
Abstract
The Panic Disorder Severity Scale (PDSS) is a clinician-administered measure of panic disorder symptom severity widely used in clinical research. This investigation sought to provide clinically meaningful anchor points for the PDSS both in terms of clinical severity as measured by the Clinical Global Impression–Severity Scale (CGI-S) and to extend its clinical meaningfulness by examining its association with quality of life. A total of 63 individuals with a primary diagnosis of panic disorder were assessed on completion of a 6- or 8-week psychotherapy or pharmacotherapy trial for the treatment of panic disorder. As expected, the PDSS was correlated with both the CGI-S and quality of life. These results provide further support for the validity and clinical utility of the PDSS and provide simple anchors to help guide the potential use of the PDSS scale to measure treatment progress in clinical practice.
Keywords
Panic disorder (PD) is a common anxiety disorder that is associated with substantial impairment, economic burden, and comorbidity (Kessler et al., 2006). Effective psychological and pharmacological treatments have been developed for PD (e.g., Chambless & Ollendick, 2001; Schmidt & Keough, 2010). Beyond simply employing one of these empirically supported treatments, clinicians have been increasingly expected to document treatment outcomes with validated measures.
The Panic Disorder Severity Scale (PDSS; Shear et al., 1997) is a seven-item, clinician-administered measure of PD and agoraphobia symptom severity that has become a widely used standard measure. Five items of the PDSS assess the core Diagnostic and Statistics Manual (fourth edition, text revision; DSM-IV-TR; American Psychiatric Association, 2000) symptoms of PD, and two additional items assess impairment in social and occupational functioning. Each item is scored on a 0 to 4 scale for a total of 28 points. The PDSS has demonstrated sound psychometric properties. In an initial sample of patients with primary PD and mild or no agoraphobia, the PDSS was shown to have acceptable internal consistency (Cronbach’s α = .65), high interrater reliability with intraclass correlation coefficients ranging from .87 to .88, and high convergent validity with a number of anxiety-related measures (Shear et al., 1997). In a follow-up study of the measure in a sample of individuals with and without PD, the PDSS demonstrated good internal consistency (Cronbach’s α = .88) and test–retest reliability (r = .71), with individuals with PD scoring higher on the measure than those without (Shear et al., 2001). Confirmatory factor analysis from this study suggested that a one-factor solution best fit the PDSS data. Furthermore, multiple studies have documented that the PDSS is sensitive to change with treatment (see, e.g., Otto, Pollack, Penava, & Zucker, 1999; Pollack, Otto, Worthington, Manfro, Wolkow, 1998; Shear et al., 1997).
Although the PDSS is psychometrically sound and has become widely used in clinical research, there has been limited research anchoring its scores to commonly used measures of severity and impairment factors. Anchoring the PDSS scores to established measures can be helpful in ensuring the clinical utility of the PDSS as the PDSS is only useful if clinicians are able to interpret its scores in a meaningful way. Only one prior study has reported potential anchors for severity, response, and remission (Furakawa et al., 2009). This study found a baseline correlation of r = .63 between the PDSS and CGI-S and suggested anchors as follows: Normal = 0, Borderline ill = 3, Mildly ill = 8, Moderately ill = 12, Markedly ill = 16-17, and Among the most severely ill = 21-22. Our goal was to examine the relationship between the PDSS and CGI-S in a different way that might enhance clinical utility. We determined the mean change in the PDSS total score associated with each anchor point on the CGI-S. Additionally, we examined the association of these PDSS anchors with quality of life, as measured by the commonly used Quality of Life Enjoyment and Satisfaction Scale–Short Form (Q-LES-Q-SF; Endicott, Nee, Harrison, & Blumenthal, 1993).
Method
Participants
A total of 63 individuals aged 18 years and older with a primary PD diagnosis who had completed a 6- or 8-week psychotherapy or pharmacotherapy trial for the treatment of PD, with or without agoraphobia, were included in the current sample. All participants reviewed the procedures, risks, and benefits of the trials with a psychologist or psychiatrist, and they agreed to participate by signing an informed consent document. Psychiatric diagnoses were then determined by a psychologist or psychiatrist using the SCID-I/P (First, Spitzer, Gibbon, & Williams, 2002). Participants with a lifetime history of bipolar disorder or schizophrenia were excluded, as were participants with current alcohol or substance abuse or dependence and those with severe medical disorders likely to result in hospitalization acutely. All clinician-rated measures were administered by trained psychologists or psychiatrists.
Measures
In addition to the PDSS, the following measures of clinical severity and quality of life were administered.
Clinical Global Impression–Severity Scale (CGI-S)
The CGI-S (Guy, 1976) is a one-item, clinician-rated scale of illness severity. Clinicians rate the participant on a modified 7-point scale that was anchored to assess PD severity from 1 (Normal) to 7 (Among the most severely ill patients).
Quality of Life Enjoyment and Satisfaction Questionnaire–Short Form (Q-LES-Q-SF)
The Q-LES-Q-SF (Endicott et al., 1993) is a 16-item self-report inventory designed to measure quality of life across a range of dimensions, such as physical health, mood, and social relationships. Participants rate their satisfaction in each domain on a Likert-type scale from 1 (Very poor) to 5 (Very good). Total scaled scores range from 0 to 100, with higher scores representing higher subjective quality of life.
Results
The average duration of illness among these individuals was 10.5 years (SD = 11.3). The sample had a mean age of 38.7 years (SD = 12.3) and was primarily Caucasian (96.8%) but was mixed in terms of gender (54.0% female). In addition, the sample had a number of comorbid mood and anxiety diagnoses: 63.5% met the diagnostic criteria for at least one comorbid disorder, and 52.4% met the criteria for an anxiety disorder in addition to PD.
Analyses indicate that the PDSS was correlated with both the CGI-S (r = .88, p < .001) and the Q-LES-Q-SF (r = −.51, p < .001). On average, a 1-point increase on the CGI-S corresponded to an increase of 0.34 points in the PDSS mean score (a2.40-point increase in the PDSS raw score). See Table 1 for specific anchor points for the PDSS on the CGI-S. Based on these findings, we suggest the following guides for the PDSS total score: 0-3 = Normal, 4-5 = Borderline ill, 6-9 = Mildly ill, 10-16 = Moderately ill, 17-21 = Markedly ill, and 22-28 = Severely ill.
PDSS Scores by CGI-S
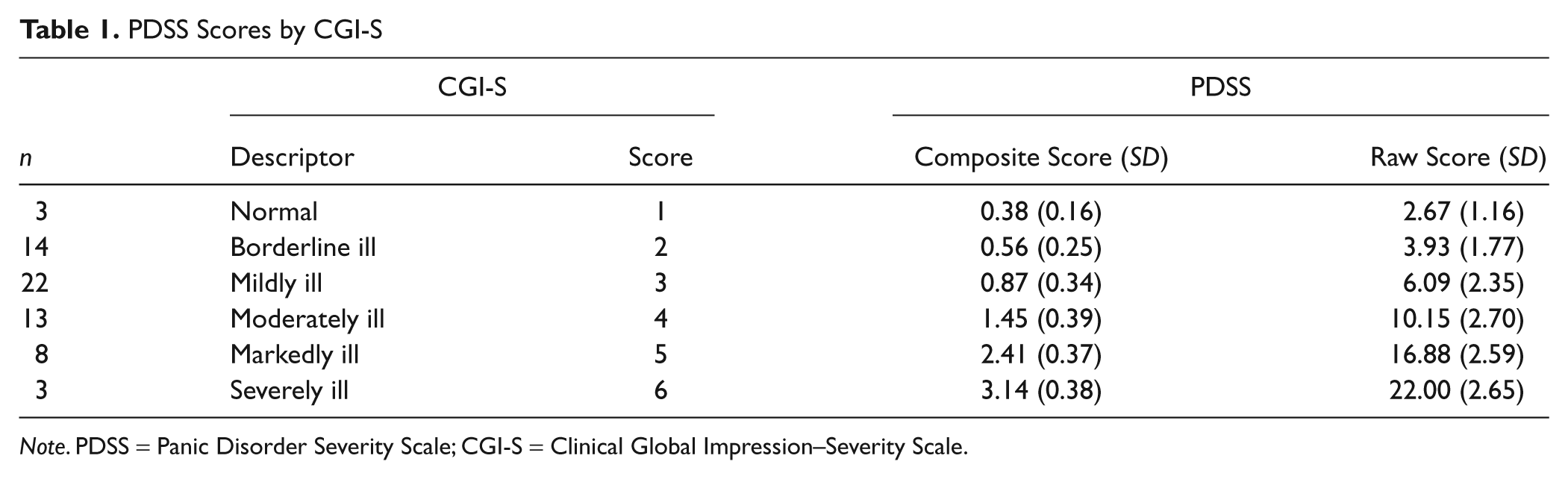
Note. PDSS = Panic Disorder Severity Scale; CGI-S = Clinical Global Impression–Severity Scale.
Discussion
Our results provide further support for the validity and clinical utility of the PDSS and provide simple anchors to help guide the use of the PDSS scale in judgments about PD severity in clinical practice. As anticipated, an increase in PDSS scores was strongly associated with an increase in illness severity as rated by the CGI-S. For example, a total PDSS score of 5 or lower is equivalent to a CGI-S rating of Normal or Borderline ill and might indicate that psychiatric treatment is not warranted, whereas a PDSS score of 10 or greater indicates that the individual is at least Moderately ill and is in need of psychiatric intervention. Beyond specific illness severity, the strong negative association between the PDSS and quality of life supports the supposition that elevated PDSS scores are also indicative of a lower quality of life across a range of dimensions.
As with all investigations, these results should be viewed in light of their limitations. The sample was modest in size, primarily Caucasian, and composed of treatment-seeking individuals at one center, which may limit the generalizability of the current results. Nonetheless, these results provide simple, meaningful anchors to help guide the potential use of the PDSS scale in the measurement of treatment progress in clinical practice. The PDSS was developed to assess the core symptoms of PD based on the DSM-IV, which is anticipated to be replaced by the publication of the DSM-5 in May 2013 (American Psychiatric Association, 2010). However, the proposed revisions to the core PD criteria include only slight changes in wording to enhance clarity and clinical utility (American Psychiatric Association, 2010); therefore, it is anticipated that the utility of the PDSS as an assessment of PD symptom severity will not be affected by the proposed changes.
Our results showed greater correlation between the CGI-S and PDSS (r = .88) than the findings of Furawaka and colleagues (r = .63) and provide similar anchors for the PDSS. Despite being only seven questions that can be rapidly administered, the PDSS is more comprehensive and less subjective than the CGI-S and, thus, can be used by clinicians with minimal training in clinical as well as research settings to comprehensively track symptoms and treatment effects over time.
Footnotes
Meghan E. Keough is now at the Department of Psychiatry and Behavioral Sciences, University of Washington School of Medicine.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This investigation was supported in part by a grant awarded by the National Institute of Health (5K23MH01831) to Dr. Simon and by funding from the Highland Street Foundation.