
Abstract
Psychometric properties of the Armenian-language posttraumatic stress disorder (PTSD) Checklist–Civilian version (PCL-C) and the DSM-5 PTSD symptom set were examined in a long-term cohort of earthquake survivors. In 2012, 725 survivors completed the instruments. Item-/scale-level analysis and confirmatory factor analysis (CFA) were performed for both scales. In addition, exploratory factor analysis (EFA) was conducted for DSM-5 symptoms. Also, the differential internal versus external specificity of PTSD symptom clusters taken from the most supported PTSD structural models was examined. Both scales had Cronbach’s alpha greater than .9. CFA of PCL-C structure demonstrated an excellent fit by a four-factor (reexperiencing, avoidance, numbing, and hyperarousal) model known as numbing model; however, a superior fit was achieved by a five-factor model (Elhai et al.). EFA yielded a five-factor structure for DSM-5 symptoms with the aforementioned four domains plus a negative state domain. This model achieved an acceptable fit during CFA, whereas the DSM-5 criteria-based model did not. The Armenian-language PCL-C was recommended as a valid PTSD screening tool. The study findings provided support to the proposed new classification of common mental disorders, where PTSD, depression, and generalized anxiety are grouped together as a subclass of distress disorders. Recommendations were made to further improve the PTSD diagnostic criteria.
Keywords
The burden of disaster-caused posttraumatic stress disorder (PTSD) among exposed subjects is substantial worldwide and the prevalence of PTSD in the areas of natural disasters varies widely, depending on the intensity of exposure, degree of human and material loss, availability of support, and personality traits (Neria, Nandi, & Galea, 2008).
The 1988 Spitak earthquake in Armenia was one of the worst natural disasters of the 20th century. It produced an unprecedented high prevalence of PTSD, ranging from 65% to 95% among different populations of heavily affected adults and children (Goenjian, 1993; Goenjian et al., 1995; Pynoos et al., 1993). Two years after the earthquake, a psychopathological investigation was carried out among a geographically stratified subsample of participants from a large-scale postearthquake cohort study (Armenian et al., 2000). The authors found that almost half of the population in the earthquake zone met the criteria for PTSD. The persistence of PTSD symptoms in this population was attributed to the severity of the disaster-associated losses and long-lasting postdisaster adversities causing persistent stress (Goenjian et al., 1994).
A follow-up investigation of this subsample was conducted in 2012. As the PTSD diagnostic criteria changed since the time of the baseline assessment and several new well-validated self-reporting measures of PTSD, based on Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) criteria (American Psychiatric Association, 2000) were developed, the follow-up study in 2012 applied one of the most widely used PTSD screening instruments at the present—the PTSD Checklist–Civilian version (PCL-C; Weathers, Litz, Herman, Huska, & Keane, 1993). This instrument was chosen because of its demonstrated favorable psychometric properties in a variety of populations (Adkins, Weathers, McDevitt-Murphy, & Daniels, 2008; McDonald & Calhoun, 2010; Ruggiero, Del Ben, Scotti, & Rabalais, 2003; Wilkins, Lang, & Norman, 2011). It has also been translated and validated for different ethnic/racial groups (Hem, Hussain, Wentzel-Larsen, & Heir, 2012; Li et al., 2010; Marshall, 2004; Passos, Figueira, Mendlowicz, Moraes, & Coutinho, 2012). However, its operational characteristics have demonstrated considerable variation across populations and research methods (McDonald & Calhoun, 2010).
It is well recognized that the internal structure of PTSD, mirrored in the factor structure of PCL, is an important subject to investigate, as it could shed light on core constructs representing PTSD, confirm its distinctiveness as a diagnostic unit, contribute to modeling the frequent comorbidity of PTSD with other mood and anxiety disorders and improving diagnosis, prevention, and treatment of this condition (Elhai & Palmieri, 2011).
The DSM-IV criteria for PTSD assume a first-order three-factor model for PCL (i.e., PTSD) with reexperiencing, avoidance/numbing, and hyperarousal domains. However, there is inadequate empirical evidence for this latent structure in the literature (Yufik & Simms, 2010). Studies using different populations and settings suggest various factor structures for PTSD, including indirect hierarchical four-factor (Wu, Chan, & Yiu, 2008), two-factor (Passos et al., 2012; Taylor, Kuch, Koch, Crockett, & Passey, 1998), four-factor with distinct avoidance and numbing domains (King, Leskin, King, & Weathers, 1998; Marshall, 2004; Schinka, Brown, Borenstein, & Mortimer, 2007), four-factor with a dysphoria domain (Gauci & MacDonald, 2012; Palmieri, Weathers, Difede, & King, 2007; Simms, Watson, & Doebbeling, 2002; Yufik & Simms, 2010), and five-factor (Elhai et al., 2011; Wang et al., 2011) models. The four-factor models have the most abundant empirical evidence in populations with various traumatic exposures, while the recently proposed five-factor model has the advantage of combining these well-supported models into a single better-fitting structure (Elhai et al., 2011; Wang et al., 2011).
These previous findings indicate the need to investigate the psychometric properties of PCL with new study populations, especially when applying a translated version of this instrument. The Armenian-language version of the PCL-C was first developed and used in this postearthquake cohort. Thus, the objective of this study was to investigate the psychometric properties of the Armenian-language PCL-C, including its factor structure, internal consistency, and correlation with measures of related psychopathology. Additionally, as the new DSM-5 criteria for PTSD were recently released, we used this opportunity to investigate the properties of the new set of PTSD symptoms and symptom clusters suggested by DSM-5. A number of recent studies have explored the factor structure of this new symptom set and mostly supported the dimensions suggested by DSM-5 PTSD criteria (Biehn et al., 2013; Contractor et al., 2014; Elhai et al., 2012). Nevertheless, Miller et al. (2013) emphasized the need of future research examining alternative structural models of DSM-5 PTSD symptom set. Elhai et al. pointed out the importance of investigating new structural models of PTSD among population groups presenting a different culture (Elhai et al., 2011). Thus, we felt worthwhile studying the internal structure of the DSM-5 PTSD criteria in our study population.
Method
Participants
The study participants were a subsample of a cohort study initiated in 1990 to explore the impact of the 1988 earthquake on survivors’ health. The cohort consisted of all employees of the health care services in the earthquake zone and their family members—32,743 individuals in total (Armenian, Melkonian, Noji, & Hovanesian, 1997). In 1991, a geographically stratified subsample of that cohort consisting of 1,785 adults (between the ages of 16 and 70) from areas most affected by the earthquake participated in the initial phase of the study known as Post Earthquake Psychopathological Investigation (Armenian et al., 2000; Armenian et al., 2002). The follow-up phase of this study was conducted in 2012. The Institutional Review Board of the American University of Armenia reviewed and approved the study protocol. Of the original sample (N = 1,785), information was obtained on 1,487 (83%) individuals, of which 725 individuals participated in the follow-up assessment. The rest were either dead (N = 309), incapable to participate due to ailments (N = 89), unwilling to participate (N = 64), or moved out of the country (N = 300).
Measures
We used the self-administered Armenian-language version of the PCL-C to measure the current status of PTSD in this study cohort, regardless of the type of traumatic exposure causing the disease (although the entire sample was directly exposed to the 1988 earthquake, we used PCL-C to capture the potential impact of any lifetime traumatic event, not necessarily the earthquake). The PCL-C consists of 17 items exactly corresponding to the DSM-IV PTSD symptoms. Each item has a 5-point rating scale ranging from 1 (not at all) to 5 (extremely). Thus, the scale yields a cumulative score of 17 to 85. Two methods were suggested to assess the PTSD status using this scale: (a) computing the cumulative score with a threshold level varying within broad boundaries (from 30 to 60) in different studies and populations (McDonald & Calhoun, 2010; Terhakopian, Sinaii, Engel, Schnurr, & Hoge, 2008) and (b) using a symptom cluster–based method coinciding with the DSM-IV criterion B (at least one reexperiencing symptom of the five—Items B1 through B5), Criterion C (at least three avoidance/numbing symptoms of the seven—Items C1 through C7), and Criterion D (at least two hyperarousal symptoms of the five—Items D1 through D5; American Psychiatric Association, 2000). Some studies used a combination of cumulative score and symptom cluster approach to achieve better estimates (McDonald & Calhoun, 2010). However, recent findings suggest that the score-based approach outperforms the symptom cluster–based approach in achieving higher diagnostic efficiency (Chiu et al., 2011).
Two members of the research team (AD and VK) translated the PCL-C into Armenian language after several rounds of forward and backward translations until a full concordance between the translation and the original instrument was reached. This was followed by pretesting among a convenience sample of 13 survivors of the 1988 earthquake currently living in the earthquake zone. They were asked to respond to the scale items taking a note of the language expression and identifying any items they were not comfortable with or had a difficulty to understand. No such items were identified. The finalized Armenian-language PCL-C faithfully reflected the original scale in terms of both items’ content/sequence and response options.
After applying the PCL-C, we asked four additional items on new symptoms introduced by DSM-5 criteria for PTSD (using the same PCL-C response scale) to be able to investigate the properties of the new set of symptoms as well. The latter includes 16 of the 17 PCL items (except C7 item on foreshortened future) and four new items, one of which reflects reckless/self-destructive behavior, while the remaining three reflect negative emotional state expressed by feelings of distorted blame, loss of trust, fear, anger, guilt, and so on. These four items also passed the rounds of forward and backward translations and pretesting before being finalized in Armenian.
According to DSM-5 diagnostic criteria for PTSD, Criterion B remains unchanged (Items B1-B5), Criterion C consists of two avoidance items (C1 and C2), Criterion D combines the remaining four numbing items with the three new negative emotional state items (D1-D7), and Criterion E combines the five hyperarousal items with a new item on reckless/self-destructive behavior (E1-E6), (American Psychiatric Association, 2013). The item mapping for PCL-C and DSM-5 symptoms is presented in the online appendix (http://asm.sagepub.com/supplemental).
To measure the exposure to potentially traumatic event(s) (DSM-IV Criterion A), a trauma exposure checklist was included in the instrument. This checklist was modified from the Trauma History Screen (Carlson et al., 2011), with the purpose to make it relevant to the study population and feasible to implement. In particular, we asked about the earthquake exposure of this postearthquake cohort separately from the other disasters. The checklist measured the number of times each traumatic event happened, the age when it happened, and the degree of the emotional distress it caused each time on a 4-point response scale ranging from 0 (mildly stressful) to 3 (greatly stressful).
Depression was measured using the validated revised Armenian-language version (Demirchyan, Petrosyan, & Thompson, 2011) of the Center for Epidemiologic Studies–Depression Scale (Radloff, 1977). This self-report scale excluded the four positively worded items (4th, 8th, 12th, and 16th) from the initial 20-item scale, retaining the remaining 16 items and the 4-point response scale ranging from 0 (rarely or none of the time) to 3 (most or all of the time) with a summed score in a range of 0 to 48. A 12/13 cutoff (proportionate to the 15/16 cutoff commonly recommended for the original 20-item scale) was used to distinguish between nondepressed and possibly depressed individuals.
Anxiety was measured through the 10-item Anxiety subscale of the Symptom Checklist-90-R, a 90-item multidimensional self-reporting inventory validated as a whole and for each subscale (Derogatis, 1994). The Anxiety subscale items had 5-point response scale ranging from 0 (not at all) to 4 (extremely). The summed score ranged from 0 to 40 and a 10/11 threshold was used to identify individuals with possible anxiety. The subscale was translated into Armenian using the same approach of forward and backward translations and pretesting.
Analysis
For both PCL-C and DSM-5 PTSD symptom set, SPSS 11.0 statistical software was used for item-and scale-level analyses, including testing for internal consistency. For PCL-C, this was followed by confirmatory factor analysis (CFA) using the AMOS 18 structural equation modeling program to estimate the fit of the following five most-supported models (see the online appendix at http://asm.sagepub.com/supplemental): a model corresponding to the DSM-IV diagnostic criteria (American Psychiatric Association, 2000) with three first-order intercorrelated factors of reexperiencing, avoidance/numbing, and hyperarousal (Model 1); a model with four first-order intercorrelated factors of reexperiencing, avoidance (C1-C2), dysphoria (C3-C7; D1-D3), and anxious arousal (D4-D5; Simms et al., 2002; Model 2); an indirect hierarchical four-factor (reexperiencing, avoidance, numbing, and hyperarousal) model with a single higher order factor of PTSD (Wu et al., 2008; Model 3); a model with four first-order intercorrelated factors of reexperiencing, avoidance, numbing, and hyperarousal recommended by King et al. (1998; Model 4); and a model recommended by Elhai et al. (2011) with five first-order intercorrelated factors of reexperiencing, avoidance, emotional numbing, dysphoric arousal (D1-D3), and anxious arousal (Model 5).
Since there is relatively little supporting evidence for the latent structure of DSM-5 PTSD symptom set in the literature, CFA alone is not recommended for the explorative detection of its latent structure, as it could provide equal support to several quite different models (Wittchen, Hofler, & Merikangas, 1999). For any new sufficiently large symptom set, Hurley et al. (1997) recommended first to explore its internal structure in one sample using exploratory factor analysis (EFA) and then confirm it in another sample using CFA, as replication largely enhances the scientific value of the findings. In a recent article, Miller et al. (2013) also highlighted the importance of supplementing CFA with other statistical methods to investigate the internal structure of the DSM-5 PTSD symptom set. Thus, following the approach suggested by MacCallum, Roznowski, Mar, and Reith (1994), we randomly divided the total sample of 725 cases into half; the first half (363 cases) was used to conduct EFA and the second half (362 cases) to run CFA.
EFA with principal axis factoring was used to identify the underlying domains of DSM-5 PTSD symptom set. The number of extracted factors was determined applying parallel analysis for principal axis factoring using ViSta-7.2.04 statistical software, as parallel analysis was shown to be one of the most accurate tests for estimating the optimal number of factors during EFA (Fabrigar, Wegener, MacCallum, & Strahan, 1999). In addition, Scree test and clinical judgment were used. Oblique rotation (Promax) was chosen as recommended when the factors are expected to correlate (Costello & Osborne, 2005). Then, CFA was applied to compare the DSM-5 criteria-based PTSD structure (Model 1n with four first-order intercorrelated factors of reexperiencing, avoidance, negative cognitive state, and hyperarousal/recklessness) with the EFA-detected structures.
The choice of goodness-of-fit indices was based on the two-index presentation strategy recommended by Hu and Bentler (1999). However, to avoid potential shortcomings of using a combination of two indices, we supplemented the maximum likelihood (ML)–based standardized root mean square residual (SRMR) with two other indices recommended by this strategy: the ML-based comparative fit index (CFI), and the root mean square error of approximation (RMSEA), so that all three major “clusters” of fit indices, each reflecting some unique aspect of the model, are included (Matsunaga, 2010). The cutoff values used for these indices as recommended by Hu and Bentler (1999) were close to 0.08 (or lower) for SRMR, close to 0.95 (or higher) for CFI, and close to 0.06 (or lower) for RMSEA. Chi-square testing for differences was used to statistically compare the nested models’ fit. Nonnested models were compared descriptively using Akaike information criterion (AIC) and expected cross-validation index (ECVI), lower values of which indicate a better fit of the model (Akaike, 1987; Brown, 2006). The practical significance of the difference between the models with different complexity levels was also examined using the Tucker–Lewis Index (TLI), as this index incorporates a penalty for model complexity. A TLI difference of 0.01 or more between two competing models was viewed as indicative of practical significance (Gignac, 2007). As the assumption for multivariate normality of the data was not violated—all univariate skewness values were less than 2.0 and kurtosis values much less than 7.0 (Curran, West, & Finch, 1996), an ML estimation procedure was applied. Each item was specified to load on a single factor. For PCL-C, 4.7% (34 cases) and for DSM-5 PTSD symptom set, 5.1% (37cases) of the sample had missing data at the item level. All the cases with any missing response at the item level were excluded from the analysis during EFA (resulting in 346 valid cases for DSM-5 PTSD symptom set) and when calculating SRMR during CFA (resulting in 342 valid cases for DSM-5 PTSD symptom set and 691 for PCL-C). For all the other fit indices, the cases with up to 14 missing values (720 for PCL-C and 360 for DSM-5 PTSD symptom set) were maintained in the data set.
Finally, to investigate the construct validity of the PTSD scales, we examined the correlation of PTSD and its domain scores with the scores of lifetime trauma (LT) and the closely related psychopathologies of anxiety and depression. Steger’s Z test (i.e., Williams’s T test) was used to identify significant differences between these correlations (Steiger, 1980). As the underlying domains of PTSD differ in their specificity to PTSD, some (e.g., reexperiencing, avoidance) being more closely related to it whereas others (e.g., numbing, hyperarousal) reflecting the general distress common to other mood and anxiety disorders, and since the Simms et al. dysphoria scale is believed to be the most complete representation of general distress bridging PTSD with depression and anxiety (Gootzeit & Markon, 2011; Simms et al., 2002; Watson, 2005), we used symptom dimensions taken from different structural models of PTSD to correlate with the external constructs and to compare their differential internal versus external specificity.
Results
Descriptive Findings
The demographic characteristics of the sample are presented in Table 1. The respondents’ mean age was 58.4 years (SD = 12.1; range = 39-90 years). The count of women in the sample was double that of men but women did not substantially differ from men in basic demographic characteristics. The vast majority of respondents had secondary education or higher, almost half were employed and more than one fourth were retired. Respondents reported from 1 to 7 potentially traumatic events during their lifetime with a mean of 2.6 (SD = 1.1) events. The most endorsed traumatic event was 1988 earthquake, followed by sudden death of close family or friend (Table 1). The average LT score, calculated as the sum of traumatic events multiplied by the perceived stressfulness of each (on a 0-3 scale), was 7.4 (SD = 3.4; range = 1-19), indicating that the majority of the reported events were perceived as greatly stressful (mean perceived stressfulness of 2.8).
Demographic Characteristics of the Sample.
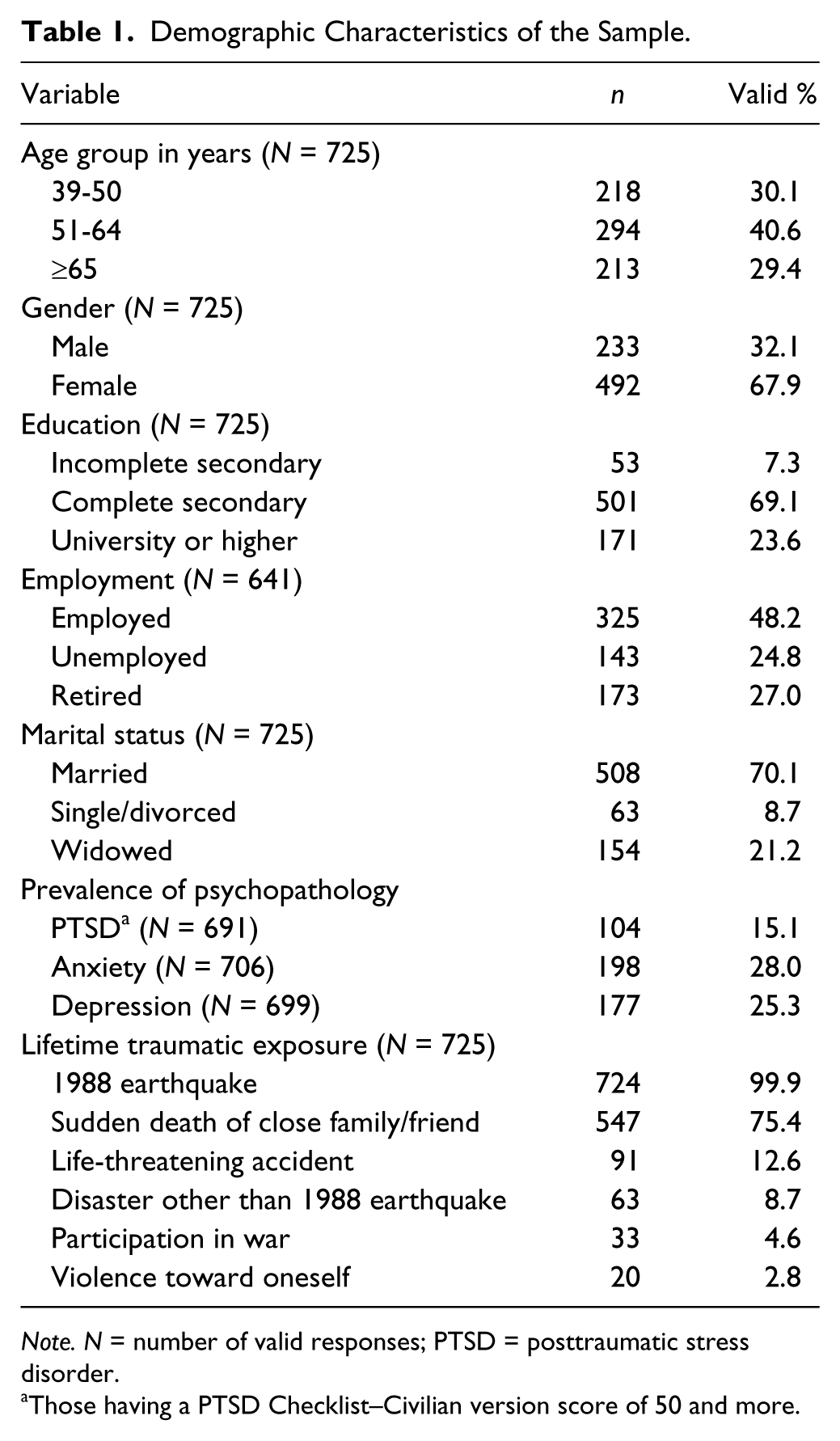
Note. N = number of valid responses; PTSD = posttraumatic stress disorder.
Those having a PTSD Checklist–Civilian version score of 50 and more.
PCL-C Scale
The average PCL-C cumulative scale score was 36.3 (SD = 13.6). The estimated prevalence of PTSD, based on threshold ≥50, was 15.1% (confidence interval [CI] = 12.5% to 17.9%; Table 1). There was no gender difference in the prevalence of PTSD. Among the other measured psychopathologies, the prevalence of anxiety was the highest, 28.0% (CI = 24.8% to 31.5%), followed by depression, 25.3% (CI = 22.1% to 28.7%). There was no gender effect for anxiety, whereas for depression the rate for females was significantly higher than that for males (28.8% [CI = 24.8% to 33.1%] versus 17.9% [CI = 13.1% to 23.5%], p = .001).
Table 2 presents the PCL-C item means, measures of internal consistency, and factor loadings of the best fitting PCL-C model (Model 5) in CFA. The internal consistency of the PCL-C Scale as measured by Cronbach’s alpha was .918. Each of the 17 items added to the internal consistency of the overall scale. Mean item–total correlation for the scale was 0.60 (range = 0.47-0.67). Cronbach’s alpha for the symptom cluster subscales defined by DSM-IV was also above the acceptable threshold level of .80: .864 for cluster B symptoms (reexperiencing), .838 for Cluster C symptoms (avoidance/numbing), and .822 for Cluster D symptoms (hyperarousal).
PCL-C Item Means, Corrected Item–Total Correlations, Cronbach’s Alphas if Item Deleted, Standardized Factor Loadings and Factor Correlations for the Model 5 (Elhai et al., 2011) in CFA.
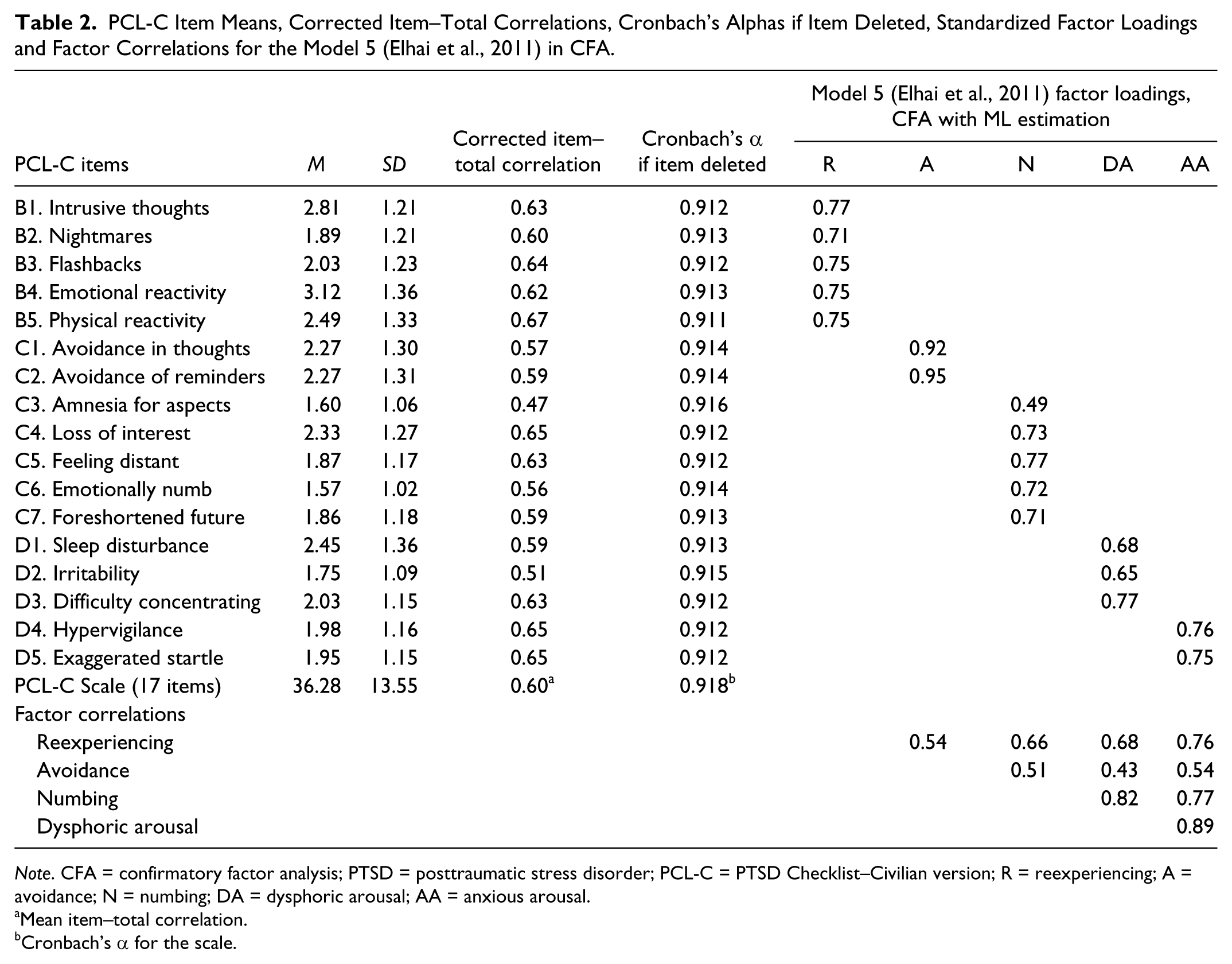
Note. CFA = confirmatory factor analysis; PTSD = posttraumatic stress disorder; PCL-C = PTSD Checklist–Civilian version; R = reexperiencing; A = avoidance; N = numbing; DA = dysphoric arousal; AA = anxious arousal.
Mean item–total correlation.
Cronbach’s α for the scale.
CFA with the ML estimation was used to assess the fit of this and four other recommended models for PCL-C, as described in the “Method” section. The goodness-of-fit indices for all these models are summarized in Table 3. All the models except Model 1 (based on DSM-IV criteria) achieved acceptable fits (RMSEA value less than 0.08; CFI and TLI values greater than 0.90; Hu & Bentler, 1998). Model 3 achieved close-to-excellent fit, whereas both Model 4 and Model 5 achieved excellent fits (RMSEA close to 0.06 and CFI close to 0.95). Chi-square values were compared between the three nested models (Models 1, 4, and 5), indicating that Model 4 fits the data significantly better than Model 1 (Δχ2 = −851.09; p < .001) and Model 5 fits the data significantly better than Model 4 (Δχ2 = −44.67; p < .001). The nonnested models (Models 2 and 3) were compared with each other and with the three nested models descriptively, using AIC and ECVI values. The differences in these values indicated a better fit of Model 5 compared with Model 3 (ΔAIC = −51.84; ΔECVI = −0.077), of Model 4 compared with Model 3 (Δ AIC = −15.17; Δ ECVI = −0.021), of Model 3 compared with Model 2 (Δ AIC = −65.64; Δ ECVI = −0.092), and of Model 2 compared with Model 1 (Δ AIC = −764.28; Δ ECVI = −1.063). Altogether, the five-factor Model 5 emerged as the best fitting model. However, as the two best-fitting models (Model 5 and Model 4) had different complexity levels (Model 5 had fewer degrees of freedom, indicating a larger number of freely estimated parameters than Model 4), we compared the practical significance of these models to one another. The difference in the TLI values between Model 5 and Model 4 was <.01, indicating a lack of practical significance between the fit of these models. Table 2 demonstrates standardized factor loadings and factor intercorrelations of Model 5 ranging from 0.43 to 0.89, with the highest correlation (0.89) observed between the two arousal factors, which was significantly higher than the next highest correlation observed between dysphoric arousal and numbing (0.89 vs. 0.82, Z = 6.4, p < .01). The numbing factor in this model was highly correlated with the arousal factors (0.82 for dysphoric and 0.77 for anxious arousal), whereas the avoidance factor was relatively weakly correlated with the arousal factors (0.43 and 0.54, respectively) and the numbing factor (0.51).
Goodness-of-Fit Indices of the Five PCL and Three DSM-5 Models in Confirmatory Factor Analysis With Maximum Likelihood Estimation.
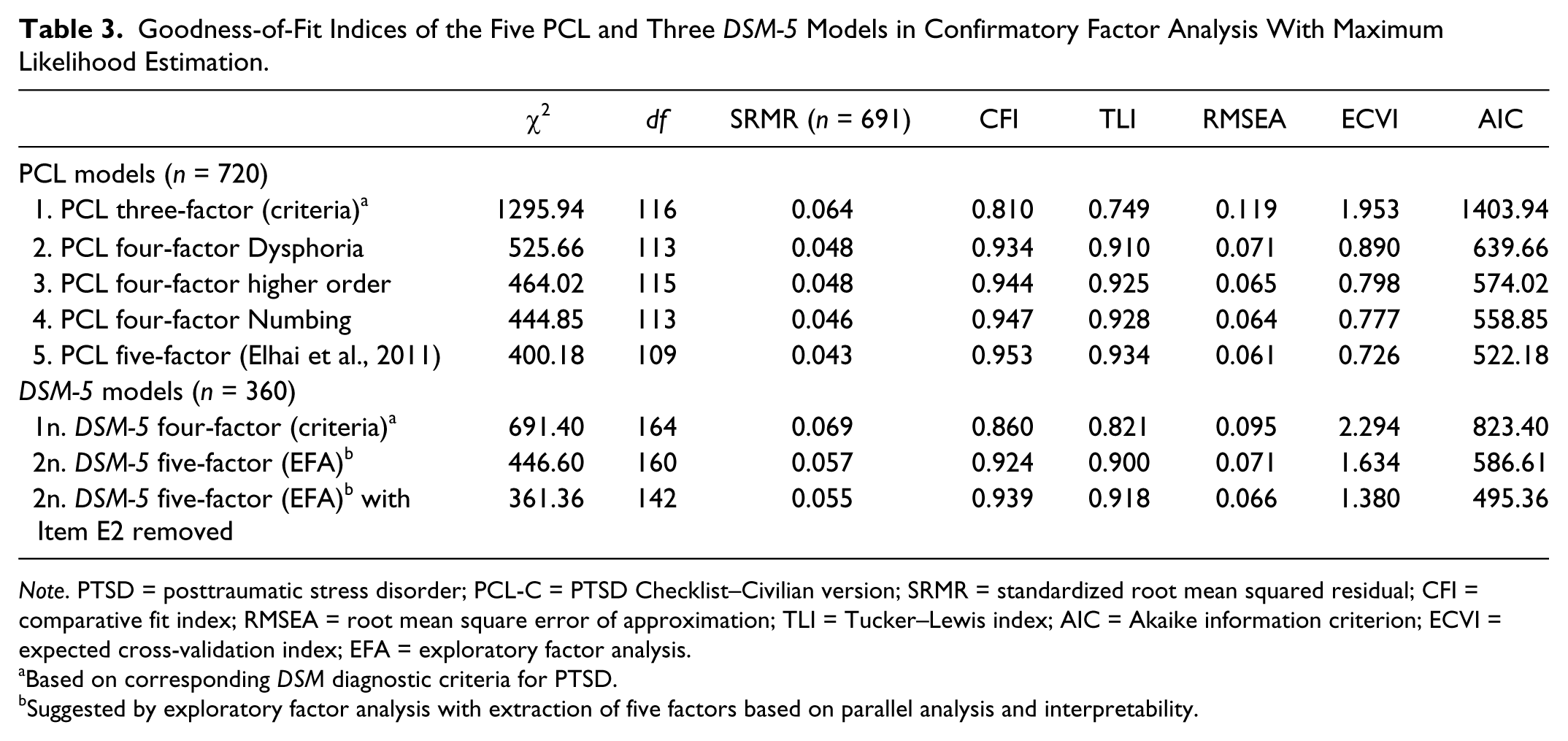
Note. PTSD = posttraumatic stress disorder; PCL-C = PTSD Checklist–Civilian version; SRMR = standardized root mean squared residual; CFI = comparative fit index; RMSEA = root mean square error of approximation; TLI = Tucker–Lewis index; AIC = Akaike information criterion; ECVI = expected cross-validation index; EFA = exploratory factor analysis.
Based on corresponding DSM diagnostic criteria for PTSD.
Suggested by exploratory factor analysis with extraction of five factors based on parallel analysis and interpretability.
DSM-5 PTSD Symptom Set
Overall, the internal consistency of the DSM-5 PTSD symptom set was comparable to that of the PCL-C Scale (Table 4). It had similar Cronbach’s α (.919) and slightly lower mean item–total correlation (0.58, range = 0.42-0.66). Nineteen of the 20 items (except Item E2 on reckless/self-destructive behavior) added considerably to the internal consistency of the scale (Table 4). Item E2 had the lowest item–total correlation (0.42) and the lowest mean value (1.09). All four symptom clusters defined by DSM-5 criteria had acceptable internal consistency (Cronbach’s α > .8).
DSM-5 PTSD Item Means, Corrected Item–Total Correlations, Cronbach’s Alphas if Item Deleted, and Factor Loadings of DSM-5 PTSD Symptom Set Identified through EFA With Promax Rotation.
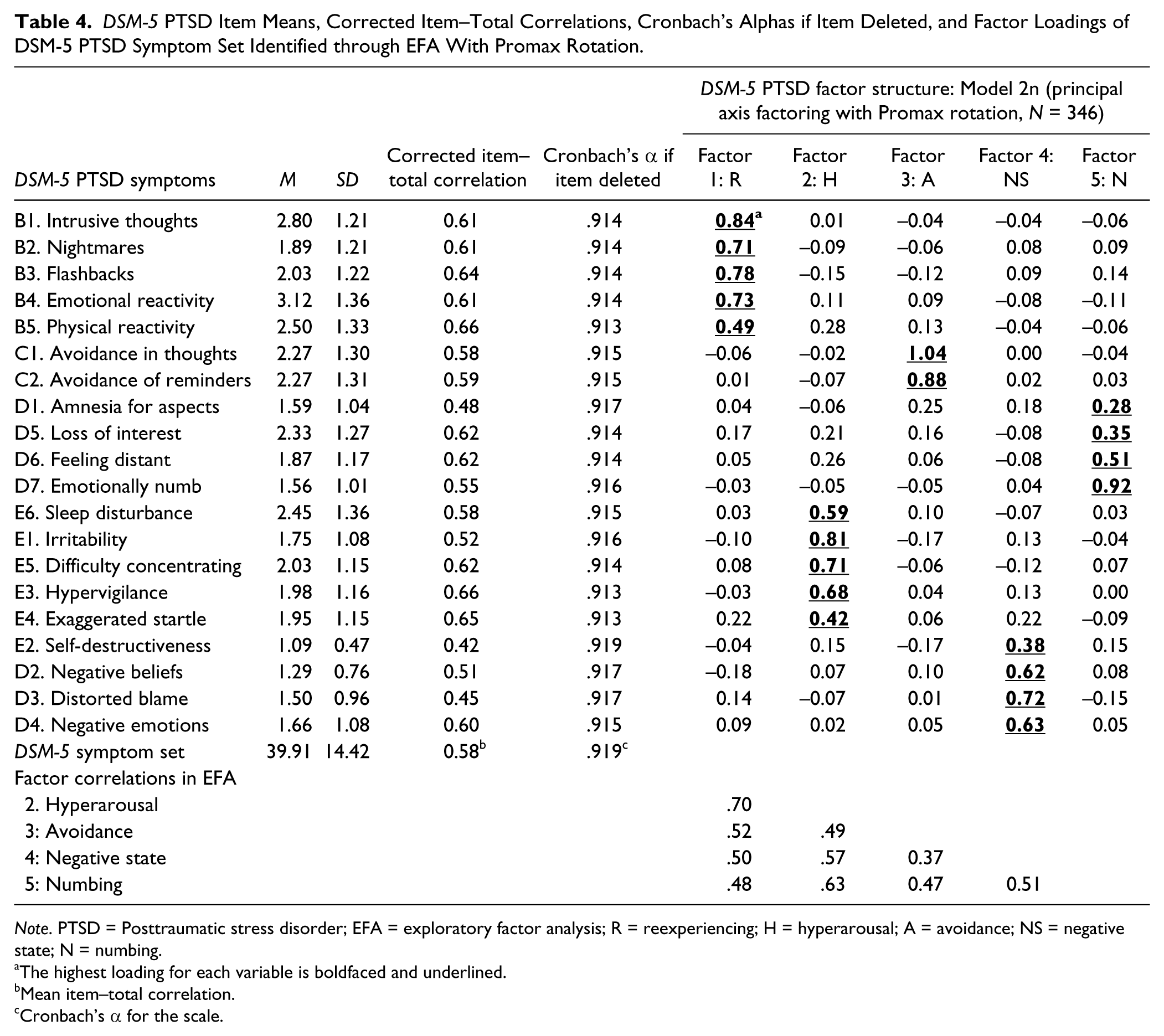
Note. PTSD = Posttraumatic stress disorder; EFA = exploratory factor analysis; R = reexperiencing; H = hyperarousal; A = avoidance; NS = negative state; N = numbing.
The highest loading for each variable is boldfaced and underlined.
Mean item–total correlation.
Cronbach’s α for the scale.
EFA (principal axis factoring) was carried out on a random half of the data set to identify the latent structure of the 20-item DSM-5 PTSD symptom set. Four eigenvalues were greater than one and the scree test suggested four-five factors, whereas the parallel analysis clearly indicated five eigenvalues being higher than the stimulated random samples’ mean eigenvalue, with the sixth eigenvalue slightly over that mean. Of the tested three EFA factor solutions with extraction of four, five, and six factors, the five-factor solution (Model 2n, Table 4) achieved the best clinical interpretability. Its first and third factors corresponded to the DSM-5 symptom clusters B (B1-B5) and C (C1; C2), respectively. However, its second factor loaded high on the five hyperarousal items (E1; E3-E6), the fourth factor on the four newly introduced negative state items (E2; D2-D4), and the fifth factor on the four numbing items (D1; D5-D7). After the rotation, all these five factors were strongly inter-correlated, with the highest correlation observed between hyperarousal and reexperiencing (0.70), followed by that between hyperarousal and numbing (0.63), and the lowest correlation (0.37) between avoidance and negative state (Table 4).
The fifth numbing factor of this model demonstrated signs of instability: two (D1 and D5) of the four numbing items had loadings of 0.35 or less and it broke up into two factors when forcing a six-factor solution. Thus, we reexamined the PTSD factor structure with inclusion of the item on foreshortened future (the C7 item of the DSM-IV criteria, which was removed from DSM-5 criteria) to check whether it would improve the stability of this factor. With the inclusion of this item the same factor structure of PTSD was revealed, and the numbing domain became more stable—four of the five items had loadings 0.50 and higher (only Item D1 had a loading of 0.33, which was still higher than that in the DSM-5 criteria-based model).
During CFA conducted on the other random half of the data set, the EFA-derived five-factor model (Model 2n) achieved acceptable fit (RMSEA value <0.08; CFI and TLI values >0.90), as shown in Table 3, whereas the model based on DSM-5 symptom clusters (Model 1n) failed to achieve acceptable fit. The considerable differences between AIC and ECVI values of these models (Δ AIC = −236.79; Δ ECVI = −0.66) indicated better fit for the EFA-derived five-factor model. Removal of the Item E2 (reckless/self-destructive behavior) from the scale further improved the fit indices of the EFA-derived five-factor model (Table 3).
Correlations Between PTSD Domains and External Constructs
Table 5 demonstrates the correlations between selected PTSD domain scores and the scores of depression, anxiety, and lifetime trauma. We included in this table PTSD constructs based on the two structural models most supported in the literature—King et al. (1998) numbing model and Simms et al. (2002) dysphoria model. Thus, we looked at the correlations between depression, anxiety, lifetime trauma, and the following PCL-based PTSD domains: reexperiencing, avoidance, numbing (King), hyperarousal (King), dysphoria (Simms), anxious arousal (Simms). In addition, we included the domain of negative state, containing the DSM-5-introduced symptoms of negative alterations in cognition and mood and the reckless/self-destructive behavior, and behaving as a distinct construct in our study.
Intercorrelations of Selected PTSD Construct Scores and Their Correlations (Pearson Correlation Coefficients) With Depression, Anxiety, and Lifetime Trauma Scores.
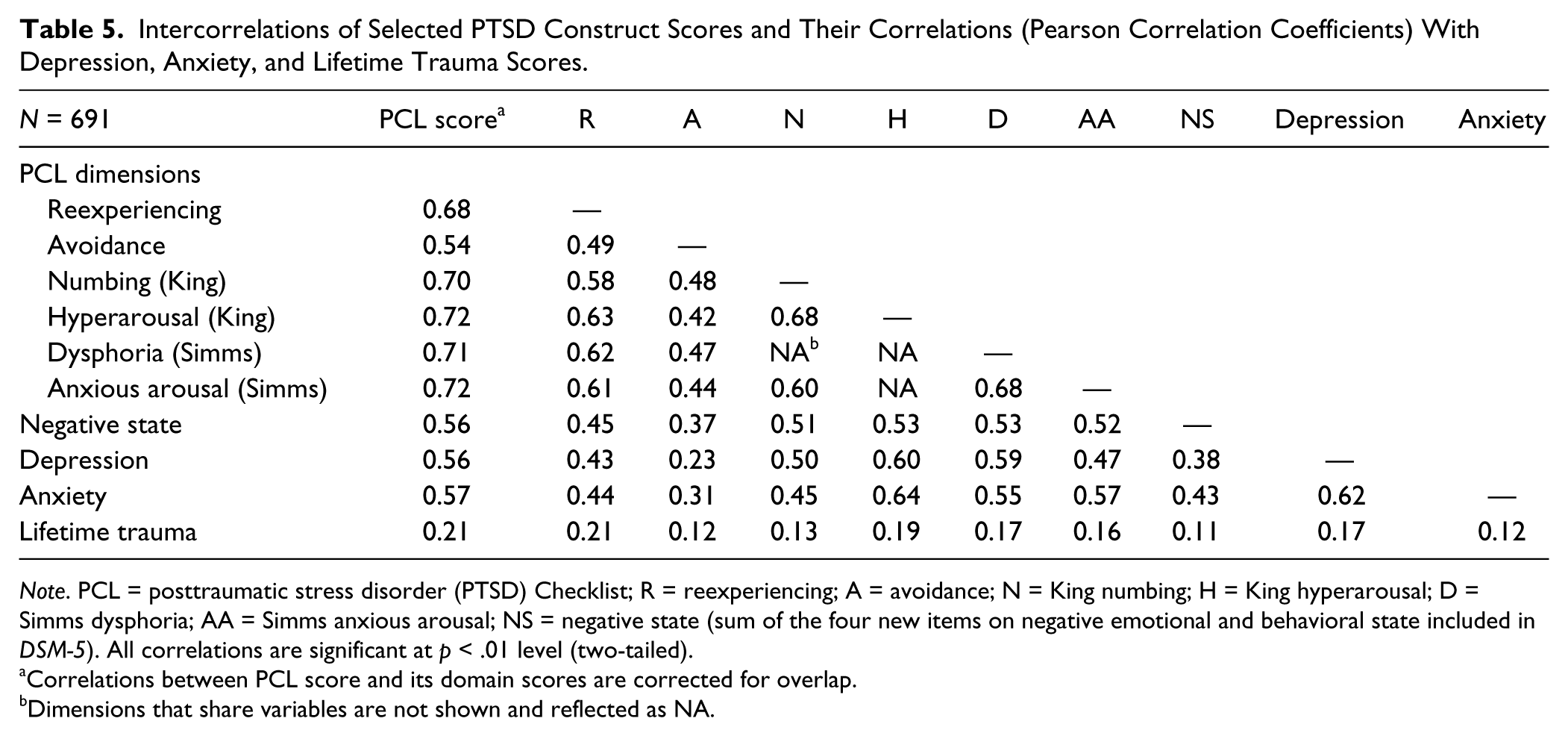
Note. PCL = posttraumatic stress disorder (PTSD) Checklist; R = reexperiencing; A = avoidance; N = King numbing; H = King hyperarousal; D = Simms dysphoria; AA = Simms anxious arousal; NS = negative state (sum of the four new items on negative emotional and behavioral state included in DSM-5). All correlations are significant at p < .01 level (two-tailed).
Correlations between PCL score and its domain scores are corrected for overlap.
Dimensions that share variables are not shown and reflected as NA.
All the observed correlations between these constructs and external variables were statistically significant at p < .01 level (two-tailed). All PTSD domains were highly intercorrelated. For the King et al. (1998) constructs, the highest correlation was observed between hyperarousal and numbing (0.68), followed by that between hyperarousal and reexperiencing (0.63). For the Simms et al. (2002) constructs, the highest correlation was detected between dysphoria and anxious arousal (0.68), followed by that between dysphoria and reexperiencing (0.62). For both models, the correlations between avoidance and the other constructs (varying between 0.42 and 0.49) were significantly weaker than the weakest correlation (0.58) observed between other PCL domains (for the lowest difference, Z = 2.9, p < .01).
All the PTSD domains (including negative state) correlated with PCL score (corrected for overlap) significantly more than with depression and anxiety, demonstrating ability to discriminate between PTSD and external psychopathology (Z > 3.4, p < .01). It is noteworthy that avoidance and reexperiencing correlated with the other PTSD constructs significantly stronger than with external psychopathology (Z > 7.4, p < .01), whereas hyperarousal and dysphoria domains correlated more with depression and anxiety than with avoidance (Z > 2.3, p < .05). Numbing and negative state were in-between correlating with avoidance and external psychopathology almost equally.
Anxiety and depression were highly intercorrelated and correlated equally highly with the PCL score. Both correlated highly with hyperarousal/dysphoria, moderately with numbing, reexperiencing, negative state, and least with avoidance. Interestingly, hyperarousal (King et al., 1998) and dysphoria (Simms et al., 2002) correlated equally highly with depression (0.60 and 0.59, respectively), while hyperarousal correlated higher with anxiety, than dysphoria did (0.64 vs. 0.55, Z = 5.7, p < .01). Of the PTSD constructs, anxious arousal and avoidance were more related to anxiety than depression (Z = 3.7, p < .01 for anxious arousal and Z = 2.5, p < .05 for avoidance). The other constructs were almost equally related to both (the differences were insignificant). The lifetime trauma score had low to moderate correlation with PTSD score (0.21), a higher correlation with reexperiencing than with avoidance (Z = 2.4, p < .05) and numbing (Z = 2.3, p < .05). The correlation of both anxiety and depression with trauma exposure was significant but lower (the difference was significant for anxiety, Z = 2.8, p < .01, while insignificant for depression).
Discussion
In this study, we investigated the psychometric properties and the factor structures of the Armenian-language translation of PCL-C and the DSM-5 PTSD symptom set in a cohort of earthquake survivors. As a whole, PCL-C demonstrated good psychometric properties. This study compared five models of PCL-C factor structure that received strong support in different studies (Elhai et al., 2011; Gauci & MacDonald, 2012; King et al., 1998; Palmieri et al., 2007; Simms et al., 2002; Wang et al., 2011; Wu et al., 2008; Yufik & Simms, 2010). Of the models tested, only the three-factor model reflecting the DSM-IV criteria for PTSD demonstrated unacceptable fit to the data. The King et al. (1998) four-factor numbing model, which differed from the DSM-IV criteria-based structure only in the separation of the avoidance/numbing domain into two distinct domains of avoidance (C1-C2) and numbing (C3-C7), reached a close-to-excellent fit. However, the five-factor intercorrelated model (Elhai et al., 2011) provided a superior fit to the data. This model differed from the King et al. (1998) numbing model only in the separation of the Hyperarousal domain into two subdomains—dysphoric arousal (Items D1-D3) and anxious arousal (Items D4 and D5). Consistent with the observation by Wang et al. (2011), this model bridged the two most-supported factor structures of PTSD, the King et al. (1998) four-factor numbing model and the four-factor dysphoria model developed by Simms et al. (2002). The dysphoria domain introduced by this model is believed to best capture the symptoms of PTSD that are the reflection of a general negative affect inherent to other distress disorders, whereas the other PTSD domains are less clearly related to these disorders (Simms et al., 2002).
Of note, in an experimental study dysphoria model fit best when the data were collected about a specific traumatic event, while the numbing model fit best when the traumatic exposure was not specified (Elhai et al., 2009). This is consistent with the present findings, as we did not specify any traumatic event but asked the participants to think of the worst event they had ever experienced when completing the survey.
In the study by Wang et al. (2011), the numbing model fit better in an earthquake survivor sample, while the dysphoria model fit better in a violent riot victim sample, suggesting that the conflicting results may be, among other factors, due to differences in the type of traumatic exposure. This observation is also consistent with our results: The numbing model fit better than the dysphoria model in our cohort of earthquake survivors, more than half of which (54.1%) reported having in mind the earthquake in 1988 while answering the PTSD items.
Both the four-factor dysphoria model and the five-factor model contain two two-item factors (avoidance and anxious arousal), which is a shortcoming, because the factors with only two items are underidentified and thus inherently unstable (Warner, 2008). Also, although the five-factor model demonstrated the best fit to the data, the difference between the fit indices of this model and the four-factor numbing model lacked practical significance. The two new arousal factors, dysphoric and anxious arousal, introduced by this model, were much more closely related to each other than to the remaining factors. The strength of correlation between these factors (close to 0.90) raised a question whether these two arousal factors were actually distinct. Armour et al. (2012) also observed very high correlation (0.97) between the two arousal factors of the five-factor model in a primary care patient sample, and expressed a concern that this strength of correlation could be a sign of multicollinearity despite the model being statistically superior to the King et al. numbing model. Considering other examples of the same phenomenon either between dysphoric and anxious arousal or between dysphoric arousal and numbing, combined with the lack of differential associations between these highly correlated factors and external psychopathology, they concluded that in certain populations, the four-factor models may be less problematic and more parsimonious than the five-factor model (Armour et al., 2012). Thus, practically, the five-factor model did not provide considerably more value than the King et al. (1998) four-factor numbing model.
Both these best-fitting models indicated the need for grouping the numbing and avoidance symptoms into different clusters in the PTSD diagnostic criteria, especially considering that these two factors were relatively weakly interrelated. The numbing factor was more closely related to the hyperarousal than to the avoidance symptoms, a finding well supported by other studies (King et al., 1998; Marshall, 2004; Palmieri et al., 2007; Passos et al., 2012; Schinka, Brown, Borenstein, & Mortimer, 2007). Also, the distinct-from-avoidance nature of numbing was reflected in the pattern of their relationship with depression. Numbing strongly correlated with depression, whereas avoidance only weakly, as noted in other studies as well (Asmundson, Stapleton, & Taylor, 2004; King et al., 1998).
The PCL score highly correlated with anxiety and depression scores, which in their turn were highly intercorrelated. The correlation coefficients between PTSD and these two psychopathologies were practically equal (0.57 and 0.56, respectively), which is consistent with the reports about the similarity of these disorders, serving as a basis for some researchers to propose a new classification of common mental disorders, where PTSD, dysthymic disorder, major depression, and generalized anxiety are grouped together as a diagnostic subclass of distress disorders instead of being divided into two separate classes of mood and anxiety disorders (Cox, Clara, & Enns, 2002; Slade & Watson, 2006; Watson, 2005, 2009).
Although the King et al. (1998) numbing model fit the data better than the Simms et al. (2002) dysphoria model in the current study, we felt worthwhile to look at the patterns of correlations of the factors of both numbing and dysphoria models with the external variables of depression, anxiety, and lifetime trauma to see whether the dysphoria model demonstrated superior ability of discriminating between external and internal constructs, than the numbing model did (Gootzeit & Markon, 2011). In a meta-analysis, Gootzeit and Markon (2011) compared these two models, and showed that although the hyperarousal and numbing dimensions of the King et al. (1998) model were strongly related to depression and anxiety, the dysphoria dimension of the Simms et al. (2002) model was a stronger predictor of both anxiety and depression, and even, trauma history. Our findings did not support this evidence. We found that hyperarousal factor (King et al., 1998) correlated with the external variables equally/more than dysphoria factor (Simms et al., 2002) did, meaning that it captured general distress equally/better in this study. Nevertheless, our findings are consistent with the findings of Miller et al. (2010). They also did not find an evidence for better discriminant validity of Simms et al. dysphoria factor relative to the King et al. hyperarousal factor in relation with external constructs (Miller et al., 2010).
As expected, both the PCL-C scale score and its domain scores correlated significantly with the LT score. This finding is consistent with other studies showing a positive relationship between the number and/or severity of traumatic exposures and the PCL score (Chiu et al., 2011; Keen, Kutter, Niles, & Krinsley, 2008). Of the examined PTSD constructs, the strongest relationship was observed between reexperiencing and LT, closely followed by that between hyperarousal (King) and LT, indicating that despite the low convergent validity of the hyperarousal (King) domain, it still belongs to PTSD.
Overall, the findings of this study confirm the well-recognized need of separating the avoidance/numbing domain into two distinct domains: avoidance and numbing. Ideally, at least one new item should be added to the avoidance domain to ensure its stability. The construct of hyperarousal should be further investigated to find ways to reduce its heterogeneity and to increase its ability to discriminate between PTSD and other anxiety/affect disorders.
The DSM-5 criteria for PTSD address some shortcomings of the previous one. Most important, the avoidance and numbing domains are separated. Also, the newly introduced items on negative alterations in cognition and mood showed specificity to PTSD. However, the combination of these items with the numbing items did not receive empirical support, as the negative emotion/behavior items constituted a separate factor in EFA, which correlated with hyperarousal more tightly than with numbing. The removal of the item on foreshortened future from the PTSD diagnostic criteria increased the instability of the numbing domain. The heterogeneity of the hyperarousal domain was even increased with inclusion of the item on reckless/self-destructive behavior, as it reduced the internal consistency of this subscale. Miller et al. (2013) also found that the “reckless/self-destructive behavior” symptom did not cohere well with the remaining symptoms of hyperarousal and suggested eliminating it from the core diagnostic criteria of PTSD.
The CFA supported the EFA-identified five-factor structure of the DSM-5 PTSD symptom set in this study with reexperiencing, avoidance, numbing, hyperarousal factors similar to that of the King et al. (1998) numbing model plus a new factor of negative state consisting of the new symptoms of negative cognition/mood and behavior. Indeed, the DSM-5 criteria-based solution failed to achieve acceptable fit in reflecting the latent structure of PTSD.
The main limitation of the current study was its reliance on self-report measures without clinical interview data. Because of this, the study did not measure the criterion validity of the Armenian-language PCL-C to suggest an efficient cutoff score to diagnose PTSD among Armenian population. However, this study has a number of practical and theoretical implications. It suggests that the Armenian-language PCL-C behaves very similarly to the original English-language instrument. Thus, this scale can be recommended as a valid tool for measuring PTSD symptoms in the Armenian population. Studying this unique population with its cultural specificity and traumatic exposure, the study provided good evidence for the cross-cultural validity of both the PCL-C and the PTSD structural models. The intercorrelated five-factor model best captured the latent structure of the Armenian PCL-C. However, the four-factor numbing model could also, more than adequately, serve as a sound representation of the underlying constructs of PTSD. DSM-5 diagnostic criteria for PTSD could be improved by treating the three new negative emotion items as a separate domain, eliminating the item on reckless/self-destructive behavior and keeping the item on foreshortened future.
Footnotes
Acknowledgements
The authors are grateful to Dr. Byron Crape for his thorough review and feedback on the article.
Declaration of Conflicting Interests
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Turpanjian Family Educational Foundation supported this study.