
Abstract
This commentary explores Medicaid's role for children with special health care needs today and considers how changes to Medicaid's federal financing structure under a per capita cap or block grant could affect coverage for these children.
I. Introduction
About 14.2 million children, or 19% of all children in the U.S., have special health care needs. 1 They “have or are at increased risk for chronic physical, developmental, behavioral, or emotional conditions and also require health and related services of a type or amount beyond that required by children generally.” 2 Their needs result from a range of conditions, such as Down syndrome, cerebral palsy, and autism. They may require ongoing services, such as nursing care to live safely at home and therapies to address developmental delays.
Medicaid plays a key role for children with special health care needs by making coverage affordable and covering services that private insurance typically does not. Medicaid and the Children's Health Insurance Program (CHIP) cover about half (48%) of children with special health care needs. Medicaid/CHIP is the sole source of coverage for 41% of these children. Another 7% have Medicaid/CHIP to supplement private insurance (Figure 1). Legislative proposals that reduce and limit federal Medicaid funding through a block grant or per capita cap may pose a particular risk to children with special health care needs. While Congress did not pass such legislation in 2017, the Trump Administration's FY 2019 proposed budget continues to advance these proposals, and Congress may consider them again.
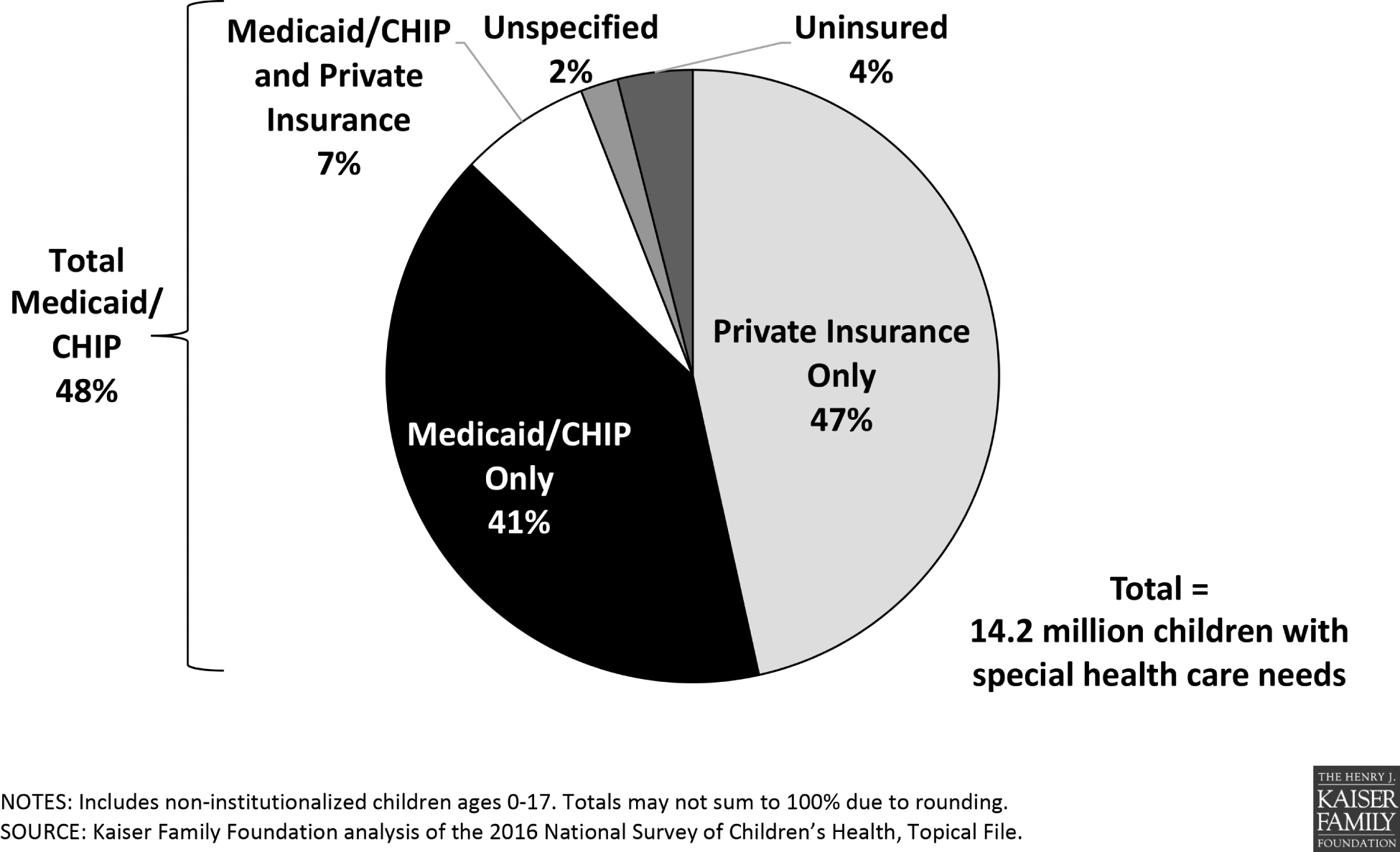
Health insurance status of children with special health care needs, 2016
This commentary explores Medicaid's role for children with special health care needs and how it could change if federal financing is reduced and capped. Part II describes key characteristics of these children. Part III describes Medicaid's role for them today. Part IV defines their major Medicaid eligibility pathways, implicated in Part V, which considers how changes to Medicaid's federal financing structure could affect these children's coverage.
II. Characteristics of Medicaid Children with Special Health Care Needs
A. Family Income
Many — but not all — Medicaid/CHIP children with special health care needs live in low-income families, below 200% of the federal poverty level (FPL, less than $41,560/year for a family of 3 in 2018). Of the 5.8 million children with special health care needs who have Medicaid/CHIP as their only coverage, nearly eight in 10 (78%) live in low-income families. Medicaid/CHIP-only children with special health care needs are significantly more likely to live in low-income families than those with private insurance only (17%) (Figure 2).
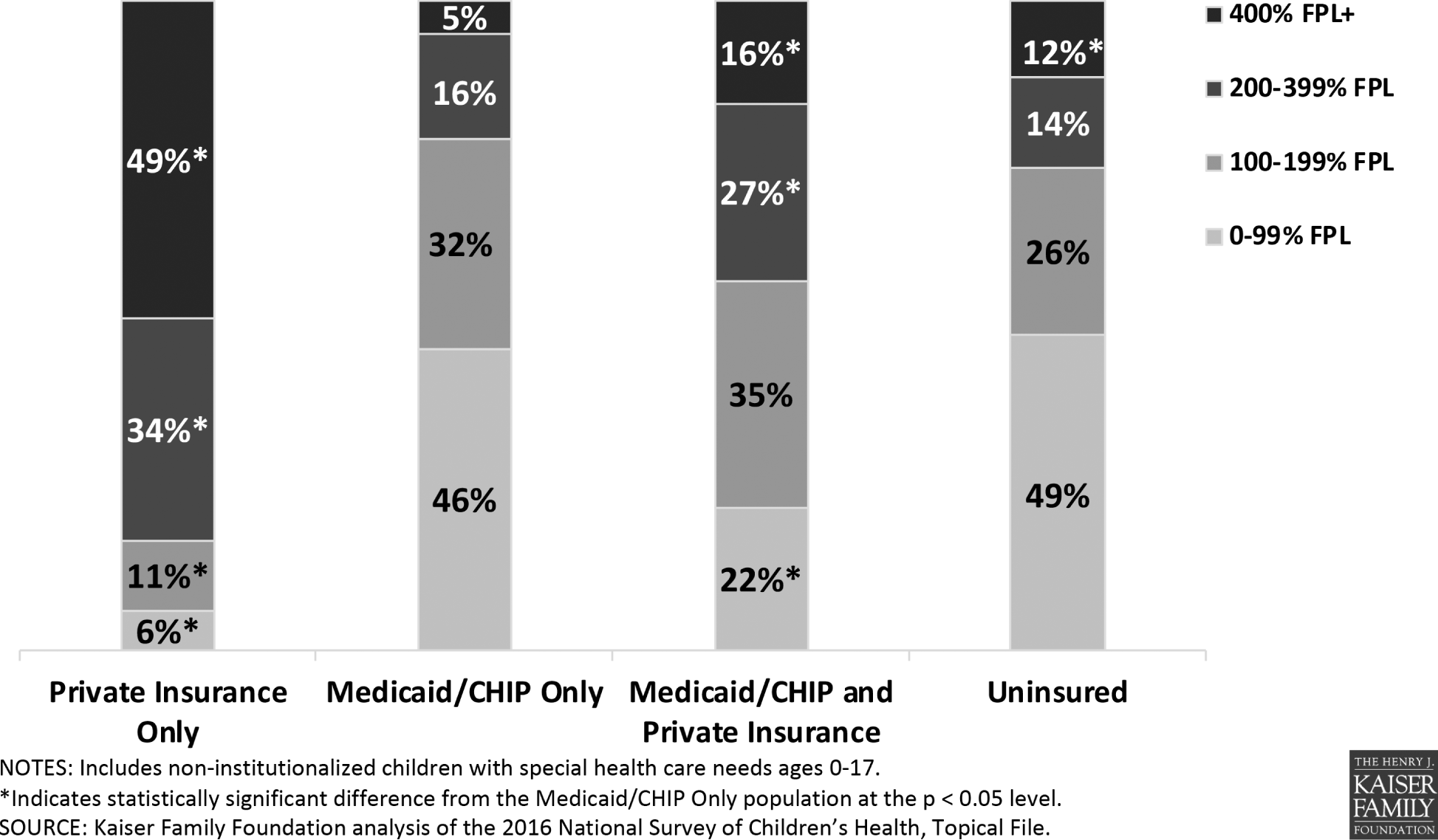
Household income of children with special health care needs by coverage status, 2016
Children with special health care needs with both Medicaid/CHIP and private insurance are significantly more likely to live in moderate to upper income families, compared to those with Medicaid/CHIP-only. Sixteen percent of those with both Medicaid/CHIP and private insurance live in families with income of 400% FPL or higher ($83,120/year for a family of 3 in 2018), compared to 5% of those with Medicaid/CHIP only, and half (49%) of those with private insurance only. Still, nearly six in 10 (57%) of the 1 million children with special health care needs who have both Medicaid/CHIP and private insurance live in a low-income family (Figure 2).
B. Health Status
Medicaid/CHIP children with special health care needs have significantly greater needs compared to those with private insurance only. About 4 in 10 (37%) Medicaid/CHIP-only children with special health care needs have 4 or more chronic conditions, compared to less than a quarter (23%) of those with private insurance only. As a result of their poorer health, those with Medicaid/CHIP-only are significantly more likely (25%) to require 3 or more health care services during a year, compared to those with private insurance alone (17%). Medicaid/CHIP-only children with special health care needs also are significantly more likely to have their health affect daily activities, with nearly twice as many (43%) having 4 or more functional difficulties compared to those with private insurance alone (24%) (Figure 3).
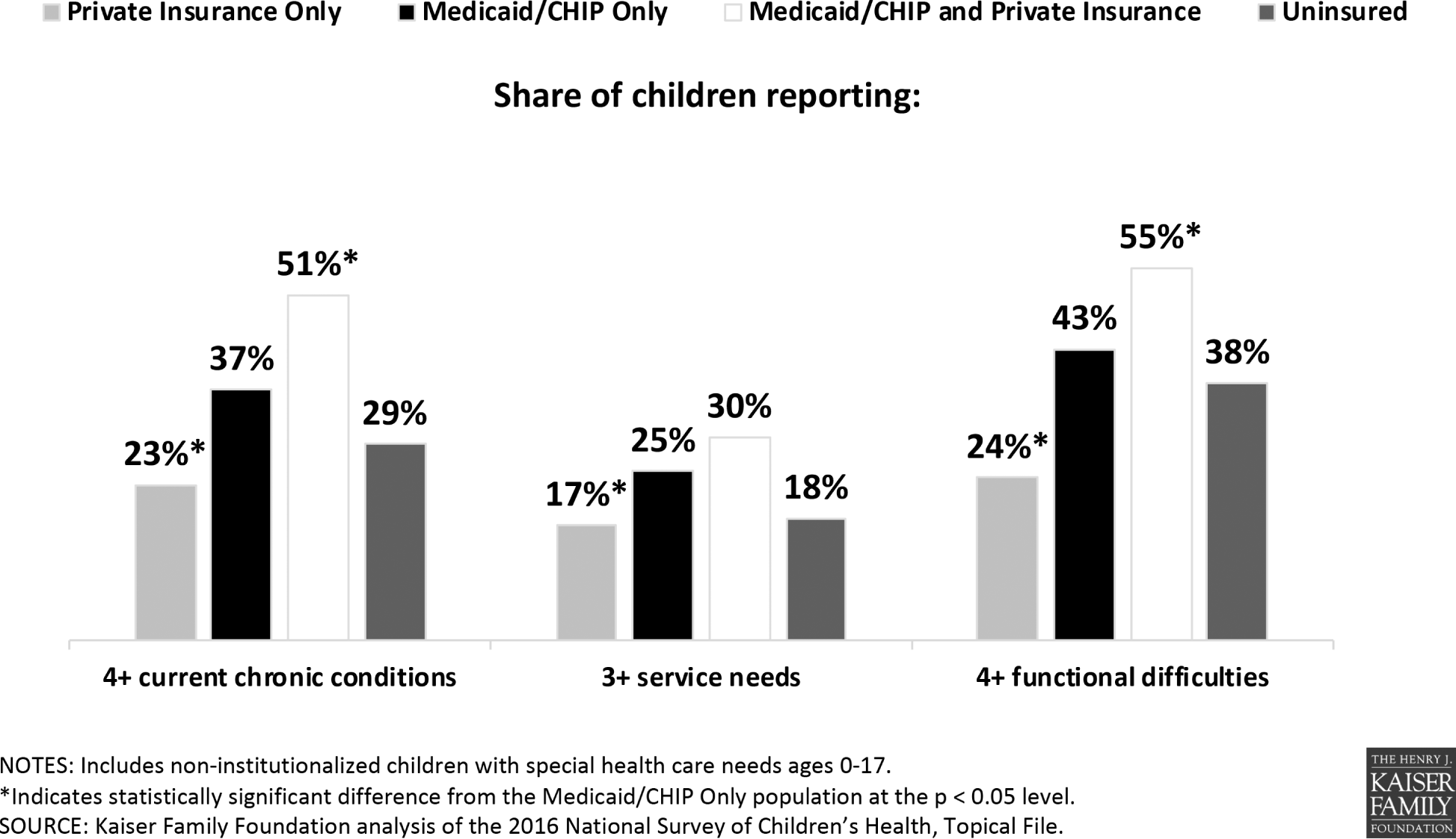
Health status of children with special health care needs, by coverage status, 2016
Children with special health care needs who have both Medicaid/CHIP and private insurance are significantly more likely to have greater needs than those with Medicaid/CHIP-only. Over half of those with Medicaid/CHIP and private insurance have 4 or more chronic conditions (51%), and over half have 4 or more functional difficulties (55%) (Figure 3).
III. Medicaid's Role for Children with Special Health Care Needs
A. Comprehensive Benefit Package
Medicaid covers a wide range of services for children with special health care needs. Medicaid's Early and Periodic Screening Diagnostic and Treatment (EPSDT) benefit includes regular medical, vision, hearing, and dental screenings; medical services like doctor visits, hospitalizations, x-rays, lab tests, and prescription drugs; behavioral health, dental, hearing, and vision care; physical, occupational, and speech therapy; and medical equipment and supplies. Medicaid also covers long-term care services, such as private duty nursing, attendant care, and assistive technology, that help children with chronic needs live with their families. Medicaid offers transportation to appointments and case management to coordinate medical, social, and other services for children with multiple needs.
Medicaid children receive services that are “medically necessary.” Specifically, the federal EPSDT standard entitles children to services that are necessary to “correct or ameliorate” physical or mental health conditions. These services must be provided for children, regardless of whether a state chooses to cover them for adults. 3
Likely due to the EPSDT benefit, Medicaid/CHIP children with special health care needs are significantly more likely to report that their coverage always meets their needs (87%), compared to those with private insurance only (56%). Two-thirds (66%) of those with both Medicaid/CHIP and private insurance report that their coverage is adequate, perhaps due to this group's greater health needs (Figure 4).
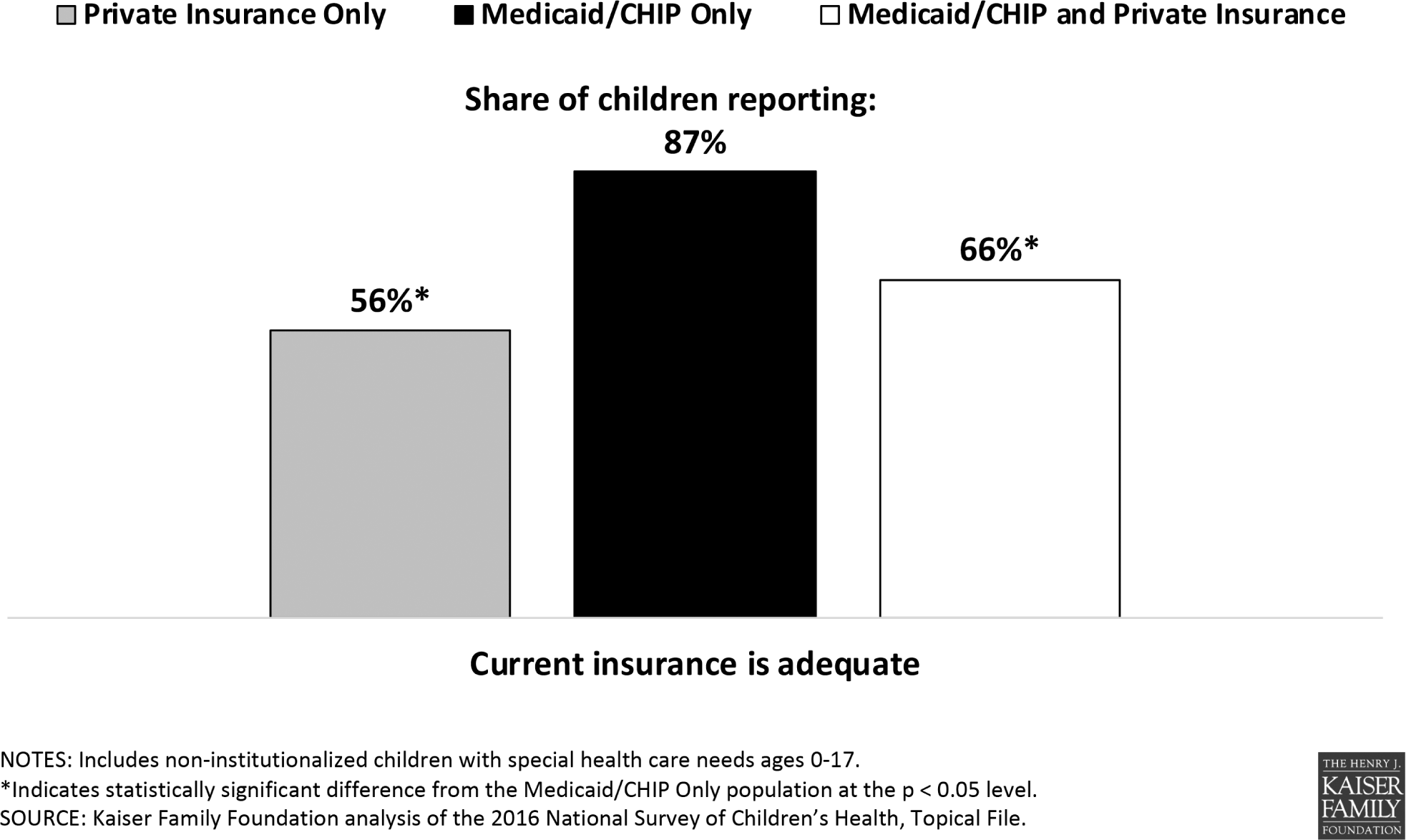
Insurance adequacy among children with special health care needs, by coverage status, 2016
B. Private Coverage Supplement
Medicaid fills in coverage gaps for privately insured children with special health care needs. Private insurance typically is designed to meet the needs of a generally healthy population rather than people with more intensive or chronic needs. Consequently, private insurance usually does not cover long-term care services and may limit coverage of other services important to children with special health care needs. Some privately insured children with special health care needs access Medicaid for wrap-around coverage for the medically necessary services on which they depend to live at home. Additionally, some children with special health care needs receive therapy through special education at school, and Medicaid supplements those services by covering additional therapies that are necessary for a child to function outside of school, at home and in the community.
C. Affordability
Because the program serves children with low incomes and/or whose extensive health needs result in high costs, Medicaid limits out-of-pocket spending. Most children are exempt from premiums and cost-sharing to ensure that coverage is affordable. In the limited circumstances in which premiums can be charged, the amounts are capped. For example, the Family Opportunity Act option allows states to cover children with significant disabilities in families with income up to 300% FPL ($62,340/year for a family of three in 2018) and charge premiums up to 5% of gross countable income. 4
Insurance affordability is a particular concern for families of Medicaid/CHIP children with special health care needs. Families of Medicaid/CHIP-only children with special health care needs are more than two and a half times as likely (53%) to find it somewhat or very often hard to cover basic needs like housing or food since their child's birth compared to those with private insurance alone (20%).
Consequently, Medicaid/CHIP-only children with special health care needs are significantly more likely to report that out-of-pocket costs are always reasonable (82%) compared to those with private insurance only (19%). They also are significantly less likely to incur annual costs of $1,000 or more (3%) compared to those with private insurance only (36%). Additionally, Medicaid's cost-sharing protections make private coverage affordable for children with both coverage sources: 43% of this group reports that out-of-pocket-costs are always reasonable, likely due to their greater health needs, and 14% incur annual costs of $1,000 or more (Figure 5).
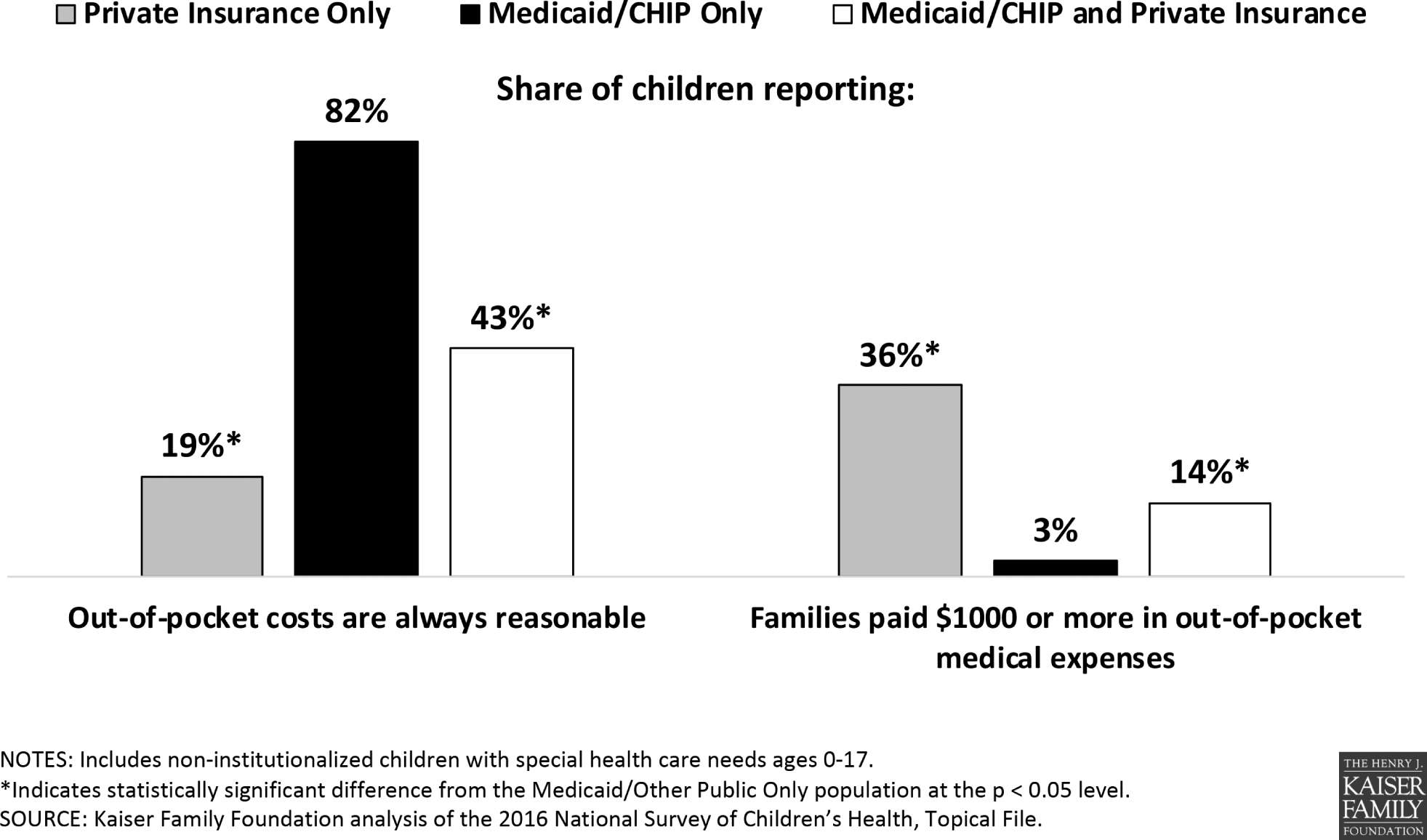
Insurance affordability for children with special health care needs, by coverage status, 2016
Insurance affordability is a particular concern for families of Medicaid/CHIP children with special health care needs. Families of Medicaid/CHIP-only children with special health care needs are more than two and a half times as likely (53%) to find it somewhat or very often hard to cover basic needs like housing or food since their child's birth compared to those with private insurance alone (20%) (Figure 6). Medicaid/CHIP-only children with special health care needs are nearly twice as likely (18%) to live in families who had to reduce their work hours or stop working due to their child's health needs, compared to those with private insurance alone (10%). Over one-third (36%) of those with both Medicaid/CHIP and private insurance have difficulty affording basic needs, and over one-quarter (27%) of this group live in families who had to reduce their work hours or stop working due to their child's health needs (Figure 6).
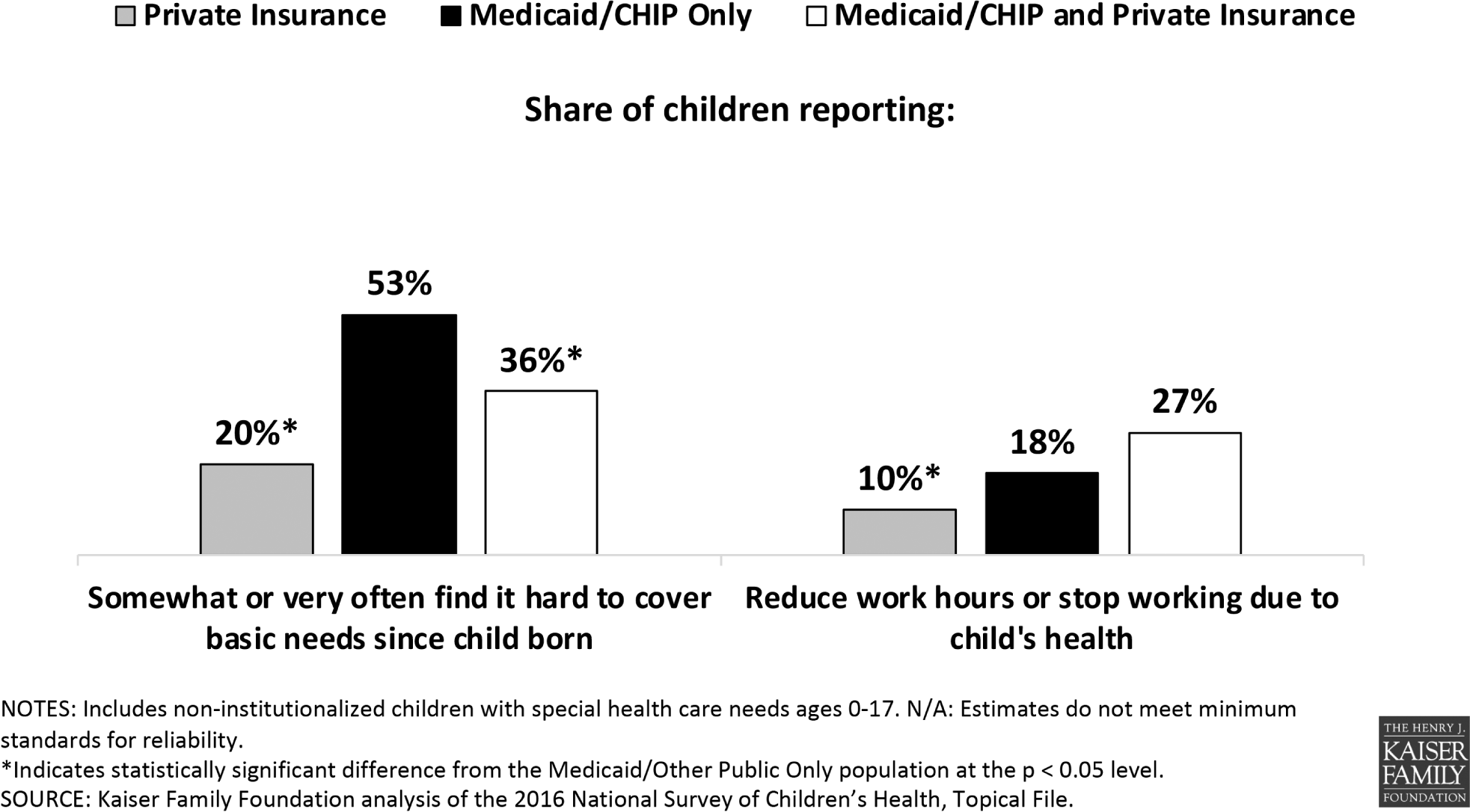
Financial impact on family among children with special health care needs, by coverage status, 2016
IV. Medicaid Eligibility for Children with Special Health Care Needs
There are 2 main ways that children with special health care needs qualify for Medicaid: poverty-related pathways based solely on low income and disability-related pathways that consider medical needs. Children with disabilities are a subset of the larger population of children with special health care needs.
A. Poverty-Related Pathways
Some children with special health care needs qualify for Medicaid based solely on their family's low income. Under the Affordable Care Act, states must cover all children in families with incomes up to 138% of the federal poverty level (FPL, $28,676/year for a family of three in 2018). Some Medicaid children with special health care needs also could qualify in a disability-related pathway (discussed below) but are instead enrolled through a poverty-related pathway because it is administratively easier and faster to establish eligibility based on low family income than based on disability. Other Medicaid children with special health care needs use more health services than those without special health care needs due to their health conditions but may not meet the stringent criteria to receive federal Supplemental Security Income (SSI) benefits or otherwise qualify “based on a disability.” Instead, these children qualify in poverty-related pathways.
B. Disability-Related Pathways
The major disability-related pathway, SSI benefits, requires children to meet family income and asset limits as well as medical criteria. States must cover children who receive SSI. However, most Medicaid children with disabilities (81%) do not receive SSI, indicating that they qualify for Medicaid on another basis (Figure 7); other data indicate that many of these children are eligible based on low family income. 5
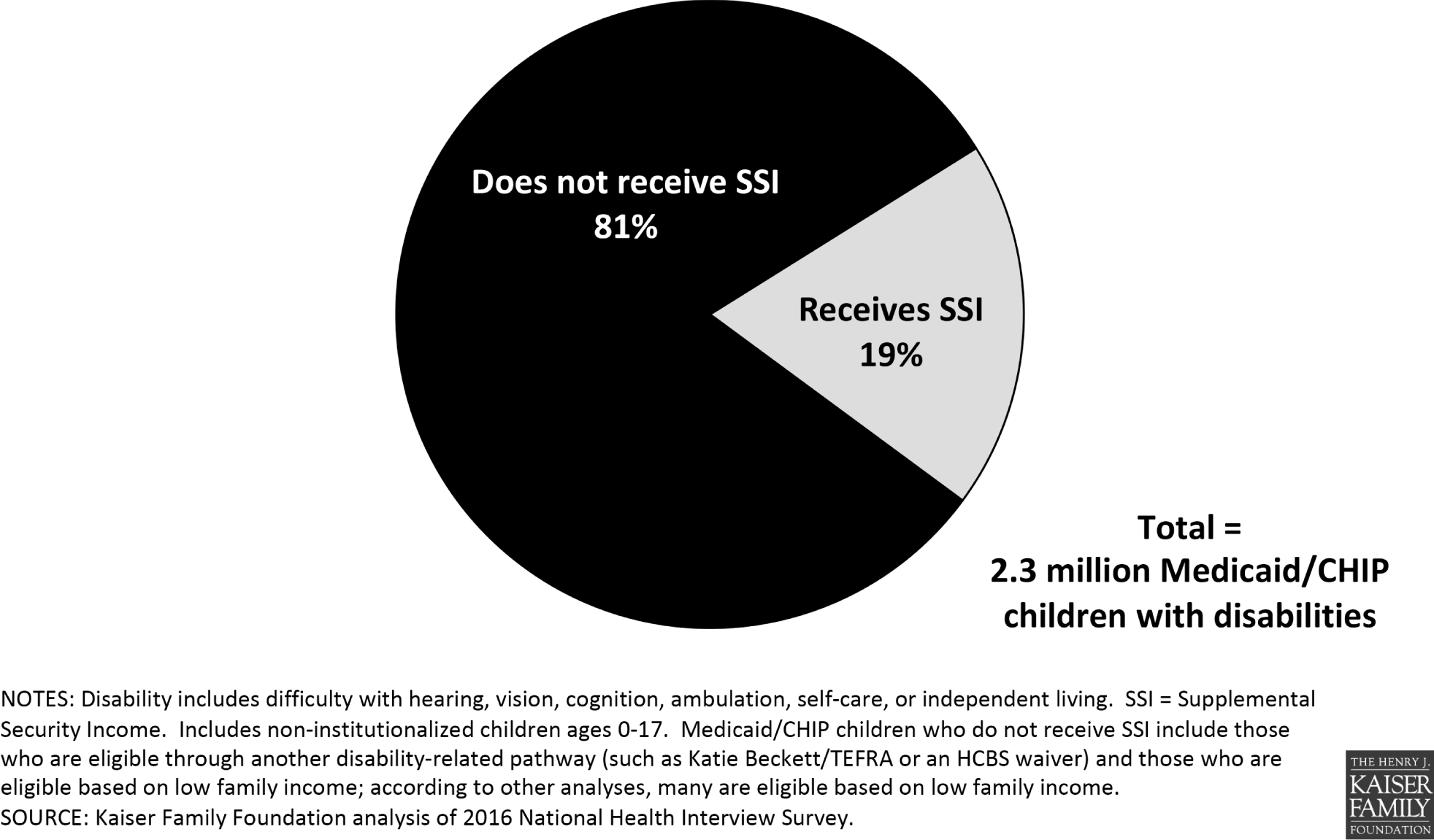
Medicaid/CHIP children with disabilities by SSI status, 2016
Other disability-related pathways disregard parental income or have higher income limits. Nearly all states choose to expand Medicaid financial eligibility for children with special health care needs through these optional pathways. As reflected by different state policy choices, the share of these children covered by Medicaid/CHIP varies by state. Twenty-two states provide Medicaid/CHIP to between 35% and 49% of the children with special health care needs living in their state. Another 22 states provide Medicaid/CHIP to between one-half and two-thirds of all children with special health care needs living in their state. Seven states cover between 23% and 34% of children with special health care needs (Figure 8).
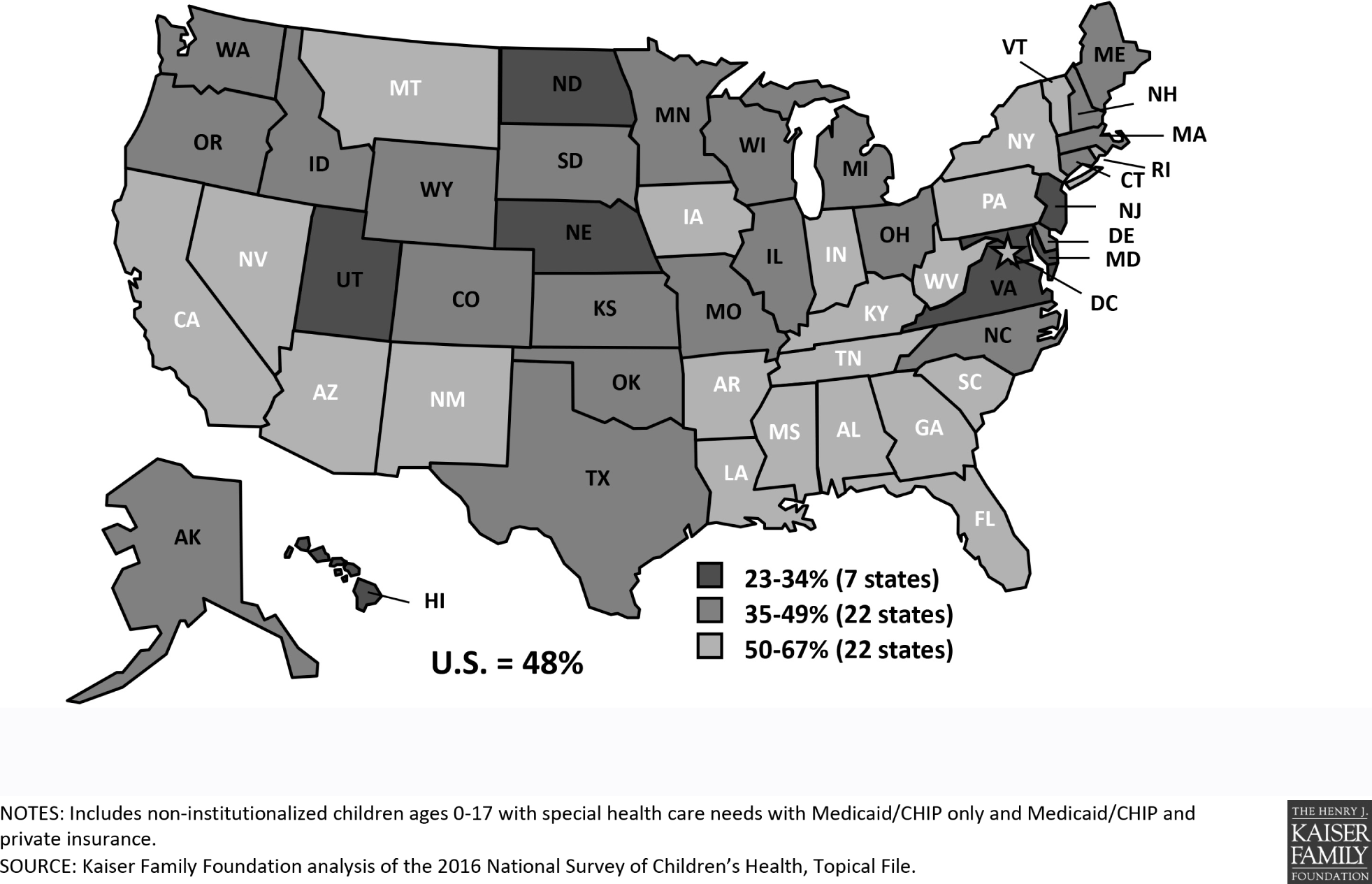
Share of children with special health care needs covered by Medicaid/CHIP, 2016
V. Implications of Federal Medicaid Financing Changes for Children with Special Health Care Needs
A. 2017 Legislative Proposals
Since the program's creation, Medicaid has guaranteed federal matching payments to states with no pre-set limit. 6 Instead, federal spending matches state spending and accounts for increases, such as those due to new services created by medical advances or higher enrollment during economic downturns. By contrast, under a block grant, states would receive a pre-set amount of federal funding. Under a per capita cap, Congress would limit how much to reimburse states per enrollee. Under either model, a base spending year would be established, and the cap would increase by a specified amount each year, typically tied to inflation or inflation plus some percentage. To achieve federal savings, the limit would be below projected growth rates and would not account for changes in state costs beyond the growth limit.
The American Health Care Act (AHCA), passed by the House in 2017, provided for a per capita cap, based on state spending in FY2016, with a state option to instead choose a block grant for certain populations, including children in poverty-related pathways. 7 Two bills considered by the Senate, the Better Care Reconciliation Act (BCRA) 8 and the Graham-Cassidy amendment, 9 provided for a per capita cap for most populations, including children in poverty-related pathways but excluding children in disability-related pathways. Neither the BCRA nor Graham-Cassidy included a block grant option for any Medicaid children.
B. Potential Risk to Children with Special Health Care Needs
Medicaid coverage for children with special health care needs could be at risk if federal financing is reduced and capped under a per capita cap or block grant as under the AHCA. While nearly all medically necessary services for children are mandatory under EPSDT, states can provide — and may look to scale back — some optional community-based long-term care services offered through waivers, which can be expensive. Additionally, many disability-related eligibility pathways for children are optional and thus potentially at risk if states must adjust to reduced federal funding. Even if optional eligibility pathways are not eliminated, budgetary pressures could lead states to scale back optional long-term care waiver services and/or provider payments, with impacts on these children's access to care and coverage that are less visible than a reduction in eligibility pathways.
Congressional proposals to exempt spending for children eligible in disability-related pathways from a per capita cap, as under the BCRA or Graham-Cassidy, are unlikely to protect children with special health care needs. As discussed above, most of these children are eligible for Medicaid through a poverty-related pathway, not a disability-related pathway, and therefore would be subject to federal funding reductions under a per capita cap. Additionally, states are likely to implement changes required to respond to federal funding caps, such as provider payment reductions, across their programs rather than by population, impacting these children regardless of eligibility pathway.
VI. Conclusion
Medicaid plays an important role for children with special health care needs. It serves as the only source of coverage for many children with special health care needs in low and middle income families. It covers children with greater health needs compared to those with private insurance alone. It also supplements private insurance, often for children with the greatest health needs, by covering services that are excluded from private insurance or for which private coverage is limited. Medicaid provides a wide range of medical and long-term care services and makes coverage affordable by limiting out-of-pocket costs. If Medicaid's federal financing structure is reduced and capped under a block grant or per capita cap, states might lower provider reimbursement rates, eliminate optional home and community-based waiver services, and/or eliminate optional eligibility pathways, placing coverage for children with special health care needs at risk.
Footnotes
Acknowledgements
The author is grateful for the contributions of Julia Foutz, formerly of the Kaiser Family Foundation, who performed the data analysis presented in this commentary.
Note
The author has no conflicts of interest to declare.