
Abstract
Psychological inflexibility (PI) refers to the overarching and nonadaptive avoidance of thoughts and feelings. PI is a transdiagnostic process that is present in numerous psychopathologies, such as anxiety and mood disorders, addictive behaviors, and chronic pain, as presented by American adults and adolescents. Despite the high rates of depression and depressed mood among Spanish and Latino adolescents and the observed relation between PI and adjustment problems at this age, an instrument assessing PI in Spanish-speaking adolescents is lacking. In this study, we assessed the psychometric properties of a Spanish adaptation of the Avoidance and Fusion Questionnaire for Youth with 483 students from Spain (mean age 13.89 years). The Spanish Avoidance and Fusion Questionnaire for Youth proved to be a two-factor psychometrically sound instrument. Total PI scores correlated positively with depression and negatively with satisfaction with life. The predictive validity results showed cognitive fusion and experiential avoidance to be two interrelated but distinct processes that characterize PI.
Keywords
The term third wave of behavior therapies (TWBT) was first coined by Hayes (2004) to refer to a new set of therapies that, as compared with previous therapeutic models, all shared an emphasis on psychological acceptance and the establishment of new behavioral repertories. Far from being a mere switch in the techniques employed to produce psychological change, the TWBT was born as a model of human suffering that necessarily resulted in the definition of new and fundamentally different therapeutic goals (for a thorough review of its roots, see Hayes, 2004; Hayes, Luoma, Bond, Masuda, & Lillis, 2006).
The TWBT model of human suffering postulates that the presence of thoughts, sensations, and feelings that are experienced as negative (e.g., fear, traumatic memories, failure expectancies, self-doubts, negative judgments, etc.) is inevitable under certain circumstances, as they are natural products of normal human language and cognition (Hayes, Barnes-Holmes, & Roche, 2001). To the extent that they are processes present in all verbally competent humans, not just in those presenting a formal diagnosis of psychopathology, they are not the cause of human suffering. Nonetheless, negative thoughts and feelings will certainly contribute to the occurrence and exacerbation of suffering depending on how a person reacts in their presence (Hayes, Wilson, Gifford, Follette, & Strosahl, 1996). Within this model, attempts to somehow down-regulate thoughts and feelings that are experienced as negative are called psychological inflexibility (PI; Hayes et al., 1996). Specifically, PI refers to the dominance of internal events such as thoughts and feelings over contingencies in determining value-directed actions (Bond et al., 2011; Hayes et al., 1996). PI becomes life-constricting when it occurs across life domains and regardless of any contextual circumstances that suggest its utilization is unworkable (e.g., Torneke, Luciano, & Valdivia-Salas, 2008; Valdivia-Salas, Sheppard, & Forsyth, 2010).
There is a considerable amount of research revealing PI as a transdiagnostic process that is present in numerous diagnostic categories, such as anxiety and mood disorders, addictive behavior, body-image problems, and chronic pain (Hayes et al., 1996; Hayes et al., 2006; Kashdan, Barrios, Forsyth, & Steger, 2006; Ruiz, 2010). There is also evidence that PI is a consistent predictor of daily anxiety-related symptoms and emotional distress, as well as a diminishment of positive life appraisals and emotions (Kashdan et al., 2006). As for its role as a linking process between the occurrence of a psychologically distressing event and diminished well-being, there is extensive evidence from trauma survivors (for a detailed review, see Kashdan, Breen, & Julian, 2010). In posttrauma growth, for instance, there is evidence that, under the same levels of distress and number of trauma events, people scoring high on PI tended to report minimal growth and life meaning, and more generally, diminished well-being. The opposite results were found with people scoring low on PI (Kashdan & Kane, 2011). Last, there is evidence that the use of emotion inhibition and rumination leads to problematic distress only when these strategies are rigidly employed with the goal of reducing distress (Kashdan et al., 2006).
PI is typically assessed with the Acceptance and Action Questionnaire–II (AAQ-II; Bond et al., 2011), which presents improved psychometric properties and factor structure while maintaining similar external validity to the first version (AAQ-I; Hayes, 2004). The AAQ-II includes seven items assessing the unwillingness to experience unwanted emotions and thoughts (e.g., “I worry about not being able to control my worries and feelings”) and the inability to be in the present moment and behave toward a valued direction when unwanted thoughts and feelings appear (e.g., “Worries get in the way of my success”). Respondents rate how true each statement is for them on a 7-point scale ranging from 1 (never true) to 7 (always true). The AAQ-II has been validated with Spanish adults (Ruiz, Langer, Luciano, Cangas, & Beltrán, 2013), clinical and nonclinical German adults (Gloster, Klotsche, Chaker, Hummel, & Hoyer, 2011), subclinical Dutch adults (Fledderus, Voshaar, ten Klooster, & Bohlmeijer, 2012), nonclinical Italian adults (Pennato, Berrocal, Bernini, & Rivas, 2013), and Chinese college students and elite athletes (Zhang, Chung, Si, & Liu, 2014). The AAQ-II has been defined as a single-factor instrument across countries, suggesting that there are no cultural or linguistic factors that may affect the conceptual framework and/or the factor structure of this measure of PI.
Since the AAQ was first developed, there have been a number of versions that have been tailored to specific disorders or populations. Relevant to this article is the Avoidance and Fusion Questionnaire for Youth (AFQ-Y; Greco, Lambert, & Baer, 2008). The AFQ-Y was developed by modeling item content after the AAQ to measure PI as a single construct. It contains 17 items (e.g., “My thoughts and feelings mess up my life,” “I stop doing things that are important to me whenever I feel bad”), and respondents rate how true each statement is for them on a 5-point scale ranging from 0 (not at all true) to 4 (very true). The initial cross-validation study was conducted with a healthy sample of 1,188 12-year-old children. Results showed that AFQ-Y scores correlated positively with anxiety (r = .58), internalizing and externalizing problems (such as depression and conduct problems; r = .64), and somatic complaints (including headache, stomachache, and dizziness; r = .37 to .45) with medium- to large-effect sizes; and negatively with overall quality of life (r = −.30 to −.39) with medium to large effect sizes. Analysis of the factor structure yielded arguable unidimensionality with raw scores not fitting the single-factor confirmatory factor analysis (CFA) model. However, a shorter version containing 8 items, AFQ-Y8, proved clearly unidimensional. The authors noted that the 17-item version assessed one factor (PI), which reflected two interrelated processes that characterize PI, namely Cognitive Fusion (CF) and Experiential Avoidance (EA).
CF is the process by which thoughts about an event become merged with the actual event. In other words, thoughts are taken literally so that, instead of experiencing them as mental events that do not necessarily need to be acted on, the person is dominated by or entangled with them (e.g., Gillanders et al., 2014; Herzberg et al., 2012). On the other hand, EA is the tendency to fight against unwanted thoughts and feelings, resulting in deliberate efforts to change their content or frequency (Hayes et al., 1996; Luciano, Rodríguez-Valverde, & Gutiérrez, 2004; Torneke et al., 2008). EA and PI are highly related constructs, with the former limited to unwanted contents, while the latter refer to a general tendency toward positive and negative thoughts and feelings (Bond et al., 2011).
Withdrawal from a social interaction as a response to the thought “I look stupid, I better hide” may illustrate PI as a single theoretical construct reflecting two overlapping processes, CF and EA. This behavior stems both from CF, or the act of believing the statement “I look stupid” as if it were a fundamental truth about oneself; and EA, or the act of being unwilling to establish contact with such a thought, which is experienced as aversive, and doing whatever it takes to make it go away. The model theorizes that CF and EA contribute to each other in a sort of vicious cycle: EA produces instant relief from the negative feelings that accompany unwanted or negatively experienced thoughts. And, in turn, this relief potentiates the whole rationale sustaining EA, namely, there are thoughts and feelings that do not let us live the life we want, that is, CF (for a detailed description of this mutual contribution, see Hayes et al., 1996, Luciano et al., 2004).
Research employing the AFQ-Y is still scarce but has consistently shown the presence of PI in diverse forms of suffering or adjustment problems in U.S. adolescents. Venta, Sharp, and Hart (2012) found that AFQ-Y scores moderately predicted the diagnosis of anxiety disorders among inpatient adolescents (mean age 16.14 years). The same authors also showed that, among adolescents (mean age 16.24 years), the unwillingness to tolerate aversive private experiences mediated the relation between alexithymia and difficulties in regulating their emotions (Venta, Hart, & Sharp, 2013). PI has also proved to be a key repertoire in borderline personality features. Schramm, Venta, and Sharp (2013) found that AFQ-Y scores explained the variability of borderline symptoms beyond the difficulties in emotion regulation, and partially mediated their relation. PI as measured with the AFQ-Y has also been related to chronic tic disorder (Best, 2009) and repetitive nonsuicidal self-injury behaviors in 16-year-old adolescents (Howe-Martin, Murrell, & Guarnaccia, 2012). In the only longitudinal study to date, Ciarrochi, Kashdan, Leeson, Heaven, and Jordan (2011) explored the effect of mindfulness abilities, emotional awareness, experiential acceptance, and some personality traits on changes in the emotional well-being of 16-year-olds over a 1-year period. Results showed that experiential acceptance predicted increasing positive affect and decreasing sadness and fear.
One of the most prevalent forms of adolescent suffering in Spanish-speaking populations is depression. Epidemiological studies conducted in Spain, for instance, have estimated that the prevalence of clinical depression during adolescence ranges between 4% and 14% (Aláez, Martínez-Arias, & Rodríguez, 2000; Bragado et al., 1995; Subira, Obiols, Mitjavila, Cuxart, & Domenech-Llavería, 1998), turning depression into the second most prevalent adolescent psychological problem in this country (Aláez et al., 2000). Among nonclinical Spanish adolescents, depression symptoms are also common, with rates increasing from 6% to 8% in the 1990s, to 12% to 13% during the past decades (Martínez, 2006; Moreno, Del Barrio, & Mestre, 1996). As for Latino adolescents in the United States, research has shown that this group reports higher level of depression and depressed mood than White, African American, and Asian American adolescents (Joiner, Perez, Wagner, Berenson, & Marquina, 2001; Siegel, Yancey, Aneshensel, & Schuler, 1999), even after controlling for age, gender, and socioeconomic status (Roberts, Roberts, & Chen, 1997; Siegel, Aneshensel, Taub, Cantwell, & Driscoll, 1998). These figures are specially alarming when considering the relation between depressive symptomatology/negative affect during adolescence and the elevated risk of developing problems during adulthood such as depression, suicidal behavior, functional deterioration, and antisocial behavior (Fergusson, Horwood, Ridder, & Beautrais, 2005; Fröjd, Nissinen, Marttunen, Koivisto, & Kaltiala-Heino, 2008; Lewinsohn, Solomon, Seeley, & Zeiss, 2000; Ritakallio et al., 2008).
Despite the high rates of depression and depressed mood among Spanish-speaking adolescents and the observed relation between PI and adjustment problems during adolescence, there is no instrument that assesses PI in the Spanish language and adapted to this age. Aiming to fill this gap, we administered a Spanish version of the AFQ-Y to a sample of adolescents in Spain to analyze its psychometric properties. Given the limitations of the original evaluation, in which the 17-item version showed arguable unidimensionality, in our validation study, we included expanded tests of its factor structure, reliability, and external validity.
Method
Participants
We employed randomized cluster sampling to select participants. The unit (cluster) was the school. The sampling frame was all the public schools in the target region. Each school on the list was assigned a weight equivalent to the number of students attending the school. Five schools were selected, and the principals of all of them agreed to participate. A total of 483 students (237 males and 246 females) belonging to four compulsory secondary education courses filled out the questionnaires. The age range was 11 to 17 years old (M = 13.89, SD = 1.38). To analyze the temporal reliability of the instrument, the same sample completed the questionnaires twice, separated by a 4-week interval. Only 18 of the initial 483 students (3.7%; 12 males and 6 females) failed to complete the second assessment.
Measures and Instruments
Psychological Inflexibility
We employed the AFQ-Y (Greco et al., 2008). It includes 17 items that assess PI (e.g., “My thoughts and feelings mess up my life,” “The bad things I think about myself must be true,” “I push away thoughts and feelings that I don’t like,” and “I stop doing things that are important to me whenever I feel bad”). Respondents rate how true each item is for them, on a 5-point scale ranging from 0 (not at all true) to 4 (very true). High scores reveal PI, which implies the tendency to get fused with the content of thoughts and feelings, and to act on such content by somehow down-regulating it. We note that although PI refers to a general tendency toward positive and negative private experiences, the AFQ-Y only assesses such tendency with the negative ones. We translated the instrument into Spanish with the parallel back-translation procedure (Brislin, 1986). The items were first translated from English into Spanish by expert translators. The items were then back-translated into English and compared with the original ones. Finally, three experts and five students evaluated the adequacy of the items to the construct being assessed. We found no major difficulties with the semantic equivalence of the items in Spanish. The final version included 17 items, the same as the original instrument (see the appendix).
Depressive Symptomatology
We used the reduced version of the Scale of Depressive Symptomatology (Crockett, Randall, Shen, Russell, & Driscoll, 2005), adapted to Spanish by Herrero and Meneses (2006). It contains 7 items assessing depressed mood. Respondents rate how often they feel as described in each item, on a 4-point scale ranging from 1 (rarely—less than once per week) to 4 (most of the time—7 days a week), with high total scores corresponding to a major depressive state. In our sample, the instrument showed suitable internal consistency (Cronbach’s α = .83).
Satisfaction With Life
We employed the Satisfaction with Life Scale (SWLS; Diener, Emmons, Larsen, & Griffin, 1985), translated into Spanish by Atienza, Pons, Balaguer, and García-Merita (2000). The SWLS includes five items, which provide a general index of overall Satisfaction With Life (SWL) of children from 11 years old on. Respondents rate how much they agree with each statement, on a 7-point scale ranging from 1 (I totally disagree) to 7 (I totally agree). Higher scores indicate greater SWL. SWLS scores correlate negatively with measures of loneliness, perceived stress, and depressive symptoms, among others. The instrument showed suitable internal consistency in our sample (Cronbach’s α = .81).
Procedure
We contacted the principals of the target schools to explain the purpose of the research and to request their permission to carry out the study. After we had obtained permission from the school principals, we requested the parents/tutors’ consent for their children to participate in the study. Once in the classroom, the researchers described the goals of the study and informed the students that their participation was voluntary, anonymous, and confidential, and that there were no good or bad answers. At least one researcher was present during the administration of the instruments to provide students with the necessary support to successfully complete the instruments.
Data Analysis
We first calculated the descriptive statistics (variance and covariance; mean, SD, skewness, and kurtosis) of the observable variables included in the CFA by using the statistical package SPSS for Windows version 21 (IBM Corp, 2012).
The authors of the AFQ-Y proposed an arguable one-factor solution for the 17-item version of the instrument because of the inadequate goodness-of-fit data (Greco et al., 2008). For this reason, we conducted a CFA to test for two factorial solutions, with weighted least squares mean and variance adjusted estimation, using 6.1 Mplus (Muthén & Muthén, 1998-2010). We first tested for a one-factor model, assuming PI as the only factor. In the next step, a two-factor model was evaluated, assuming CF and EA as two separate factors. We used Cronbach’s alpha to test the reliability of the instrument.
In order to examine the instrument’s concurrent validity and to further analyze the two factorial solutions, we conducted two path analyses. Within each path model, the means of the items conforming each factor served as input, and SWL and Depression served as third variables. We employed the maximum-likelihood robust estimation.
Last, to establish the instrument’s predictive validity, we tested three models with longitudinal path analysis methodology. The first model only included CF and EA; in the second model, the variable Depression was incorporated as dependent variable; in the third model, Depression was replaced with SWL, also as dependent variable. To establish the differences between nested models (free and fixed to zero), we conducted a log-likelihood ratio test.
Confidence intervals were calculated by using the bootstrap with the 2000 resampling technique, using the maximum-likelihood estimator. The following goodness-of-fit indices were reported: chi-square test (χ2) for model fit, root mean square error of approximation, comparative fit index, and Tucker–Lewis index. Following Browne and Cudeck’s (1993) indications, root mean square error of approximation values close to .05, close to .08, and higher than .10 indicate good, reasonable, and bad fit, respectively. Comparative fit index values should be higher than .90 (Marsh, Wen, & Hau, 2004). Tucker–Lewis index values between .90 and .95 are considered acceptable. Finally, missing data were replaced by the method of linear interpolation usually employed by Mplus.
Results
Descriptive Analysis of the Items
Table 1 shows the descriptive statistics for the items included in the Spanish version of AFQ-Y as well as for the factors tested (variance, covariance, mean, standard deviation, skewness, and kurtosis). The means ranged from 3.56 (Item 6) to 1.96 (Item 14), and the standard deviations ranged between 1.52 (Item 15) and 1.22 (Item 2). Skewness and kurtosis were lower than 1. Overall, the covariances suggest the presence of two factors, CF and EA, with high values among the items of the same factor (e.g., Items 3 and 4 for CF and Items 12 and 15 for EA). Total PI score, as well as CF and EA subscores, showed moderate means (2.77, 2.7, and 2.83, respectively) and moderate to high levels of covariation (higher than 0.48).
Variance (Diagonal), Covariance, and Descriptive Statistics for Each Item and Factors of the Spanish Version of the Avoidance and Fusion Questionnaire for Youth.
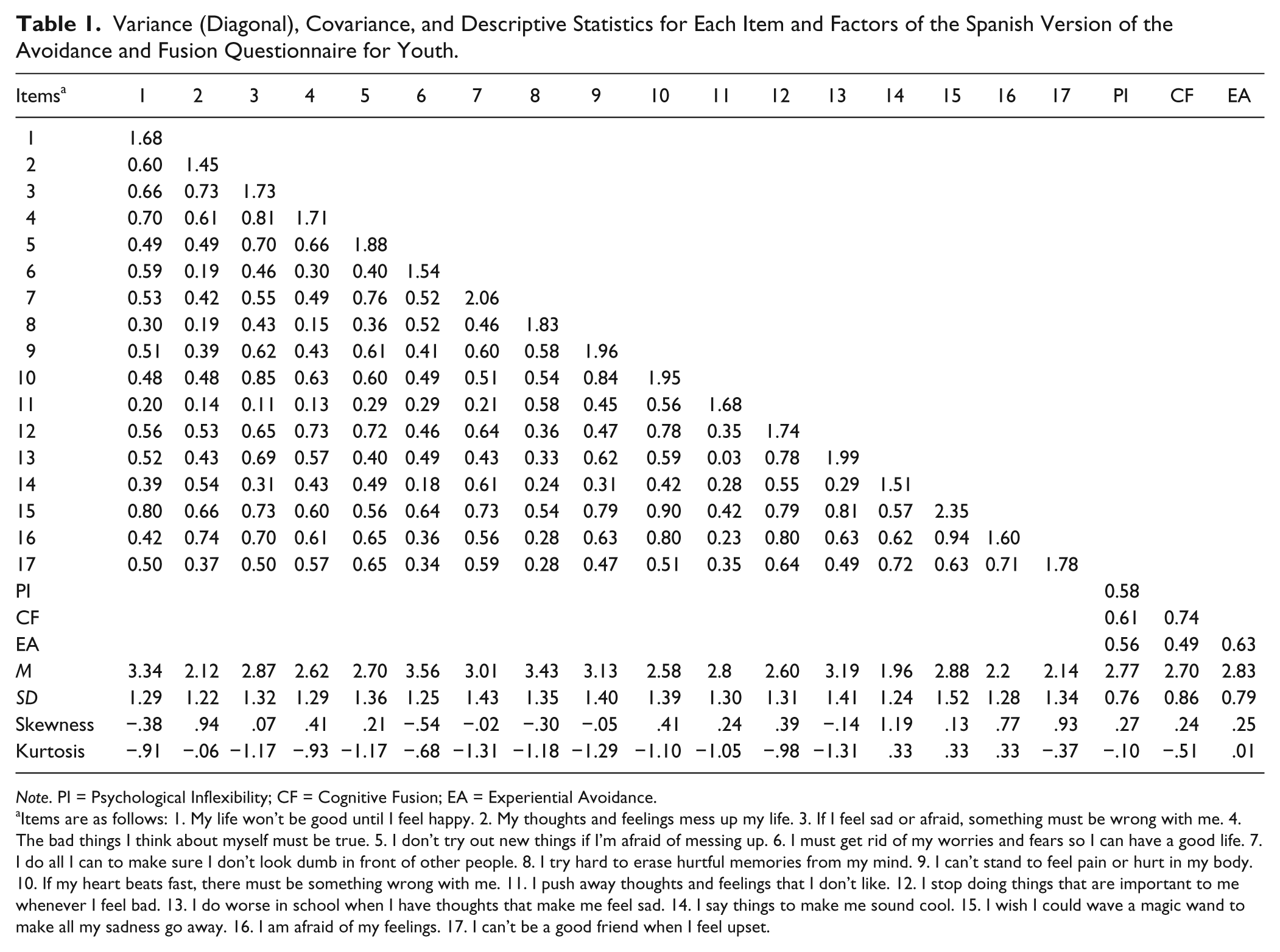
Note. PI = Psychological Inflexibility; CF = Cognitive Fusion; EA = Experiential Avoidance.
Items are as follows: 1. My life won’t be good until I feel happy. 2. My thoughts and feelings mess up my life. 3. If I feel sad or afraid, something must be wrong with me. 4. The bad things I think about myself must be true. 5. I don’t try out new things if I’m afraid of messing up. 6. I must get rid of my worries and fears so I can have a good life. 7. I do all I can to make sure I don’t look dumb in front of other people. 8. I try hard to erase hurtful memories from my mind. 9. I can’t stand to feel pain or hurt in my body. 10. If my heart beats fast, there must be something wrong with me. 11. I push away thoughts and feelings that I don’t like. 12. I stop doing things that are important to me whenever I feel bad. 13. I do worse in school when I have thoughts that make me feel sad. 14. I say things to make me sound cool. 15. I wish I could wave a magic wand to make all my sadness go away. 16. I am afraid of my feelings. 17. I can’t be a good friend when I feel upset.
Confirmatory Factor Analyses and Reliability
We conducted two CFAs. The first one considered PI as the sole factor, the same as in the original validation of the instrument (Greco et al., 2008). In the second CFA, we tested the two factors that Greco et al. (2008) identified as reflecting PI, namely CF (including Items 1, 2, 3, 4, 5, 10, 13, and 16) and EA (including Items 6, 7, 8, 9, 11, 12, 14, 15, and 17). Results showed a poor goodness-of-fit for both factorial solutions (see Table 2). As expected, the correlation between the two factors was high (r = .71). Attending to the modification indices and the content of the items, we tested the same factorial solutions but with correlated uniqueness. The results suggested two method effects: One related to the need to somehow control or suppress unwanted emotions (Items 6, 8, 11, and 15), and the other related to the actual act of suppressing such unwanted emotions as a way of feeling better or relieved (Items 5, 7, 12, and 14). Both factorial solutions—one-factor and two-factor—showed adequate goodness-of-fit (see Table 2). As evidence of reliability, the alpha had values of .87, .81, and .76 for PI, CF, and EA, respectively.
Fit Indices of the Two Confirmatory Factor Analyses Conducted.

Note. df = degrees of freedom; RMSEA = root mean square error of approximation; CFI = confirmatory fit index; TLI = Tucker–Lewis index.
Concurrent Validity
Figure 1 shows the path analysis models conducted on the one-factor (PI; see Model A) and the two-factor (CF and EA; see Model B) solutions. As shown in Model A, the relation of PI with Depression was positive and significant (β = .45, p < .05), and with SWL, it was negative and significant (β = −.13, p < .05). As shown in Model B, the correlation between CF and EA was high (r = .71, p < .05), but their effects on the criterion variables were different. On the one hand, the relation of CF with Depression was positive and significant (β = .53, p < .05), and with SWL, it was negative and significant (β = −.37, p < .05). On the other hand, EA only showed a positive and significant relation with SWL (β = .23, p < .05).

Regression weights and standardized regression weights of concurrent validity models.
Given that both models (one-factor and two-factor) were just identified, none of the goodness-of-fit indices could be calculated.
Predictive Validity
The concurrent validity study suggested that CF and EA are two distinct processes, as they related differently to Depression and SWL. For this reason, although both the one-factor and the two-factor solutions showed almost identical fit to the data, we tested the predictive validity for the two-factor solution only.
Figure 2 shows the three path analyses tested. Model A only included CF and EA; in Model B, Depression was incorporated as dependent variable; in Model C, Depression was replaced with SWL. Each of these models is further developed in Tables 3, 4, and 5, respectively. In all models, the free solutions were just identified. The other solutions showed inadequate or poor goodness-of-fit indices.
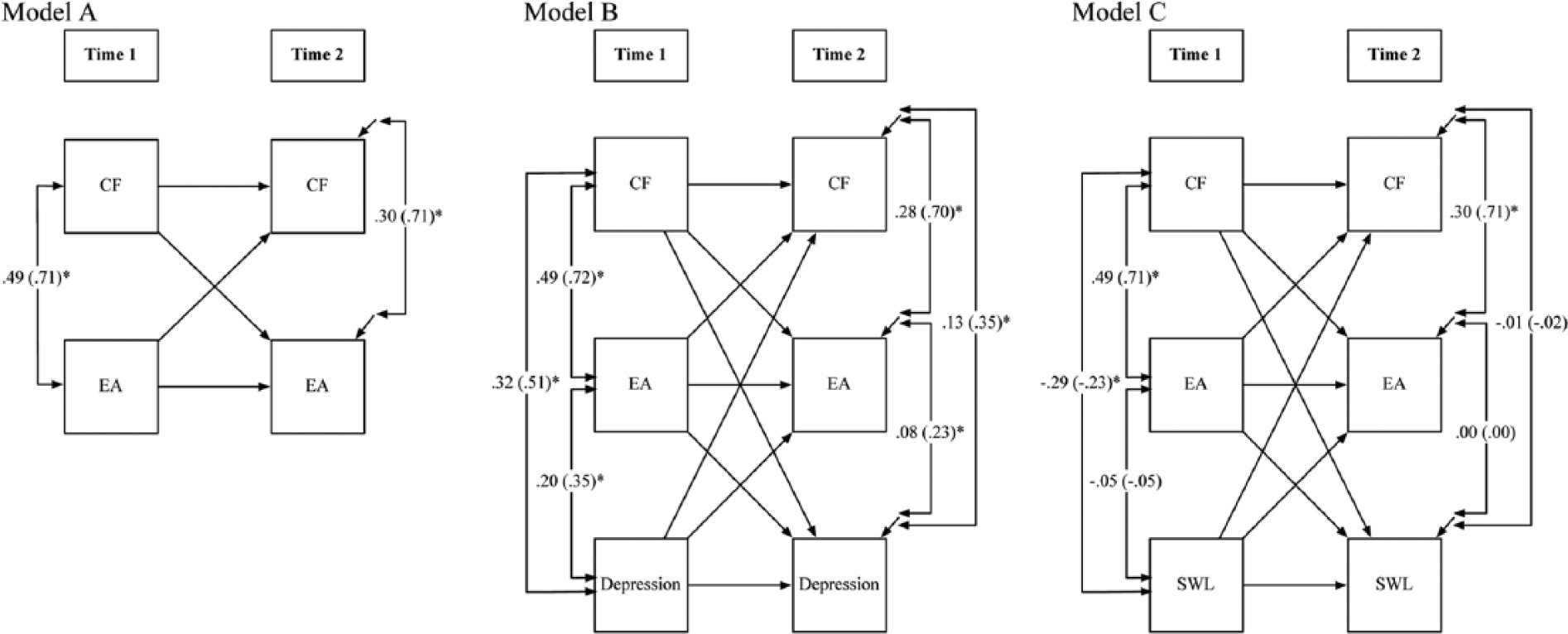
Longitudinal path models.
Longitudinal Path Analysis of Cognitive Fusion (CF) and Experiential Avoidance (EA; See Also Model A in Figure 2).
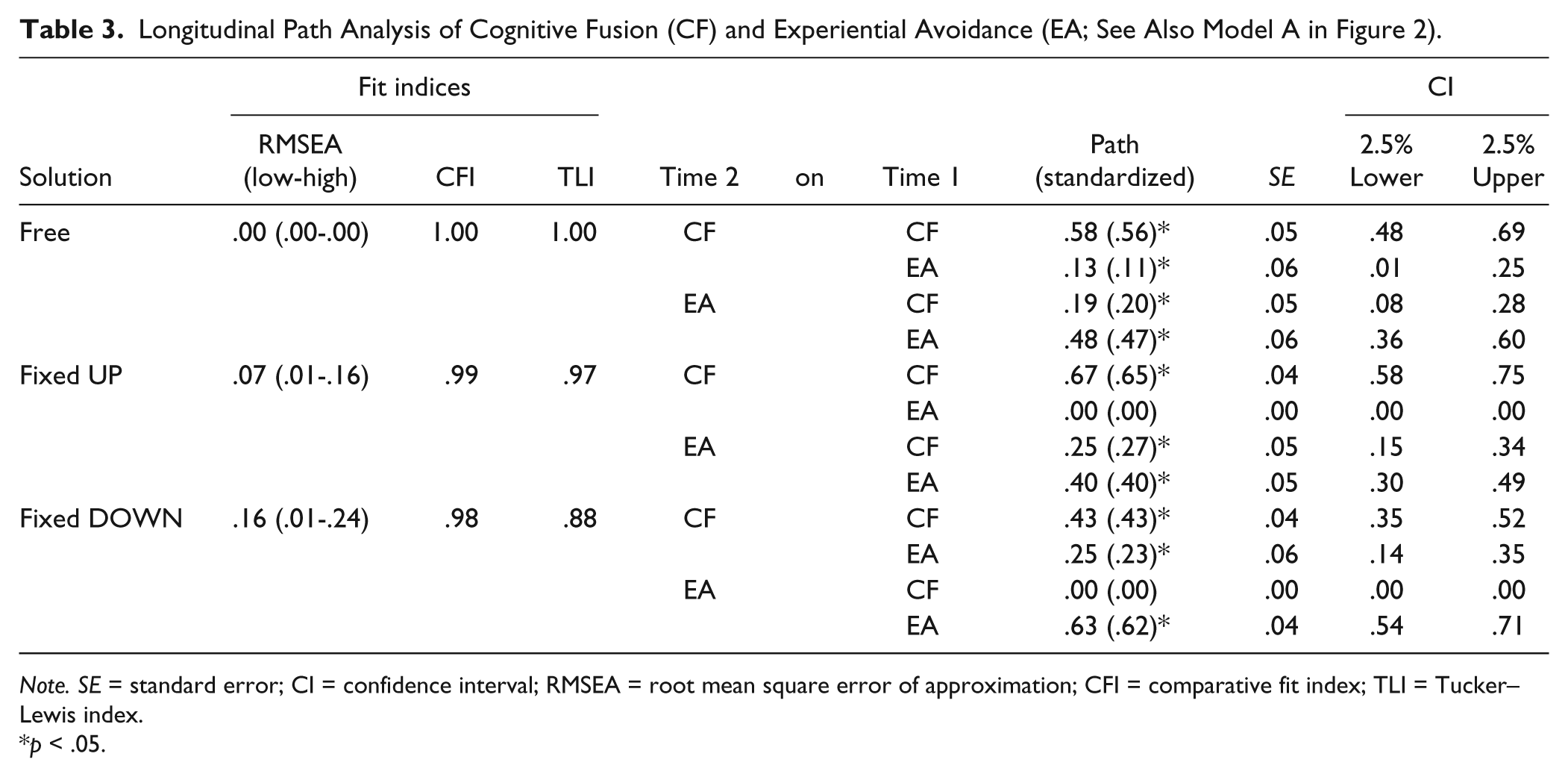
Note. SE = standard error; CI = confidence interval; RMSEA = root mean square error of approximation; CFI = comparative fit index; TLI = Tucker–Lewis index.
p < .05.
Longitudinal Path Analysis of Cognitive Fusion (CF), Experiential Avoidance (EA), and Depression (See Also Model B in Figure 2).
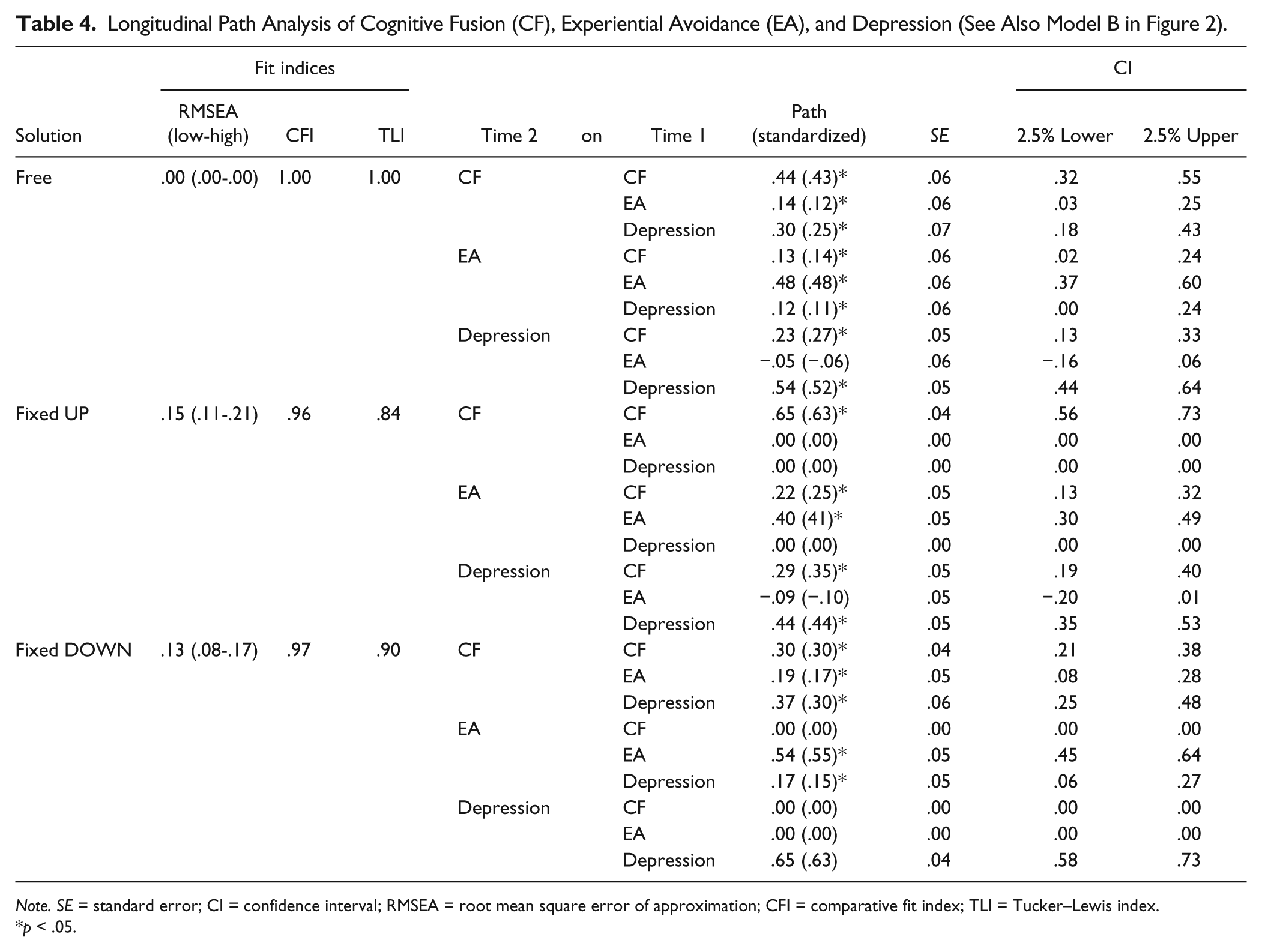
Note. SE = standard error; CI = confidence interval; RMSEA = root mean square error of approximation; CFI = comparative fit index; TLI = Tucker–Lewis index.
p < .05.
Longitudinal Path Analysis of Cognitive Fusion (CF), Experiential Avoidance (EA), and Satisfaction With Life (SWL; See Also Model C in Figure 2).
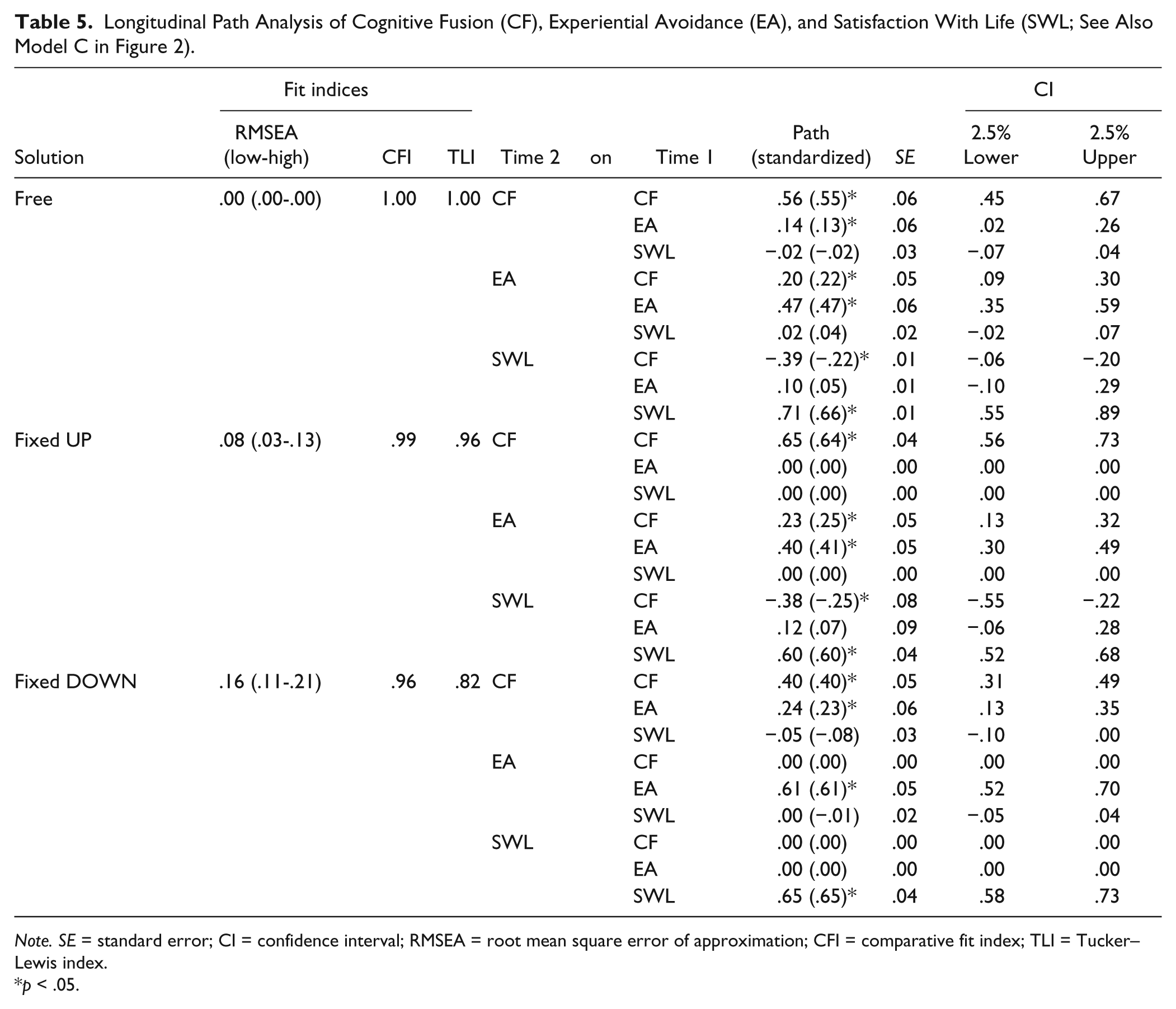
Note. SE = standard error; CI = confidence interval; RMSEA = root mean square error of approximation; CFI = comparative fit index; TLI = Tucker–Lewis index.
p < .05.
Within Model A (see Figure 2 and Table 3), we established an UP path with CF as the predictor of EA; and a DOWN path with EA as the predictor of CF. In the free solution, all the relations were positive and significant. Consequently, the relation between EA and CF was significant in both directions. However, we note that the effect size was higher when EA predicted CF (β = .20, p < .05) than the other way around (β = .11, p < .05). Additionally, the log-likelihood test showed that the UP and DOWN solutions were both significantly worse than the free solution (Δχ2 = 3.916, p < .05; and Δχ2 = 13.806, p < .01, respectively). This suggests that the relation between CF and EA was nonrecursive, in other words, they maintained a bidirectional relation. The correlation between CF and EA was high (r = .49, p < .05), and the explained variance was 42.3% for CF and 40.3% for EA.
As compared with Model A, within Model B (see Figure 2 and Table 4), the UP path also included CF and EA as predictors of Depression; and the DOWN path also included Depression as predictor of CF and EA. As with the concurrent validity results, Depression was explained by CF (β = .27, p < .05) but not by EA (β = −.06, p > .05). The comparison of the different solutions (free and fixed) showed a nonrecursive effect between CF and EA, and between CF and Depression (DOWN [Δχ2 = 22.827, p < .01] and UP [Δχ2 = 34.410, p < .01], respectively). The explained variance was 46.5% for CF, 41.3% for EA, and 44.7% for Depression.
Last, as compared with Model A, within Model C (see Figure 2 and Table 5), the UP path also included CF and EA as predictors of SWL; and the DOWN path also included SWL as predictor of CF and EA. In this case, results differed from those in the concurrent validity study, that is, only CF but not EA explained SWL (β = −.22, p < .05). Furthermore, SWL did not explain either CF or EA (ps > .05). Thus, we only found a nonrecursive relation between CF and EA (DOWN [Δχ2 = 34.973, p < .01]; UP [Δχ2 = 10.651, p < .01]). The explained variance was 41.9% for CF, 40.4% for EA, and 52.5% for SWL.
Discussion
The goal of the present study was to analyze the psychometric properties of the Spanish version of the AFQ-Y with a sample of Spanish adolescents.
Overall, the psychometric properties of the instrument were good when considering a correlational two-factor structure with method effects. At first, the analysis of the factor structure yielded inconclusive results, as in the validation of the original instrument (Greco et al., 2008). None of the tested factorial solutions (one-factor and two-factor) were satisfactory, leading us to incorporate method effects possibly related to the wording of the items. One of these method effects related to the need to somehow control or suppress unwanted emotions, the other method effect related to the actual act of suppressing such unwanted emotions as a way of feeling better or relieved. We note that the items containing the method effects in our study were the same items that Greco et al. (2008) removed from the original version to develop the shorter eight-item version that, in fact, proved unidimensional. Thus, the method effects in the original scale may have masked the identification of the CF and EA factors, which showed good reliability in our study. Future research will confirm the occurrence of method effects in this scale, whether they coincide with those we identified, and whether the method effects we found relate to issues other than the wording of the items, such as random features of the sample or the presence of subfactors.
Our results support the instrument’s concurrent validity, with total AFQ-Y scores correlating positively with depression symptomatology and negatively with SWL, as expected. A closer look at the data yields interesting results. CF and EA scores correlated differentially with our outcome variables. On the one hand, CF correlated positively with Depression and negatively with SWL. This is, the more the adolescents regarded thoughts and feelings as believable and good reasons to behave (i.e., CF), the more they reported feeling depressed and dissatisfied with their lives. This result is in line with the model and the empirical evidence on CF as a source of suffering (Gillanders et al., 2014; Herzberg et al., 2012). On the other hand, EA only correlated with SWL and did so positively. That is, the more the adolescents reported suppressing unwanted thoughts and feelings (i.e., EA), the more they reported being satisfied with their lives. This finding may seem to contradict the model, which regards EA as a transdiagnostic process present in many psychopathologies (Hayes et al., 1996; Kashdan et al., 2006). Tentatively, however, this may be related to (a) the instant relief that EA provides from the distress produced by unwanted thoughts and feelings (Hayes et al., 1996) and (b) the feeling of being in control of one’s life that EA produces (e.g., Hayes et al., 1996; Luciano et al., 2004). In colloquial terms, the distress adolescents experience as they entangle with the content of their negative thoughts and feelings improves as they do something to avoid or escape from such thoughts and feelings. This result also implies that EA at nonclinical levels, as in our sample, may be an adaptive coping strategy. As a matter of fact, avoidance of thoughts and feelings is common and only becomes a problem when it is generalized and occurs regardless of its workability in the long run. All in all, although the CFA yielded inconclusive data regarding the superiority of one of the two solutions tested, the analysis of the concurrent validity of the instrument seems to support the idea that the Spanish AFQ-Y assesses two factors that, although intimately related, may produce different patterns of relations with different aspects of well-being.
Considering convergent validity results, the predictive validity of the scale was tested for the two-factor solution by conducting a path analysis. The results showed that CF predicted EA, Depression, and SWL. However, EA only predicted CF, showing a nonrecursive pattern of influence. In other words, increased levels of CF predicted EA, and in turn, the predominant use of avoidance as an emotion regulation strategy led to increased levels of CF. The fact that the relation between CF and EA proved to be nonrecursive implies that whereas avoiding may momentarily reduce suffering, leading to increased SWL (see convergent validity results), its maintenance over time leads to increased CF, which predicts depression and diminished SWL (see predictive validity results).
Our findings, both cross-sectional and longitudinal, have important theoretical and clinical implications. As for the former, our study yields empirical support to the notion that CF and EA are two distinct processes that, nonetheless, are closely related and mutually contribute to each other. As mentioned before, the fundamental tenet of the TWBT is that thoughts and feelings are not the causes of behavior (e.g., Hayes et al., 2006). The same goes for thoughts and feelings that are experienced as aversive or threatening, such as “I look stupid” or “I’m not worth it,” although they seem like very good reasons to do something (e.g., turn away or withdraw). Within this approach, acting rigidly on the content of thoughts and feelings regardless of its long-term workability is the result of, at least, two processes, namely, CF and EA.
It is through CF that we take the content of the thought and/or feeling as a fundamental truth. CF is an adaptive process that allows the survival of the human species (Hayes et al., 2006). Our community teaches us to take words literally because this is good for survival. It is because literality is highly useful in our daily lives that we also use it when it comes to thoughts and feelings about ourselves and about the world around us. There is fusion in the act of believing “I am not worth it” as a fundamental truth about oneself. There is also fusion in the act of believing “My life will improve when I manage to control my fears” as a fundamental truth about life. However, if the person became fused to the content of the latter thought, she would probably act on it by trying somehow to make her fears go away. This is an example of EA that may become problematic if the only reason to engage in most daily activities is to get rid of unwanted thoughts and feelings. As an emotion regulation strategy, EA may become highly pervasive because of the instant relief it produces (Luciano et al., 2004).
Indeed, looking for causes and acting on them is also highly adaptive during the normal socialization process (Hayes et al., 2006; Luciano et al., 2004), as it is the basis of problem-solving behavior. But there is a setback: The very act of acting on what we believe is the cause and actually solving the problem strengthens the whole rationale supporting such problem solving. In the applied domain, the fact that a person down-regulates her negative affect and then feels better or relieved and continues with her daily routine reinforces the whole rationale sustaining the down-regulation, namely: (a) there is a reason for my suffering; (b) the conclusion, “I suffer because of my thoughts and feelings” is right; and (c) acting on my thoughts and feelings is the right thing to do before I can continue with my daily routine. Generally speaking, EA, which is usually regarded as the result of CF, is also the process that strengthens CF (for a detailed discussion, see Hayes et al., 1996; Luciano et al., 2004). Our results provide empirical support to the notion that CF and EA are two distinct processes that contribute to each other in a sort of vicious cycle (for similar results in the context of PI in chronic pain, see McCracken, Vowles, & Eccleston, 2004).
Our findings have important clinical implications as well. The cross-sectional data inform that CF, and not EA, is the process that relates to more depressive symptoms and diminished SWL. Furthermore, the longitudinal data reveal that EA nurtures CF, which in turn, contributes to enhanced EA, increased depressive symptomatology, and diminished SWL. Hence, it seems that CF should be the core target in therapy. We note, however, that the relation between CF and EA proved to be nonrecursive. That is, CF contributes to lower SWL, but EA strengthens CF. In line with this, treatment and prevention programs should focus on altering the behavior of inflexibly acting on negative thoughts and feelings as if their content were fundamental truths and good reasons to behave. This is the focus of Acceptance and Commitment Therapy (ACT; Hayes, Strosahl, & Wilson, 1999, 2012), which is proving to be useful in a number of domains (for a recent review, see Ruiz, 2010). One of these domains relates to children, adolescents, and their parents. Although ACT–consistent work with these populations is still in its infancy, the evidence so far is promising (for a review, see Coyne, McHugh, & Martinez, 2011).
We note that the purpose of the present study was to validate the Spanish version of the AFQ-Y. With this in mind, we only collected measures in two periods. Thus, the aforementioned theoretical and clinical implications are only tentative, and further confirmatory analyses, including larger samples and larger longitudinal designs, are necessary to establish moderation or mediation effects and clarify the observed nonrecursive pattern of influence. This is the first time the AFQ-Y has been used with a Spanish sample of nonclinical adolescents, and the results suggest that there are no cultural or linguistic factors influencing the model. But future validation studies with diverse adolescent samples, including clinical samples, are needed before we can affirm that processes such as PI, CF, and EA are universal. To conclude, we assert that the Spanish adaptation of the AFQ-Y has good psychometric properties and can be used to detect the tendency toward CF as well as the predominant use of EA in nonclinical Spanish-speaking adolescents. In this sense, the instrument could be used to identify those Spanish adolescents whose present tendencies might become problematic if maintained over time.
Footnotes
Appendix
Acknowledgements
We thank Beatriz Sebastián and David Carralero for their assistance during questionnaires administration.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially supported by grants from the Fundación Universitaria Antonio Gargallo and Obra Social Ibercaja (ref. 2012/B007; ref. 2013/B005); and Department of Industry and Innovation, Government of Aragon, Spain (ref. S114).