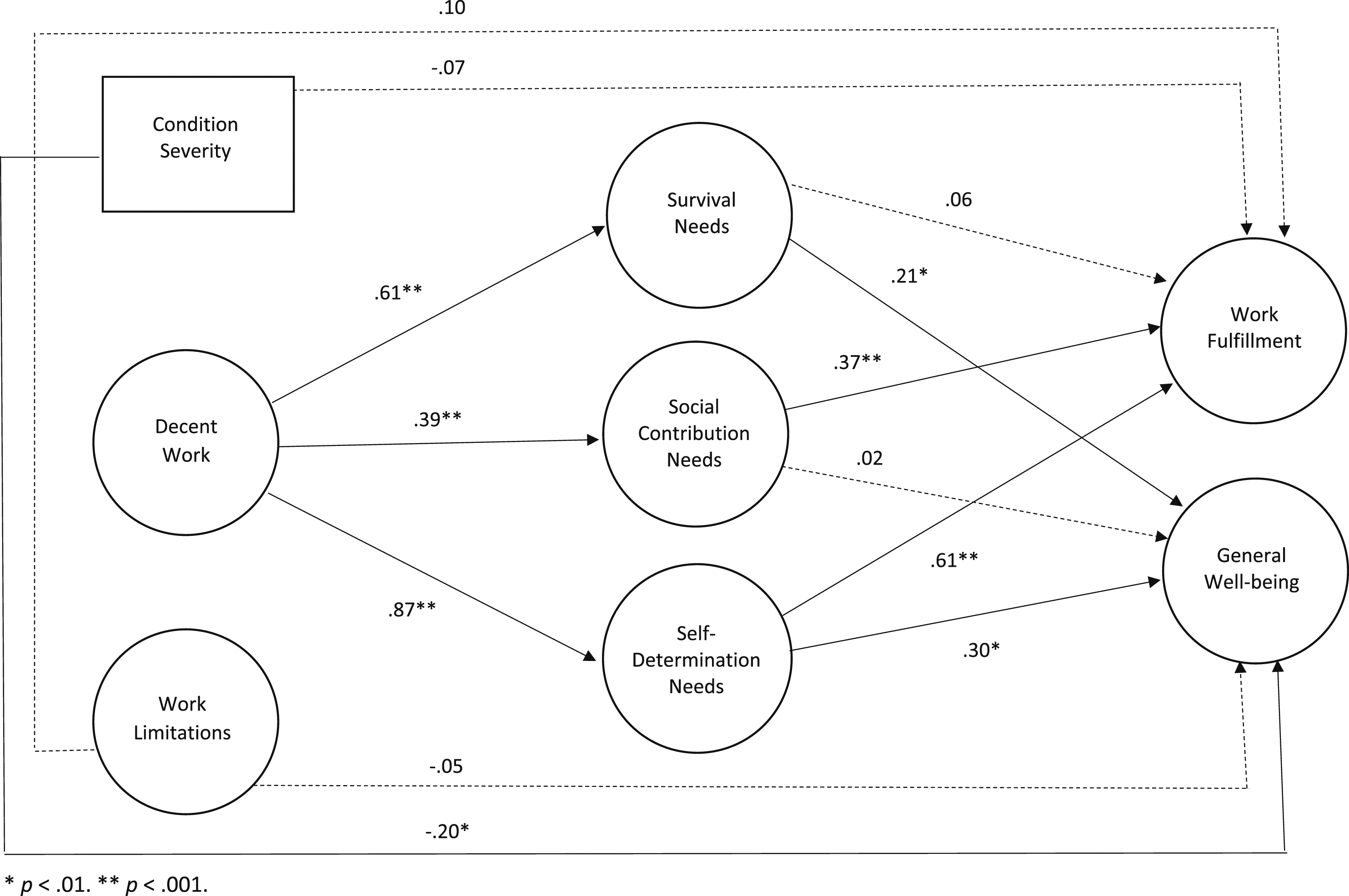
Although the hypothesized structural model fit the data well, we also considered an alternative model that included additional direct paths from decent work to work fulfillment and general well-being. Results indicated that this model provided a good fit to the data, χ2 (558, N = 346) = 1072.74, p < .001, CFI = .94, RMSEA = .052, 90% CI [.047, .056], SRMR = .064. However, the alternative model did not fit the data significantly better than did the hypothesized model, Δχ2 (2, N = 346) = 5.62, p > .05). Furthermore, the alternative model produced an out-of-range path coefficient from self-determination need satisfaction to work fulfillment (β = 1.06). Therefore, we interpreted the hypothesized fully mediated model.
Mediation Results
Bootstrap Tests of Hypothesized Indirect Effects.

Note. N = 346. Survival = Survival Need Satisfaction; Social Contribution = Social Contribution Need Satisfaction; Self-Determination = Self-Determination Need Satisfaction; β = standardized path coefficient; B = mean indirect effect; SE = Standard error of mean; CI = Confidence interval for mean indirect effect.
aValues are based on unstandardized path coefficients.
Discussion
The current study examined predictors of work fulfillment and general well-being with a sample of employed individuals with CM. Using a PWT framework, we sought to build on existing research (e.g., Duffy et al., 2019) by examining the connection of decent work to each of these outcomes, both directly and via the fulfillment of survival, social contribution and self-determination needs. Additionally, we make unique contributions by (a) studying a sample of adult workers with a specific chronic health condition and (b) exploring the added predictor variables of condition severity and workplace limitations. In the following sections, we discuss our findings by highlighting results of the model as a whole and then highlighting results specific to our added constructs.
Overall Model Findings
A slew of studies have examined correlations between decent work and proposed PWT outcomes (e.g., Allan, Tebbe, et al., 2019; Duffy et al., 2021; Seol et al., 2023), in particular job satisfaction, work meaning, and life satisfaction. However, only two current studies have examined the full PWT outcome model akin to the current study, which were completed with a general sample of working adults (Duffy et al., 2019) and Navy midshipmen (Seol et al., 2023), exploring the three need satisfaction mediators with various physical and mental health as outcome variables. One other study by Autin et al. (2019), with a similar general sample of employed adults, looked at the three need satisfaction variables predicting job and life satisfaction in a structural model, but did not include decent work. These studies offer useful comparisons to the results from the current study, which was completed with a more specific sample of employed adults with a chronic health condition and tested the full PWT outcome model.
In the current study, like Duffy et al. (2019) and Seol et al. (2023), viewing one’s job as decent significantly predicted all three need satisfaction constructs. Workers that were more likely to attain decent work were also more likely to feel their work met their needs for survival, social contribution, and self-determination. Akin to Duffy et al. (2019), of the three need satisfaction links, the strongest was the connection between decent work and self-determination need satisfaction. This adds more evidence to the notion that attaining decent work may be especially linked with feeling competence, autonomy, and relatedness in one’s job for all workers.
The connection between need satisfaction and outcomes, as well as how the different needs functioned as mediators, are also interesting to compare to prior studies. In Duffy et al. (2019) and Autin et al. (2019), all three needs significantly predicted mental health/life satisfaction, whereas in the current study social contribution needs did not predict general well-being. In Autin et al. (2019), only social contribution and self-determination needs predicted job satisfaction, which is identical to the current study as survival need satisfaction was a nonsignificant predictor of work fulfillment. Finally, in Seol et al. (2023), the three needs predicted PTSD and post traumatic growth. First, considering the similarities, it may be that meeting survival needs through one’s job has less of a connection with how one feels about that job and more of a connection with overall mental and physical health. Second, considering the differences, it may be that - for the specific sample in the current study - contributing to society via one’s job is important for enhanced work fulfillment but is less important for enhanced overall well-being. This difference could be due to differences in how each of these studies conceptualized overall well-being, or could be related to our specific sample. Future research would be needed to examine these possibilities.
Finally, the significance of numerous direct paths within the model allowed us to test our mediation hypotheses. Specifically, we proposed decent work would link with greater work fulfillment and general well-being because of enhanced survival, social contribution, and self-determination need satisfaction. Like Duffy et al. (2019), decent work connected to general well-being via survival and self-determination needs. Participants in our study with greater levels of decent work were more likely to have enhanced well-being because of meeting survival and self-determination needs at work. Additionally, social contribution and self-determination needs significantly mediated the links between decent work and work fulfillment. This suggests that participants in our study with greater levels of decent work were more likely to be fulfilled with their work because of that work allowing for the contribution to others and boosting a sense of self determination.
It is critical to note that because this was a cross-sectional study, we cannot infer causation with our results. However, results generally support key propositions from PWT as they apply to a unique sample of employed adults with CM. They also speak to some potentially interesting differentiation that occurs in how decent work links to well-being in the workplace compared to general well-being. Namely, self-determination needs consistently explain the relation of decent work to work fulfillment and general well-being, whereas survival needs appear to be more explanatory for the decent work-general well-being relation and social contribution needs appear to be more explanatory for the decent work‐work fulfillment relation. Although future research will be needed to replicate these findings, they have important theoretical implications as some needs may only explain the relation of decent work attainment to certain types of well-being outcomes.
Sample Specific Constructs
In the current study we included the severity of participants condition and their workplace limitations as two variables also proposed to relate to work fulfillment and general well-being. Including them in the model as direct predictors of our key outcomes variables allowed us to (a) see if these paths were significant and (b) partial out the variance attributed by these constructs when examining the role of other PWT variables within the model.
Perhaps the most interesting takeaway from the inclusion of these variables was their small to minimal connection with either outcome. Only condition severity was negatively related with general well-being, and neither variable was related to work fulfillment. Given the well-established connection between the severity of one’s chronic illness and general well-being (Huber et al., 2008; Ryan et al., 2007; Yaghmaian & Smedema, 2019), the connection of these variables in the current study makes sense. However, the fact that neither variable predicted work fulfillment may showcase a positive finding from our study. Namely, for our sample of chronically ill workers, their ability to be fulfilled within the workplace may have much more to do with that work meeting their needs for social contribution and self-determination and much less to do with the severity of their condition or how much that condition was hindering their work. From a practical perspective, this may have important implications in conceptualizing best ways to improve the work-related well-being of employees with chronic health conditions.
Practical Implications
The results of this study may have important practical implications, in particular when working with individuals who have chronic health conditions around career related concerns. A recent article by Blustein et al. (2019) highlighted how PWT may be best used in a counseling setting. In that article, the authors argued counselors should conduct a needs assessment around clients’ work concerns and explore possibilities for agentic change using a variety of techniques, such as critical reflection and action and broadening social support. In the current study we demonstrate that need satisfaction was the primary connector between decent work and work and well-being outcomes. As such, working with clients with chronic health conditions may involve efforts to both (a) find decent work via new employment and (b) help clients maximize need satisfaction within their current job.
For the former, a key to this process is understanding what decent work looks like for specific clients. Although PWT has a detailed definition of the construct, this may not be universal. For example, some individuals with chronic health conditions may view workplace protections as a central component of decent work. Next is goal setting - what needs to happen to find a decent job? Blustein et al. (2019) suggest proactive engagement as key – encouraging clients to reflect on their barriers to decent work attainment and to identify people, situations, and personal characteristics that can be drawn on as tools to work past these barriers. On the other hand, when clients are in jobs that are not meeting their needs – but are also not in a position to leave those jobs – the goal is to build greater need satisfaction where possible. Although survival need satisfaction may be less easy to change without switching jobs, job crafting strategies (Berg et al., 2013) may be useful in helping clients find ways to make their work more prosocial (social contribution needs) or to find ways to build greater autonomy and interpersonal connection (self-determination needs). Here counselors would need to understand each client’s specific work environment and pinpoint areas where crafting may be possible.
Limitations and Future Directions
The results and conclusions of the current study need to be considered cautiously given a variety of limitations. First and foremost, the study was cross sectional and thus causality cannot be determined. Although the variables were positioned according to theory, longitudinal studies would be needed to confirm these findings. There have been several recent attempts to study these constructs across time, namely looking at how decent work predicts meaningful work, turnover intentions, and physical health (e.g., Allan et al., 2020; Duffy et al., 2021; Wan & Duffy, 2022). These studies have generally shown decent work to significantly predict these variables across time, but more work is needed to tease apart the bi-directional relations amongst this group of constructs. Second, although a strength of this study is focusing on a particular sample of understudied participants, the sample is still very specific and may limit the degree to which we can extend our findings.
However, given the high rate (54.9%) of comorbid conditions experienced by our participants, our findings may generalize to the larger population of American workers with chronic health conditions. Future research is needed to test some of the ideas from this study – especially around how certain needs mediate the decent work-well-being relation – with larger samples and samples with a greater variety of marginalized identities. It may be that individuals with health conditions that more directly affect work related tasks or workplace experiences may be more likely to have threats to decent and fulfilling work. Indeed, looking at differences between health conditions with models in this study would be an interesting research direction. Third, our sample was predominantly white, raising the question of how applicable these findings would be for individuals with multiple marginalized identities. Finally, our study is limited by survey methodology, where we are unable to capture the potential wide-ranging impacts an individual’s health condition may have on their workplace experiences. Qualitative studies would be very helpful in better understanding these experiences.
Conclusion
Collectively, our results build on existing research (e.g., Duffy et al., 2019; Seol et al., 2023) by providing preliminary support for the applicability of PWT’s outcomes of decent work in adult workers diagnosed with CM. Consistent with PWT, our results underscore the importance of decent work—via the fulfillment of survival, social contribution, and self-determination needs—in the work fulfillment and general well-being of workers with CM. Finally, for our sample of workers with CM, the severity of their chronic health condition had a modest but significant negative effect on their general well-being, but not on their level of work fulfillment.
Footnotes
Acknowledgments
We thank the people who participated.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Conquer Chiari Research Grant awarded to the University of Akron from the Conquer Chiari Foundation (1000003844).