
Abstract
This study sought to translate, using a back-translation procedure, and evaluate the psychometric characteristics of Depression in the Medically Ill questionnaire (DMI-18) and its short version (DMI-10) in a Spanish population. Patients with somatic disorders (N = 366) completed the translated DMI-18 and another depression questionnaire. Among these, 167 were also assessed by a mental health professional (gold standard) to test criterion validity. Furthermore, coefficient alpha for both the versions were high (>.90), and convergent validity assessed against the Beck Depression Inventory for Primary Care, the Hospital Anxiety and Depression Scale, and the Patient Health Questionnaire–9 was satisfactory (r > .74). Confirmatory factor analysis results supported the one-factor model. When compared with the gold standard, sensitivity and specificity were 93% and 73% for DMI-18 and 87% and 74% for DMI-10, respectively. Thus, both the versions are acceptable measures that can be used by nonpsychiatric professionals to detect affective comorbidities in their patients.
Depression is common among patients with somatic disorders, with a prevalence of approximately 20% (Hilton et al., 2006; Kilbourne, Daugherty, & Pincus, 2007) and is associated with poorer prognosis and reduced quality of life (Adelman, Greene, Friedmann, & Cook, 2008; Herrero et al., 2003). However, depression often goes undiagnosed and untreated in these patients, partly because some symptoms of depression, such as apathy, fatigue, and disturbed sleep are similar to those of many somatic conditions (Herrero et al., 2003). Overlooking depression is a lost opportunity for improving the quality of life, reducing hospital stays, improving treatment adherence, and reducing the risk of suicide in patients with somatic disorders (Koening, 1997; Newport & Nemeroll, 1998).
An instrument for detecting depression, which is simple to administer, easy to score, and specifically designed for patients with somatic disorders, would be invaluable for clinicians (Bambauer, Locke, Aupont, Mullan, & McLaughlin, 2006; Beck, Steer, Ball, Ciervo, & Kabat, 1997; Diez-Quevedo, Rangil, Sánchez-Planell, Kroenke, & Spitzer, 2001; Herrero et al., 2003; Kroenke, Spitzer, & Williams, 2001; Sharp & Lipsky, 2002; Zigmond & Snaith, 1983). Ideally, depression assessment in primary and secondary care should be restricted to variables and items that avoid confounding owing to medical illness (Parker, Hilton, Bains, & Hadzi-Pavlovic, 2002). Currently, three measures that exclude somatic items exist: the Beck Depression Inventory for Primary Care (BDI-PC; Beck, Steer, & Brown, 2000), the Hospital Anxiety and Depression Scale (HADS; Herrero et al., 2003), and the Depression in the Medically Ill questionnaire (DMI; Parker et al., 2002).
The BDI-PC is a short version of the Beck Depression Inventory–II (BDI-II; Beck, Steer, & Brown, 1996), a questionnaire created to assess the severity of depression in patients with mental disorders and to detect possible depression in normal populations. Thus, this tool was not originally designed for the detection of affective conditions in patients with somatic disorders. To the best of our knowledge, only the HADS and the DMI have been so designed. The HADS is the most commonly used tool for measuring depression in primary care. It is largely based on the symptom of anhedonia among all the symptoms of depressive disorders (Herrero et al., 2003). The problem with anhedonia in primary care patients is that it appears to be associated with somatic symptomatology (Parker et al., 2002). The DMI is a valid measure of depression in the medically ill, focusing on cognitive symptoms, and includes not only anhedonia but also all areas central to depression (depressed mood, anhedonia, pessimism, low self-esteem, etc.; Parker et al., 2002; Parker, Hilton, Hadzi-Pavlovic, & Bains, 2001). So far, only English and Chinese versions of the DMI are available in two versions of different lengths: the original 18-items version (DMI-18) and the short 10-items version (DMI-10), whereas other tools, such as HADS, have been translated and validated into several languages.
In summary, the DMI provides a simple, easy, and “cognitive” measure of depression, based on the belief that excluding somatic items overcomes the confounding effects of medical illness.
The aim of this study was to develop a Spanish-language version of both the versions of the DMI and to test their psychometric properties, including internal structure, convergent validity, and criterion validity. We have also provided the sensitivity and specificity of optimal cutoff points for screening depression using the Primary Care Evaluation of Mental Disorders (PRIME-MD; Spitzer et al., 1994) structured clinical interview, Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition (DSM IV;; American Psychiatric Association, 1994) with the major depressive disorder diagnosis as the criterion variable.
Method
Participants
The study sample included 366 patients who were admitted to one of the several services of Galdakao-Usansolo Hospital or those who came in for a consultation to our outpatient clinics between November 2007 and April 2008. Galdakao-Usansolo Hospital is a 400-bed general hospital with a coverage area of 300,000 inhabitants. The hospital covers an area called Comarca Interior, situated in the Basque Country (northern Spain), and has a mixed urban, suburban, and rural population. The age distribution, education level, sources of employment, socioeconomic status, and health care services of the urban population are representative of the overall Basque Country (Instituto Vasco de Estadística, 2006). Health care in this region is provided by the public network of the Basque Health Care Service, Osakidetza, which provides free unrestricted care to nearly 100% of the population. Patients from the pain, obstetrics and gynecology, endocrinology, gastroenterology, neurology, pneumology, and psychiatry units were included in this study. The sociodemographic data obtained from the participants included gender, age, marital status, education level, and employment status. The clinical data collected included duration of the disease and any psychiatric medication taken. The majority of the participants had a European background and five were from South America. Furthermore, patients were included in the study only if they were between 18 and 85 years of age, evaluated at the hospital for a somatic illness, spoke Spanish, and agreed to collaborate in the study after being briefed about the study and its voluntary nature. Patients were excluded if they, at the physician’s discretion, had a severe physical disease, cognitive deterioration, any brain disease, or a psychotic disorder that might have compromised their ability to participate in the study by completing the questionnaires.
Instruments
The study participants completed a Spanish-language version of the DMI-18 questionnaire (Parker, Hilton, Bains, & Hadzi-Pavlovic, 2001) that had been translated from English as described subsequently. The items ranged from none (rated 0) to always (rated 3). The study participants also completed one of the following three short, easily administered depression scales, all applied in their Spanish versions.
The BDI-PC (Harcourt Assessment Inc., 2006) consisted of seven cognitive and affective items, extracted from the 21-item BDI-II (Beck et al., 1996; Sanz, García-Vera, Espinosa, Fortun, & Vázquez, 2005). It was developed for evaluating the symptoms of depression in patients reporting somatic and behavioral symptoms that may be attributable to biological, medical, alcohol, and/or substance abuse problems. Its items evidenced good internal consistency (Cronbach’s α = .92) and showed strong correlation with the Millon Clinical Multiaxial Inventory II (MCMI II) major depression and dysthymia subscales (r ≥ .68; Penley, Wiebe, & Nwosu, 2003; Sanz et al., 2005). In this study, we applied the Spanish version of the BDI-PC (Harcourt Assessment Inc., 2006; see the appendix).
The HADS (Herrero et al., 2003; Zigmond, & Snaith, 1983) was specially designed for identifying and quantifying depression and anxiety in physically ill patients. The HADS is a 14-item measure that includes a 7-item depression subscale (HADS-D) for measuring cognitive and emotional aspects of depression, predominately anhedonia, and a 7-item anxiety subscale (HADS-A) for measuring cognitive and emotional aspects of anxiety. Only the HADS-D subscale was used for the purposes of the current study. This subscale was found to have good internal consistency (Cronbach’s α = .84) as well as predictive validity (specificity = 87%; sensitivity = 72%) when applied to a Spanish population (Herrero et al., 2003).
The Patient Health Questionnaire–9 (PHQ-9; Kroenke et al., 2001) is the mood module of the Patient Health Questionnaire (PHQ; Spitzer, Kroenke, Williams, & the Patient Health Questionnaire Primary Care Study Group, 1999), a self-administered version of the PRIME-MD (Spitzer et al., 1994). The PHQ-9 consists of nine items designed to correspond to the nine diagnostic criteria for major depressive disorder covered in the DSM-IV (American Psychiatry Association, 1994; Wilhelm, Kotze, Waterhouse, Hadzi-Pavlovic, & Parker, 2004), including somatic symptoms, such as fatigue, insomnia, and anorexia. The items are rated from 0 to 3 according to increasing frequency of difficulties. In this study, we used the Spanish validation of the PHQ-9, which has a sensitivity of 89%, specificity of 87%, and correlates strongly with the total BDI score (r = .76; Diez-Quevedo et al., 2001).
Mental health professionals (six psychiatrists and four psychologists) performed the psychiatric interview using the mood module of the PRIME-MD structured psychiatric interview in Spanish (Baca et al., 1999). The mood module of the PRIME-MD has nine items that represents the nine DSM-IV depression criteria with dichotomous response categories (yes/no). The sensitivity and specificity of this instrument was found to be 72% and 86%, respectively (Baca et al., 1999).
Procedures
Back-translation procedure
Adaptation of the DMI for Spanish speakers was performed using the back-translation procedure, which optimizes conceptual equivalency (Aaronson et al., 1992; Brislin, 1970).
Translation from English to Spanish was carried out by two independent native Spanish-speaking translators who are proficient in English. The research team systematically reviewed and compared the two translations, arriving at a first consensus version. Subsequently, two other independent translators, whose native language was English and who were fluent in Spanish, back-translated the consensus version. Potential mistranslations of the original items were identified and retranslated until agreeing at a final back-translation version that was sent to the DMI’s original author (Dr. Parker) who compared it with the original version and gave his approval. The final version was administered to two small groups, one made up of patients and the other of clinical experts. After evaluating the results of this intelligibility test, small modifications were made, resulting in a final version of the Spanish DMI-18.
Validation of the translated questionnaire
All the patients who approached to take part in the study were informed about its nature by their physicians and advised of their informed consent to take part in the study. Patients who chose to participate were recruited by one of our investigators (MO or CLH), who emphasized that their participation in the study was voluntary.
Each participant was asked to complete a series of sociodemographic questions, the DMI-18 questionnaire, and one of the other three depression screening questionnaires: HADS, BDI-PC, or PHQ-9. The patients did not complete the DMI-10 questionnaire anew, and instead, a DMI-10 score was extracted for each participant from the respective items in the DMI-18. Regarding the HADS, the participants completed all 14 items, but for the purpose of this article, only the depression subscale (HADS-D) items were taken into account. Given that completing the entire battery of tests would be burdensome for the patients, we aimed for one third of the sample to complete the HADS, another one third of the sample to complete the BDI-PC, and another one third to complete the PHQ-9. The questionnaires were handed to consecutive patients, until the intended quota was approximately achieved.
After completing these materials, a mental health professional who was blinded to the results of the DMI-18 conducted a psychiatric interview of a subset of the participants on our behalf. This subset was determined by the mental health professional’s and the patients’ availability. The mental health professionals were based on the PRIME-MD to determine a diagnosis of depression. The interrater reliability of the interviewers was assessed by reviewing videotapes of 10 patient interviews originally performed by a clinical professional with wide experience in diagnosing depressive disorders (JAP). These patients did not take part in the validation study. The interrater reliability was estimated with the kappa coefficient, considering two classification categories (major depression: yes or no). The minimum kappa (κ) value accepted was set as .61 (Fayers & Machin, 2007b; Viera & Garrett, 2005). A total of 10 evaluators met this requirement. Six of them obtained a κ value of .67, for two, the κ value was .83, and for the remaining two, the κ value was 1.00.
All the study procedures were approved by the institutional review board of our hospital.
Results
Evaluation of the First Version of the Questionnaire
A total of 11 native Spanish-speaking patients who were diagnosed with depression completed the DMI-18. The average time needed was 4 minutes (SD = 2 minutes). The length of the questionnaire was considered to be adequate by seven of the participants, whereas three considered it to be short, and one response was lost. All the patients considered the questions to be adequate for detecting depression. There was also a meeting with three mental health professionals, experts in diagnosing affective disorders who, after recommending some small modifications, considered the questionnaire to be simple and sufficient both in its format, length, and objective of detecting depression.
Validation of the Translated Questionnaire
Sample description
A total of 366 patients were recruited for the study. Twelve were excluded for not answering more than nine items of the DMI, leaving a cohort of 354 patients. Of them, 125 patients completed the BDI-PC, 97 completed the HADS, and 130 completed the PHQ-9. Of the total sample, 167 were interviewed by the PRIME-MD structured clinical interview. Statistically significant differences between the interviewed and non interviewed patients were found only for the variables of gender (χ2 = 10.97; p < .001) and psychiatric drug use (χ2 = 30.18; p < .001). Sociodemographic characteristics of the entire sample are shown in Table 1.
Sociodemographic Data of the Patient Sample (N = 354).
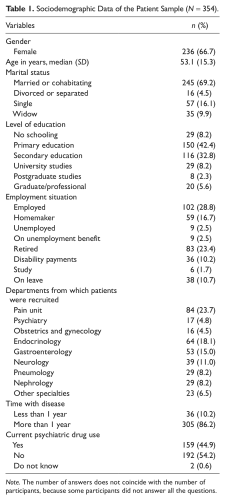
Note. The number of answers does not coincide with the number of participants, because some participants did not answer all the questions.
Missing data treatment
The missing values were imputed using the mean imputation method. This consists of substituting the missing response in an item for the mean of the responses that the participant provided on the rest of his or her items (Fayers & Machin, 2007a). The mean imputation was performed whenever more than 50% of the items had been sufficiently answered. All the 46 missing values found were imputed. More specifically, 41 participants did not answer one item, 4 participants did not answer two items, and 1 participant did not answer three items. However, no missing values pattern was observed.
Sample estimation
To estimate the sample size for the predictive precision study, we assumed that the depression rate in our medical setting would be 30% (Kilbourne et al., 2007). After interviewing 170 patients using the PRIME-MD, we expected to estimate a sensitivity of 85% with a 95% confidence interval (CI) of ±10% and a specificity of 70% with a 95% CI of ±8% (Mulrow et al., 1995).
Reliability of the DMI-18 and DMI-10
Cronbach’s alpha and average interitem correlation were calculated for examining the internal consistency. For the DMI-18, the values were .95 and .54, and for the DMI-10, the values were .91 and .52, respectively.
Structural validity
Confirmatory factor analysis (CFA) for DMI-18 and DMI-10 were performed using the unweighted least squares estimation method. This technique gives robust estimates when used with non-normally distributed data, similar to the DMI items, all of which have only four alternative replies (Brown, 2006). Based on the original DMI study (Parker et al., 2002), two hypothetical models were tested: (a) a two-factor solution model (Model 1) in which the items were divided into two intercorrelated dimensions (cognitive and affective) and (b) a one-factor solution model (Model 2), with depression being the single latent factor. The values of goodness of fit index (GFI) >.9, adjusted goodness of fit index (AGFI) >.8, and a root mean square residual (RMR) and standardized root mean square residual (SRMR) <.1 indicate a good model fit (Cole, 1987). Only items with a statistically significant factor loading (p < .05) and with loading values >.40 were accepted. Following these rules, both the models were supported by our data, having both highly satisfactory GFIs, and elevated factor loadings, with the latter also being statistically significant (p < .001; Table 2). However, in Model 1, the two factors were highly correlated (r = .91), suggesting that this model also supports a unidimensional scale.
Standardized Estimates of Unweighted Least Squares and Fit Indexes for the Two-Factor Solution (Model 1) and One-Factor Solution (Model 2; N = 354)
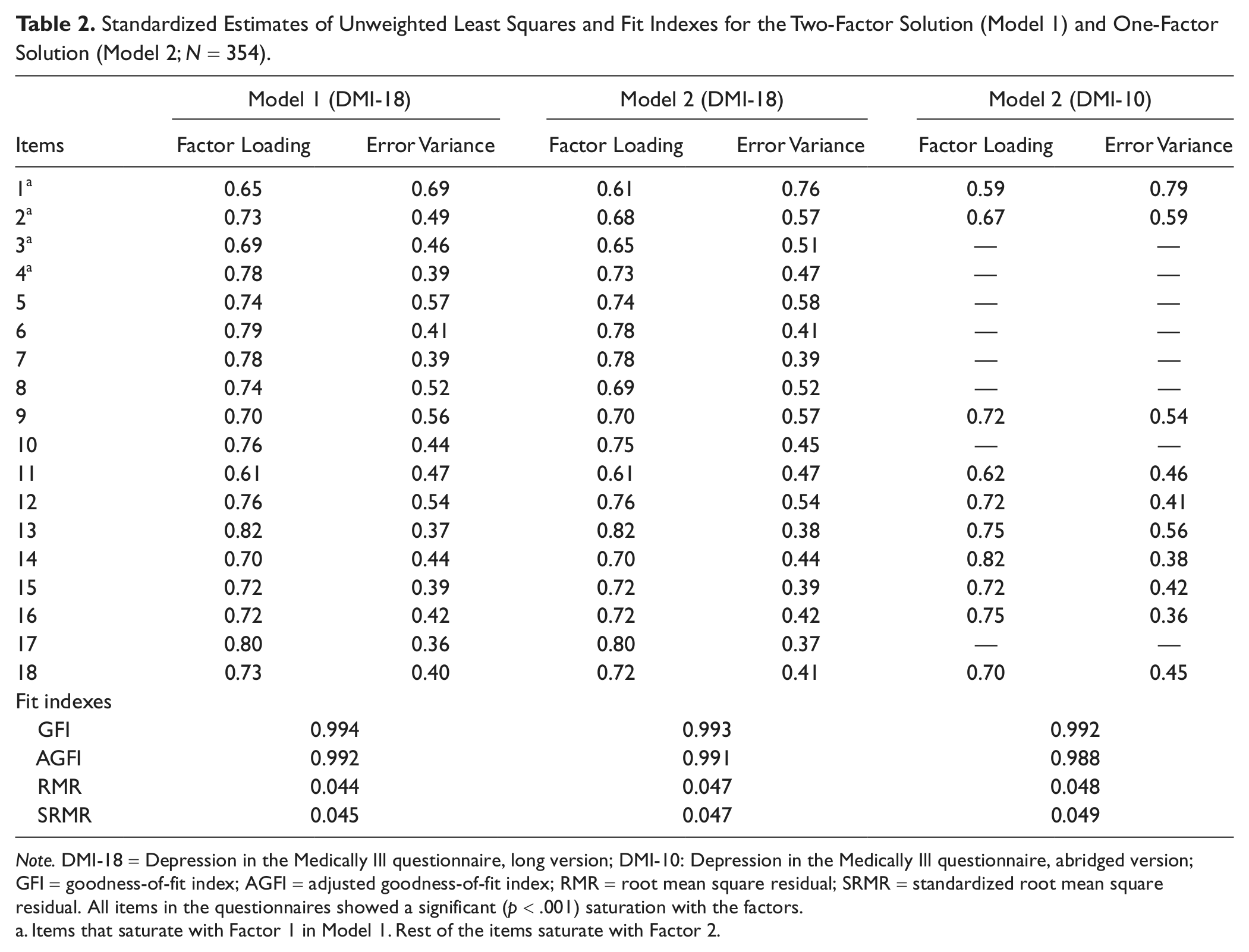
Note. DMI-18 = Depression in the Medically Ill questionnaire, long version; DMI-10: Depression in the Medically Ill questionnaire, abridged version; GFI = goodness-of-fit index; AGFI = adjusted goodness-of-fit index; RMR = root mean square residual; SRMR = standardized root mean square residual. All items in the questionnaires showed a significant (p < .001) saturation with the factors.
Items that saturate with Factor 1 in Model 1. Rest of the items saturate with Factor 2.
Convergent validity
Convergence between the new instruments scores (DMI-18 and DMI-10) and the established validated questionnaires scores (HADS-D, BDI-PC, and PHQ-9) was examined by implementing Pearson’s correlation coefficient. In addition, 95% CIs were also calculated (Table 3). The correlations were moderate to strong, all being >.70 (Hatcher, 1994).
Mean (SD) scores of the DMI-18 and DMI-10 by HADS-D, PHQ-9, and BDI-PC Categories.
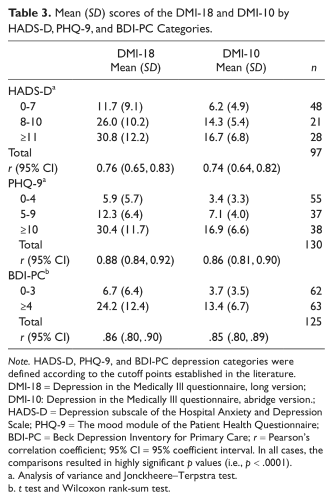
Note. HADS-D, PHQ-9, and BDI-PC depression categories were defined according to the cutoff points established in the literature. DMI-18 = Depression in the Medically Ill questionnaire, long version; DMI-10: Depression in the Medically Ill questionnaire, abridge version.; HADS-D = Depression subscale of the Hospital Anxiety and Depression Scale; PHQ-9 = The mood module of the Patient Health Questionnaire; BDI-PC = Beck Depression Inventory for Primary Care; r = Pearson’s correlation coefficient; 95% CI = 95% coefficient interval. In all cases, the comparisons resulted in highly significant p values (i.e., p < .0001).
Analysis of variance and Jonckheere–Terpstra test.
t test and Wilcoxon rank-sum test.
Known-groups validity
The mean (standard deviation; SD) scores of the DMI-18 and DMI-10 in three ordered HADS-D and BDI-PC, and two PHQ-9 categories, according to depression severity were calculated (Table 3). For the HADS-D, a cutoff point of 8 was used for possible and 11 for probable depression case. Scores <7 indicated the absence of depression (Zigmond & Snaith, 1983). For the BDI-PC, a cutoff point of 4 was used to define the presence of depression, with a score of ≥4 indicating potential presence of depression (Beck et al., 2000). Finally, for the PHQ-9, following the suggestion of the questionnaire author (Kroenke et al., 2001), score ≤4 was considered to indicate no depression, a score between 5 and 9 was considered to indicate mild depression, and ≥10 was found to denote moderate to severe depression (Kroenke et al., 2001). Three group mean differences were evaluated using a one-way analysis of variance (ANOVA; DMI-18 for HAD-D categories, F(2, 94) = 34.61, p < .0001; DMI-18 for PHQ-9 categories, F(2, 127) = 105.59, p < .0001; DMI-10 for HAD-D categories, F(2, 94) = 35.13, p < .0001; DMI-10 for PHQ-9 categories, F(2, 127) = 95.33, p < .0001). The t test was used for two group comparisons (DMI-18 for BDI-PC categories, t(123) = −9.89, p < .0001; DMI-10 for BDI-PC categories, t(123) = −10.13, p < .0001). The nonparametric Jonckheere–Terpstra (JT) test for trend was also implemented for comparing the values of the HADS-D categories (DMI-18, Z = 6.49, p < .0001; DMI-10, Z = 6.47; p < .0001), PHQ-9 (DMI-18, Z = 9.24, p < .0001; DMI-10, Z = 9.00; p < .0001), and the Wilcoxon rank-sum test for the BDI-PC (DMI-18, Z = −7.679, p < .0001; DMI-10, Z = −7.773, p < .0001). In all cases, the DMI scores increased along the ordered categories of the other questionnaires and their values differed significantly among groups.
Criterion validity
The DMI scores of the 167 patients interviewed by the PRIME-MD (gold standard) were used to assess the accuracy and predictive validity of both the versions of the DMI. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were analyzed. The estimates were presented with a 95% CI. To determine the optimal cutoff point for sensitivity and specificity, two receiver operating characteristic (ROC) curves were created, one for the DMI-18 and the other for the DMI-10 (Murphy et al., 1987). The most appropriate cutoff point was considered to be that which minimized the sum of false positives and false negatives (Herrero et al., 2003). For the DMI-18, three different cutoff points, among which the cutoff value of 20 suggested in the original validation study was found, are presented in Table 4. These data suggest that a cutoff point of 15 in the DMI-18 minimizes the sum of false positives and false negatives, correctly classifying 83.8% of the sample and resulting in a PPV of 80% and a NPV of 91%. For the DMI-10, among the three cutoff points evaluated, the value that best balances the sensitivity and specificity is observed to be 9, coinciding with the original study. Therefore, the DMI-10 was found to have an accuracy of 80.8%, with a PPV of 79% and NPV of 83%. These data, together with the psychometric values of the questionnaire, are shown in Table 4. The area under the curve (AUC; Figure 1) represents the ability of the questionnaire to discriminate between cases and noncases. AUC values between 0.5 and 0.7 indicate poor discrimination, those between 0.7 and 0.9 indicate average discrimination, and those greater than 0.9 indicate high discrimination (McDowel & Newell, 1996). Both the versions of the DMI questionnaire demonstrated high discriminatory ability, with the AUC of DMI-18 being 0.90 (95% CI = 0.85-0.94) and of DMI-10 being 0.89 (95% CI = 0.84-0.94).
Validity and Predictive Precision of the DMI-18 and DMI-10 When Compared With PRIME-MD (N = 167).
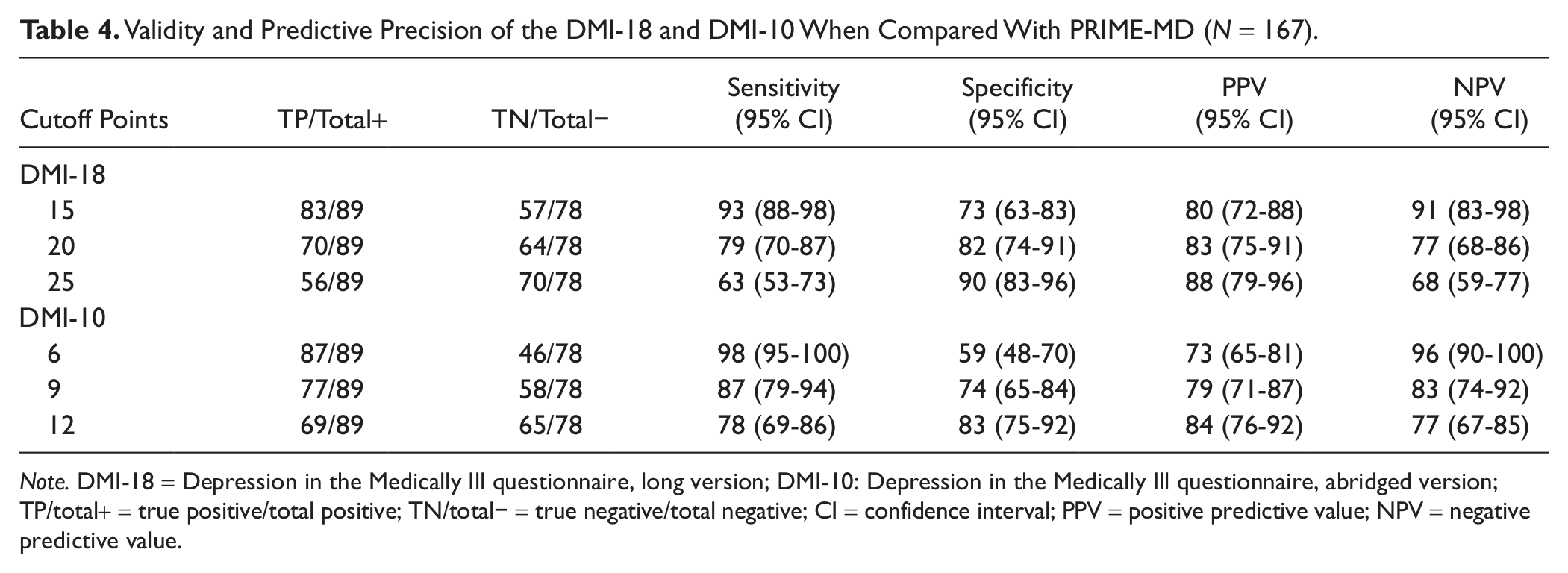
Note. DMI-18 = Depression in the Medically Ill questionnaire, long version; DMI-10: Depression in the Medically Ill questionnaire, abridged version; TP/total+ = true positive/total positive; TN/total− = true negative/total negative; CI = confidence interval; PPV = positive predictive value; NPV = negative predictive value.
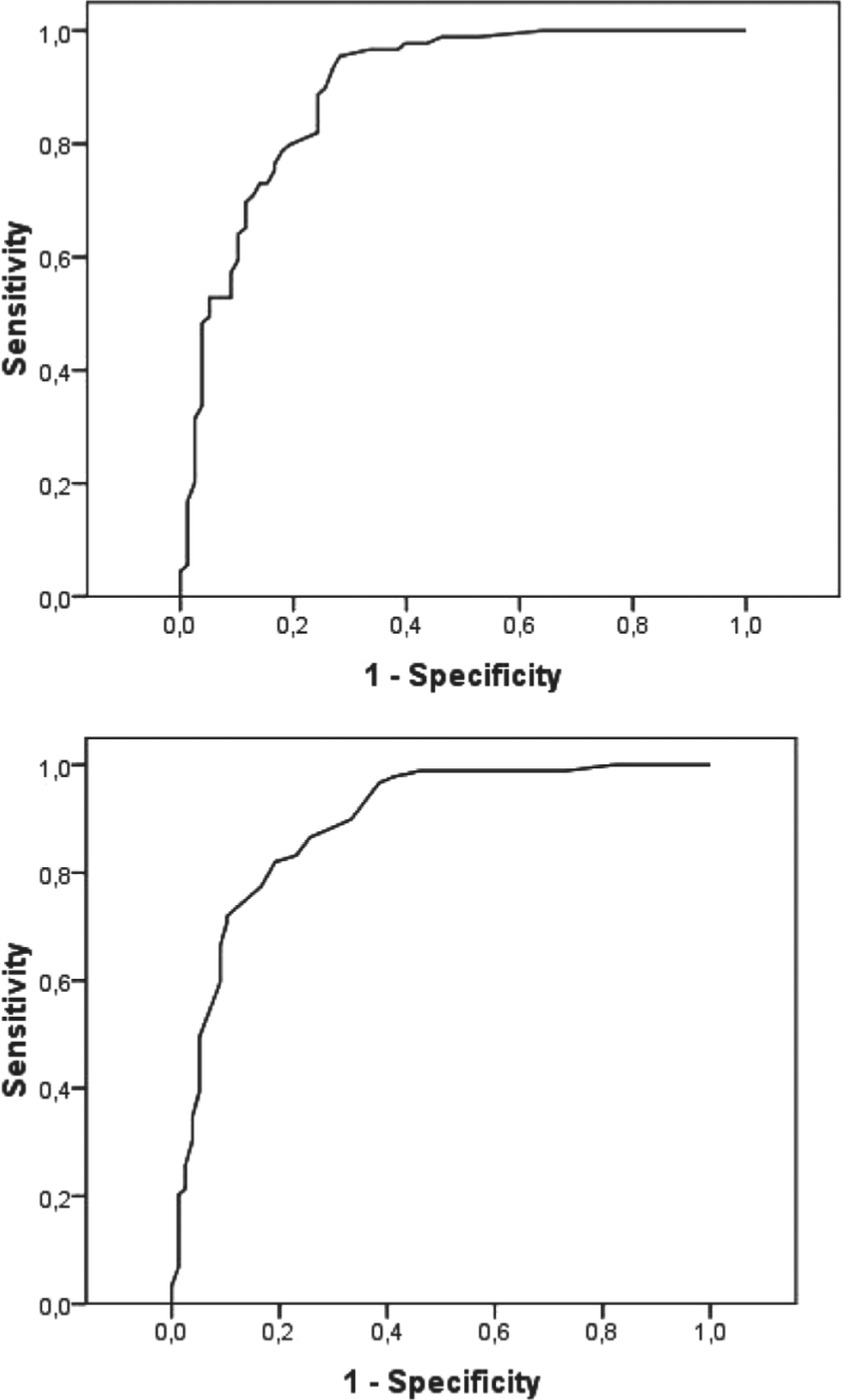
Receiver operating characteristics (ROC) curve graph and area under the curve (AUC) for the performance of the Depression in the Medically Ill (DMI)-18 and DMI-10 questionnaires for detecting depression.
Statistical analyses were carried out using SAS Version 9.2 for Windows. The ROC curves were plotted in SPSS Version 16.
Discussion
Several studies have reported that depression is a frequent comorbid condition, which affects many patients (Herrero et al., 2003; Kilbourne, et al., 2007; Pignone et al., 2002; Sharp & Lipsky, 2002; Watnick, Pei-Li, Demadura, & Ganzini, 2005). Nevertheless, to detect it is not an easy task. In a clinical context, it is important to have effective tools that may allow clinicians, especially family physicians as well as other clinicians apart from psychologists and psychiatrists, to quickly and safely screen and refer those patients for whom depression is suspected to a mental health specialist. This study, with a large sample of patients with different somatic diseases who responded to various mental health questionnaires, considering the final depression diagnosis performed by experimented mental health professionals as a gold standard, attempted to show the value of the DMI-18 and DMI-10. The DMI-18 and the DMI-10 provide an easy-to-use and quick-to-respond tool to assess depression in all kinds of patients.
The Spanish version of the DMI-18 and DMI-10 appeared to be conceptually equivalent to the original. This was supported by the cognitive interviews with the target population and by the high level of concordance between the original version and the one obtained using back-translation.
The internal consistency of the translated DMI-18 and DMI-10 was satisfactory, with a Cronbach’s alpha value and an average interitem correlation coefficient surpassing the cutoff established in the literature (Hair, Anderson, Tatham, & Black, 1998; Nunnally & Bernstein, 1994). This indicates that both the questionnaires can be used reliably for individual patients (McHorney & Tarlov, 1995). Correlations between both the DMI questionnaires and HADS-D, BDI-PC, and PHQ-9 were as expected and indicated satisfactory convergent validity for the two new instruments. Increasing HADS-D, PHQ-9, and BDI-PC scores coincided with increasing DMI scores.
With regard to known-groups validity, both the questionnaires (DMI-18 and DMI-10) detected statistically significant differences between the categories established for the HADS-D, BDI-PC, and PHQ-9 questionnaires to detect depression severity. With respect to criteria validity, both the versions of the translated DMI adequately discriminated between depressed and nondepressed patients. Both the sensitivity (DMI-18: 93%; DMI-10: 87%) and specificity (DMI-18: 73%; DMI-10: 74%) surpassed the minimal acceptable levels (84% for the sensitivity; 72% for the specificity) found by Mulrow et al. (1995) in an analysis of nine widely used instruments for the detection of depression in primary care settings.
In the original DMI study, Parker et al. (2002) recommended using a cutoff point of 20 for the DMI-18 and 9 for the DMI-10. In our study, the best cutoff point for detecting depression was 15 for the DMI-18 and 9 for the DMI-10. The choice of a given cutoff point represents a compromise between sensitivity and specificity. Increasing the cutoff point generally achieves greater specificity, while reducing sensitivity. If our aim is to identify the greatest number of individuals with depression, even at the cost of obtaining a higher number of false positives, we should choose a lower cutoff point. However, if we can provide intervention only to a smaller group of patients with serious disorders, a higher cutoff point would be more appropriate (Herman, 1997).
To evaluate the DMI’s internal structure, the original authors performed an exploratory factor analysis (EFA) of 23 items, from which three factors were extracted, grouped into cognitive, somatic, and anxiety items. To develop the final questionnaire, the authors eliminated the somatic items, after which no structural analysis was performed. Even though no CFA was performed, Parker seemed to hypothesize that all the items load on two factors (cognitive and anxiety); however, even so, at the end, he opted for having just one total score, summing up all the 18 items. We performed both a two-factor and a single-factor CFA on the DMI-18, following Parker’s final hypothesis. Both the hypothetical models turned out to be equally acceptable. However, we decided to retain the one-factor structure, because of the high correlation among the two factors and also for being the most parsimonious and theoretically meaningfully solution. Only the single-factor solution was fitted to the DMI-10. Therefore, our study provides with an additional powerful tool to the validation of the DMI versions employing CFA, which has more advantages than EFA (Batista-Foguet, Coenders, & Alonso, 2004).
The factor analyses results confirmed the unidimensional structure that the original authors seemed to have hypothesized for both the questionnaires (DMI-18 and DMI-10), showing a good fit (Parker et al., 2002).
We agree with the original authors (Parker et al., 2002) in recommending the use of the abridged version of the DMI (DMI-10), given that the analysis shows very little loss of the ability to discriminate depression between the DMI-10 and DMI-18.
A possible limitation of this work is the fact that in the study population, patients with major depression were underrepresented and the majority of the sample was made up of patients who scored near the cutoff for depression. In other words, the study included a number of patients for whom we could be less certain about whether or not they were depressed. Although this allowed us to test the psychometric characteristics of the translated version of the DMI, it interfered with its discriminatory ability and possibly affected the sensitivity and specificity analyses. A second possible limitation is that the interviewed sample mainly comprised women, many of whom reported psychiatric drug use. As this was not a prevalence study and we were not interested in obtaining clinical results, we consider that this limitation has not interfered with the aim of our study. Third, in the interrater reliability study of the collaborating psychiatricians, six of the raters produced moderate levels of κ. Finally, CFA of the DMI-10 was made using the same sample as the CFA of the DMI-18.
Our study was conducted in Spain. All the participants in this study were Spanish-speaking and a Spanish DMI translation was used. Future studies need to test how these tools perform in Spanish-speaking populations from diverse cultural backgrounds and countries.
In conclusion, the Spanish-language long (DMI-18) and short (DMI-10) versions of the DMI questionnaire, which we have translated and tested appear to be useful as depression screening instruments. Given the easiness of use of the DMI-10 and its similar psychometric properties, when compared with the DMI-18, we recommend its use for screening depression in medically ill patients. Its incorporation in a clinical routine may facilitate the diagnosis of depression, ensuring that patients are treated not only for their organic disease but also for their depression if diagnosed.
Footnotes
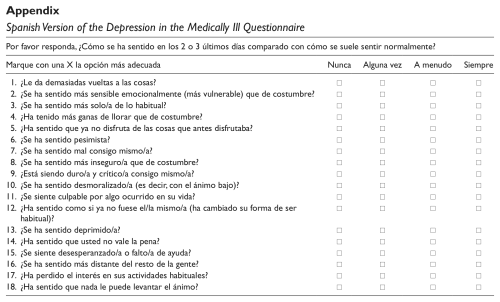
Appendix
Spanish Version of the Depression in the Medically Ill Questionnaire
| Por favor responda, ¿Cómo se ha sentido en los 2 o 3 últimos días comparado con cómo se suele sentir normalmente? | ||||
|---|---|---|---|---|
| Marque con una X la opción más adecuada | Nunca | Alguna vez | A menudo | Siempre |
| 1. ¿Le da demasiadas vueltas a las cosas? | □ | □ | □ | □ |
| 2. ¿Se ha sentido más sensible emocionalmente (más vulnerable) que de costumbre? | □ | □ | □ | □ |
| 3. ¿Se ha sentido más solo/a de lo habitual? | □ | □ | □ | □ |
| 4. ¿Ha tenido más ganas de llorar que de costumbre? | □ | □ | □ | □ |
| 5. ¿Ha sentido que ya no disfruta de las cosas que antes disfrutaba? | □ | □ | □ | □ |
| 6. ¿Se ha sentido pesimista? | □ | □ | □ | □ |
| 7. ¿Se ha sentido mal consigo mismo/a? | □ | □ | □ | □ |
| 8. ¿Se ha sentido más inseguro/a que de costumbre? | □ | □ | □ | □ |
| 9. ¿Está siendo duro/a y crítico/a consigo mismo/a? | □ | □ | □ | □ |
| 10. ¿Se ha sentido desmoralizado/a (es decir, con el ánimo bajo)? | □ | □ | □ | □ |
| 11. ¿Se siente culpable por algo ocurrido en su vida? | □ | □ | □ | □ |
| 12. ¿Ha sentido como si ya no fuese el/la mismo/a (ha cambiado su forma de ser habitual)? | □ | □ | □ | □ |
| 13. ¿Se ha sentido deprimido/a? | □ | □ | □ | □ |
| 14. ¿Ha sentido que usted no vale la pena? | □ | □ | □ | □ |
| 15. ¿Se siente desesperanzado/a o falto/a de ayuda? | □ | □ | □ | □ |
| 16. ¿Se ha sentido más distante del resto de la gente? | □ | □ | □ | □ |
| 17. ¿Ha perdido el interés en sus actividades habituales? | □ | □ | □ | □ |
| 18. ¿Ha sentido que nada le puede levantar el ánimo? | □ | □ | □ | □ |
Acknowledgements
We thank Dr. Parker for his help with this article. We are also very grateful to the participants who voluntarily took part in this study, to the mental health professionals of the Galdakao-Usansolo Hospital (Aranzazu Madrazo, Edurne Aristegui, Mónica Galván, Mª Natividad Silva, Mª Jose Horcajo, Belén Berjano, Patricia Fernández, Javier García, Estela Saez and Elida Belén Grande) for conducting the interviews, and to the services of this hospital that participated in the study (pain unit, obstetrics and gynecology, endocrinology, gastroenterology, neurology, pneumology, and psychiatry units) for helping with patient screening.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article:
The adaptation and validation of the DMI questionnaire was made possible by a grant from the Instituto de Salud Carlos III (file PI06/90421).