
Abstract
The Facial Action Coding System (Ekman & Friesen) has shown promise as a behavioral measure of emotional experience. The current study examined the degree of (de)synchrony between self-reported and facial expressions of fear, disgust, and sadness in response to a traumatic event–relevant film among individuals who had experienced a traumatic motor vehicle accident. Given high rates of comorbidity between posttraumatic stress symptoms (PTSS) and depressive symptoms, the potential impacts of both PTSS and depressive symptoms on emotional responding were examined. Results demonstrated synchrony between self-reported and facial expressions of disgust and sadness; however, no association between measures of fear was observed. Furthermore, depressive symptoms were associated with greater fear responding and PTSS were associated only with self-reported fear. Together, results support the importance of examining discrete negative emotions, rather than broad valence categories, when examining fear-based responding in traumatic event–exposed populations. Additional research examining the psychometric properties of the Facial Action Coding System as a measure of discrete emotional experiences among traumatic event–exposed individuals is needed to advance multimodal assessment approaches that yield incremental information for understanding emotional responding in this population.
Emotional responses consist of multiple components across cognitive (e.g., appraisals), behavioral (e.g., facial expressions), and physiological (e.g., sympathetic nervous system activation) domains (Lang, 1979). As a multifaceted construct, emotion is best measured via multiple indicators across each of these systems (Bradley & Lang, 2000; Larsen & Prizmic-Larsen, 2006). However, when obtained concurrently, measures of cognitive, behavioral, and physiological responding evidence relatively weak correlations (Lang et al., 1993). Thus, measuring a single response system is unlikely to provide a comprehensive description of the emotional experience of interest. Research has also demonstrated that discrete emotions, such as fear and disgust, are associated with different patterns of cognitive, physiological, and behavioral responding. For instance, a recent study demonstrated that fear-relevant films elicited significant increases in heart rate and self-reported fear, whereas disgust-relevant films elicited only self-reported disgust but no significant psychological changes (Fernandez et al., 2012). This research highlights the importance of examining (de)synchrony within discrete types of emotional responses rather than broad valence categories (e.g., positive vs. negative affect).
One explanation for observed desynchrony relates to the strategies one uses to modulate an emotional experience, referred to as emotion regulation (Gross, 1998). Emotion regulation is posited to affect the frequency, intensity, and persistence of an emotional reaction (Lanteigne, Flynn, Eastabrook, & Hollenstein, 2014), which may influence measurement of a given emotion across systems. Expressive suppression is an emotion regulation strategy defined by the withholding of ongoing emotion-expressive behavior, such as facial expressions (Gross, 1998). Suppression of the expression of disgust can reduce its overt expression, increase physiological arousal associated with the emotional response, and yet have little effect on self-report of disgust (Gross & Levenson, 1993). Importantly, recent research has demonstrated that expressive suppression is common among traumatic event–exposed individuals and is associated with more severe posttraumatic stress disorder (PTSD) symptoms (Boden, Westermann, et al., 2013). Accordingly, it is necessary to examine multiple modes of emotional responding among traumatic-event–exposed people in order to most adequately capture these differing aspects of emotional responses.
Research has demonstrated that significant difficulty regulating distressing trauma-related emotions is a hallmark feature of PTSD (Keane & Barlow, 2002). Cognitive models suggest that symptoms of PTSD are associated with an overutilization of emotion regulation strategies generally considered ineffective (e.g., expressive suppression) and underutilization of strategies considered more effective (e.g., cognitive reappraisal; Boden, Westermann, et al., 2013). Moreover, clinical research indicates that PTSD is highly comorbid with depression (Kessler, Chiu, Demler, & Walters, 2005), which may also affect synchrony in emotional responding. A recent meta-analysis suggested depression is characterized by “emotion context insensitivity” (Bylsma, Morris, & Rottenberg, 2008; Rottenberg, 2005) or a reduction in both positive and negative emotional reactivity. Furthermore, recent research has demonstrated that major depressive disorder is highly associated with expressive suppression (Campbell-Sills, Barlow, Brown, & Hofmann, 2006). Finally, reduced emotional clarity, defined as one’s meta-knowledge of his or her own emotional experience (e.g., Boden, Thompson, Dizen, Berenbaum, & Baker, 2013; Gratz & Roemer, 2004), is associated with higher PTSD symptom levels (Ehring & Quack, 2010). This is noteworthy as limited clarity regarding one’s emotional experience would be expected to affect self-report of such an experience to a greater degree than behavioral responding. Together, the elevated likelihood of traumatic-event–exposed people attempting to suppress emotional expression along with relatively limited clarity of their emotional experience highlights the importance of concurrently examining multiple modes of traumatic-event–related emotional responding.
A robust literature has used controlled laboratory-based stressors to examine self-report and physiological indices of posttraumatic stress-related emotional responding (e.g., Lindauer et al., 2006; Orr & Roth, 2000). However, only two studies have examined (de)synchrony between self-report and behavioral measures of emotional responding in this population. First, facial expressions of negative affect were negatively correlated with self-reported negative affect among women with PTSD (Wagner, Roemer, Orsillo, & Litz, 2003). However, a composite of all negative facial expressions and a rating scale ranging from “unhappy” to “very unpleasant” were used. Similarly, when compared with women with no history of trauma, women with PTSD reported higher ratings of negative affect in response to both positively and negatively valenced films; however, there were no significant differences in facial expressions of negative affect between the two groups (Orsillo, Batten, Plumb, Luterek, & Roessner, 2004). The authors concluded that individuals with PTSD may exercise volitional suppression of emotional expressivity. A limitation of the coding system used by Orsillo et al. (2004) was the reliance on assessing the frequency of congruent facial expressions (e.g., negative expressions in response to a negative film) but did not assess the frequency of discrete negative emotions. Because PTSD has been associated with a range of distinct, albeit overlapping, negative emotions (Pitman et al., 1990; Pitman, Orr, Forgue, de Jong, & Claiborn, 1987), the ability to more precisely distinguish among a range of negative responses that may be elicited by trauma-relevant stimuli will advance understanding of how traumatic event–exposed people respond to emotion-eliciting stimuli.
The Facial Action Coding System (FACS; Ekman & Friesen, 1978) is a psychometrically sound behavioral measure of expressed emotion that has potential to advance understanding of traumatic event–related emotional responding. Given the relation between expressive suppression and PTSD, behavioral measures are likely necessary to fully understand emotional responding within this population. The FACS measures movement of individual facial muscles, including movements underlying expressions of “basic” emotions (e.g., fear, disgust, sadness). Behavioral measures, such as the FACS, may be particularly advantageous when using an emotion elicitation procedure that necessitates completion of the entire task before measuring self-reported emotion. Such aggregation of the total emotional experience may be vulnerable to distortions, even across relatively short periods of time, and also require one to impose language on nonverbal aspects of emotional experiences (Sayette et al., 2012). Furthermore, the FACS overcomes limitations associated with potential overlap of emotion labels. For example, one study found that heightened self-reported positive affect in response to trauma cues was an artifact of overlapping variance between anxious arousal and items used to measure positive affect (i.e., “alert,” “attentive,” “active”; Nosen et al., 2012). In contrast, the FACS allows for coding and differentiation of overlapping negative affective states. Finally, the standardization of coding procedures in the FACS facilitates replication of this behavioral measure across research studies.
The current study compared behavioral and self-report measures of emotional responding with a film emotion-elicitation procedure that vividly presented both audio and visual traumatic event cues (e.g., Holmes, 2003; Horowitz & Becker, 1973). Based on prior work (Orsillo et al., 2004), we predicted that posttraumatic stress symptoms (PTSS) would (a) be positively related to self-reported fear, sadness, and disgust, but (b) not relate to facial expressions of fear, sadness, and disgust. Furthermore, consistent with Wagner et al.’s (2003) findings, we predicted that facial expressions of fear, sadness, and disgust would negatively correlate with self-reported fear, sadness, and disgust, respectively. Finally, associations between emotional responding and symptoms of depression were also explored to evaluate the potential impact of co-occurring depressive symptoms on emotional responding among traumatic event–exposed populations. Consistent with previous research (Bylsma, Morris, & Rottenberg, 2008), it was hypothesized that depressive symptoms would be associated with reduced emotional reactivity, both in terms of self-report and facial responding.
Method
Participants
Participants for this study were recruited using print and media advertisements distributed in the Northwest Arkansas area. Interested individuals completed a phone prescreening interview during which study exclusion criteria was assessed. Individuals who had experienced any traumatic event in the past 30 days, endorsed current suicidal intent, or were unable to provide written informed consent were thanked for their interest but were not invited to participate. Individuals meeting inclusion criteria were invited to the laboratory to participate.
The final sample was composed of 60 community-recruited adults (Mage = 32.83, SD = 15.72; 78% female) who had experienced a motor vehicle accident involving actual or threatened death, serious injury, or threat to the physical integrity of self or others (American Psychiatric Association, 2000). Eighty-five percent of participants identified as Caucasian, 5% as African American, 5% as multiracial, 1.7% as Native Hawaiian/Pacific Islander, 1.7% as Asian (1.7%), and 1.7% as “Other.” Twenty-two participants (36.7%) met diagnostic criteria for PTSD.
Measures
Clinician-Administered PTSD Scale
The Clinician-Administered PTSD Scale (CAPS; Blake et al., 1995) is a semistructured clinical interview that was used to index the frequency and intensity of 17 symptoms of PTSD and to identify individuals satisfying criteria for a current diagnosis of PTSD. The CAPS has excellent psychometric properties and is considered a gold standard in PTSD assessment (Weathers, Keane, & Davidson, 2001). Severity of PTSS was defined as the sum of intensity and frequency symptom scores. Diagnosis of PTSD was made using the 1, 2 scoring rule recommended by Weathers, Ruscio, and Keane (1999). A predoctoral researcher trained in CAPS administration conducted all interviews (S.J.B.). Prior to data collection, the first author (S.J.B.) completed a training protocol which required (a) observation of a trained administrator (M.T.F.), (b) observed administration of the interview followed by feedback, and (c) independent administrations of the interview to a mock participant followed by review of ratings. This training procedure was implemented until S.J.B. reached 100% interrater reliability with M.T.F.
Visual Analog Scale
Self-reported fear, disgust, and sadness were measured using Visual Analog Scale ratings (Freyd, 1923). Participants were first oriented to the scales with a verbal explanation of anchors and placing vertical lines on the scale to indicate ratings. Specifically, participants were instructed to place a vertical mark to indicate ratings of different emotions on separate 100-mm lines ranging from 0 (none) to 100 (extreme) following presentation of the car accident video.
Facial Action Coding System
Facial expressions were coded using the FACS (Ekman & Friesen, 1978). The FACS scoring system was used to code any instances of facial movements that corresponded with prototypical or major variant expressions of the emotions disgust, fear, and sadness as defined by Ekman, Friesen, and Hagar (2002) during the first minute of the trauma-relevant video. The observed range of expressions was 0 to 2 for each emotion. A FACS-certified coder (S.J.B.) scored all videos and interrater reliability was estimated using a subset of videos (25%) scored by a second certified coder (M.J.Z.). Good to excellent interrater reliability was observed between coders (disgust, κ = 1.00; fear, κ = .64; sadness, κ = .74). These values represent substantial agreement between observers (Viera & Garrett, 2005). After independent coding was completed, raters met to discuss any discrepancies. The coders then collaboratively reviewed segments of tape with any discrepancies (e.g., determining movements that distinguished between fearful and surprised expressions) until agreement was reached. This resulted in the minimal differences between coders evidenced by the interrater reliability kappas.
Mood and Anxiety Symptom Questionnaire
The Mood and Anxiety Symptom Questionnaire is a well-established, 62-item questionnaire that measures symptoms of anxiety and depression (Watson et al., 1995). Participants rate symptom descriptors (e.g., “felt hopeful about the future”) on a scale ranging from 1 (not at all) to 5 (extremely). The anhedonic depression scale was used to measure symptoms specific to depression. Previous research has demonstrated excellent internal consistency for this scale (Buckby, Yung, Cosgrave, & Killackey, 2007).
Procedure
Procedures received IRB approval prior to data collection. After providing informed consent, the CAPS was administered. Participants then viewed an 8.5-minute video consisting of a compilation of actual and media-produced scenes depicting car collisions. The content of the video included images of cars colliding with auditory components of breaking glass, screeching tires, and loud crashes. The video was designed to specifically elicit trauma-relevant fear; thus, images that could elicit disgust (e.g., body parts, blood) were not included in the video. Facial responses were captured by a video recorder behind the stimulus presentation computer and the experimenter exited the room during stimulus presentation. Participants were informed that this segment of the protocol would be recorded, but it was not revealed that their facial expressions were being monitored. Following presentation of the stressful video participants viewed a 5-min, positively-valenced video to reduce acute distress. Participants were then debriefed regarding the purpose of the study, provided referrals for available psychological services in the local community, and compensated $30.
Results
Table 1 includes correlations among PTSS severity, self-reported emotions, emotional facial expressions, and symptoms of depression. In partial support of the hypothesis that PTSS would be associated with self-reported emotional responding, greater PTSS were associated only with higher self-reported fear (r = .35, p < .05). As hypothesized, PTSS severity was not associated with facial expressions of fear, disgust, or sadness. Contrary to predictions that self-reported and behavioral measures of emotion would be negatively associated, self-reported sadness was associated with more facial expression of sadness (r = .32, p < .05) and self-reported disgust was associated with more facial expressions of disgust (r = .32, p < .05). However, self-reported fear was not significantly associated with facial expressions of fear (r = .24, p > .05). As expected, a strong correlation was observed between PTSS severity and symptoms of depression (r = .66, p < .001). Finally, contrary to the “emotion context insensitivity” hypothesis, higher symptoms of depression were associated with higher self-reported fear (r = .29, p < .05).
Correlations Among Posttraumatic Stress Symptoms, VAS Self-Reported Emotions, FACS Emotions, and Depression.
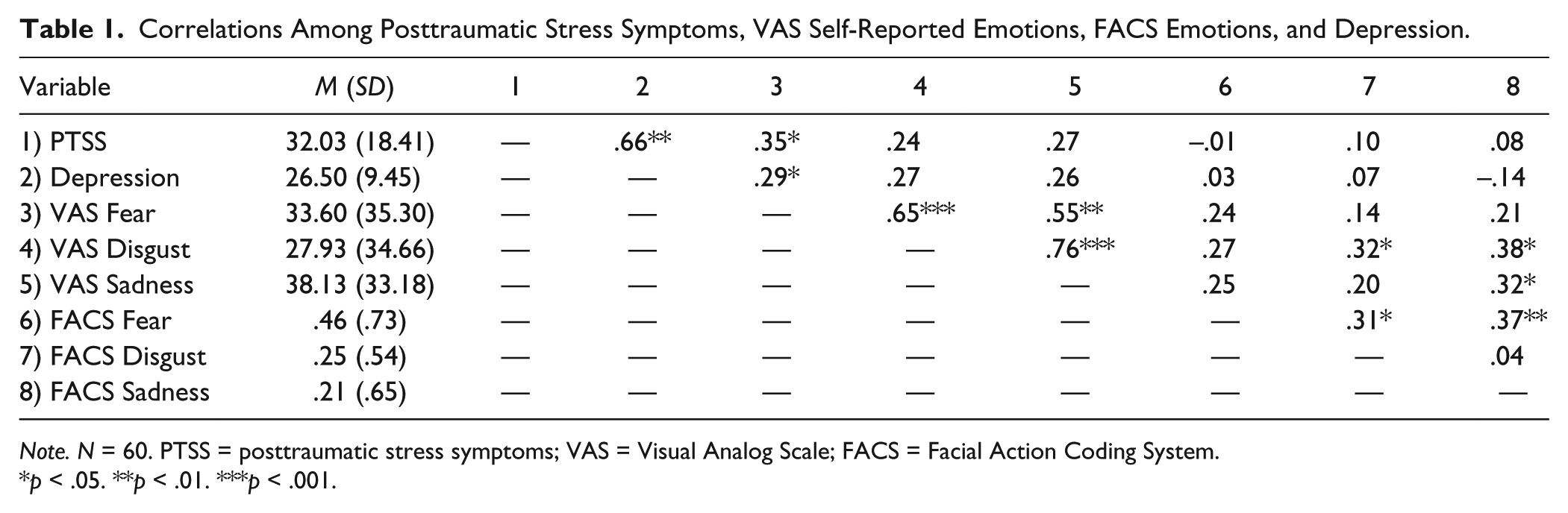
Note. N = 60. PTSS = posttraumatic stress symptoms; VAS = Visual Analog Scale; FACS = Facial Action Coding System.
p < .05. **p < .01. ***p < .001.
Descriptive statistics revealed that most participants experienced few instances of sadness or disgust (mode for both FACS and Visual Analog Scale = 0) during the fear elicitation video. Because of the low observed frequency of these events, measures of sadness and disgust were positively skewed to the extent that the assumption of normality required for parametric comparisons (paired-samples t tests) was not met. Thus, the data were analyzed using a Wilcoxon sign rank test, a nonparametric alternative to a paired-sample t test (Myers & Well, 2003). The results of each comparison are summarized in Table 2. Results revealed nonsignificant differences between self-reported ratings of fear and both disgust and sadness (ps > .05). However, participants self-reported significantly higher levels of sadness than disgust in response to the video (Z = 2.64, p < .01). Wilcoxon sign rank tests further suggested more facial expressions of fear compared with sadness (Z = 3.23, p < .01) and disgust (Z = −2.13, p < .05). Frequency of facial expressions of sadness and disgust did not significantly differ (Z = −1.46, p > .05).
Results and Effect Sizes of Wilcoxon Sign Rank Tests.

Note. N = 60. VAS = Visual Analog Scale; FACS = Facial Action Coding System.
p < .05. **p < .01.
Discussion
Effective treatment for PTSD relies on accessing and processing the full range of trauma-relevant emotions (e.g., fear, disgust; Foa & Rothbaum, 1998). However, numbing and suppression of emotional experiences are hallmark symptoms of PTSD that may interfere with treatment progress. Existing research has demonstrated inconsistencies in emotional responding across response domains among traumatic event–exposed populations (e.g., desynchrony between self-report and physiological indices; Lindauer et al., 2006). However, only two studies have examined (de)synchrony between self-report and behavioral measures of emotional responding in this population. The current results support suggestions that self-report and behavioral measures of emotion yield nonoverlapping measures of experienced emotion and therefore provide a more complete evaluation of elicited negative affect when used together.
Consistent with existing research, PTSS severity was positively correlated with self-reported fear (Orsillo et al., 2004). However, PTSS severity was not related to self-reported disgust or sadness. Interestingly, results demonstrated synchrony between sadness and disgust in regard to self-report and facial expressions, but no relation between self-reported and facial expressions of fear was observed. Given that the stimuli in the current study were designed to primarily elicit fear, it is not surprising that a lower frequency of sadness and disgust ratings and facial expressions were observed. Indeed, it is possible that sadness and disgust would be related to PTSS severity when stimuli selected to elicit these emotions are specifically used. However, it is notable that stimuli designed to elicit fear did not result in agreement between self-report and behavioral expressions of fear. Consistent with previous research documenting desynchrony across behavioral and self-report domains (Wagner et al., 2003), it may be posited that participants reporting fear suppressed the expression of this emotion. Indeed, incongruities in emotional responding are theorized to be most likely following trauma cues (e.g., Foa, Zinbarg, & Rothbaum, 1992) and the stimulus used in the current study specifically aimed to elicit fear. Future work should investigate whether exposure to stimuli selected to elicit sadness or disgust would result in synchronous responding for those emotions as observed here. This type of work would allow for determining if the differences in synchrony across emotion types observed here were due to the method used or if fear is atypical in its desynchrony in the context of PTSS.
Finally, results indicated that PTSS severity was not correlated with facial expressions as measured by the FACS. This finding is consistent with existing research (i.e., Orsillo et al., 2004; Wagner et al., 2003), which also concluded that PTSS may not be related to facial reactions to trauma-relevant cues. Given the relative paucity of existing research that has used standardized facial coding systems within PTSD populations, the explanation for this apparent lack of association is not yet clear. It is possible that the tendency to suppress emotional expression among those with elevated PTSS severity may blunt facial expressivity. Given that research has documented both negative interpersonal (e.g., poorer communication abilities) and emotional (e.g., increased negative affect) consequences of suppression (Butler et al., 2003), blunted facial expressivity in PTSD may contribute to the maintenance of symptoms. It is also notable that self-reported and behavioral measures of fear were not associated, while fear was the only negative emotion correlated both with PTSS and depressive symptoms. Because of the paucity of existing research examining (de)synchrony between PTSD and co-occurring disorders in regard to facial expressions of emotional responding, future research would benefit from examining whether PTSD and depression have unique and combined influences on emotional responding across domains.
Contrary to prior work (Wagner et al., 2003), facial responding and self-report were not inversely related. In fact, facial expressions of disgust and sadness were positively correlated with higher self-reported disgust and sadness. This finding suggests more synchrony between self-report and behavioral measures of responding than previously demonstrated. It is possible that although increased physiological responding has been observed during suppression of overt expression of emotion (e.g., Gross, 1998), suppression of emotion expression may not increase self-report of emotional experience, as observed here and previously (Gross & Levenson, 1993). The different patterns observed across studies may also be due to different emotions being examined; studies have examined aggregate measures of negative affect (Orsillo et al., 2004; Wagner et al., 2003), the effects of suppressing disgust (Gross & Levenson, 1993), and specific emotions elicited by a film designed to minimize disgust reactions. Additional research comparing and contrasting (de)synchrony across emotions will significantly advance understanding emotional responding to traumatic event cues.
Although results suggested more facial expressions of fear than sadness, there were no significant differences in the self-report of these two emotions. Furthermore, more facial expressions of fear than disgust were observed, whereas these two emotions were not significantly different at the self-report level. In combination with the fact that the video was designed to specifically elicit fear, these results suggest that behavioral measures of emotion are beneficial to the real-time assessment of emotional responding to traumatic event cues. Indeed, behavioral measures may circumvent reliance on ability to transform a nonverbal experience into specific emotion labels and allow researchers to capture a range of emotional experiences rather than a single aggregate measure. In fact, emotion research is limited when focused too exclusively on “peak” emotional intensity, thereby artificially chunking emotions into static states (R. J. Davidson, 2000; Raz et al., 2012). Furthermore, gathering self-report measures of affect during stimulus presentation may introduce a distraction. The use of both behavioral and self-report measures, therefore, can be considered complimentary, rather than conflicting methods that can provide more in-depth information regarding the unfolding of an emotion over time without measurement interference. Finally, although the FACS is currently a time-intensive method to evaluate facial responding, automated computer-vision approaches are likely to enhance its feasibility in the near future (Cohn & Sayette, 2010); furthermore, the method will retain standardization and allow for improved replication of studies using the same behavioral measure of emotional responding.
The current sample was relatively small, and was composed largely of Caucasian females. Accordingly, future research should investigate (de)synchrony across multiple measures of trauma-related emotion among more diverse samples, including among individuals with a range of traumatic events and a large sample of those with versus without PTSD. Furthermore, no neutral video was administered; thus, the specificity of facial responding and self-report in response to the car accident video cannot be fully explicated. Future research should use a control video to demonstrate specificity of negatively valenced responding to the stressful video. Additionally, the current study analyzed facial responding that occurred during the first minute of stimulus presentation, resulting in a relatively small number of observations. Future studies would benefit from increased access to trained FACS coders or automated approaches to coding to enable measurement of facial responding throughout stimulus presentation. Furthermore, gathering self-report and behavioral information at multiple time points during stimulus presentation would allow for examinations of (de)synchrony across the onset, peak, and offset of a full emotional experience. Finally, although the current study accounted for blunting of facial responding that may be associated with symptoms of depression, the sociorelational framework of expressive behaviors suggests that facial expressions are socially motivated (Vigil, 2008) and, thus, may not occur in the absence of an audience. Contrasting data suggest that even congenitally blind individuals express emotion (Vermeulen, 2009). Future research should therefore consider the possible influence of other present individuals (including the experimenter) and/or recording devices on facial responding as it may relate to increased facial responding or, potentially, intentional masking of expressions.
Taken together, results suggest that discrete negative emotions typically experienced in the context of PTSS may differ in regard to the degree of (de)synchrony they evidence across response domains. Because effective treatment for PTSD requires processing of negative emotions, it is imperative to understand whether certain emotions are more readily elicited or more easily self-reported by individuals than others. Finally, the evidenced relation between self-reported fear within the context of both PTSS and depressive symptoms suggests that desynchrony may be due, in part, to the presence of commonly co-occurring disorders among individuals with PTSD which may need to be addressed as a specific component of treatment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.