
Abstract
This investigation examined the measurement properties of the Three Domains of Disgust Scale (TDDS). Principal components analysis in Study 1 (n = 206) revealed three factors of Pathogen, Sexual, and Moral Disgust that demonstrated excellent reliability, including test–retest over 12 weeks. Confirmatory factor analyses in Study 2 (n = 406) supported the three factors. Supportive evidence for the validity of the Pathogen and Sexual Disgust subscales was found in Study 1 and Study 2 with strong associations with disgust/contamination and weak associations with negative affect. However, the validity of the Moral Disgust subscale was limited. Study 3 (n = 200) showed that the TDDS subscales differentially related to personality traits. Study 4 (n = 47) provided evidence for the validity of the TDDS subscales in relation to multiple indices of disgust/contamination aversion in a select sample. Study 5 (n = 70) further highlighted limitations of the Moral Disgust subscale given the lack of a theoretically consistent association with moral attitudes. Lastly, Study 6 (n = 178) showed that responses on the Moral Disgust scale were more intense when anger was the response option compared with when disgust was the response option. The implications of these findings for the assessment of disgust are discussed.
Disgust is a basic emotion that is recognizable across cultures (Ekman, 1992). It has a universal facial expression (Ekman & Friesen, 1975) and is marked by distinct physiological correlates, including vomiting (Rozin & Fallon, 1987), increased salivation (Angyal, 1941), and activation of the parasympathetic branch of the autonomic nervous system (Levenson, 1992). Insight into the function of disgust can be traced back to Darwin (1872/1965) who noted that disgust “. . . refers to something revolting, primarily in relation to the sense of taste, as actually perceived or vividly imagined; and secondarily to anything which causes a similar feeling, through the sense of smell, touch and even of eyesight” (p. 253). The emphasis on taste has motivated views of disgust as primarily a food rejection emotion (Angyal, 1941). This is consistent with the notion that disgust may function primarily as a guardian of the mouth (Rozin & Fallon, 1987; Rozin, Haidt, & McCauley, 2000) to ward off the oral incorporation of tainted foods. The link between disgust and foods was the foundation for the development of the first measure of disgust, the Disgust and Contamination Sensitivity Questionnaire (Rozin, Fallon, & Mandell, 1984), which assesses attitudes toward certain foods.
There is growing recognition of disgust as an emotion that is experienced in response to stimuli beyond foods. This observation has led to the view that disgust serves a more general protective function and this protective funcmay be observed across multiple domains (Rozin, Haidt, & McCauley, 1993). For example, it has been observed that gore and dismemberment of the human body often elicits disgust across cultures, as does a range of sexual acts, especially incest (Haidt, McCauley, & Rozin, 1994). Social concerns such as interpersonal contamination and sociomoral violations also elicit disgust in many cultures (Haidt, Rozin, McCauley, & Imada, 1997). The heterogeneity of disgust has led to the hypothesis that disgust may have a broader disease-avoidance function that extends beyond the oral incorporation of contaminated foods (Oaten, Stevenson, & Case, 2009). The heterogeneity of disgust has also led to attempts to develop a theoretically informed categorical system for the broad range of disgust elicitors (Rozin & Fallon, 1987).
The most widely accepted classification system of disgust to date was described by Rozin et al. (2000). This system consists of four broad categories of disgust: core, animal-reminder, interpersonal, and moral disgust elicitors. Core disgust is characterized by a real or perceived threat of oral incorporation and a reactive sense of offensiveness that is elicited by certain foods, animals, and body products, particularly those associated with garbage and waste. Animal-reminder disgust elicitors consist of reminders of our own mortality and inherent animalistic nature. Certain sexual practices, injury to the body or violations of its outer envelope, and death are subsumed within this category. Interpersonal disgust functions to protect the soul and social order and is elicited by contact with individuals who are unknown, ill, tainted by disease, misfortune, or immorality. Lastly, moral disgust is characterized by moral violations, which reveal that a person is morally “sick,” “twisted,” or more generally, lacking the normal human motives. Aversion to the four disgust domains may be acquired through learning experiences over time. In fact, recent research has shown that core disgust is acquired early in development (to promote avoidance of pathogens), whereas the other disgust domains are acquired later in development (Stevenson, Oaten, Case, Repacholi, and Wagland, 2010). Oral rejection is the initial organizing principle of disgust reactions and it is this “core disgust” that appears to be transmitted. This basic oral rejection system may have been adapted through evolution to motivate avoidance of other classes of aversion.
The classification system proposed by Rozin and colleagues informed the development of the Disgust Scale (DS; Haidt et al., 1994). The DS is a measure of individual differences in disgust sensitivity across eight domains: (a) food that is spoiled, is culturally unacceptable, or has been fouled in some way; (b) animals that are slimy or live in dirty conditions; (c) body products, including feces, mucus, body odors, and so on; (d) body envelope violations or mutilation of the body; (e) death and dead bodies; (f) sex involving culturally deviant sexual behavior; (g) hygiene, or violations of culturally expected hygiene practices; and (h) sympathetic magic, which involves stimuli without infectious qualities that either resemble contaminants (e.g., feces-shaped candy) or were once in contact with contaminants (e.g., a sweater worn by an ill person). Although the DS is regarded as the gold standard for the assessment of disgust (Olatunji & Sawchuk, 2005), the poor internal consistency of the eight subscales have restricted its broader utility. For example, poor alpha coefficient estimates were found for each of the subscales in two independent samples (ranging from .27 to .63) in the initial DS validation study (Haidt et al., 1994). Numerous other studies have reported rather poor internal consistency estimates for the DS subscales as well (Björklund & Hursti, 2004).
A revision of the DS by Olatunji et al. (2007) removed problematic items resulting in the Disgust Scale–Revised (DS-R), which assesses three domains of disgust: core disgust, animal-reminder disgust, and contamination-based disgust. Importantly, items assessing reactions to sexual behaviors (“I think homosexual activities are immoral”) were removed given evidence that these items did not consistently relate to the other disgust domains. Although sexual acts that are perceived as immoral may elicit disgust, they may also evoke a blend of other emotions, including anger. The implication of this is that sexual disgust may be qualitatively different from other domains of disgust. In addition to identifying three subscales with better internal consistency, the DS-R also indentified subscales that were in line with established theoretical views regarding the classification of disgust elicitors (Rozin et al., 2000). However, the utility of the theoretical disgust classification system posited by Rozin and colleagues, and the assessment of its key aspects by the DS-R have recently been questioned. Tybur, Lieberman, and Griskevicius (2009) contend that the theoretical and empirical support for a distinct animal-reminder disgust domain is tenuous. A second criticism posited by these authors states that it is not clear whether the domains of core, animal-reminder, and contamination disgust are necessarily conceptually distinct. Rather than assessing theoretically distinct aspects of disgust, the three disgust domains may be best explained as sources of disease. Lastly, Tybur and colleagues observed that the DS-R ignores sexual acts and moral transgressions, both of which also elicit disgust.
To address what the authors consider the theoretical and measurement limitations regarding disgust, Tybur et al. (2009) recently proposed an adaptationist model of disgust as well as a scale that is derived from this model. This model, predicated on consideration of the selection pressures that recurred over evolutionary history, proposes three functionally specialized domains of disgust: pathogen disgust, which motivates the avoidance of infectious microorganisms; sexual disgust, which motivates the avoidance of sexual situations that would jeopardize one’s reproductive success; and moral disgust, which motivates the avoidance of social norm violators. In examining these three domains of disgust, Tybur and colleagues developed a new measure of disgust sensitivity. The Three-Domains of Disgust Scale (TDDS; Tybur et al., 2009) is a self- report measure of disgust responding in three domains: moral disgust (e.g., deceiving a friend), sexual disgust (e.g., hearing two strangers having sex) and pathogen disgust (e.g., stepping on dog poop). Internal consistency of the scale was adequate and factor analysis provided support for the three-factor model of the TDDS. Furthermore, the scale showed a distinct pattern of responding across gender and was found to be differentially related to various personality traits, perceived vulnerability to disease, and psychopathic tendencies.
A more recent study replicated the three-factor structure of the TDDS and found that pathogen disgust, but not sexual or moral disgust, predicted women’s preferences for masculinity in male faces (DeBruine, Jones, Tybur, Lieberman, & Griskevicius, 2010). Consistent with an adaptationist view of disgust, this finding may indicate that concerns about disease may function to bias women’s mate preferences toward masculine men. Although the available data on the factor structure and psychometric properties of the TDDS is promising, an independent and comprehensive psychometric evaluation of this measure is needed. Such an evaluation is particularly needed given that the adaptationist view, from which the TDDS is derived, has been proposed as an improvement on current theoretical and measurement models of disgust (Tybur et al., 2009). Given that disgust is now a construct of interest in several research topics within psychology (Olatunji & Sawchuk, 2005), examination of new measures may have important cross-disciplinary implications. Furthermore, data on specific psychometric properties of the TDDS, including test–retest reliability are absent. On the basis of these and other limitations, a series of analyses were conducted across several studies and several methods to examine the factor structure, reliability, validity, and specificity of the TDDS. With regard to specificity, the goal of this investigation is to delineate the extent to which the domains of disgust assessed by the TDDS are reliable/valid and the extent to which they are distinct from each other in relation to various criterion variables. The specificity of the TDDS will be examined across multiple studies that build on one another by using different criterion measures and different modalities of assessment.
Although the factor structure of the TDDS has a theoretical basis and recent research has replicated its factor structure (DeBruine et al., 2010), exploratory factor analysis (EFA) of the TDDS items is largely limited to one investigation (Tybur et al., 2009). In Study 1 of the present investigation, it was predicted that EFA of TDDS items would yield a clearly interpretable three-factor solution (pathogen disgust, sexual disgust, and moral disgust) that would be supported by confirmatory factor analysis (CFA) in Study 2. Importantly, Study 1 reexamines the TDDS factor structure from an exploratory approach to ensure that the initial three-factor structure was not extracted as an artifact of sample characteristics specific to the original sample. The convergent and divergent validity of the TDDS scales is also examined across multiple studies. For example, the available literature points strongly toward associations between obsessive–compulsive disorder (OCD) symptoms and disgust (Olatunji, Cisler, McKay, & Phillips, 2010). Accordingly, it was predicted that correlations between the TDDS scales and OCD-related symptom variables (e.g., contamination fear, excessive washing) would be significant and stronger than correlations between the TDDS scales and unrelated variables (e.g., depression). Study 3 then builds on these findings in examining the relationship between scores on the TDDS scales and the “Big Five” personality dimensions of neuroticism, extraversion, openness, agreeableness, and conscientiousness.
Gender differences on the TDDS scales were also examined across multiple studies and it was predicted that differences, where women score higher than men, would be most pronounced for Sexual Disgust compared with Pathogen Disgust and Moral Disgust. This prediction is predicated on the notion that unlike the other disgust domains, the items on the Sexual Disgust scale (“A stranger of the opposite sex intentionally rubbing your thigh in an elevator”), reflect a substantially greater threat for women as this may be a precursor to sexual coercion or aggression (Tybur, Bryan, Lieberman, Caldwell Hooper, & Merriman, 2011). In Study 4, the association between the TDDS scales and disgust sensitivity, behavioral avoidance, and physiological responding is examined among those high in contamination fear. Based on the findings of Tybur et al. (2009) it is predicted that the Pathogen Disgust scale, but not the other scales, would uniquely predict disgust sensitivity, responding during a behavioral test in a public restroom, and physiological responding during exposure to disgust images. In Study 5, it is predicted that Sexual Disgust and Moral Disgust, but not Pathogen Disgust, would be uniquely associated with various moral attitudes, particularly those marked by the moral foundation of purity/sanctity. Lastly, Study 6 examines the extent to which the emotion of disgust is experienced more intensely than anger in response to the TDDS items. It was predicted that whereas disgust would be experienced more intensely than anger in response to Pathogens and Sexual acts, anger would be experienced more intensely than disgust in response to moral acts.
Study 1 Method: Exploratory Factor Analysis
Participants
A total of 206 participants were recruited from undergraduate courses at a southern university in exchange for research credit. Participants ranged in age from 18 to 26 years (M = 19.42, SD = 1.21) and were predominantly Caucasian (77%) and female (73%). In all, 110 of these participants completed the assessment battery a second time, approximately 12 weeks later. These participants ranged in age from 18 to 26 years (M = 19.73, SD = 1.22) and were predominantly Caucasian (78%) and female (73%).
Measures
TDDS (Tybur et al., 2009) is a 21-item self-report measure of disgust responding in three domains: moral disgust (e.g., deceiving a friend), sexual disgust (e.g., hearing two strangers having sex), and pathogen disgust (e.g., stepping on dog poop). Items are scored on a 7-point Likert-type scale ranging from not at all disgusting (0) to extremely disgusting (6).
The Padua Inventory (PI; Burns, Keortge, Formea, & Sternberger, 1996) Contamination subscale consists of 10 items assessing contamination fear. Items are scored on a 5-point Likert-type scale ranging from 0 (not at all) to 4 (very much). The PI demonstrated adequate internal consistency in the present study (α = .87). The PI was used to assess the convergent validity of the TDDS.
The Center for Epidemiological Studies–Depression Scale (CES-D; Radloff, 1977) is a 20-item measure that assesses the frequency of depressive symptoms experienced during the past week. Items are scored on a 4-point scale ranging from 0 (rarely or none of the time [less than one day]) to 3 (most or all of the time [5 to 7 days]). The CES-D demonstrated good internal consistency in the present study (α = .91). The CES-D was used to assess the divergent validity of the TDDS.
Procedure
Participants completed a questionnaire packet containing the above measures in a classroom setting at two time points approximately 12 weeks apart and received course credit for their participation.
Results
Preliminary analyses
Each of the 21 TDDS items evidenced acceptable corrected item–total correlations (range = .38 to .64) based on the recommended criterion of .30 (Nunnally & Bernstein, 1994). The TDDS total score (M = 73.56, SD = 18.95) was not correlated with age (r = −.13, p = .07) and was significantly higher among women than among men, t(197) = 6.69, p < .001. Means and SDs for the TDDS items are presented in Table 1.
Principal Components Analysis of the Three Domains of Disgust Scale (TDDS): Loadings, Communalities (h2), Means (M), and Standard Deviations (SD) for the Three-Factor Solution
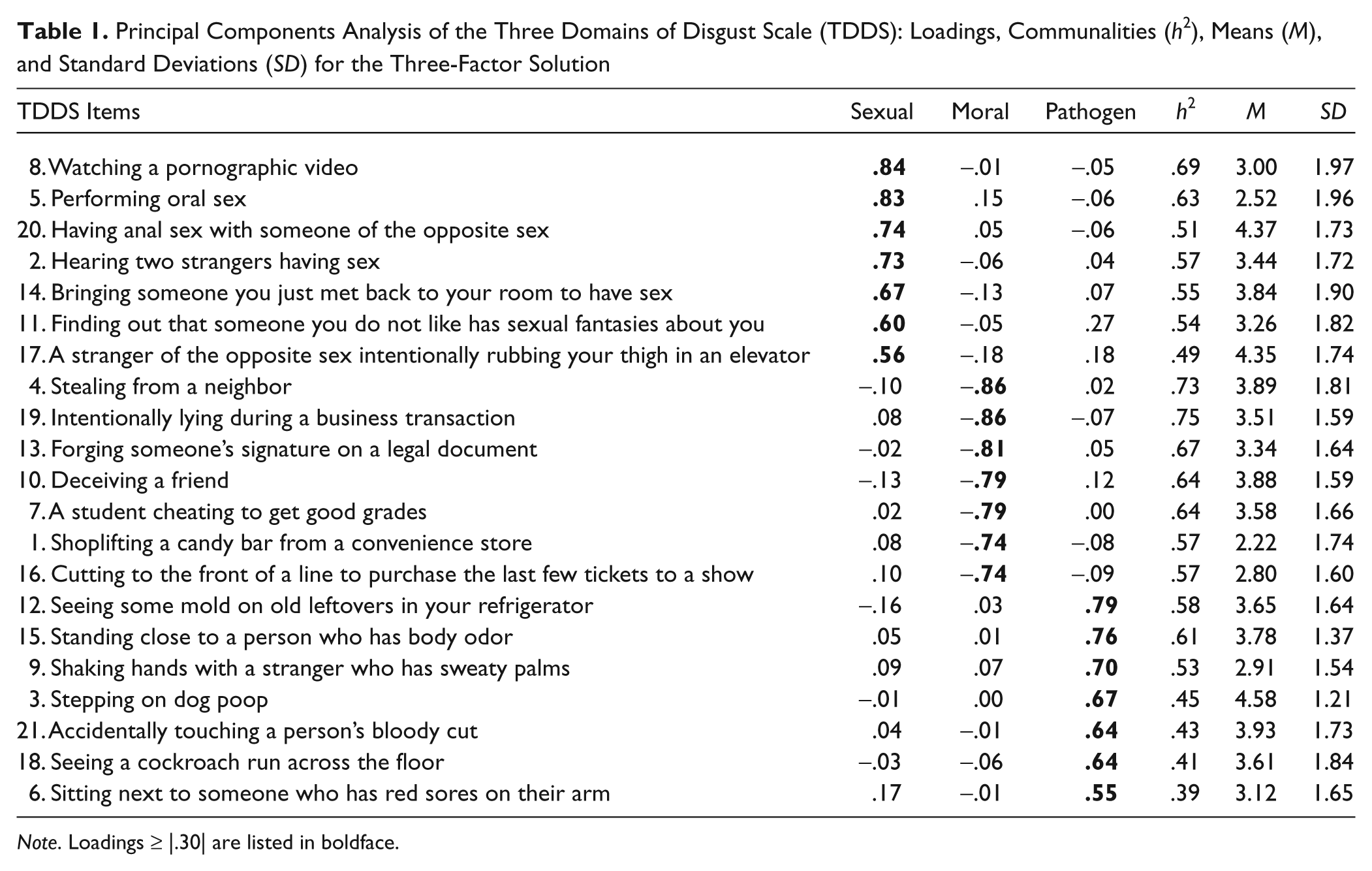
Note. Loadings ≥ |.30| are listed in boldface.
Exploratory factor analysis
Principal components analysis with oblique (oblimin) transformation was used to examine the lower order factor structure of scores on the TDDS. Parallel analyses and factor interpretability were used to determine the number of factors to retain. Parallel analysis is a statistical procedure for determining the break in the scree plot and is one of the most accurate methods for determining the number of factors to retain (Zwick & Velicer, 1986). Parallel analyses were conducted twice, once using the mean eigenvalues and once using the 95th percentile eigenvalues (Longman, Cota, Holden, & Fekken, 1989). The first four eigenvalues of the EFA were 6.03, 3.61, 2.38, and 1.01. However, parallel analysis indicated a clearly interpretable three-component solution for both the mean and 95th percentile eigenvalues (these findings are available on request). Table 1 presents the pattern matrix (i.e., loadings) and communalities for the three-component solution. This solution accounted for a substantial portion of the variance in the TDDS items (57.34%). The three-component solution of the TDDS had good simple structure (Thurstone, 1947). Based on the criterion of |.30| as a salient loading, there were no items with loadings on multiple components.
Component I was composed of seven items with salient loadings (M = 24.77, SD = 9.55). This component was labeled “Sexual Disgust” as each item involves responses to various sexual scenarios. Component II was composed of seven items with salient loadings (M = 23.16, SD = 9.39), each of which assesses various moral transgressions. Accordingly, this component was labeled “Moral Disgust.” Component III was also composed of seven items with salient loadings (M = 25.61, SD = 7.60). This component was labeled “Pathogen Disgust” as each item involves responses to various sources of contagion. The three subscale scores showed adequate internal consistency (αs for Components I, II, and III = .86, .91, and .81, respectively). The Sexual (r = .78), Moral (r = .68), and Pathogen (r = .66) Disgust component scores were highly correlated with the TDDS total score (ps < .001). The Sexual Disgust component score was also significantly correlated with the Moral Disgust (r = .25, p < .001) and Pathogen Disgust (r = .37, p < .001) component scores. The Moral Disgust component score was also significantly correlated with the Pathogen Disgust component score (r = .15, p < .05). Paired sample t tests revealed higher scores on the Pathogen Disgust, t(202) = 3.17, p < .01, and Sexual Disgust, t(201) = 2.07, p < .05, component, compared with the Moral Disgust component. However, scores on the Pathogen Disgust and Sexual Disgust component did not significantly differ from each other, t(203) = 1.15, p = .24.
Gender differences
A 2 (gender: male, female) × 3 (TDDS: pathogen, sex, moral) mixed model analysis of variance (ANOVA) on scores on the three TDDS components revealed a significant main effect of Gender, F(1, 194) = 44.78, p < .001, partial η2 = .18, and TDDS, F(2, 388) = 5.57, p < .01, partial η2 = .03, that was qualified by a significant Gender × TDDS Scale interaction, F(2, 388) = 5.38, p < .01, partial η2 = .02. Examination of the interaction revealed that women reported more Pathogen, t(197) = 3.93, p < .001; Sexual, t(196) = 6.78, p < .001; and Moral, t(195) = 3.21, p < .01, Disgust than men. However, consideration of the effect sizes revealed that the gender difference was larger for Sexual Disgust (Cohen’s d = 0.97) compared with Pathogen (Cohen’s d = 0.56) and Moral (Cohen’s d = 0.46) Disgust (see Figure 1 for mean gender difference on the three TDDS scales).
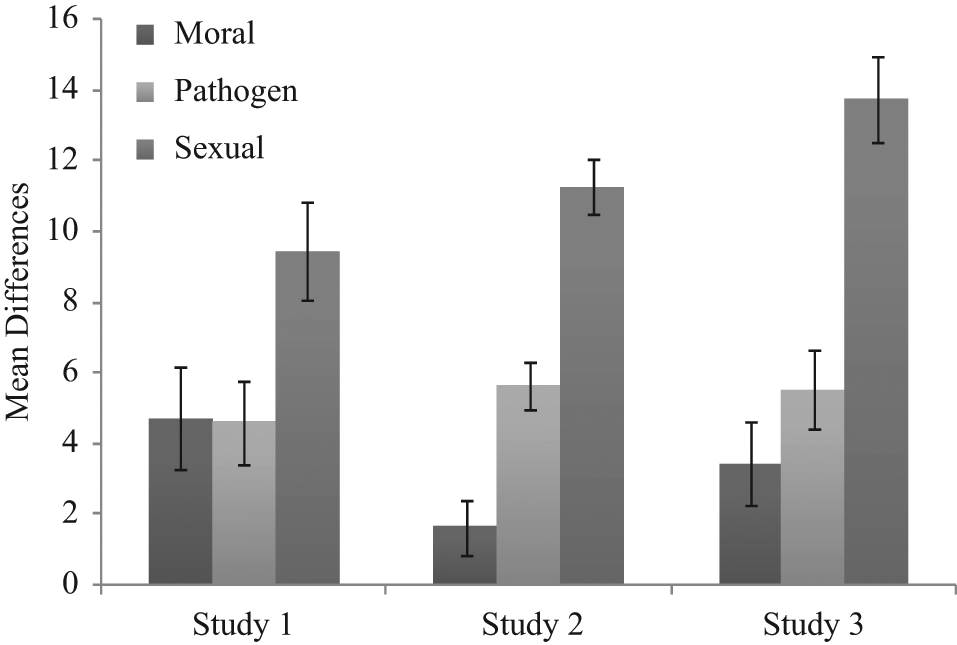
Mean gender differences on the three subscales of the Three Domains of Disgust Scale in Studies 1, 2, and 3
Convergent and divergent validity
To examine the convergent and divergent validity of the three scales of the TDDS, Pearson correlations coefficients were computed between the three scales and a measure of contamination fear (PI) and depression (CES-D). As shown in Table 2, the Pathogen Disgust scale displayed a strong association with contamination and a weaker association with depression (p < .01). The Sexual Disgust scale also displayed a significant, but small, correlation with contamination fear (p < .05) and a nonsignificant correlation with depression. The Moral Disgust scale was not significantly correlated with scores on the PI or CES-D.
Pearson Correlations Between the TDDS, Its Three Scales, and Contamination Fear and Depression
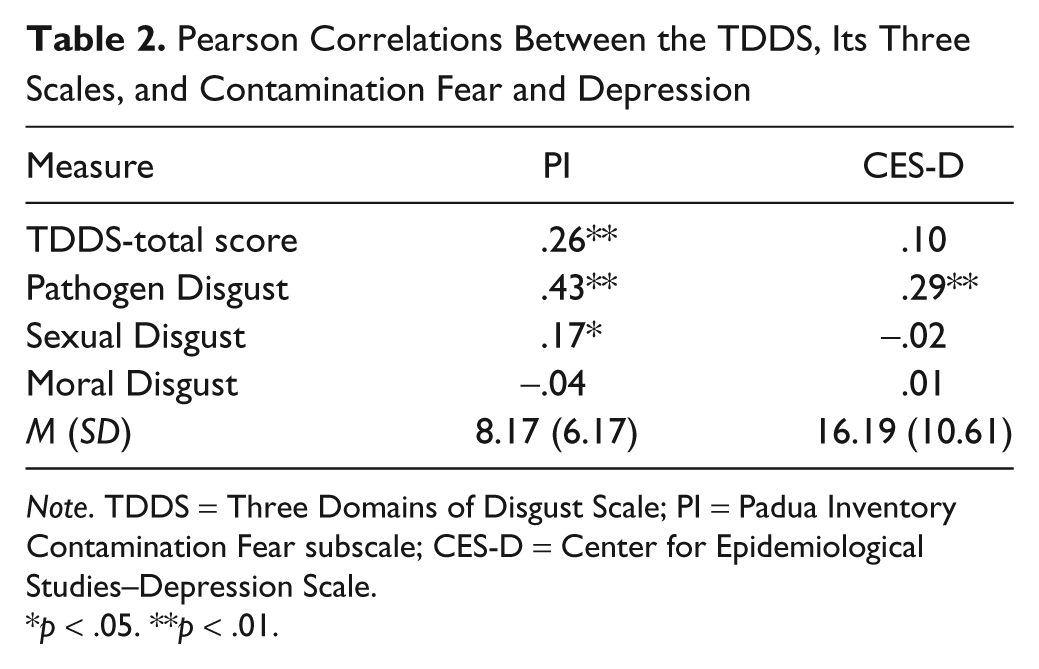
Note. TDDS = Three Domains of Disgust Scale; PI = Padua Inventory Contamination Fear subscale; CES-D = Center for Epidemiological Studies–Depression Scale.
p < .05. **p < .01.
Test–retest reliability
Table 3 shows the mean TDDS total and subscale scores for the test–retest sample (n = 110) at both time points. Those who completed the TDDS at retest did not significantly differ from those who did not complete the TDDS at retest in their baseline TDDS scores. Paired t tests indicated significant reduction in mean scores over the 12-week interval. Pearson correlation coefficients between Time 1 and Time 2 scores are also reported in Table 3. Strong correlations were detected. However, test–retest reliability for only the Pathogen Disgust and the Sexual Disgust scales fell in the range (>.70) of what is typically considered good stability of test scores (Nunnally, 1970). A test of the significance of the difference between two correlation coefficients (Fisher’s z) did show that the test–retest reliability for Pathogen Disgust (z = 3.13, p < .01) and Sexual Disgust (z = 4.01, p < .01) was significantly higher than the test–retest reliability for the Moral Disgust factor. However, the test–retest reliability for the Pathogen Disgust and Sexual Disgust scales did not significantly differ from each other, z = 0.88, p = .37.
Means, Standard Deviations (SD), and Test–Retest Reliability for the Three Domains of Disgust Scale (TDDS) and Its Subscales
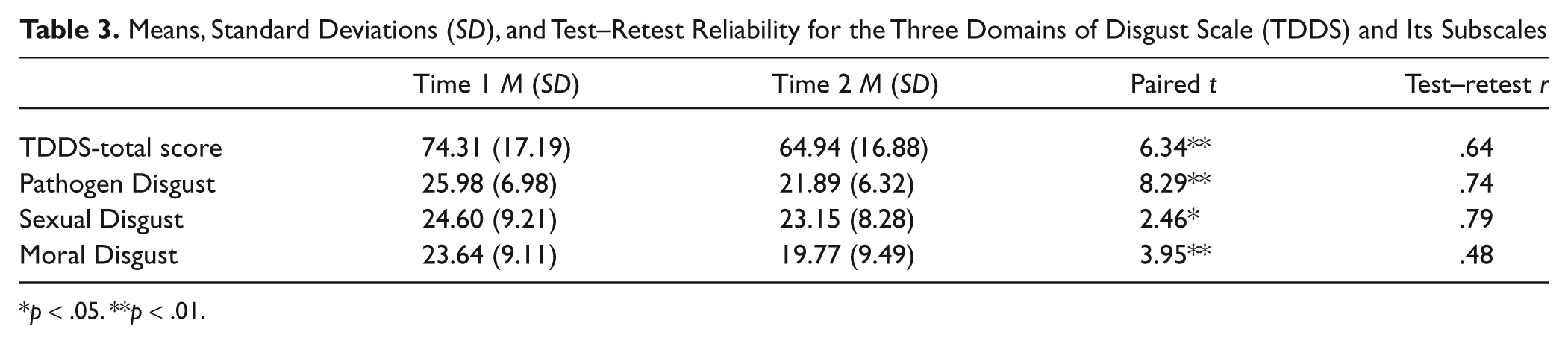
p < .05. **p < .01.
Discussion
The findings from Study 1 suggest that the TDDS is composed of three lower order components (or factors) assessing Pathogen Disgust, Sexual Disgust, and Moral Disgust. The scale scores demonstrated adequate internal consistency and were significantly correlated with each other and the TDDS total score. Scores were generally higher on the Pathogen Disgust and Sexual Disgust scales compared with the Moral Disgust scale. The strongest evidence of convergent validity, divergent validity, and test–retest reliability was found for the Pathogen Disgust and Sexual Disgust factor. The distinctiveness of the three TDDS scales was also observed when examining gender differences. If larger gender differences are observed on some TDDS scales but not others, this may suggest that some TDDS scales are distinct from other TDDS scales. Indeed, larger gender differences were observed with the Sexual Disgust scale relative to the other two scales. This pattern of findings supports the notion that the three disgust scales, particularly Moral Disgust, are distinct from each other. Significant reductions in TDDS scores were observed over the 12-week period suggesting that some habituation to the items may occur as a result of repeat administration.
Study 2 Method: Confirmatory Factor Analysis
Study 1 has important implications for the reliability and validity of the TDDS scores in nonclinical samples. However, the sample size in Study 1 is relatively small and confirmation of the factor structure and further examination of the validity of the TDDS in a larger independent sample would bolster confidence in the factorial validity. Furthermore, only two investigations have used CFA to examine the factor structure of the TDDS, suggesting that further examination of the factor structure of the TDDS is clearly warranted. Accordingly, we elected to conduct CFA of the TDDS items in a second large-scale sample. Study 2 also further examines gender differences on the TDDS scales as well as the convergent and divergent validity of the TDDS scales in relation to measures of disgust, OCD symptoms, and negative affect. The findings of Study 1 revealed that Pathogen Disgust had a strong relation with symptoms of contamination-based OCD and a weaker association with depression. Study 2 builds on these findings by examining the association between the TDDS scales and a broader array of OCD symptoms and indices of negative affect. Importantly, Study 2 uses different measures of similar constructs assessed in Study 1 to ensure that patterns of findings are not measurement specific.
Participants
A total of 406 participants were recruited from undergraduate courses at a southern university in exchange for research credit. Participants ranged in age from 18 to 65 years (M = 19.69, SD = 3.56) and were predominantly Caucasian (88%) and female (61%).
Measures
The TDDS described in Study 1 was one of the measures used in Study 2.
The Disgust Propensity and Sensitivity Scale–Revised (DPSS-R; van Overveld, de Jong, Peters, Cavanagh, & Davey, 2006) is a 16-item measure of disgust propensity (the tendency to experience disgust) and disgust sensitivity (perceived unpleasantness of feelings of disgust). Each subscale of the DPSS-R is composed of eight items that are rated on a 5-point Likert-type scale ranging from 0 (never) to 4 (always). The DPSS-R demonstrated good internal consistency in the present study (α = .90) and was used to assess the convergent validity of the TDDS.
The Obsessive Compulsive Inventory–Revised (OCI-R; Foa et al., 2002) is an 18-item self-report measure of symptoms of OCD over the past month. Items are rated on a 5-point Likert-type scale ranging from 0 (not at all) to 4 (extremely). The OCI-R subscales include washing, checking, obsessive, ordering, neutralizing, and hoarding. The OCI-R demonstrated good internal consistency in the present study (α = .88). Prior research has shown that the clearest relationship between disgust and the various symptoms of OCD is with the washing symptoms (Tolin, Woods, & Abramowitz, 2006). Accordingly, the washing subscale of the OCI-R was used to assess the convergent validity of the TDDS, whereas the remaining subscales were used to assess the divergent validity of the TDDS.
The Depression Anxiety Stress Scale (DASS-21; Lovibond & Lovibond, 2002) is a 21-item measure of symptoms of depression, anxiety, and stress over a 2-week time period. Each subscale of the DASS-21 is composed of seven items that are measured on a 4-point Likert-type scale ranging from 0 (did not apply to me at all) to 3 (applied to me very much, or most of the time). The DASS-21 demonstrated adequate internal consistency in the present study (α = .92) and was used to assess the divergent validity of the TDDS.
Procedure
All data were collected via the Internet at www.surveymonkey.com during the 2009-2010 academic year at a large southern university. All participants were enrolled in an introductory psychology course and were awarded one class credit for their participation in the study.
Data Analytic Overview
Three separate CFAs of the TDDS were conducted using AMOS 18.0 (Arbuckle, 2009): (a) to test a single-factor solution, (b) to test the original three-factor solution, and (c) to test a higher order nested model. All data were analyzed using a covariance matrix and maximum likelihood estimation. The metric was set according to the standards outlined by Kline (2004). One indicator variable from each latent construct with the highest λ value was set to 1 whereas all other indicators were allowed to freely estimate along with latent variances and covariances. Per the recommendations of Brown (2006) and Hu and Bentler (1999), multiple goodness-of-fit indices were used to evaluate model fit including the comparative fit index (CFI), standardized root mean square residual (SRMR), and root mean square error of approximation (RMSEA). CFI values between .90 and .95 are indicative of adequate fit (Bentler, 1990), SRMR values less than .08 suggest good fit (Hu & Bentler, 1999), and RMSEA values less than .08 suggest adequate fit (Browne & Cudeck, 1989; Hu & Bentler, 1999). Given that multiple, nonnested models will be compared, Akaike information criterion (AIC) values are also provided, which allow for model fit comparisons between nonnested models. The absolute values of AIC should not be interpreted. However, AIC values can be compared between two models, with lower values indicating better fit. Additionally, we chose to report the Satorra–Bentler (SB) scaled chi-square (SB-χ2), to correct for multivariate nonnormality (see the “Statistical Assumptions” subsection below).
As per the recommendations of Bagozzi and Yi (1988), several additional statistical tests were used to test model fit, including average variance extracted (AVE), composite reliability (rho), inspection of squared multiple correlations, inspection of all standardized λ values, and inspection of all standardized residual values. AVE was calculated to test the ratio of variance within the manifest variables that is explained by their respective latent construct. If AVE is greater than 0.5, then a greater amount of the variance associated with the manifest variables is explained by the latent construct than measurement error, thus a cutoff of 0.5 was used for AVE (Fornell & Larcker, 1981). Composite reliability (rho) is a test of internal consistency. Rho was presented in addition to Cronbach’s alpha because of the fact that Cronbach’s alpha assumes that all manifest variables within a latent factor are essentially tau-equivalent (equal variance and uncorrelated error; Raykov, 1997b). Given that tau-equivalence is rarely achieved with sample population data and the fact that the present data were in fact congeneric (correlations between items were not equal and SDs varied), composite rho was deemed a good complimentary measure of internal consistency (Raykov, 1997a). Cutoff values for rho are similar to Cronbach’s alpha in that a value ≥0.6 is considered acceptable, although a value ≥0.7 is considered adequate (Bagozzi & Yi, 1988). Square multiple correlation (SMC) is a measure of the ratio of variance associated with an individual manifest variable that is explained by the latent variable and is essentially equivalent to R2 in multiple regression. SMC values ≥0.5 are considered adequate, as this suggests that a greater amount of variance associated with a manifest variable is explained by the latent variable than measurement error (Bagozzi & Yi, 1988; Kline, 2004). Generally, all standardized λ values should be significant and ≥0.6 (Bagozzi & Yi, 1988), although a more liberal cutoff value of 0.4 is generally accepted (Kline, 2004). Last, standardized residuals provide a measure of the degree of discrepancy between the model-implied and sample covariance matrices (Brown, 2006). Standardized residual values are essentially equal to z-scores, therefore, a value ≥ |1.96 | is considered significant (p ≤ .05) and is suggestive of an ill-fitting item (Brown, 2006). However, given that standardized residual values are positively influenced by sample size, a more liberal cutoff of |2.58 |, p ≤ .01 has been suggested (Byrne, 2001).
Results
Statistical assumptions
The Mahalanobis distance (d2) test statistic was used to test for multivariate outliers. Given the large number of significantly multivariate outliers per p1 (with p1 being the probability that any case in the data set would exceed a given d2 value for a case), we used the recommendations of Byrne (2001) and all d2 values were plotted and inspected for cases that were significantly spread from the remaining cases. Inspection of all significant d2 values suggested that five cases had d2 values that were considerably spread from the other cases. These cases were subsequently removed and all further analyses were conducted with the outlier removed data set (n = 401).
Generally, an individual variable is considered to be significantly skewed if its absolute skewness value exceeds 3 (Kline, 2004). The largest skewness value in the present data set was equal to −0.85 (TDDS-4). An individual variable is considered to be significantly kurtotic if its absolute value exceeds 10 (Kline, 2004). The largest kurtosis value in the present data set was equal to 1.38 (TDDS-8). These data support univariate normality within the TDDS items. Multivariate normality was assessed with Mardia’s multivariate kurtosis coefficient. Mardia’s coefficient was equal to 20.14 in the present sample—a value that is well above the accepted cutoff value of 5 (Byrne, 2001)—therefore, data were considered mulitivariate nonnormal.
We first tested a single-factor model (all 21 items loaded onto one factor) to determine if the data were more parsimoniously explained by a unitary construct of disgust. As was expected, SB chi-square of the single-factor model was significant, SB-χ2(189) = 1684.64, p < .001. Additionally, alternative fit indices suggested that the single-factor solution did not adequately model the sample data: CFI = .546, RMSEA = .157 (90% confidence interval [CI] = .151, .163), SRMR = .147, and AIC = 2127.89. Additionally, each of the manifest variables did not adequately load onto the latent factor (range of standardized β = .30 to .76). These results suggest that a single-factor model does not adequately fit the data.
The SB chi-square for the three-factor model (see Figure 2) was significant, SB-χ2(186) = 501.97, p < .001. Alternative fit indices were all within acceptable parameters: CFI = .902, RMSEA = .073 (90% CI = .067, .080), SRMR = .052, and AIC = 677.27. These findings suggest that the three-factor model fits the data more accurately than the single-factor model. AVE was acceptable for the Moral and Sexual factors but not Pathogen: Moral = .514, Sexual = .562, and Pathogen = .447. Standardized composite rho values were greater than .7 for all latent variables: TDDS-M (ρ) = .89, TDDS-S (ρ) = .91, TDDS-P (ρ) = .87. Cronbach’s alpha values were also greater than .7 for all latent variables: TDDS-M (α) = .88, TDDS-S (α) = .90, TDDS-P (α) = .85, thus suggesting adequate internal consistency. Fornell and Larcker (1981) tests of discriminant validity indicated that the AVE within each off the three TDDS latent factors was greater than the covariance between the latent factors themselves, thus suggesting adequate discriminant validity between the TDDS factors. Moreover, zero-order correlations between each of the latent factors were moderate (r = .32 to .60), thus providing further support for discriminant validity between the TDDS factors.
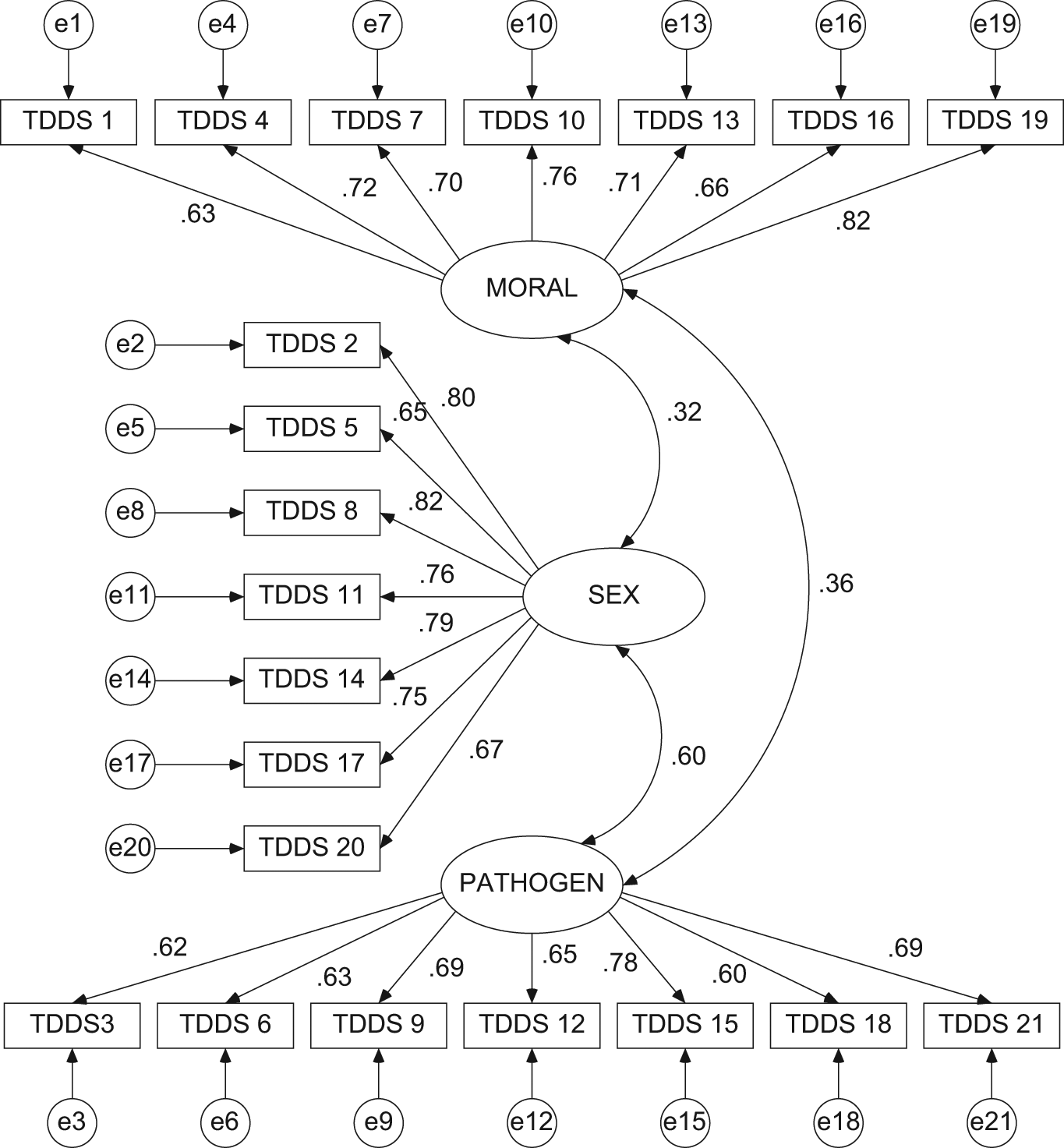
Three-factor structure of the Three Domains of Disgust Scale (TDDS) with regression weights
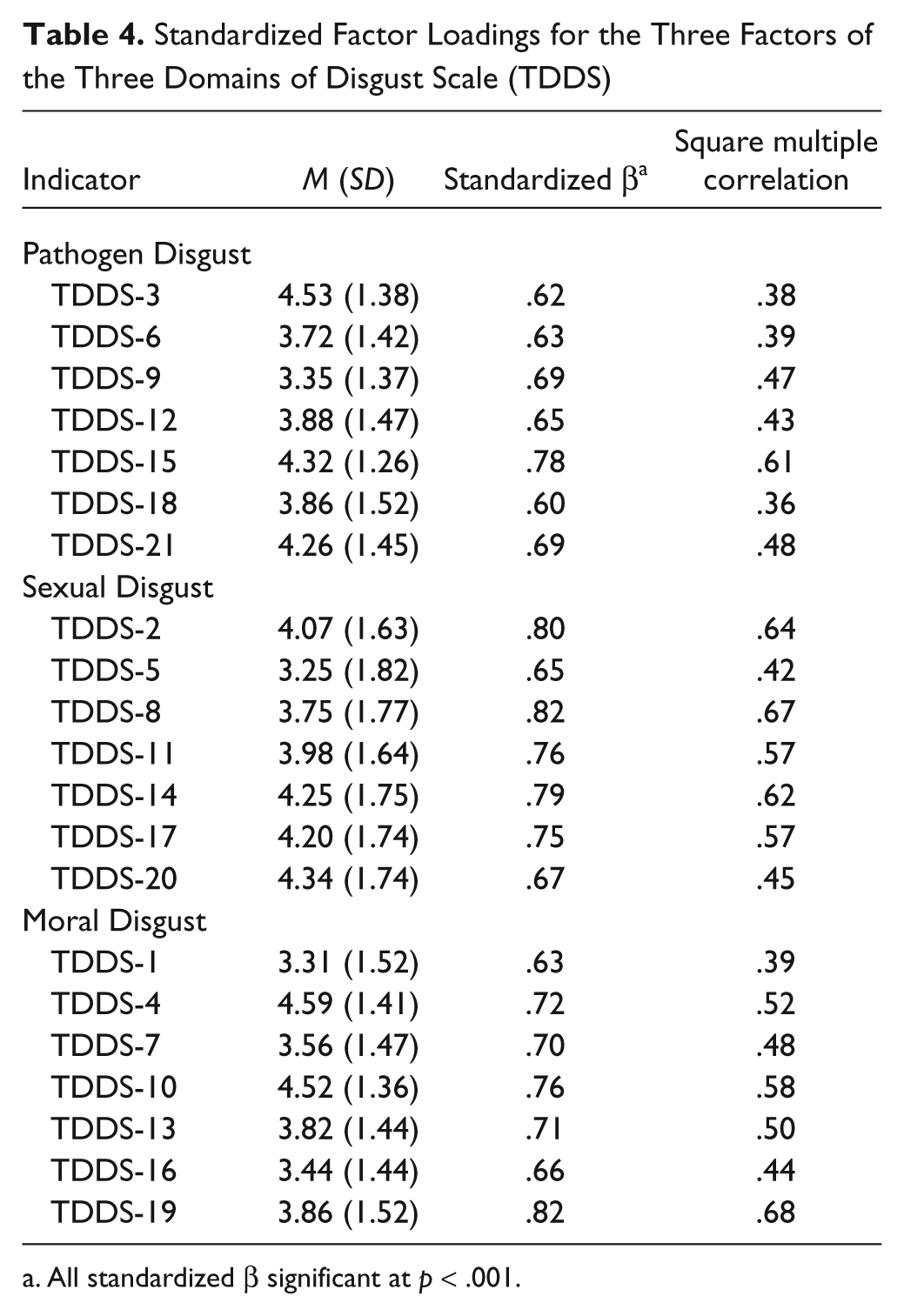
All standardized λ values were greater than .60 and significant (p ≤ .001; see Table 4); however, not all SMC values were ≥0.5 (R2 = .36 to .67; see Table 4). Inspection of the standardized residual covariance matrix indicated that several TDDS items were sources of moderate model strain (z ≥ |1.96 |, p ≤ .05). However, only TDDS Item 5 (“performing oral sex”) exceeded the cutoff value of z ≥ |2.58 |. TDDS Item 5 had several standardized residual covariance values less than −1.96 with the largest value being −3.27 (Items 5 and 16: “cutting to the front of the line to purchase the last few tickets to a show”). These data suggest that the specified model underestimated the zero-order relations between TDDS Item 5 and other manifest variables. The fact that Item 5 shared significant standardized residual covariance values with items from all three factors of the TDDS and especially the Moral Disgust factor suggest that the model does not adequately fit the data for Item 5.
Standardized Factor Loadings for the Three Factors of the Three Domains of Disgust Scale (TDDS)
All standardized β significant at p < .001.
Last, we tested a second-order CFA model to determine whether a single higher order factor accounted for the interrelations between the three first-order factors. The metric was set in the same manner as the CFA of the three-factor solution, except the regression weight of the path between Pathogen and the higher order “Disgust” factor which was also set to 1. As was expected, the SB chi-square of the second-order model was significant, SB-χ2(186) = 501.97, p < .001, whereas all alternative fit indices suggested adequate fit: CFI = .902, RMSEA = .073 (90% CI = .067, .080), SRMR = .052, and AIC = 677.27. Each of the first-order factors adequately loaded onto the higher order factor (range of standardized β = .44 to .81). Inspection of the standardized residual covariance matrix indicated that several TDDS items were significant sources of model strain (i.e., z > 1.96, p ≤ .05). Once again, the most concentrated source of model strain was localized around Item 5. The second-order factor accounted for varying amounts of variance in the first-order factors (R2s: Moral = .19, Sexual = .54, Pathogen = .66). These results indicate that the second-order factor adequately explains the covariance between the three first-order factors, although the use of a total score may not be warranted given that factor loadings of the first-order factors are not equivalent.
Gender differences
To replicate the pattern of gender differences found in Study 1, a 2 (gender: male, female) × 3 (TDDS: pathogen, sex, moral) mixed model ANOVA on scores on the three TDDS scales revealed only a significant main effect of Gender, F(1, 399) = 126.27, p < .001, partial η2 = .24, and a significant Gender × TDDS Scale interaction, F(2, 798) = 60.00, p < .001, partial η2 = .13. Examination of the interaction revealed that women reported more Pathogen, t(399) = 8.35, p < .001; Sexual, t(399) = 14.16, p < .001; and Moral, t(399) = 2.09, p < .05, Disgust than men. However, consideration of the effect sizes revealed that the gender difference was larger for Sexual Disgust (Cohen’s d = 1.41) compared with Pathogen (Cohen’s d = 0.83) and Moral (Cohen’s d = 0.20) Disgust (see Figure 1 for mean gender difference in the three TDDS scales).
Convergent and divergent validity
As shown in Table 5, the Pathogen and Sexual Disgust scales were moderately correlated with disgust propensity and disgust sensitivity whereas the Moral Disgust scale had near-zero correlations with disgust propensity and disgust sensitivity. The Pathogen and Sexual Disgust scales were also moderately correlated with the OCI-R washing subscale whereas the correlation between the Moral Disgust scale and the OCI-R washing subscale was near zero. Fisher’s z tests of differences between correlation coefficients indicated that the correlations between the OCI-R washing subscale and the Pathogen (r = .22) and Sexual (r = .13) Disgust scales were not significantly different, z = 1.31, p = .19. The Moral and Sexual Disgust scales were not significantly related to any other OCI-R subscales (rs = −.02 to .07), the Pathogen Disgust scale was significantly correlated with OCI-R Ordering (r = .17, p ≤ .001) and Checking (r = .10, p ≤ .05) subscales. All three of the TDDS subscales had minimal correlations with each of the three DASS subscales. The Sexual Disgust scale was significantly negatively correlated with the DASS-Depression subscale and the Pathogen Disgust scale was significantly positively correlated with the DASS-Stress subscale.
Pearson Correlations Between Subscales of the TDDS and Measures of Disgust, Obsessive–Compulsive Symptoms, and Distress
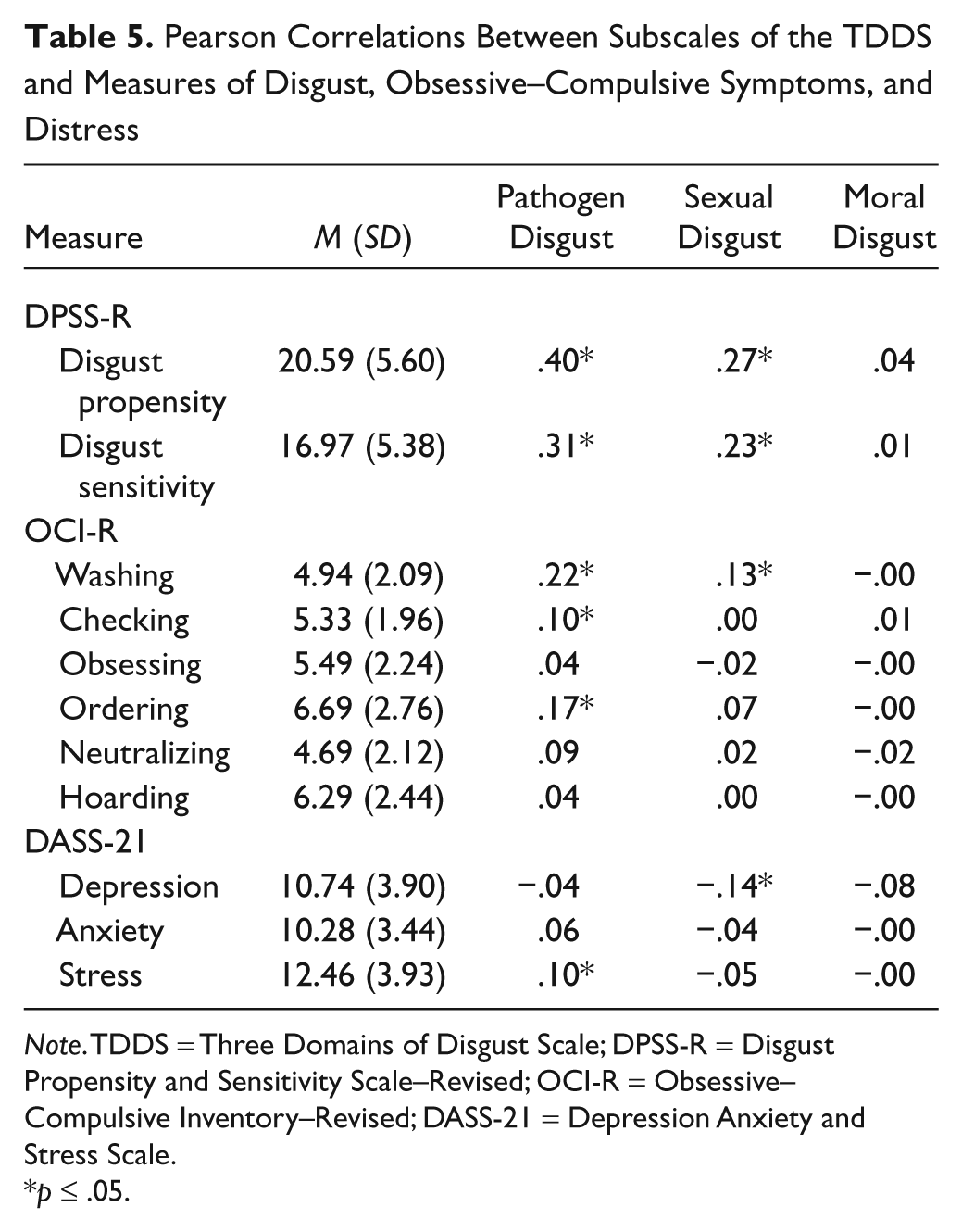
Note. TDDS = Three Domains of Disgust Scale; DPSS-R = Disgust Propensity and Sensitivity Scale–Revised; OCI-R = Obsessive–Compulsive Inventory–Revised; DASS-21 = Depression Anxiety and Stress Scale.
p ≤ .05.
Discussion
CFA provided support for the three-factor model of the TDDS. In contrast, a single-factor model of the TDDS that depicts disgust as a unitary construct did not yield an acceptable fit to the data. However, Moral Disgust accounted for the least percentage variance with respect to the variance accounted for by the three factors. Although support was found for a model where a higher order factor accounted for the interrelations between the three first-order factors, the variance accounted for by the three factors suggests that Moral Disgust may be relatively distinct from the other two factors. The data also suggest that use of a TDDS total score may not be warranted given that factor loadings of the first-order factors were not equivalent. The Pathogen and Sexual Disgust scales were modestly correlated with related measures of disgust and washing whereas the Moral Disgust scale was not. This is consistent with Study 1, which suggests that the three scales are relatively distinct from each other, particularly Moral Disgust. The three TDDS scales also display small to nonsignificant correlations with measures of depression, anxiety, and stress. This finding suggests that patterns of scoring on the TDDS may have little relevance for general psychopathology. Consistent with Study 1, larger gender differences were observed with the Sexual Disgust factor relative to the other two scales.
Study 3 Method: Further Examination of Convergent and Divergent Validity
The overall pattern of findings observed in Study 2 suggests that the TDDS scales have very minimal associations with specific measures of psychopathology, including depression, anxiety, and stress. This is inconsistent with prior research using other measures of disgust that has revealed more robust associations with specific measures of psychopathology (Olatunji et al., 2007). This relative absence of a more meaningful association with specific measures of psychopathology in Study 2 highlights the need for further examination of criterion variables that do converge with the TDDS scales in a more meaningful way. Accordingly, we elected to further examine the validity of scores on the TDDS scales in another independent sample. Rather than using specific measures of psychopathology, more robust evidence of convergent validity may be revealed when examining the association between the TDDS scales and more broad measures of personality. Specifically, the extent to which scores on the TDDS scales relate to individual differences in personality as indexed by the “Big Five” personality dimensions of neuroticism, extraversion, openness, agreeableness, and conscientiousness was examined. It was predicted that Pathogen Disgust (but not necessarily Sexual or Moral Disgust) would be positively correlated with neuroticism. Due to proposed functional differences, it was also predicted that the remaining TDDS would show unique patterns of relations with Big Five personality traits. Study 3 also attempts to replicate the pattern of gender differences on the TDDS scales observed in the prior studies.
Participants
A total of 200 participants were recruited from undergraduate courses at a large southern university in exchange for research credit. Participants ranged in age from 18 to 28 years (M = 19.59, SD = 1.44) and were primarily Caucasian (88%) and female (61%).
Materials
The TDDS described in Study 1 was one of the measures used in Study 3.
The Big Five Inventory (BFI; John & Srivastava, 1999) is a 44-item measure that is commonly used to assess the “Big Five” personality dimensions: neuroticism, extraversion, openness, agreeableness, and conscientiousness. The answer format is a 5-point Likert-type scale ranging from 1 (disagree strongly) to 5 (agree strongly). The BFI demonstrated adequate internal consistency in the present study (α = .75) and was used to assess the validity of the TDDS. It predicted that distinct correlations will be observed between the Pathogen Disgust scale and neuroticism. Given the functional specificity of each of the domains of the TDDS, it was predicted that the domains should show a distinct pattern of relations with Big Five dimensions. As Tybur et al. (2009) observed for example, agreeableness is a social attribute that may be associated with the Sexual Disgust and Moral Disgust scales but not the Pathogen Disgust scale.
Procedure
Participants completed the paper-and-pencil measures in a classroom format.
Results
TDDS correlates
Table 6 shows that the Big Five traits were differentially correlated to the three TDDS scales. The Pathogen Disgust scale was positively related to conscientiousness (p < .05), whereas the Sexual Disgust scale and the Moral Disgust scale were positively related to agreeableness and conscientiousness (ps < .01). However, the magnitude of the correlations between the three TDDS scales and the Big Five traits were modest (Table 6).
Pearson Correlations Between Subscales of the TDDS and Measures of Personality
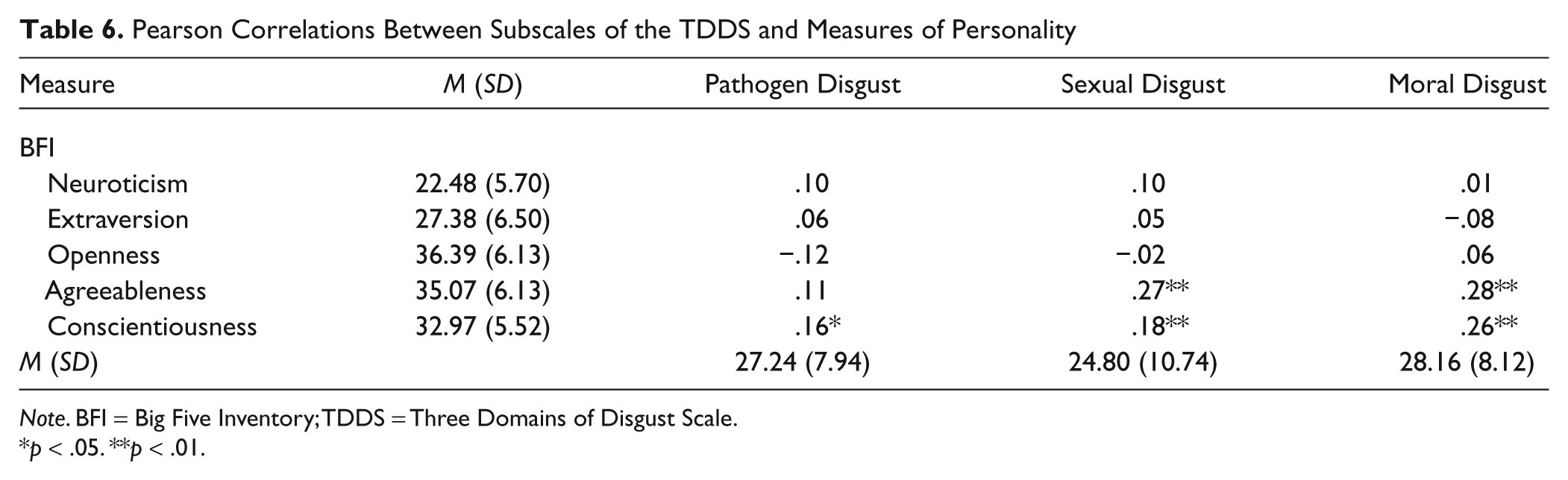
Note. BFI = Big Five Inventory; TDDS = Three Domains of Disgust Scale.
p < .05. **p < .01.
Gender differences
To replicate the pattern of gender differences in Study 1 and Study 2, a 2 (gender: male, female) × 3 (TDDS Scale: pathogen, sex, moral) mixed model ANOVA on scores on the three TDDS scales revealed a significant main effect of Gender, F(1, 191) = 71.92, p < .001, partial η2 = .27, and TDDS Scale, F(2, 382) = 25.01, p < .001, partial η2 = .12, that was qualified by a significant Gender × TDDS Scale interaction, F(2, 382) = 35.45, p < .001, partial η2 = .15. Examination of the interaction revealed that women reported more Pathogen, t(195) = 5.05, p < .001; Sexual, t(196) = 11.25, p < .001; and Moral, t(195) = 2.94, p < .01, Disgust than men. However, consideration of the effect sizes revealed that the gender difference was larger for Sexual Disgust (Cohen’s d = 1.60) compared with Pathogen (Cohen’s d = 0.72) and Moral (Cohen’s d = 0.42) Disgust (see Figure 1 for mean gender difference in the three TDDS scales).
Discussion
This investigation replicates the earlier findings regarding gender differences in the three scales of the TDDS such that larger gender differences were observed with the Sexual Disgust scale relative to the other two scales. Although prior research has found an association between measures of disgust sensitivity and neuroticism (Haidt et al., 1994; Olatunji, Haidt, McKay, & David, 2008), neuroticism was not found to be associated with any of the three scales of the TDDS. However, higher scores on the Sexual Disgust and the Moral Disgust scales were associated with more agreeableness and conscientiousness. The Pathogen Disgust scale was largely unrelated to measures of personality and only mildly associated with conscientiousness. These findings further highlight the distinctiveness of the three TDDS scales. Importantly, the magnitude of the association between the TDDS scales and personality traits were modest in the unselected sample.
Study 4 Method: Self-Report, Behavioral, and Physiological Correlates of the TDDS Scales
Study 4 examines the psychometric properties of the TDDS using a multimethod approach of assessment. Specifically, the association between the three TDDS scales and self-reported disgust proneness, behavioral avoidance, and physiological responding in a select sample of those high in contamination fear was examined. It has been proposed that the fear of contamination may be marked by dysregulated disgust processing (Olatunji, Sawchuk, Lohr, & de Jong, 2004). Examination of the TDDS in a sample of those high in contamination fear may then reveal more robust psychometric properties than those observed in the prior investigations with an unselected sample. Given that those high in contamination fear are especially prone to experiencing disgust (Olatunji et al., 2004), disgust and contamination may be more strongly associated in memory, perhaps through various learning modalities, among such individuals. The tight coupling of disgust and contamination in this sample may yield stronger associations between the TDDS scales and self-reported disgust, behavioral avoidance of contamination, and physiological responding during exposure to disgust content.
Participants
Undergraduate students were screened (N = 546) using the Contamination and Washing subscale of PI (Burns et al., 1996), to identify potential participants high in contamination concerns. Individuals who scored 1 SD above the mean on the PI contamination subscale were invited to participate in the present study, of which 47 completed participation (mean age = 19.31 years, SD = 1.18; Caucasian = 73%; female = 57%). Participants’ mean score on the PI was 19.27 (3.80) which is higher than the mean reported by Burns et al. (1996) for patients with OCD (13.87).
Measures
The TDDS and the PI described in Study 1 were used.
The DS-R (Olatunji et al., 2007) is a 25-item questionnaire assessing sensitivity to core, animal-reminder, and contamination disgust on a 5-point Likert-type scale. Thirteen of its items are rated on a scale from 0 (strongly disagree) to 4 (strongly agree). The other 12 items are rated on a scale from 0 (not disgusting at all) to 4 (extremely disgusting). The DS-R had an α coefficient of .84 in the present study.
Behavioral Avoidance Task
The behavioral avoidance task (BAT) took place in a standard-size public restroom located in the psychology building where participants were asked to engage in five steps of increasing perceived contamination risk. Participants were asked if they were willing to touch (a) the inside of the sink, (b) the inside of the trash can, (c) the toilet seat, (d) the rim of the toilet, and (e) the inside of the toilet bowl. Immediately after each step of the task, anxiety and disgust ratings on an 11-point scale (0 = no anxiety/disgust at all to 10 = severe anxiety/disgust) were obtained.
Image Viewing Task
The image viewing task consisted of five disgust and five neutral expressions from the Karolinska Directed Emotional Faces (Lundqvist, Flykt, & Öhman, 1998) and five disgust (i.e., rotting foods) and five neutral (i.e., inanimate objects) images from International Affective Picture System (Lang, Bradley, & Cuthbert, 2005). The 20 images were randomly presented individually for 4,000 milliseconds each. During the period of image presentation, participants’ Galvanic skin response (GSR) was measured. GSR was digitally recorded using BIOPAC GSR100C module for MP100. Ag–AgCl electrodes were used and attached with Velcro straps (BIOPAC Systems, Goleta, CA) to the phalanges of the second and third digits on the hand which the participants were not using to respond. A saline-based gel was used as a conductive electrolyte. Skin conductance was monitored at 200 Hz and was stored offline for analysis, using AcqKnowledge software (BIOPAC Systems, Goleta, CA). GSR levels were visually inspected and corrected for artifacts before they were analyzed statistically. Change scores were used to assess physiological responsiveness by subtracting GSR values for a baseline period (4 seconds before exposure to the images) from the GSR values for each image.
After each presentation of an image, participants were asked to rate how pleasant the image made them feel on a scale of 0 (most unpleasant) to 8 (most pleasant). The disgust images (M = 1.74, SD = 0.25) were rated significantly more unpleasant than the disgust faces (M = 3.00, SD = 0.12), neutral images (M = 4.37, SD = 0.18), and neutral faces (M = 3.98, SD = 0.16), ps < .01. Disgust faces were rated significantly more unpleasant than neutral images and neutral faces (p < .01). Lastly, neutral faces were rated significantly more unpleasant than neutral images (p < .01).
Procedure
Participants first completed the self-report measures and the BAT. Participants then completed the image viewing task where physiological responding was assessed.
Results
TDDS scales and disgust domains of the DS-R
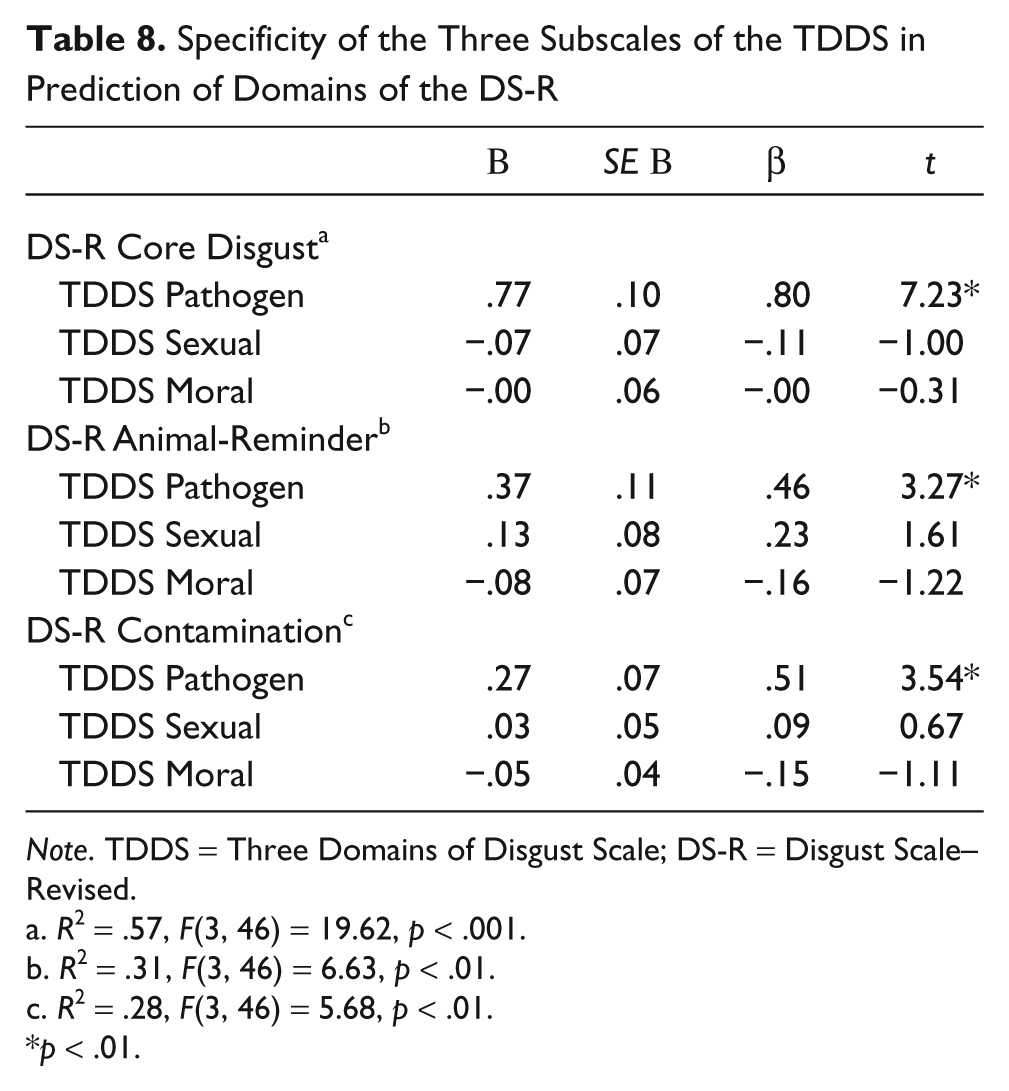
As shown in Table 7, the Pathogen Disgust scale of the TDDS was significantly associated with the Core, Animal-Reminder, and Contamination Disgust subscales of the DS-R (ps < .01). The Sexual Disgust factor of the TDDS was correlated with only the Animal-Reminder subscale of the DS-R (p < .05) and the Moral Disgust scale was not related to any of the DS-R subscales. Three hierarchical multiple regression analyses were then conducted to examine the specific contribution of the three TDDS scales in predicting the disgust domains of the DS-R. As shown in Table 8, only Pathogen Disgust explained significant variance in each of the three disgust domains of the DS-R.
Self-Report, Behavioral, and Psychophysiological Correlates of the Subscales of the TDDS

Note. TDDS = Three Domains of Disgust Scale; DS-R = Disgust Scale–Revised; BAT = Behavioral Avoidance Task.
p < .05. **p < .01.
Specificity of the Three Subscales of the TDDS in Prediction of Domains of the DS-R
Note. TDDS = Three Domains of Disgust Scale; DS-R = Disgust Scale–Revised.
R2 = .57, F(3, 46) = 19.62, p < .001.
R2 = .31, F(3, 46) = 6.63, p < .01.
R2 = .28, F(3, 46) = 5.68, p < .01.
p < .01.
TDDS scales, behavioral avoidance, and physiological responding
As shown in Table 7, none of the TDDS scales were associated with the number of steps taken on the BAT. However, the Pathogen Disgust scale of the TDDS was significantly associated with anxiety and disgust responding to the BAT (ps < .01), whereas the Sexual Disgust and Moral Disgust scales of the TDDS was not. Regarding psychophysiology, a significant association was observed only between the Pathogen Disgust scale and GSR during viewing of the disgust images (p < .05).
Discussion
These findings show that the Pathogen Disgust scale, but not the other scales, uniquely predicted disgust sensitivity to core, animal-reminder, and contamination stimuli in a select sample of individuals high in contamination fear. These findings suggest that a pathogen prevention mechanism may be a common process to the three disgust domains of the DS-R in this sample. However, such definitive inferences may be premature given that no test of differential validity was conducted in the present study. The Pathogen Disgust scale, but not the Sexual or Moral Disgust scales, of the TDDS also predicted anxiety and disgust responding during a behavioral test in a public restroom and physiological responding during exposure to disgust images. These findings suggest that the Pathogen Disgust scale is relatively distinct from the Sexual and Moral Disgust scales and may be a closer index of the original nature and function of disgust as a contagion prevention emotion.
Study 5 Method: Disgust, Morality, and the TDDS Scales
Although these findings of Study 4 further support the discriminant validity of the three TDDS scales, the unique correlates of the Sexual and Moral Disgust scales remain unclear. This is especially important given that the Sexual and Moral Disgust scales represent the more novel contributions to the literature on the assessment of disgust as currently available measures (DS-R) are argued to be limited by the exclusive assessment of Pathogen Disgust (Tybur et al., 2009). Theoretical models suggest that disgust toward some sexual acts may derive from moral scruples (Olatunji, 2008) and disgust expressed toward moral transgressions derive largely from internalization of purity and sanctity as core values (Graham, Haidt, & Nosek, 2009). Therefore, the next investigation further examines the association between the three TDDS scales, moral attitudes, and domains of disgust assessed by the DS-R.
Participants
A total of 70 participants were recruited from undergraduate courses at a southern university in exchange for research credit. Participants ranged in age from 18 to 26 years (M = 19.42, SD = 1.21) and were predominantly Caucasian (70%) and female (87%).
Measures
The TDDS described in Study 1 and the DS-R described in Study 4 were used.
The Moral Foundations Questionnaire (MFQ; Graham et al., 2009) is a 30-item measure of moral attitudes on a 6-point Likert-type scale across domains of harm/care (underlies virtues of kindness, gentleness, and nurturance), fairness/reciprocity (generates ideas of justice, rights, and autonomy), in-group/loyalty (underlies virtues of patriotism and self-sacrifice for the group), authority/respect (underlies virtues of leadership and followership, including deference to legitimate authority and respect for traditions), and purity/sanctity (underlies the widespread idea that the body is a temple which can be desecrated by immoral activities and contaminants). The MFQ demonstrated adequate internal consistency in the present study (α = .84) and was used to assess the convergent and divergent validity of the TDDS. It is predicted that the Moral Disgust and Sexual Disgust scales of the TDDS but not the Pathogen Disgust scale will be significantly associated with the moral foundations, particularly purity/sanctity.
Procedure
Participants completed the self-report measures individually in the laboratory.
Results
TDDS scales and disgust domains of the DS-R
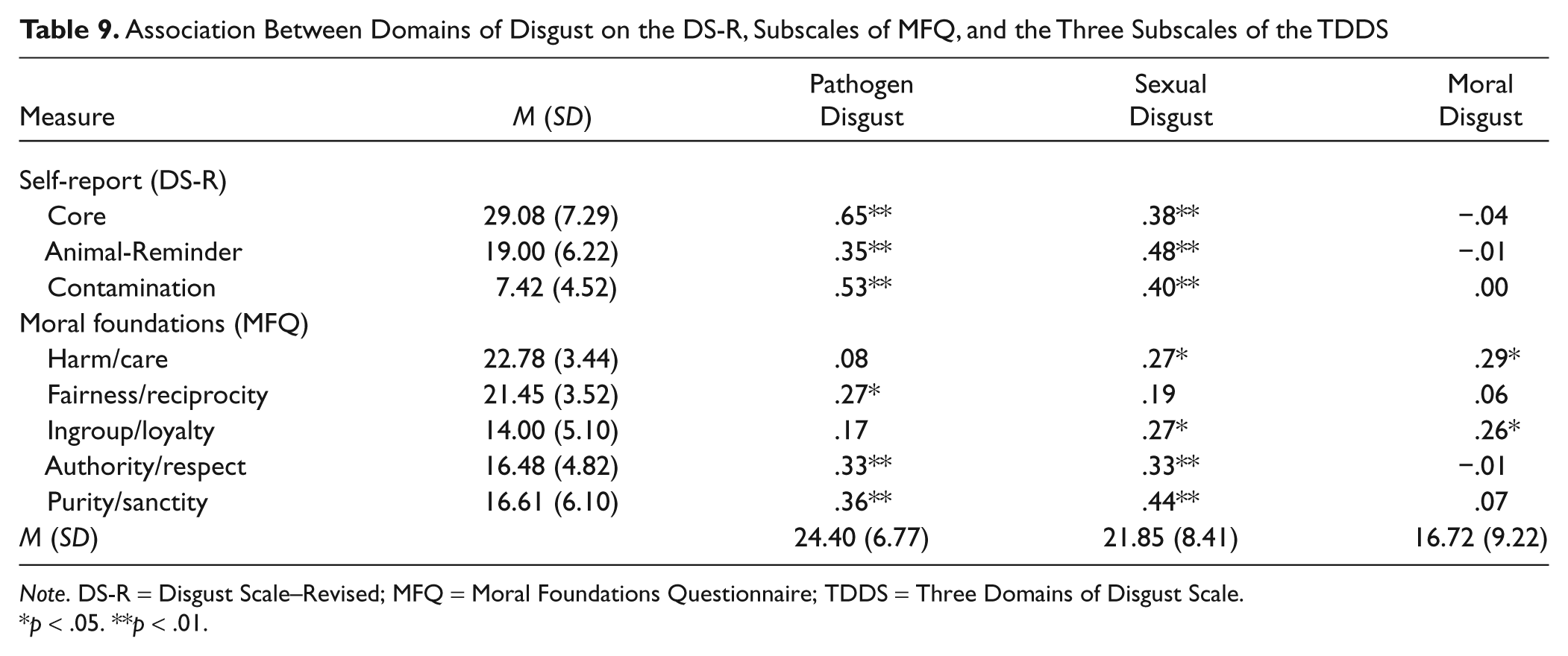
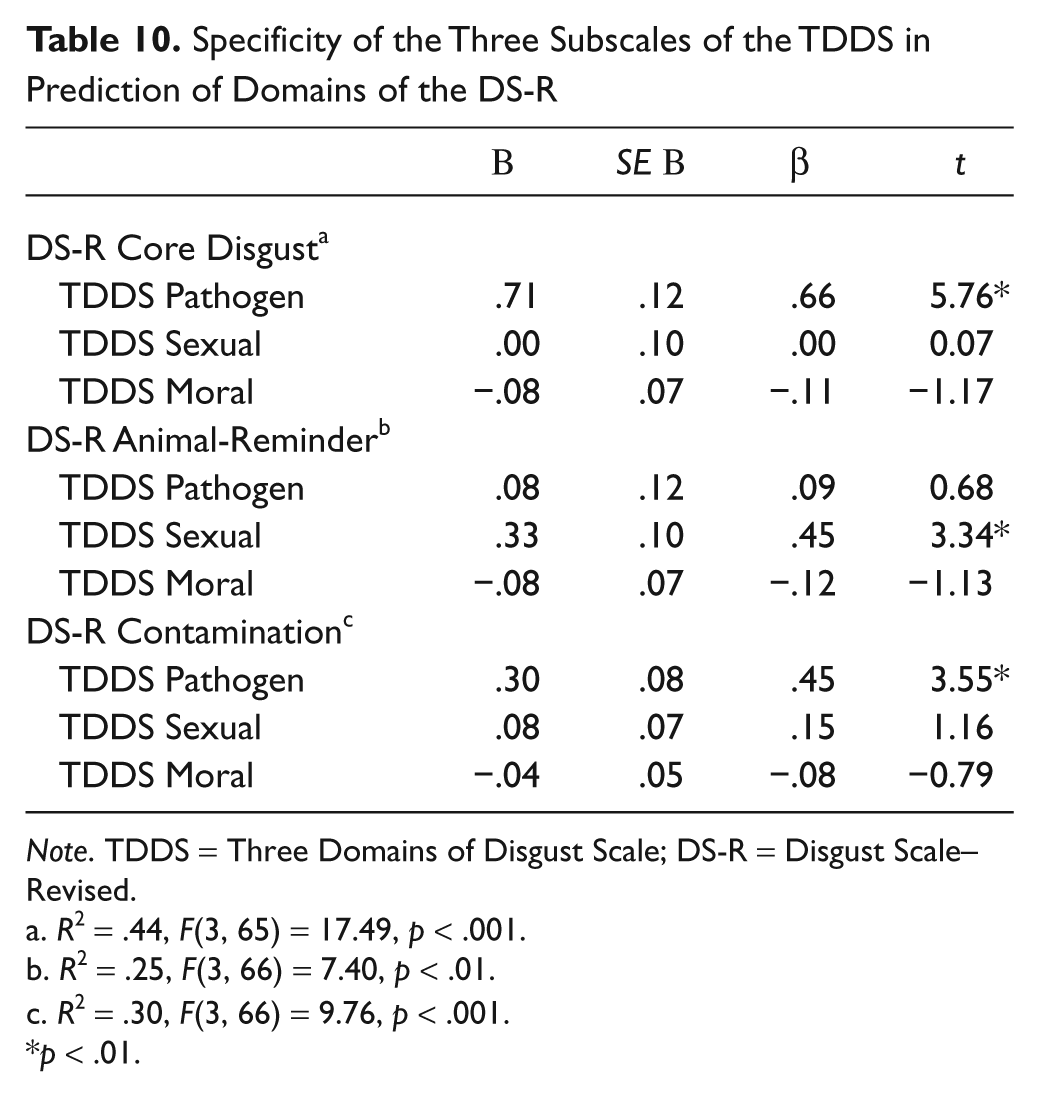
As shown in Table 9, the Pathogen Disgust scale of the TDDS was significantly associated with the Core, Animal-Reminder, and Contamination Disgust subscales of the DS-R (ps < .01). The Sexual Disgust scale of the TDDS was also significantly correlated with the three disgust domains of the DS-R in this sample (ps < .01). However, the Moral Disgust scale of the TDDS was not related to any of the DS-R subscales. A hierarchical multiple regression analysis was then conducted to examine the specific contribution of the three TDDS scales in predicting the disgust domains of the DS-R in the unselected sample. As shown in Table 10, only the Pathogen Disgust scale explained significant variance in predicting the Core and Contamination Disgust subscales of the DS-R (ps < .01). However, only the Sexual Disgust scale explained significant variance in the Animal-Reminder Disgust subscale of the DS-R (p < .01).
Association Between Domains of Disgust on the DS-R, Subscales of MFQ, and the Three Subscales of the TDDS
Note. DS-R = Disgust Scale–Revised; MFQ = Moral Foundations Questionnaire; TDDS = Three Domains of Disgust Scale.
p < .05. **p < .01.
Specificity of the Three Subscales of the TDDS in Prediction of Domains of the DS-R
Note. TDDS = Three Domains of Disgust Scale; DS-R = Disgust Scale–Revised.
R2 = .44, F(3, 65) = 17.49, p < .001.
R2 = .25, F(3, 66) = 7.40, p < .01.
R2 = .30, F(3, 66) = 9.76, p < .001.
p < .01.
TDDS scales and the moral foundations
Table 9 shows that Pathogen Disgust was significantly associated with scores on the fairness/reciprocity, authority/respect, and purity/sanctity subscales of the MFQ (ps < .05). The Sexual Disgust scale of the TDDS was significantly associated with the harm/care, in-group/loyalty, authority/respect, and purity/sanctity subscale of the MFQ (ps < .05). Moral Disgust only significantly correlated with the harm/care and in-group/loyalty subscale of the MFQ (ps < .05).
Discussion
The findings of Study 5 show that the Pathogen Disgust scale of the TDDS uniquely predicted the Core and Contamination Disgust subscales of the DS-R, whereas the Sexual Disgust scale of the TDDS uniquely predicted the Animal-Reminder Disgust subscale of the DS-R in an unselected sample. This finding is partially inconsistent with those of Study 4 where the Animal-Reminder Disgust subscale of the DS-R was uniquely predicted by only the Pathogen Disgust scale of the TDDS. This finding appears to suggest that the concept of Animal-Reminder Disgust may be marked by pathogen concerns or sexual aversions, perhaps depending on the characteristics of the sample. The present study also showed that the Sexual Disgust scale of the TDDS demonstrated the most consistent association with various moral foundations, including violations of purity/sanctity. Contrary to predictions, the moral foundation of purity/sanctity was not associated with the Moral Disgust scale of the TDDS.
Study 6 Method: Distinguishing Anger and Disgust Across the TDDS Scales
The pattern of findings in Study 4 suggests that what exactly is being assessed by the Moral Disgust scale of the TDDS is unclear. Although one might predict a robust association between moral foundations predicated on concerns of purity/sanctity and the Moral Disgust scale of the TDDS, this was clearly not the case. It may be that endorsing disgust in response to the moral violations on the TDDS does not adequately capture the emotional experience of participants. In fact, it has been suggested that moral disgust may largely be a metaphor for anger (Bloom, 2004). That is the Moral Disgust scale of the TDDS may have less to do with disgust per se and more to do with anger. Accordingly, the last investigation examines differences in the intensity of responses to the TDDS items when the emotional response option is disgust (standard TDDS) or anger (modified TDDS).
Participants and Procedure
A total of 178 undergraduates (76.5% Caucasian; 61.8% female) with a mean age of 19.31 years (SD = 0.99) were randomized to complete one of two versions of the TDDS. One group (n = 89; 79.8% Caucasian; 61.8% female; mean age = 19.20 years, SD = 0.96) completed the original version of the scale where items were scored on a 7-point Likert-type scale ranging from not at all disgusting (0) to extremely disgusting (6). The second group (n = 89; 72.8% Caucasian; 61.8% female; mean age = 19.42 years, SD = 1.02) completed a modified version of the TDDS where items were scored on a 7-point Likert-type scale ranging from not at all angry (0) to extremely angry (6). The two groups did not significantly differ on age, gender, or ethnicity (p > .10). The original (α = .87; Pathogen α = .83, Sexual α = .88, Moral α = .89) and anger modified TDDS (α = .82; Pathogen α = .85, Sexual α = .66, Moral α = .80) total scores demonstrated adequate internal consistency.
Results
A 3 (Domain: Pathogen, Sexual, Moral) × 2 (Affective Anchor: Disgust, Anger) mixed model ANOVA on emotional intensity revealed a significant main effect of Domain, F(2, 338) = 17.95, p < .001, partial η2 = .096, and Affective Anchor, F(1, 169) = 5.03, p < .05, partial η2 = .029, that was qualified by a significant Domain × Affective Anchor interaction, F(2, 338) = 30.44, p < .001, partial η2 = .153. As depicted in Figure 3, examination of this interaction revealed that disgust was rated as significantly more intense than anger for the Pathogen and Sexual scales (ps < .01). However, anger was rated as significantly more intense than disgust for the Moral scale (p < .01). Means and SDs for anger and disgust ratings for the two groups are presented in Table 11.
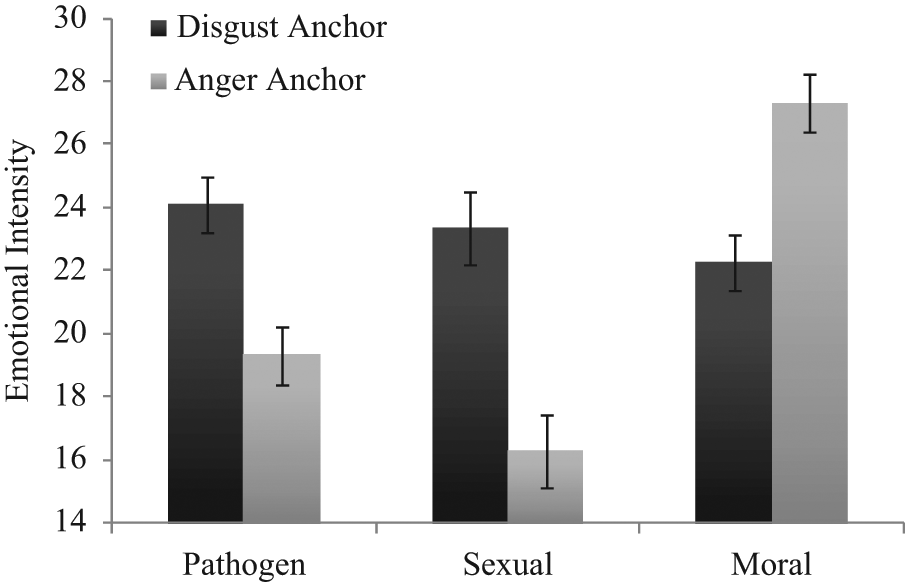
Anger versus disgust responding on the three subscales of the Three Domains of Disgust Scale
Group Differences in Disgust and Anger for the Three Subscales of the Three Domains of Disgust Scale
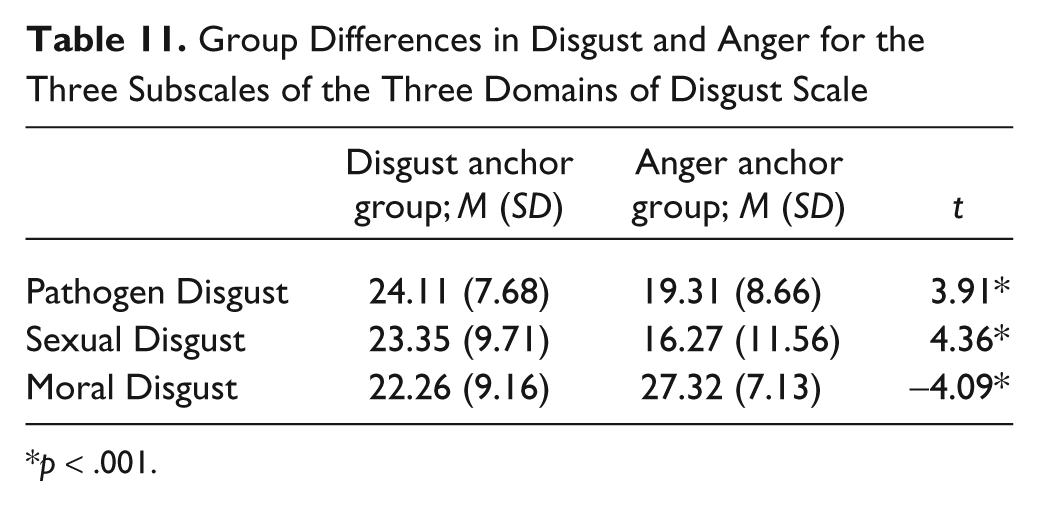
p < .001.
Discussion
The findings of Study 6 suggest that the emotion of disgust is experienced more intensely than anger in response to pathogens and various sexual acts that may be deemed inappropriate. However, the emotion of anger is expressed more intensely than disgust in response to sociomoral transgressions. These findings appear to question the emotional mechanism behind moral disgust, as assessed by the TDDS. Sociomoral transgressions appear to be unique in their ability to evoke a blend of anger and disgust. However, disgust may largely be an artifact of the intensity of the anger that is expressed toward such transgressions.
General Discussion
Disgust has been implicated in several psychological disorders and the emotion continues to influence research topics in several areas in social psychology, including prejudice, decision making, and attitude formation (Olatunji & Sawchuk, 2005). Accordingly, establishing a reliable and valid measure of disgust has important implications for advancing knowledge broadly. The DS is the mostly widely used measure of disgust to date. The DS, and its revised version, the DS-R were derived from a theoretical formation by Rozin et al. (2000). However, Tybur et al. (2009) have recently articulated limitations of the model of disgust proposed by Rozin and colleagues and its measurement by the DS-R. Tybur et al. also proposed an alternative view where disgust consists of three adaptively relevant domains: a pathogen domain, which motivates avoidance of infectious microorganisms; a sexual domain, which motivates avoidance of some sexual behaviors; and a moral domain, which motivates avoidance of moral transgressors. The authors also developed the TDDS to further investigate this disgust classification.
EFA of TDDS items revealed three lower order components labeled Pathogen Disgust, Sexual Disgust, and Moral Disgust. In addition, the EFA did not yield a single complex item (i.e., an item with salient loadings on more than one factor). CFA also revealed that the three-factor solution provided a better fit to the data than the one-factor model. In fact, the fit of the one-factor model was relatively poor. Such a pattern of findings appears to be consistent with the notion that disgust is not a unitary construct (Olatunji et al., 2004). That is, the emotion of disgust may be elicited by a wide range of stimuli that are marked by contamination, uncleanliness, impurity, or the potential for disease (Haidt et al., 1994). Unlike the DS-R, the TDDS also recognizes sexual deviance and sociomoral violations as key adaptive domains of disgust. The assessment of disgust responses to sexual acts and moral transgressions is consistent with prior work showing that disgust elicitors have expanded from contaminated foods to the social domain (Haidt et al., 1997).
Despite empirical support for the three-factor model of the TDDS, the correlation between the three scales was rather modest. Specifically, the associations between the Moral Disgust scale and the Pathogen and Sexual scales scores were low. One interpretation of these findings is that the three scales, particularly Moral Disgust, are relatively distinct from each other. A higher order CFA, examining whether a single higher order factor accounted for the interrelations between the three first-order factors, did provide an adequate fit to the data. However, the higher order factor accounted for substantially more variance in the Pathogen Disgust and Sexual Disgust compared with Moral Disgust, where the variance accounted for was minimal. Data on test–retest reliability also highlight the distinctiveness of the Moral Disgust scale of the TDDS. The test–retest reliability for Pathogen Disgust and Sexual Disgust was significantly higher than the test–retest reliability for the Moral Disgust scale. However, the test–retest reliability for the Pathogen Disgust and Sexual Disgust scales did not significantly differ from each other. Although research has shown that immorality elicits the same disgust response as disease vectors and bad tastes (Chapman, Kim, Susskind, & Anderson, 2009) and that sociomoral acts recruit common neural substrates as pathogen-based stimuli (Borg, Lieberman, & Kiehl, 2008), these findings suggest that disgust responses toward moral transgressions may be less stable and more distinct than responses to other disgust elicitors.
The distinctiveness of the three TDDS scales was also observed when examining gender differences. Prior research has shown that females report higher levels of disgust in general than males (e.g., Olatunji, Sawchuk, Arrindell, & Lohr, 2005). However, consistent evidence was found such that the magnitude of the gender differences significantly varied across the three domains. Specifically, the gender difference was larger for Sexual Disgust compared with Pathogen and Moral Disgust scales. This finding is consistent with those of Tybur et al. (2009) who found that women’s greater disgust was more pronounced in the sexual domain than the pathogen and moral domains. Drawing from their adaptationist model of disgust, Tybur and colleagues contend that this pattern likely reflects the different fitness costs men and women pay for choosing a particular individual as a sexual partner. However, a careful consideration of the pattern of means suggests that a more precise view of the data is that men express less disgust to various sexual acts (relative to other disgust domains), not necessarily that women express more disgust to various sexual acts (relative to other disgust domains). Although sexual disgust may have evolved as a solution to the adaptive problem of avoiding biologically costly sexual behaviors, the enhanced gender differences in sexual disgust may be accounted for by social learning factors (e.g., being reinforced for sex-appropriate behaviors). Consider Item 14 of the TDDS (“bringing someone you just met back to your room to have sex”), social–verbal contingencies reinforce men for expressing less disgust for such acts, whereas in women, social contingencies tend to support expression of negative affect toward such acts.
Examination of the convergent and divergent validity of the scales of the TDDS revealed a complex pattern of findings. Consistent with predictions, the Pathogen Disgust was significantly correlated with measures of disgust propensity and sensitivity, contamination fear, and washing symptoms commonly observed in OCD. Contagion concerns that motivate disease-avoidance may be a process that is shared by these constructs. However, the Sexual Disgust scale of the TDDS was only mildly associated with these measures and the Moral Disgust scale was generally unrelated to these measures. These findings suggest that physical contamination by disease vectors may be less of a motivating factor as one moves across the TDDS continuum (Pathogen → Sexual → Moral). Psychological, rather than physical, contamination may be a more central process as disgust responses evolve toward the moral domain (Rozin, Haidt, & McCauley, 1999). The more robust association between the Pathogen Disgust scale of the TDDS and measures of contagion concerns is consistent with research that has implicated disgust proneness in the etiology and maintenance of OCD-related contamination obsessions and washing compulsions (Olatunji et al., 2010).
The association between the Pathogen Disgust scale of the TDDS and the various measures of contagion was complimented by the physiological and behavioral findings. Specifically, only Pathogen Disgust correlated with physiological responding during viewing of disgust images and emotional distress during exposure to sources of contagion in a public restroom among those high in contamination fear. The Pathogen Disgust factor, unlike the Sexual and Moral Disgust factors, appears to be uniquely associated with physiological and behavioral indicators of contagion sensitivity. Concerns of contagion may partially account for the association between the Pathogen Disgust scale and symptoms of contamination-based OCD. Indeed, this association has commonly been understood in the context of a disease-avoidance model where disgust contributes to the development of contamination obsessions and washing compulsions by preventing contact with infected stimuli (e.g., Matchett & Davey, 1991). However, items on the Pathogen Disgust scale involve cockroaches, body odor, or mold. These items may reflect a fear of contact with disgust stimuli rather than the spreading of disease due to contact. Although the spreading of disease is an important attribute of disgust stimuli, the Pathogen Disgust scale may be better viewed as a “contamination” disgust scale that is similar in content to established measures of disgust. It is also important to note that these findings may be vulnerable to Type I error given the number of correlations that were considered. This highlights the need for future research extending this preliminary multimodal assessment of the convergent and divergent validity of the TDDS scales.
With the exception of mild associations with the Pathogen Disgust factor, the noncontamination symptoms of OCD and various measures of negative affect (e.g., depression, anxiety) were generally unrelated to TDDS scales. This suggests that the TDDS has some degree of convergent validity. Although prior research with the DS has revealed significant associations between disgust sensitivity and neuroticism (e.g., Druschel & Sherman, 1999), the three scales of the TDDS were found to be significantly unrelated to neuroticism in the present study. It should be noted that Tybur et al. (2009) did find a significant association between the Pathogen Disgust and neuroticism, however, this association was relatively minimal (r = .15). Neuroticism is a personality trait that is partially marked by a generalized emotional instability. However, disgust responding, as assessed by the TDDS scales, does not appear to relate meaningfully to this personality trait. The Sexual Disgust and Moral Disgust scales of the TDDS did demonstrate moderate associations with agreeableness and conscientiousness. This suggests that the tendency to be cooperative and careful may partially explain sexual aversions and revulsion felt toward moral transgressions.
According to the theory posited by Rozin et al. (2000) inappropriate sexual acts are categorized as animal-reminder disgust, a domain that reminds us that we, like animals, are mortal. However, Tybur et al. (2009) have questioned the conceptual basis of the animal-reminder disgust domain. For example, they note that the survival value of an antianimal reminder mechanism is questionable from an evolutionary perspective given limited evidence that people universally avoid reminders that they are animals. In fact, the authors found that animal-reminder disgust was more strongly related to the Pathogen Disgust scale of the TDDS than the Sexual Disgust scale. Consistent with this finding, Study 4 found that only Pathogen Disgust explained significant variance in predicting each of the three disgust domains of the DS-R in a sample of individuals high in contamination fear. Although this finding appears consistent with the notion that the three disgust domains of the DS-R are commonly explained as sources of disease, Study 5 revealed that only Sexual Disgust explained unique variance in predicting animal-reminder disgust, whereas only Pathogen Disgust explained unique variance in predicting core and contamination disgust in an unselected sample. A more parsimonious view of these findings is that stimuli that signal the presence of pathogens and inappropriate sexual acts may both map onto the animal-reminder disgust domain. The extent to which pathogens and sexual acts fall into the animal-reminder domain may be contingent on various factors including characteristics of the sample.
Perhaps the most novel aspect of the TDDS is the assessment of individual differences in moral disgust. This may be the one advantage of using the TDDS rather than the DS-R. Indeed, a growing body of research has implicated disgust in the moral domain. For example, Danovitch and Bloom (2009) found that even children were significantly more likely to endorse a disgust face after a story involving any type of moral transgression than after stories involving physical, nondisgusting events. Disgust and cleansing-related words in a word-completion task were also found to be more accessible after reading about immoral actions of criminals (Jones & Fitness, 2008). Although disgust responses in the moral domain may share some similarities with disgust toward core contaminants (Chapman et al., 2009), these responses have also been shown to be very distinct. For example, Simpson, Carter, Anthony, and Overton (2006) found that disgust responses to core elicitors weakened over time whereas sociomoral responses intensified. Thus, it is unclear if moral transgressions are represented on the same disgust dimension as other repugnance stimuli. The present finding that the Moral Disgust scale of the TDDS was unrelated to disgust proneness, as assessed by the DPSS-R and the DS-R, suggests that moral transgressions may not be accurately assessed on the same disgust spectrum as other repugnant stimuli. Sociomoral disgust may be more closely linked to more repugnant violations (e.g., incest, pedophilia, homophilia, Nazis) and the absence of such violations on the TDDS may partially account for the lack of a relationship between the Moral Disgust scale of the TDDS and measures of disgust proneness.
The Moral Disgust scale of the TDDS was also found to be unrelated to moral attitudes that are founded on concerns of purity/sanctity. This is surprising given that moral attitudes of purity/sanctity are marked by the notion that the body is a temple which can be desecrated by immoral activities. The associations with personality traits of conscientiousness and agreeableness, and moral attitudes of harm/care and in-group/loyalty suggest that rather than disgust responding, the Moral Disgust scale of the TDDS may be more accurately assessing traits of impression management and social conformity. The absence of an association between the Moral Disgust scale of the TDDS and moral attitudes of purity/sanctity may be explained by the nature of the items of the Moral Disgust scale. Moral violations of stealing and lying may be expected to be more strongly associated with moral attitudes of harm/care whereas more repugnant moral violations not observed on the TDDS (e.g., incest) may be more strongly associated with purity/sanctity. Danovitch and Bloom (2009) did find that children associate facial expressions of disgust with violations such as stealing money and telling lies and there is evidence that some level of physical disgust is experienced toward such transgressions (Chapman et al., 2009). However, the Moral Disgust scale of the TDDS does not appear to clearly assess disgust reactions to moral violations. This view is consistent with the present findings that anger was endorsed more intensely than disgust in response to the items of the Moral Disgust scale of the TDDS. This may be because none of the moral items on the TDDS address violations of purity and research has shown that disgust, but not anger, predicts stronger moral condemnation of behaviors violating purity (Horberg, Oveis, Keltner, & Cohen, 2009).
The results of this study suggest that the TDDS demonstrates psychometric and conceptual strengths and weaknesses. Convergent and divergent validity data suggest that three-factor structure of the TDDS shows some promise. Indeed, the scales appear to be rather distinct from each other. Despite these encouraging results, however, additional conceptual and psychometric refinement and validation of the TDDS is needed. For example, significant reductions in scores on the TDDS were observed over a 12-week period. Thus, it is unclear if the TDDS is a trait or state measure. Prior research using other measures has found no significant changes in disgust even after treatment (de Jong, Andrea, & Muris, 1997). This raises questions about the stability of any individual differences that may be observed on the TDDS, as its scales appear to be highly influenced by environmental contingencies. For example, it has been observed that morals change as a function of life experiences (Bloom, 2010) and disgust responses in the moral domain may also change accordingly. Given that prior research has shown that that the core, animal-reminder, and contamination subscales of the DS-R are distinct (Olatunji et al., 2008), researchers interested in the predictive utility of these disgust domains will be at a disadvantage when using the TDDS. It should be noted, however, that a limitation of the present investigation is the homogeneity of the sample (largely White females). Additional psychometric evaluation of the Moral Disgust scale of the TDDS in a more heterogeneous sample is needed to better delineate what exactly is being assessed. Indeed, the present study is limited by the assessment of the convergent validity of scores on the TDDS largely in the context of symptoms of psychopathology. A broader assessment of the convergent validity of scores on the TDDS may inform determination of the underlying construct. Also, given that the TDDS does not give respondents the opportunity to rate moral transgressions as anything but disgusting, it is not clear if other emotions (e.g., anger) may better capture affective responses to the transgressions. Future research addressing the psychometric and conceptual limitations of the TDDS will prove to be useful in determining its utility. Such research will also directly inform ongoing research aimed at accurately demarcating the domains of disgust.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.