
Abstract
Risky behaviors increase the likelihood of premature death, long-term disability, and poor mental health outcomes. Most current measures of risky behavior only assess behaviors within a single domain, fail to evaluate affective triggers for engaging in these behaviors, do not index the consequences of these behaviors, and are often limited to a narrow developmental period. The present study developed and evaluated a new 38-item questionnaire-based measure, the Risky, Impulsive, and Self-Destructive Behavior Questionnaire (RISQ), designed to address each of these limitations by expanding the breadth and depth of previous questionnaires. A bifactor model with a general factor and eight domain-specific factors (measuring drug use, aggression, self-harm, gambling, risky sexual behavior, impulsive eating, heavy alcohol use, and reckless behavior) best fit the RISQ, and indicators of internal consistency, as well as, construct validity were strong. Results provide initial validation for the RISQ as a broad, yet relatively brief, measure that quantifies and qualifies risky behaviors by assessing the severity, chronicity, and triggers for a range of harmful behaviors.
Keywords
Risky and self-destructive behaviors exact staggering costs on society by increasing the likelihood of premature death, long-term disability, and poor mental health outcomes (e.g., Moffitt et al., 2011). To date, research on this topic has largely taken a piecemeal approach and studied different types of risky and self-destructive behaviors in isolation. Although informative, this approach ignores the frequent co-occurrence of these behaviors (Thomsen, Stander, McWhorter, Rabenhorst, & Milner, 2011), may obscure common mechanisms that contribute to this spectrum of behaviors (e.g., Zuckerman & Kuhlman, 2000), and provides a circumscribed assessment of an individual’s propensity to engage in high-risk behaviors. Currently available assessments also fall short in a number of other important ways: (a) they commonly focus on behavior within a single domain, (b) they fail to evaluate the affective triggers for engaging in risky and self-destructive behaviors, (c) most scales do not index the consequences of these behaviors, and (d) they tend to only assess behaviors during a limited developmental period. The goals of the present study were to develop a new self-report measure, the Risky, Impulsive, and Self-destructive Behavior Questionnaire (RISQ), which was designed to address each of these limitations by surveying a range of risky and self-destructive behaviors and assessing affective triggers for engaging in them.
Types of Risky Behaviors
Risky and self-destructive behaviors involve the implementation of behavioral options that place individuals at substantial risk of harm (Steinberg, 2008) and reflect the tendency to execute harmful behaviors without considering the negative consequences that may occur (Horvath & Zuckerman, 1993). From an assessment standpoint, a wide range of behaviors could qualify as risky or self-destructive based on this definition. For example, some individuals take safety risks by acting aggressively, engaging in nonsuicidal self-injury or driving recklessly, while others take financial risks by making large gambling bets or dangerous investments; some individuals take health risks by using illegal drugs or binge eating, while others may partake in risky sexual behavior or criminal activity. In addition to variation in the types of risks people take, some behaviors are intended to deliberately inflict harm on oneself (e.g., suicidal behavior), whereas others could result in harm, but are not necessarily intended to do so (e.g., gambling).
Currently available behavior-based measures typically assess a single behavioral domain in depth (e.g., Subtypes of Antisocial Behavior Scale, Michigan Assessment–Screening for Alcohol and Drugs). While this type of approach provides a nuanced examination of dimensions within a single behavioral domain, it does not take into account the high rate of co-occurrence among risk-taking behaviors (Baskin-Sommers & Sommers, 2006; MacArthur et al., 2012). Consequently, a handful of scales attempt to provide a broad assessment of risk taking, measuring multiple behaviors within a single measure. The Cognitive Appraisal of Risky Events (Fromme, Katz, & Rivet, 1997) and Domain-Specific Risk-Taking (DOSPERT; Blais & Weber, 2006) scales both assess engagement in risky behaviors across multiple domains (e.g., illicit drug use, risky sexual activities, extreme sports, academic/work behaviors). Although these scales cover a range of risky activities, the behaviors assessed fall at the low to moderate end of the severity spectrum (e.g., destroying property is the most serious illegal behavior assessed on the Cognitive Appraisal of Risky Events) and, consequently, do not index behaviors with the greatest risk of harm that would be of interest to researchers in medical and forensic settings. For example, suicidal behavior, binge eating, and violent crime are conceptually and empirically linked to risk taking and impulsivity (e.g., Hamza, Willoughby, & Heffer, 2015; Murphy, Stojek, & MacKillop, 2014), but are not represented on these scales.
Alternatively, personality-based assessments conceptualize risk-taking as a trait and are developed to measure a latent construct that captures chronic risk-taking tendencies. For example, the externalizing spectrum is thought to reflect a heritable predisposition to diverse forms of disinhibition (Krueger et al., 2002) and is measured as the common variance among disinhibited psychiatric disorders (e.g., adult antisocial behavior, substance disorders) and personality traits/temperaments (e.g., Externalizing Spectrum Inventory, Krueger, Markon, Patrick, Benning, & Kramer, 2007). However, unlike behavior-based measures, these trait-based scales assume all risky behaviors have a common underlying etiology (e.g., trait impulsivity). Furthermore, they do not assess the frequency of the behavior, rarely specify a time frame for assessment, and often rely on subjective interpretations of how much a particular trait or behavior describes the individual (e.g., Likert-type scales ranging from very false to very true).
Taken together, existing behavior- and personality-based measures are either too specific (i.e., single behavioral domain) or too general (i.e., many behaviors but do not specify the frequency of the behaviors or exclude high severity behaviors). Thus, there is a gap in the literature for researchers who are interested in a relatively short measure that assesses a range of risky and self-destructive behaviors, including those with serious financial, health, and social consequences.
Affective Triggers for Risky Behavior
Research shows that risk-taking and impulsivity are likely to occur in the context of intense emotions, although the affective states that drive different behaviors vary across individuals (Loewenstein, Weber, Hsee, & Welch, 2001). Historically, numerous theoretical conceptualizations of risky, impulsive, and self-destructive behaviors have been proffered, but most fundamentally, they all center on the broad tenets of approach and avoidance. For example, conceptualizations of risky and impulsive behavior often stress individual differences in pleasure seeking (pleasurable, thrilling, or exciting experiences; Horvath & Zuckerman, 1993; Zuckerman & Kuhlman, 2000) or distress tolerance (reduce or relieve negative affective states, such as extreme distress, sadness, and anger; Leyro, Zvolensky, & Bernstein, 2010; Nock, 2010) as important in the development and maintenance of risky and impulsive behaviors. For some individuals, the tendency to engage in high-risk behaviors is motivated by thrill or pleasure seeking, for others, it is motivated by an inability to tolerate distress, and for a subset of individuals, it can be motived by a combination of these affective drives. Evaluating diversity in the affective triggers for these behaviors may be useful for characterizing the motivations behind risky and self-destructive behavior that differ in their etiological and reinforcement mechanisms.
Despite the abundance of evidence implicating approach-avoidance tendencies in risky behaviors, few assessments directly measure these tendencies and none directly measure these tendencies in conjunction with the associated behaviors. Assessing these triggers for risky and self-destructive behaviors is of fundamental importance for disentangling the processes that initiate and maintain them.
Severity of Risky Behavior
Risk-taking behaviors are quite normative. For instance, most people have violated speed limits and misused substances; and many have even engaged in more serious behaviors, including interpersonal violence and theft. In the majority of these cases, though, the behavior does not generate public concern. One key factor in determining the severity of behavior is not only in its frequency but also its likelihood of future negative outcomes. Perceived consequences has been identified as an important predictor of a variety of risky behaviors, sustained engagement of risky and self-destructive behaviors, and response to treatments aimed at reducing such behaviors (e.g., Parsons, Siegel, & Cousins, 1997). In this way, negative consequences from past behavior can serve as a proxy for evaluating the severity of the functional impairment that is present and may be used to differentiate more serious forms of self-destructive behavior from less pathological presentations (McCarthy, Pedersen, & Leuty, 2005). Unfortunately, current assessments fail to include an evaluation of the perceived consequences of past behavior, such as inpatient hospitalization, legal trouble, or relationship problems.
Chronicity of Risky Behavior
Risk-taking behavior is developmentally appropriate and desistance generally occurs naturally through maturation. However, for a subset of individuals, risk-taking and self-destructive behavior can persist, or even start, in adulthood. Therefore, there are important individual differences in the onset and chronicity of such behaviors. Despite this, most measures are designed to evaluate risky behaviors within a circumscribed developmental period (e.g., Youth Risk Behavior Survey) and do not evaluate when a particular behavior started (e.g., childhood or adulthood). Though separate measures given at different developmental periods may tap similar constructs, this approach fails to assess the onset, persistence, and desistance of behavior. Capturing the full career of risk- taking, within specific behaviors, is important to understand the natural history of risky, self-destructive, and impulsive behaviors for a given individual. For instance, age of onset is a known predictor of chronic problems (e.g., McGue & Iacono, 2014) and, thus, can be a useful indicator for differentiating trajectories of engagement in risky and self-destructive behavior. The limited scope of existing assessments, however, would necessitate the administration of multiple questionnaires to evaluate past and current behaviors. Therefore, assessing lifetime frequency, recent engagement in behavior, and age of onset in a single measure would provide a complete description of behavioral trajectories.
The Present Measure: RISQ
This study sought to address the limitations of existing measures by developing and validating a relatively brief assessment tool that captures the complexity of risky and self-destructive behaviors and is broad enough for a wide range of respondents, researchers, and professionals. The specific aims of the study were to examine the factor structure of the RISQ and evaluate its construct validity. This scale was designed to index a diverse range of behaviors and their associated affective triggers, consequences, and chronicity. These elements are often interrelated, and it is important to understand each component in order to obtain a comprehensive assessment. To evaluate these components separately, unfortunately, misleadingly parses factors that are not necessarily discrete.
Method
Participants
Community Sample
Participants consisted of 183 men (60%) and women (40%) ages 18 to 66 (M = 36.6, SD = 13.9) recruited from the general community through flyers in New Haven County, Connecticut and Internet advertisements posted nationally. Individuals age 18 or older were eligible to participate. The majority of the sample self-identified as White (58%), followed by Black/African American (32%), mixed racial identity (5%), and Asian (5%). Fifty-six percent was employed either full-time or part-time, with the remainder unemployed (36%), on disability (6%), or retired (2%). Educational attainment was as follows: 32% high school diploma, GED, or less, 50% vocational school, some college or Bachelor’s degree, and 18% graduate work or degree. Two participants were excluded due to invalid response profile on the Personality Assessment Inventory (PAI; >3 SDs from the mean on the inconsistency, infrequency, negative impression, and positive impression scales), resulting in a final sample of size of 181.
Student Sample
The second sample consisted of 259 men (28%) and women (72%) ages 18 to 55 (M = 23.1, SD = 5.6). Participants were recruited online via an anonymous link to the survey, which was distributed through e-mail to students enrolled in colleges nationwide. Individuals age 18 or older were eligible to participate. The majority of the sample self-identified as White (64%), followed by Asian (16%), Black/African American (9%), mixed racial identity (12%), American Indian (<1%), and Native Hawaiian/Pacific Islander (<1%). Educational attainment was as follows: 15% high school diploma, GED, or less, 56% some college or bachelor’s degree, and 29% graduate work or degree. One participant was excluded due to an invalid response profile on the PAI (>3 SDs from the mean on the validity scales), resulting in a final sample of size of 258.
Veteran Sample
A third sample consisted of 63 male (87%) and female (13%) military veterans ages 21 to 51 (M = 38.4, SD = 8.7). Participants were recruited from residential substance use treatment programs, outpatient psychotherapy groups, and flyers posted on the VA Boston hospital campus. Veterans who met the following criteria were eligible to participate: ages 18 to 55, past trauma exposure, and no history of a psychotic disorder. The majority of the sample self-identified as White (76%), followed by Black/African American (17%), mixed racial identity (5%), and Asian (2%). Forty-five percent was employed either full-time or part-time, with the remainder on disability (25%), unemployed (24%), retired (3%), or a full-time student (3%). Educational attainment was as follows: 22% high school diploma, GED, or less, 56% vocational school, some college or bachelor’s degree, and 22% graduate work or degree.
Procedures
Participants completed the measures either during a single in-person session or via a computer-based survey formatted on the Qualtrics system. Approval for the study was obtained from all relevant institutional review boards and regulatory committees. After a complete description of study procedures, written informed consent was obtained from participants.
Measures
Risky, Impulsive and Self-Destructive Behavior Questionnaire (RISQ)
In developing the RISQ, we sought to balance a theory-driven analysis of what behavioral domains are most representative of risky, impulsive, and self-destructive behavior (i.e., based on existing measures, strength of the empirical evidence, and core features of the construct) with a data-driven approach that allowed us to examine whether a range of behaviors, including those that are less commonly included in such a measure, are also relevant indicators. Thus, we started by generating categories of risky and self-destructive behaviors that are recognized and validated in the literature and then used factor analyses to assess whether the theory-based behavioral categories formed common reliable factors.
Development of the RISQ occurred in several stages. First, a thorough literature review was conducted to identify representative domains of risk-taking behavior. Literature searches using the terms and phrases “risky,” “risk-taking,” “impulsive,” “criminal behavior,” “self-destructive behavior,” “risk assessment,” and “impulsivity assessment” were performed in Google Scholar and PubMed. Ten domains of behaviors (illegal/criminal, alcohol, drug, gambling, eating, self-injury, aggression, sex, driving, and spending/financial) emerged as the most frequently studied. Second, based on these domains, a list of 49 questions was developed to quantify and assess a range of severity (mild, moderate, and severe) within each domain. Third, this list of 49 questions was sent to six colleagues nationwide in psychology, psychiatry, and sociology. Finally, based on feedback from colleagues, a final list of 44 items was maintained across the 10 domains of behavior and administered to three separate samples: students, community members, and veterans.
Participants responded to a set of 44 items that represented different risky and self-destructive behaviors. For each behavior, participants were asked to report: (a) How many times total have you done this in your life? (b) How many times have you done this in the past month? (c) How old were you the first time? and (d) Did it ever cause you any problems, such as going to the hospital, legal trouble, problems at work, with family or friends? Participants were also asked to rate on a 5-point Likert-type scale (0 = strongly disagree to 4 = strongly agree) how much they agreed with the following for each behavior endorsed: (e) I do this behavior to stop feeling upset, distressed, or overwhelmed and (f) I do this behavior to feel excitement, to get a thrill, or to feel pleasure. The last two questions were designed to assess Avoidance and Approach affective triggers for each behavior, respectively. The Avoidance scale assessed basic negative emotions (e.g., distress) and avoidance motivational impulses, whereas the Approach scale measured basic positive emotions and approach motivational impulses. A copy of the RISQ is available as part of supplementary materials (available online at http://asm.sagepub.com/content/by/supplemental-data).
Other Risky Behavior Measures
To examine construct validity, participants completed other self-report measures of risky and self-destructive behaviors. The community and student samples completed the: (a) DOSPERT Scale (Blais & Weber, 2006), the 90-item measure of 30 risk-taking behaviors was summed across five domains (financial decisions, health/safety, recreational, ethical, and social) to reflect the likelihood respondents might engage in risky activities (total score Cronbach’s alpha = .87); (b) Michigan Assessment–Screening Test for Alcohol and Drugs (MAST-AD 1 ; Westermeyer, Yargic, & Thuras, 2004), the 25-item measure of the consequences of alcohol and drug use was scored using the standard protocol (Cronbach’s alpha = .92); and (c) Reactive–Proactive Aggression Questionnaire (RPQ; Raine et al., 2006), the 23-item measure was summed to assess reactive (Cronbach’s alpha = .86) and proactive (Cronbach’s alpha = .88) aggression. The veteran sample competed the: (d) Mini International Neuropsychiatric Interview Suicide Scale (Roaldset, Linaker, & Bjørkly, 2012), a modified 7-item version of this scale was summed to assess lifetime history of suicidal thoughts and behaviors (Cronbach’s alpha = .90); (e) South Oaks Gambling Screen (Lesieur & Blume, 1987), a modified version of this measure was summed to reflect participants’ lifetime engagement in 13 different gambling activities (Cronbach’s alpha = .84); and (f) Three-Factor Eating Questionnaire (Stunkard & Messick, 1985), a modified 14-item version was summed to assess thoughts and behaviors related to uncontrolled eating (Cronbach’s alpha = .84) and emotional eating (Cronbach’s alpha = .79).
External Correlates
We administered a battery of questionnaires to examine the correlates of the RISQ. All participants completed the: (a) Dimensions of Anger Reactions–5 (Hawthorne, Mouthaan, Forbes, & Novaco, 2006), the 5-item questionnaire was summed to measure anger-related reactions and interference with social functioning over the past 4 weeks (Cronbach’s alpha = .87); (b) Distress Tolerance Scale (Simons & Gaher, 2005), the 15-item measure was summed to assess the ability to withstand negative physical and psychological states (Cronbach’s alpha = .93); (c) Mood and Anxiety Symptom Questionnaire–Mini (Clark & Watson, 1995), the 26-item questionnaire was summed to assess symptoms of anhedonic depression (Cronbach’s alpha = .86), anxious arousal (Cronbach’s alpha = .85), and general distress (Cronbach’s alpha = .91) in the past week; and (d) Behavioral Inhibition Scale/Behavioral Activation Scale (BIS/BAS; Carver & White, 1994), the 20-item measure was summed to assess the tendency to experience negative affect in response to threat (BIS; Cronbach’s alpha = .81) and to experience positive affect in response to reward (BAS; Cronbach’s alpha = .84). The community and student samples also completed the: (e) PAI (Morey, 1991) Borderline Personality Disorder scale (PAI-BPD; assessing affective instability, identity problems, negative relationships, and self-harm; Cronbach’s alpha = .80), Antisocial Personality Disorder scale (PAI-APD; assessing antisocial tendencies, stimulus seeking, and egocentricity; Cronbach’s alpha = .80), and Validity scales (PAI-Validity; assessing attempts to falsify or distort one’s mental state in self-reports); (f) Barratt Impulsiveness Scale–Brief (Steinberg, Sharp, Stanford, & Tharp, 2013), the 8-item measure was summed to assess impulsiveness across various situations (Cronbach’s alpha = .81); (g) Brief Sensation Seeking Scale (Hoyle, Stephenson, Palmgreen, Lorch, & Donohew, 2002), the 8-item measure was summed to assess risk-taking propensity and willingness to seek out novel sensations (Cronbach’s alpha = .79); (h) Exposure to Violence Questionnaire (Selner-O’Hagan, Kindlon, Buka, Raudenbush, & Earls, 1998), the 13-item measure was summed to assess direct and indirect exposure to violent victimization over the lifespan (total score Cronbach’s alpha = .85); and (i) Self-Regulation Questionnaire (Brown, Miller, & Lawendowski, 1999), the 63-item measure was summed to assess perceptions of self-regulatory capabilities (Cronbach’s alpha = .90).
Data Analyses
Factor Analyses
We used the lifetime behavior items in our factor analyses, because (a) we expected the factor structure to be more stable using a lifetime as opposed to a current (past month) time frame and (b) we expected the lifetime items to index more long-standing behavioral patterns, as opposed to the current items that would be more influenced by an individual’s present environmental context (e.g., residential treatment programs, probation or parole, etc.). Examination of the distribution of responses across items indicated that the items were positively skewed (values ranged from 7.1 to 22.4). To address this issue, we constrained the range of possible responses at the high end of the distribution by categorizing lifetime items into response bins: 0, 1 to 10, 11 to 50, 51 to 100, >100, which significantly reduced the skewness of the items (values ranged from 0.5 to 5.4).
A series of exploratory (EFA) and confirmatory (CFA) factor analyses were performed with the software program Mplus 7.11 (Muthén & Muthén, 2013) using the robust weighted least squares means and variance adjusted estimator. This estimator was selected, because it is appropriate for ordinal-level variables and allowed us to account for the nonnormal distribution of the data. Missing data were limited to a single item for one participant. Model fit was evaluated using standard fit indices as recommended by Hu and Bentler (1999), specifically root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), confirmatory fit index (CFI), and Tucker–Lewis index (TLI). We evaluated the measurement models based on the pattern of item loadings, interpretability of each solution, standard fit indices (RMSEA <.05, SRMR <.09, CFI and TLI ≥.95, indicating good model fit; Hu & Bentler, 1999), convergence with the hypothesized factor structure, and the comparisons of model fit using the likelihood ratio test. Thus, we selected the most well-fitting model based on a combination of the fit statistics and the conceptual framework that served as the basis of the RISQ. We calculated the likelihood ratio test using the Mplus DIFFTEST function to directly compare models.
Prior to conducting the factor analyses, the community, student, and veteran samples were combined and randomly divided into two split-half samples. We first estimated a series of EFAs in the first split-half sample (N = 250) to identify the common factors underlying the RISQ and to trim poor fitting items. Specifically, we removed items that did not load significantly on any factor, did not load on their respective hypothesized factor and/or cross-loaded on multiple factors. Next, we evaluated a bifactor rotated EFA that approximated a general factor and specific factors orthogonal to the general factor (Jennrich & Bentler, 2011). The bifactor model allowed us to examine both common variance across the RISQ items, such as general tendencies to engage in risky and self-destructive behavior, as well as unique sources of variance that may represent more specific expressions of this general tendency. In the bifactor model, each scale item is represented by a general source of shared variance across the items (i.e., general factor) and unique sources of variance shared by subsets of items that is not accounted for by the general factor (i.e., specific factors). We based the number of specific factors estimated in the EFA-based bifactor model on the results of the best-fitting EFA model to maximize the conceptual comparison of factors across models. Finally, to validate the EFA-derived factor structure and select the final model, we performed CFAs on the second split-half sample (N = 255) and evaluated the models using the fit statistics described above.
Construct Validity
We examined associations between the RISQ and other self-report measures to assess the instrument’s construct validity. These analyses were meant to be descriptive and to demonstrate that the RISQ correlates in expected ways with existing measures. With regard to the RISQ factors, we expected the strongest correlations to be between measures that assessed similar behaviors (e.g., RISQ Aggression with RPQ Aggression). With regard to the RISQ affective triggers scales, we expected the Avoidance scale to correlate most strongly with the scales that assess negative affect (Dimensions of Anger Reactions, Distress Tolerance Scale), avoidance motivation (BIS), and psychopathology symptoms characterized by negative emotionality (Mood and Anxiety Symptom Questionnaire, PAI-BPD). In contrast, we expected the RISQ Approach scale to correlate most strongly with scales that assess approach tendencies (BAS, trait sensation seeking). Finally, we expected certain measures to correlate broadly with the RISQ scales based on research showing they are general risk factors for risky and self-destructive behaviors, specifically exposure to violence and poor self-regulation (Ben-Zur, & Zeidner, 2009; de Ridder, Lensvelt-Mulders, Finkenauer, Stok, & Baumeister, 2012). Age was entered as a covariate in these analyses. Given the large sample size, only correlations with a p value less than .01 were interpreted.
Results
Factor Analyses: Scale Development
To identify the factor structure of the RISQ, we submitted the initial pool of 44 items to EFA and removed 6 items that did not load significantly on their hypothesized factor and/or cross-loaded on multiple factors. We then performed an EFA with the remaining 38 items and examined solutions with 1 to 9 factors. Model fit indices are summarized in Table 1. The single- and two-factor solutions did not achieve acceptable fit across multiple indices, and the three-factor model did not provide good fit according to the RMSEA and SRMR. Comparisons using the likelihood ratio tests indicated that models with four to nine factors all achieved significantly better fit relative to models with one less factor. However, the seven-factor model was rejected because the risky sexual behavior items cross-loaded with illegal behaviors and gambling, and the nine-factor model was rejected because only two of the risky sexual behavior items loaded uniquely on the last factor. The eight-factor model was the most interpretable solution, conformed most closely with the intended factor structure of the RISQ, and demonstrated excellent fit (RMSEA = .030, CFI = .992, TLI = .986, SRMR = .043). Standardized factor loadings for this model are presented in Table 2. The factors comprised the following: Illegal Behaviors (13 items), Aggression (5 items), Self-Harm (4 items), Gambling (4 items), Risky Sexual Behaviors (4 items), Heavy Alcohol Use (2 items), Impulsive Eating (2 items), and Reckless Behaviors (4 items). Thus, the eight-factor solution was the best fitting model from an empirical and theoretical standpoint.
Model Fit Statistics.
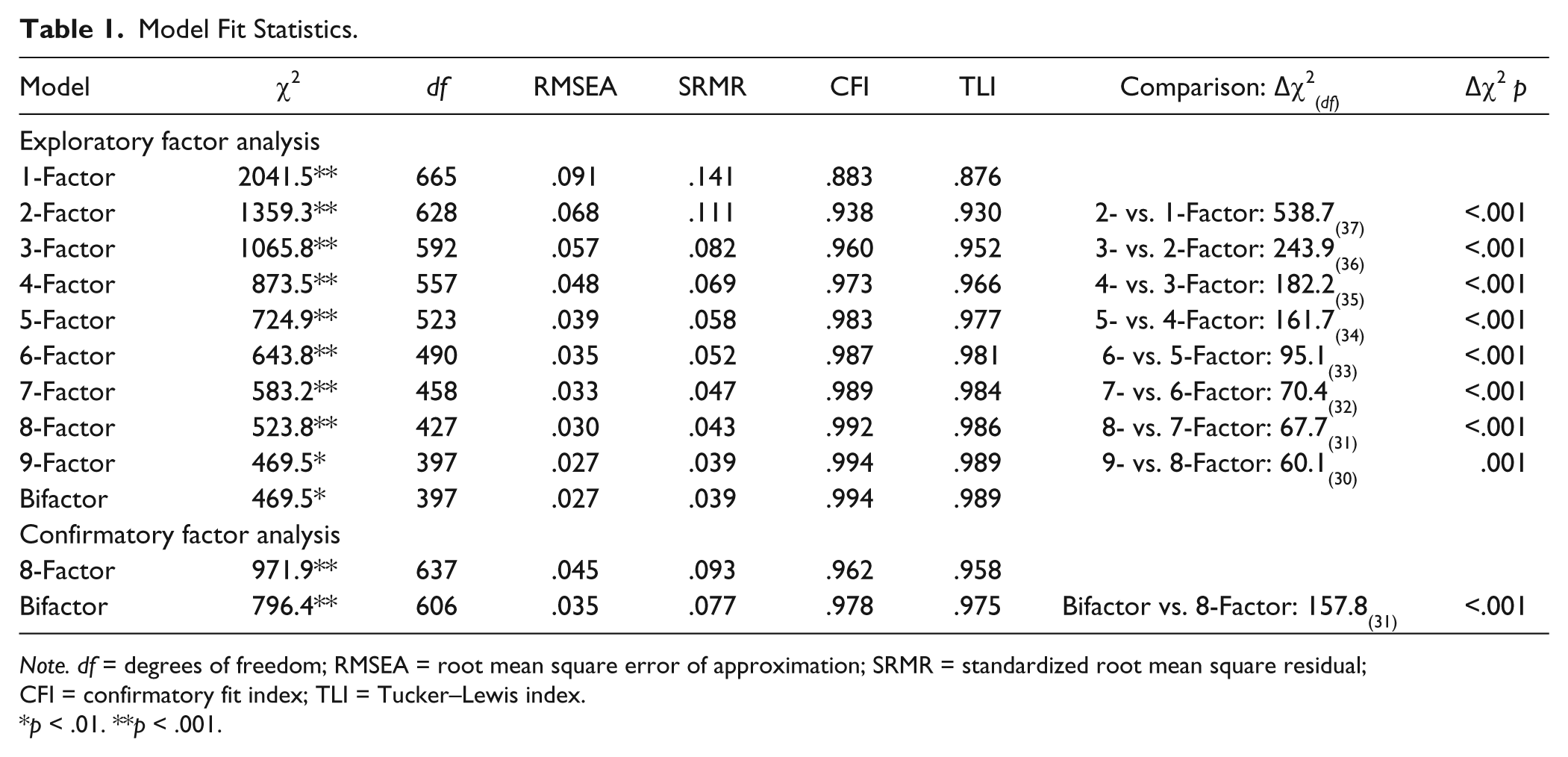
Note. df = degrees of freedom; RMSEA = root mean square error of approximation; SRMR = standardized root mean square residual; CFI = confirmatory fit index; TLI = Tucker–Lewis index.
p < .01. **p < .001.
Standardized Factor Loadings From the Exploratory Factor Analysis.
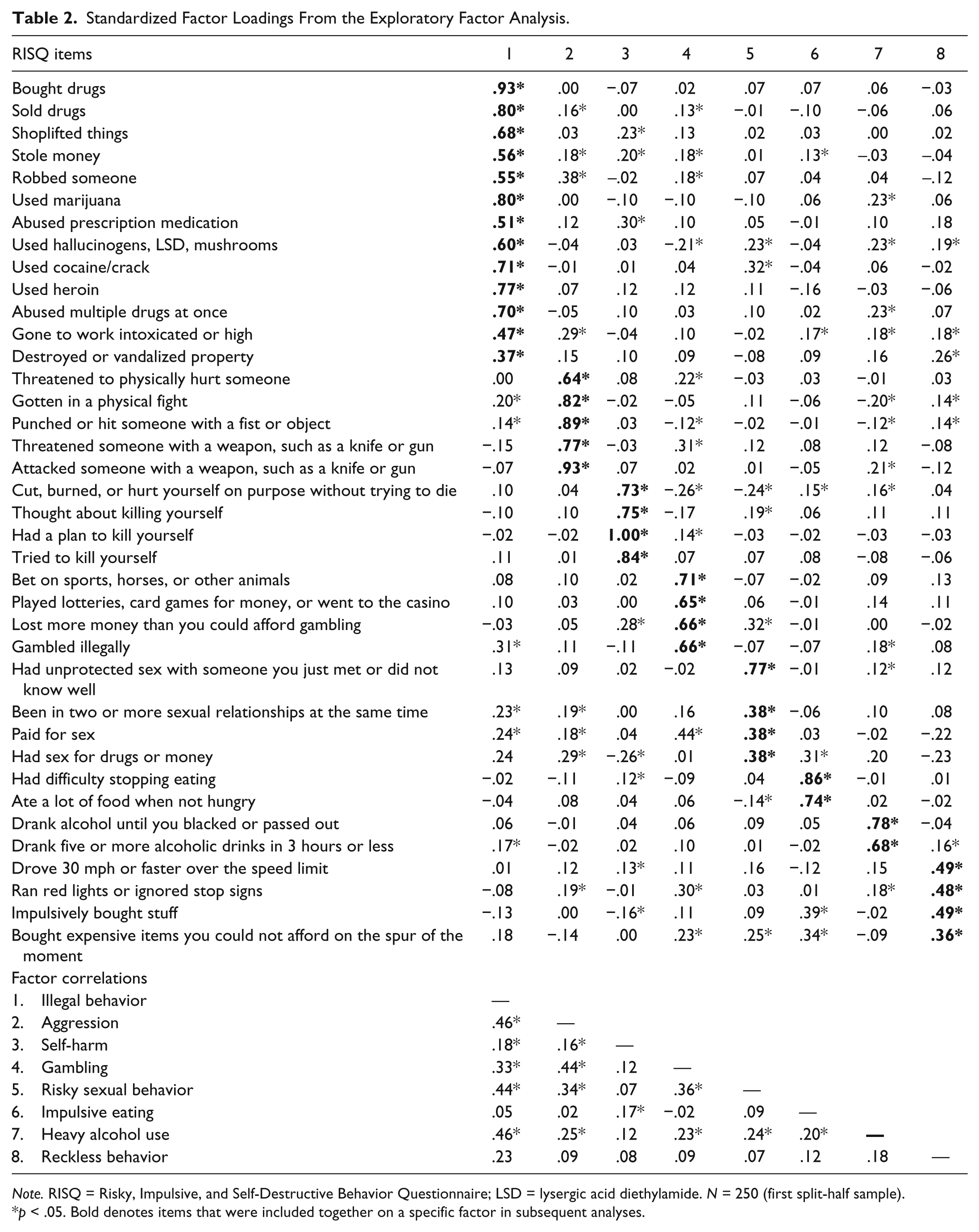
Note. RISQ = Risky, Impulsive, and Self-Destructive Behavior Questionnaire; LSD = lysergic acid diethylamide. N = 250 (first split-half sample).
p < .05. Bold denotes items that were included together on a specific factor in subsequent analyses.
Next, we estimated an EFA-based bifactor model with a general factor that captured shared variance across all of the RISQ items and the eight specific factors identified in the original EFA (see Table 2). The bifactor model achieved excellent fit across indices (RMSEA = .027, CFI = .994, TLI = .989, SRMR = .039), and standardized factors loadings are presented in Table 3. All of the items loaded significantly on a general factor, with the exception of the two impulsive eating items, which suggested these behaviors do not share variance with the other items on the RISQ. For the eight specific factors, the overall pattern of loadings paralleled those of the EFA model. The one exception to this was that several of the illegal behavior items (e.g., shoplifting, vandalism) loaded exclusively on the general factor in the bifactor model, and the remainder loaded together on a more specific Drug Behaviors Factor (eight items). Thus, results of the bifactor analysis suggested that drug behaviors reflect a distinct manifestation of risky behavior, whereas other illegal behaviors are captured by a general factor of risky and self-destructive behaviors. To determine which model was most appropriate to retain for further examination, we next compared model fit via CFAs in the second split-half sample.
Standardized Factor Loadings From the Bifactor Exploratory Factor Analysis.
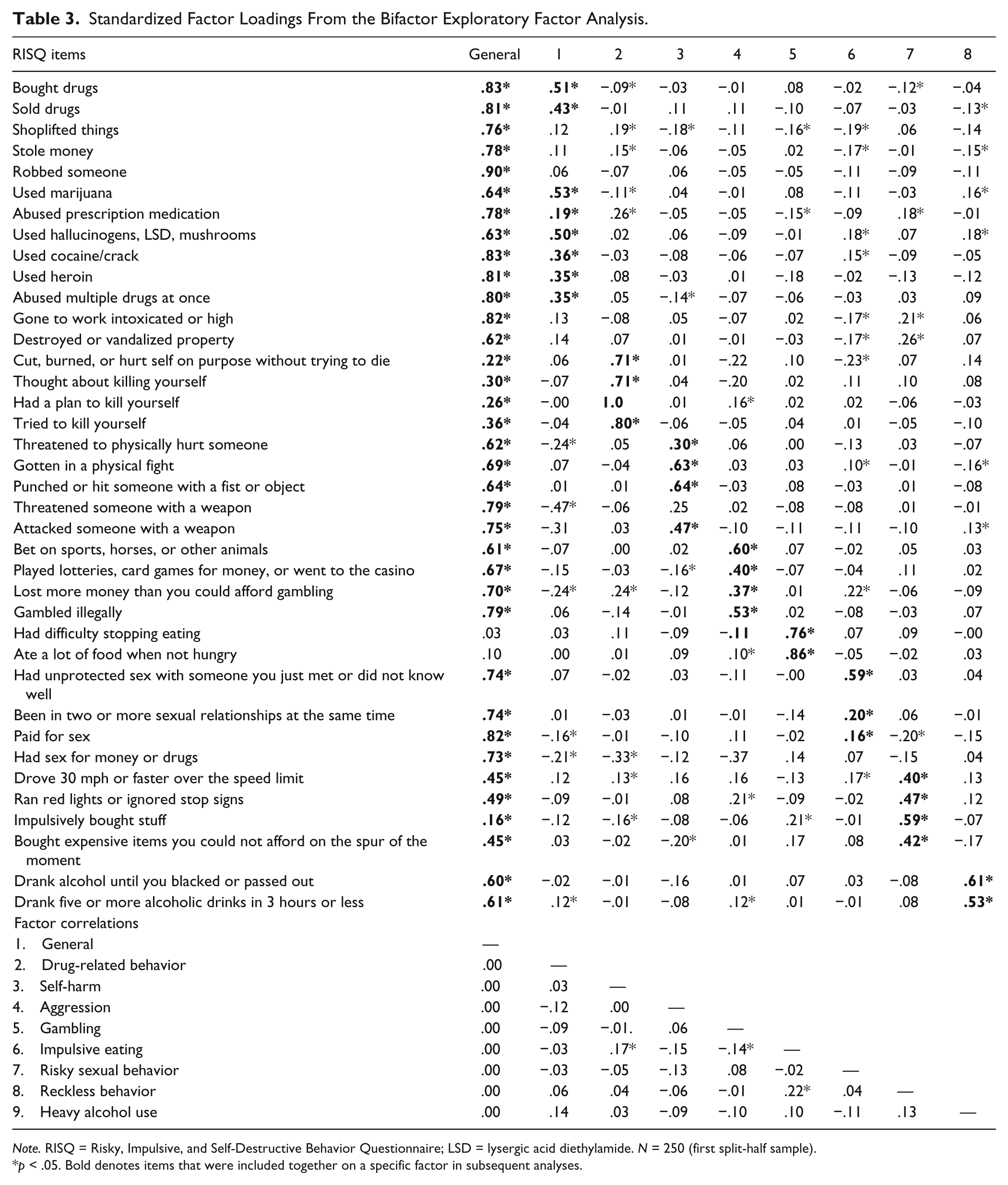
Note. RISQ = Risky, Impulsive, and Self-Destructive Behavior Questionnaire; LSD = lysergic acid diethylamide. N = 250 (first split-half sample).
p < .05. Bold denotes items that were included together on a specific factor in subsequent analyses.
Based on the EFAs, we compared a bifactor model consisting of one general factor (all items except the impulsive eating items) that was uncorrelated with eight specific factors (i.e., General Factor, Drug Behaviors, Self-Harm Behaviors, Aggression, Gambling, Risky Sexual Behaviors, Heavy Alcohol Use, Impulsive Eating, and Reckless Behaviors) with an eight-factor model that did not specify a general factor (i.e., Illegal Behaviors, Self-Harm Behaviors, Aggression, Gambling, Risky Sexual Behaviors, Heavy Alcohol Use, Impulsive Eating, and Reckless Behaviors). The model fit statistics for these analyses are summarized in the bottom of Table 1. The bifactor model demonstrated good model fit in the CFA (RMSEA = .035, CFI = .978, TLI = .975, SRMR = .077), and all of the intended RISQ items loaded significantly on the general factor (see Table 4 for standardized factor loadings). One item (“used heroin”) did not load significantly on its intended specific factor, but did load highly on the general factor. The fit indices for the bifactor model were slightly superior to the eight-factor model that did not specify a general factor (RMSEA = .045, CFI = .962, TLI = .958, SRMR = .093), and comparisons of the two models using the likelihood ratio tests indicated the bifactor model achieved significantly better fit. On the basis of these findings, the bifactor model was selected as the most well-fitting model and used in all subsequent analyses.
Standardized Factor Loadings From the Bifactor Confirmatory Factor Analysis.
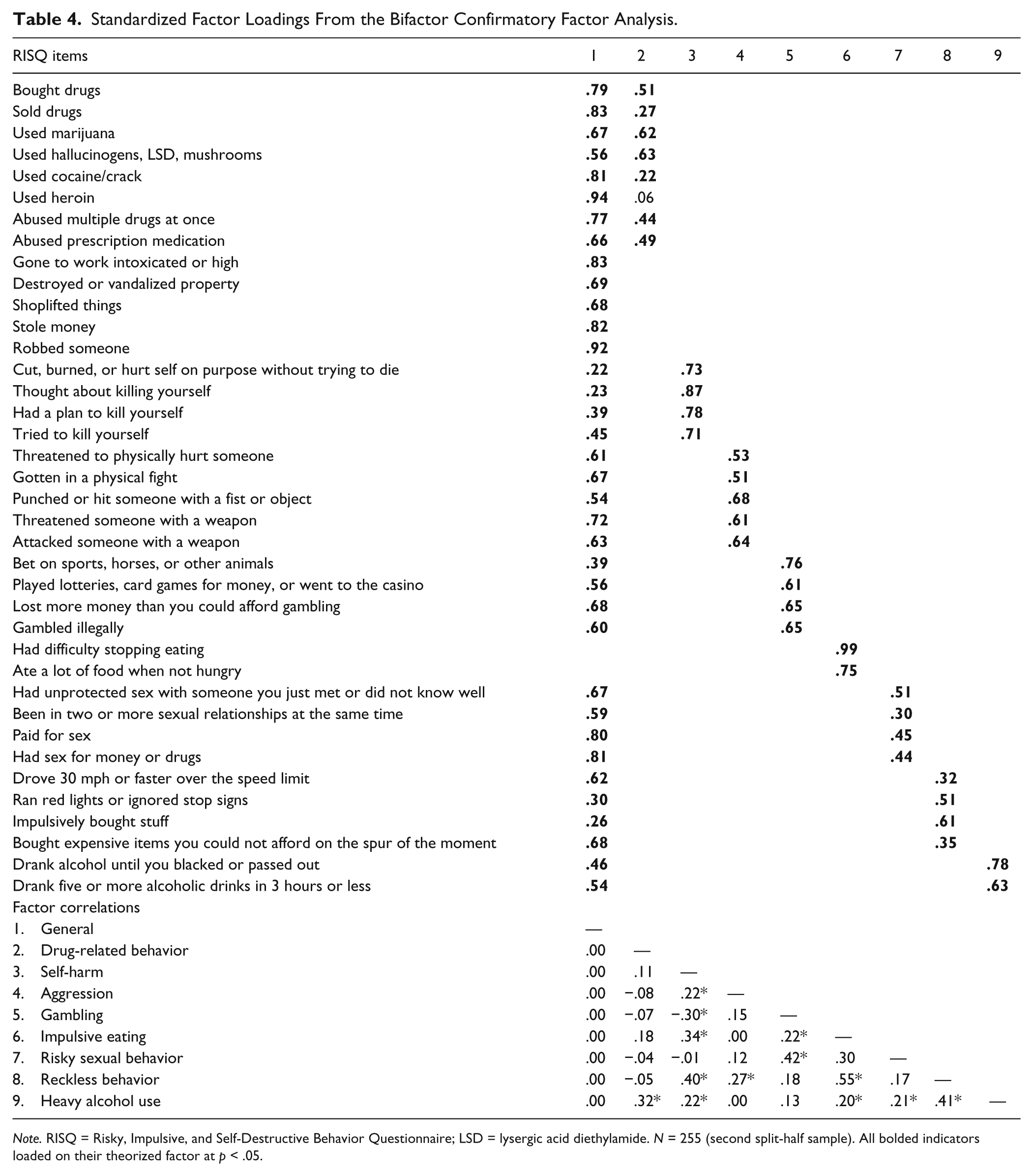
Note. RISQ = Risky, Impulsive, and Self-Destructive Behavior Questionnaire; LSD = lysergic acid diethylamide. N = 255 (second split-half sample). All bolded indicators loaded on their theorized factor at p < .05.
Internal Consistency
The scale showed excellent internal reliability for the total score (Cronbach’s alpha = .92) and acceptable to excellent reliability for each of the factors (.73-.92). The exception to this was the Reckless Behaviors factor, which showed borderline internal consistency (.63).
Demographic Correlates
Age showed a moderate positive association with lifetime frequency of behaviors (r = .46, p < .001), likely reflecting the fact that older participants had more opportunity to engage in the behaviors assessed by the RISQ. Consistent with this interpretation, total past month behavior was inversely correlated with age (r = −.14, p = .002). RISQ behaviors were negatively related to education (lifetime behaviors: r = −.12, p = .007; past month behaviors: r = −.16, p < .001) and evidenced gender differences (t = 6.9, p < .001), with men reporting more lifetime behaviors on average than women (M = 23.3, SD = 18.2 vs. M = 13.8, SD = 10.7, respectively).
Construct Validity
The correlations of the RISQ with other self-report measures of risky and self-destructive behaviors are presented in Table 5. As expected, RISQ total score was moderately correlated with the reported likelihood of future risk taking (DOSPERT); it was also associated with drug and alcohol related-problems (MAST-AD), proactive and reactive aggression (RPQ), and suicidal behavior (Mini-International Neuropsychiatric Interview [MINI]; rs = .34-.39). Several of the RISQ factors showed differential associations with the specific types of risky behavior they were intended to measure. For example, RISQ Aggression was most highly correlated with RPQ Proactive and Reactive Aggression (rs = .43-.45), RISQ Self-Harm was most highly correlated with the MINI Suicide Scale (r = .84), RISQ Gambling correlated most highly with previous gambling behavior on the South Oaks Gambling Screen (r = .65), RISQ Impulsive Eating correlated most highly with eating behavior on the Three-Factor Eating Questionnaire (rs = .44-.54), and RISQ Heavy Alcohol Use correlated with drug and alcohol problems on the MAST-AD (r = .33).
RISQ Convergent and Discriminant Validity With Risky and Impulsive Behaviors.
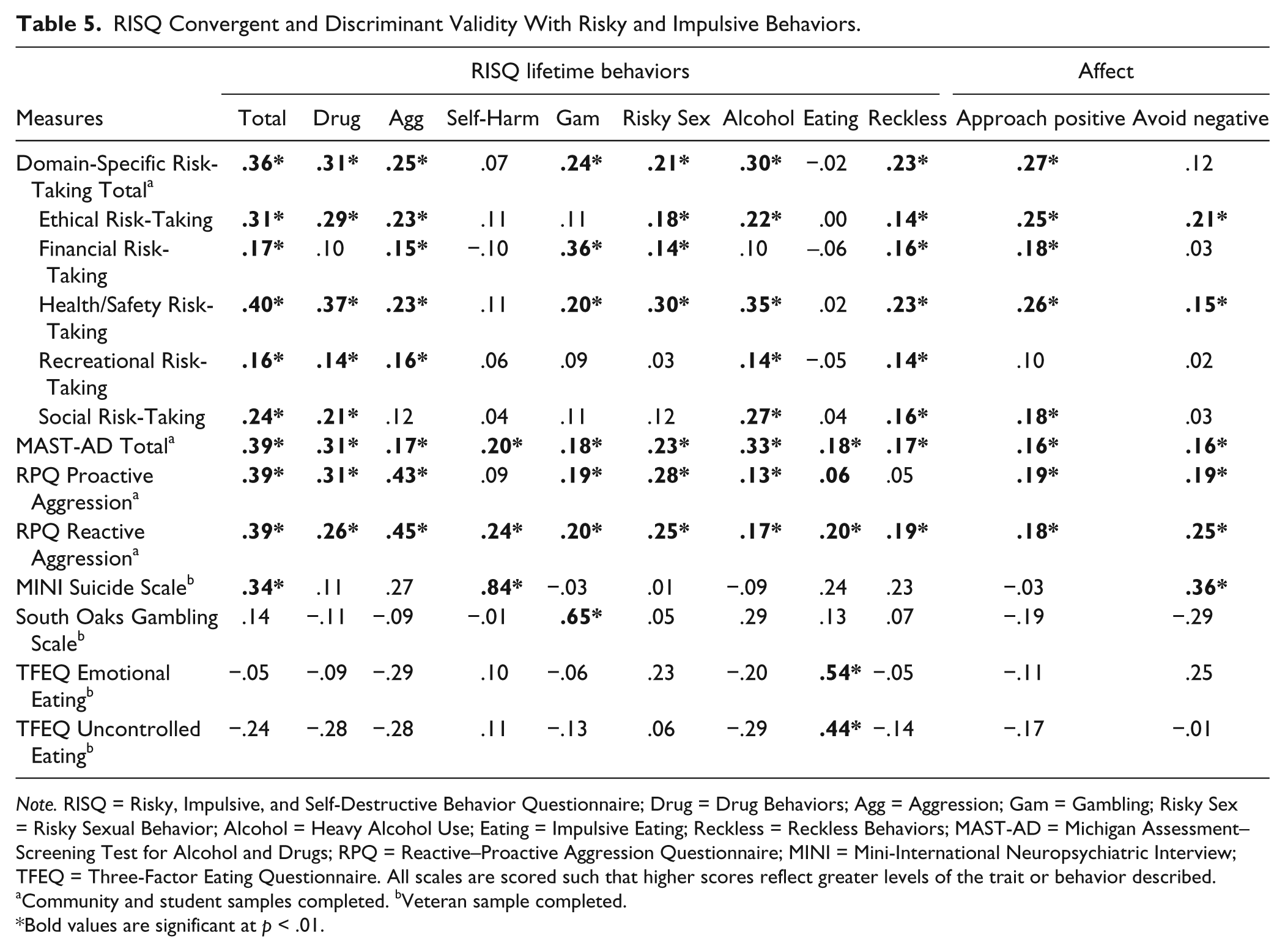
Note. RISQ = Risky, Impulsive, and Self-Destructive Behavior Questionnaire; Drug = Drug Behaviors; Agg = Aggression; Gam = Gambling; Risky Sex = Risky Sexual Behavior; Alcohol = Heavy Alcohol Use; Eating = Impulsive Eating; Reckless = Reckless Behaviors; MAST-AD = Michigan Assessment–Screening Test for Alcohol and Drugs; RPQ = Reactive–Proactive Aggression Questionnaire; MINI = Mini-International Neuropsychiatric Interview; TFEQ = Three-Factor Eating Questionnaire. All scales are scored such that higher scores reflect greater levels of the trait or behavior described.
Community and student samples completed. bVeteran sample completed.
Bold values are significant at p < .01.
A broader examination of the RISQ external correlates is presented in Table 6. As expected, RISQ total score evidenced stronger associations with disorders marked by elevated rates of risky and self-destructive behaviors, including borderline and antisocial personality disorder (rs = .37-.39), than less risky psychopathology symptoms, like anhedonic depression (rs = .11). It also correlated with sensation-seeking traits (r = .41). The RISQ factors showed varied associations with the external correlate measures, suggesting that they index distinct components of risky and self-destructive behavior. One notable finding is the consistently strong association between exposure to violence and the frequency of RISQ behaviors (total score rs = .50-.57).
RISQ External Correlates.
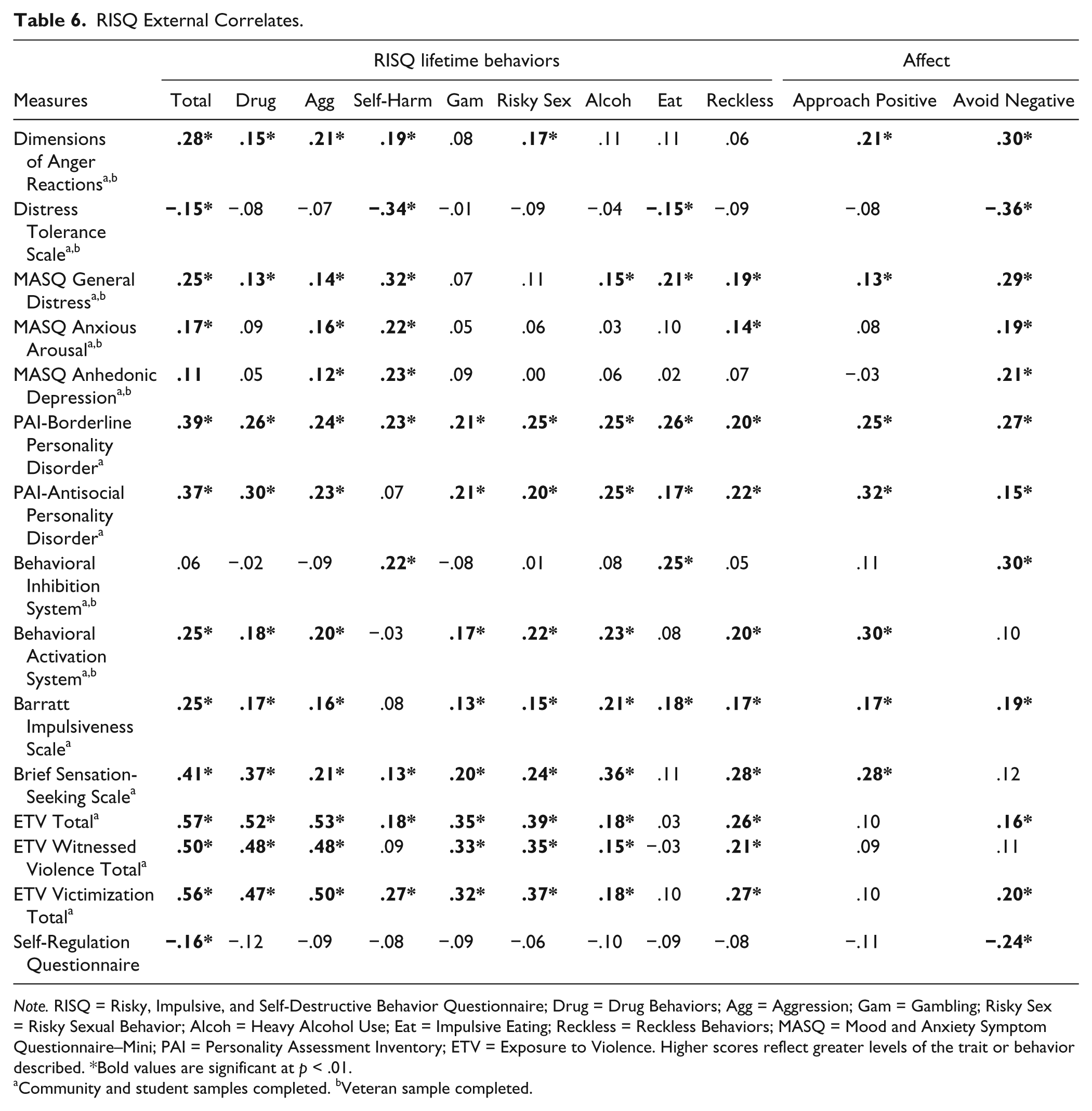
Note. RISQ = Risky, Impulsive, and Self-Destructive Behavior Questionnaire; Drug = Drug Behaviors; Agg = Aggression; Gam = Gambling; Risky Sex = Risky Sexual Behavior; Alcoh = Heavy Alcohol Use; Eat = Impulsive Eating; Reckless = Reckless Behaviors; MASQ = Mood and Anxiety Symptom Questionnaire–Mini; PAI = Personality Assessment Inventory; ETV = Exposure to Violence. Higher scores reflect greater levels of the trait or behavior described. *Bold values are significant at p < .01.
Community and student samples completed. bVeteran sample completed.
The RISQ affective scales also converged in theoretically appropriate ways with external measures. For example, the RISQ Approach scale correlated moderately with the BAS (r = .30), but not the BIS (r = .11), whereas the RISQ Avoidance scale showed the opposite pattern (BAS r = .10; BIS r = .30). Similarly, the RISQ Avoidance scale correlated negatively with distress tolerance (r = −.36) and positively with general distress on the MASQ (r = .29), whereas the RISQ Approach scale evidenced low associations with these measures (rs = −.08-.13). These findings suggest the RISQ affective scales show good convergent and discriminant validity.
Discussion
The goal of this study was to examine the psychometric properties and assessment utility of a new measure that was designed to survey and quantify a range of risky, self-destructive, and impulsive behaviors. Results provide compelling initial evidence to support the validity of the RISQ as a psychometrically sound instrument and demonstrate its utility as a relatively brief, yet broad, assessment tool for capturing the complexity of risky and self-destructive behaviors.
RISQ Factor Structure
The primary goal in developing the RISQ was to achieve representation from a broad range of behavioral indicators that measure engagement in risky and harmful behaviors. Analysis of its factor structure indicated that a bifactor model provided the best fit to the data, with a general factor that captured common variance across diverse manifestations of risky and self-destructive behavior and specific factors that index unique variance associated with distinct behavioral expressions. The specific factors represent categories of behaviors that have been consistently linked to problematic risk taking and impulsivity in the literature, specifically drug use, aggression, self-harm, gambling, risky sexual behavior, impulsive eating, heavy alcohol use, and reckless driving/spending (Bıçaksız, & Özkan, 2015; de Wit, 2009; Hoyle, Fejfar, & Miller, 2000; Mann et al., 2009). The bifactor structure of the RISQ converges with the current state of the literature that suggests risky and self-destructive behaviors frequently co-occur (pointing to potential shared etiological covariance among these phenotypes) but also show associations with distinct risk factors (implicating unique sources of etiological variance; Sadeh, Javdani, Finy, & Verona, 2011; Zuckerman & Kuhlman, 2000). Overall, findings indicate that the RISQ can be used by researchers interested in assessing general tendencies to engage in high-risk behaviors (total score) as well as those looking for a more nuanced assessment of individual differences in preferences for certain types of harmful behaviors (specific factors).
Despite considerable phenotypic heterogeneity in the behaviors captured by the RISQ, all but two of the items loaded significantly on a general factor, and the internal consistency for the total score was good. Notably, the RISQ was not designed to reflect a common latent trait or phenotype (e.g., trait disinhibition or sensation seeking). Rather, the goal was to index different manifestations of risky and self-destructive behavior that may or may not have shared etiologies and, by doing so, to create a tool that can be used to investigate diverse causes of risky behaviors. Given our approach, it is not surprising that the strength of the item loadings on the general factor varied considerably across the items (.03-.94).
One possibility is that the general factor reflects the degree to which the items represent behaviors that are predominately impulsive or risky in nature. For example, items on the Self-Harm factor may be less impulsive on average than other RISQ items given that suicidal thoughts and gestures can vary from premeditated to impulsive depending on the individual. Suicide attempts typically show stronger associations with impulsive traits than suicidal ideation (Mann, Waternaux, Haas, & Malone, 1999), and paralleling this finding, the suicide attempt item loaded more strongly on the general factor than the other self-harm items. Another possibility is that the general factor represents the severity or degree of impairment associated with risky and self-destructive behaviors that is separate from more specific phenotypic manifestations. Thus, behaviors that fall at the high end of the severity dimension would show the strongest loadings on the general factor. This interpretation is congruent with the finding that the impulsive eating behaviors, representing relatively low-severity normative behaviors, did not load significantly on the general factor. It is also consistent with the finding that illegal behaviors did not form a specific factor, but rather loaded exclusively on the general factor. Illegal behaviors are particularly severe in terms of the potential negative legal and social consequences, and individuals who engage in criminal behavior typically display a diverse array of impulsive and risky behaviors (Krueger et al., 2002). Thus, illegal behaviors may have loaded entirely on the general factor, because they represent particularly high levels of behavioral disturbance.
Construct Validity and External Correlates
Examination of the external correlates of the RISQ provided preliminary but promising support for its construct validity. The RISQ total score showed good convergent validity with other self-report measures of risk taking (DOSPERT), but was not so highly correlated as to be redundant with existing measures. Similarly, the total score correlated only moderately with measures of sensation seeking and impulsivity, which is consistent with research showing that personality-based assessments of impulsivity and risk-taking often do not covary highly with behavior-based assessments (e.g., Reynolds, Ortengren, Richards, & de Wit, 2006). In terms of demographic correlates, men reported more lifetime behaviors than women, and RISQ behaviors increased as educational attainment decreased, as would be expected based on the broader literature (Byrnes, Miller, & Schafer, 1999; Cutler & Lleras-Muney, 2010). Importantly, the RISQ factors also showed specificity in their relationships with external scales that measured related constructs (e.g., RISQ Gambling correlated strongly with the South Oaks Gambling Scale but not MINI Suicide Scale), evidence of their concurrent and discriminant validity. Although these preliminary data are encouraging, additional construct validation studies are required to fully evaluate this measure. In particular, it will be crucial to examine the RISQ in relation to criterion variables derived from clinical diagnostic interviews and objective laboratory measures of risk-taking, given that the current study relied exclusively on self-report measures.
Despite the abundance of evidence implicating approach–avoidance tendencies in risky behaviors, few assessments directly measure these tendencies. A major advancement of the RISQ over existing measures is the assessment of an individual’s motivations for engaging in different types of harmful behaviors, which provides crucial information about the affective contexts that trigger these high-risk behaviors. As expected, the RISQ Avoidance scale correlated positively with measures of negative affect, low-distress tolerance, and psychopathology symptoms characterized by negative mood (e.g., borderline personality disorder, anhedonic depression), whereas the RISQ Approach scale correlated as hypothesized with external measures of approach motivation and sensation seeking. Importantly, lifetime behaviors on the RISQ were relatively uncorrelated with external measures of emotional and motivational processes, which instead were more highly correlated with the RISQ affect scales. Present findings indicate that the RISQ affect scales capture unique information about engagement in risky and self-destructive behaviors that can be used by researchers interested in evaluating diversity in the affective triggers for these behaviors. Although outside the scope of this study, future research examining the affective and motivational correlates of these scales using psychophysiological and task-based measures that evaluate reinforcement mechanisms and emotional reactivity would strengthen the construct validity of the RISQ affect scales.
Notably, the simultaneous assessment of engagement in risky behavior and the affective triggers for these behaviors revealed divergent patterns with external correlates that would not have been apparent otherwise. For example, exposure to violence was a consistently strong predictor of engagement in risky behavior, but it was relatively uncorrelated with the affective triggers for these behaviors. This finding suggests that violence exposure is a risk factor for self-destructive behaviors, but it does not necessarily explain why individuals who are exposed to violence engage in these behaviors. Furthermore, the RISQ factors suggested a more nuanced relationship between violence exposure and risky behavior than the total score would suggest, with the pattern of associations varying across the factors. For example, although exposure to violent victimization was associated with both other-directed aggression and self-harm on the RISQ, witnessing violence was only associated with aggressing against others. These results provide an example of potential future applications of the RISQ for identifying factors that generally increase risk for harmful behaviors as well as examining heterogeneity in the relevance of such factors for different phenotypic manifestations of risky and self-destructive behavior.
Strengths and Limitations
There were a number of strengths to the study, including the assessment of three diverse samples, verification of the underlying factor structure in an independent sample, and a thorough evaluation of construct validity. However, findings should be considered alongside a number of limitations. First, behaviors at the high end of the severity continuum (e.g., robbery) were only modestly represented. Thus, cross-validation of the findings in clinical and forensic samples with greater representations of these behaviors is necessary, given that the structure and external correlates of the RISQ may differ in more severe samples. Second, the modest size of the samples is a source of potential bias. And, although a consistent factor structure emerged across the EFA and CFA, examination of the reliability of the factor structure in larger samples is necessary. Third, we did not examine the psychometric properties of the current (past month) items, because the base rates of past month behaviors were highly positively skewed. Given that the lifetime items are theorized to capture long-standing tendencies to engage in risky behavior, we expect the factor structure and external correlates of the past month behaviors to parallel those for the lifetime items. Finally, RISQ was only examined in an adult (18 and older) sample; therefore, additional research is needed to evaluate its validity for use with younger participants.
Conclusions
Risky behavior is not confined to certain stages of the lifespan or diagnostic groups; it is ubiquitous and requires precise and multilevel assessment. Present findings suggest that the RISQ is a promising self-report measure that includes a total score for assessing general tendencies to engage in risky and self-destructive behavior as well as specific factors for assessing heterogeneity in the manifestation of these behaviors. Results indicate that it has a stable factor structure, reliable scales, and convergent validity with other self-report measures of risky behavior. Thus, this initial validation study indicates that the RISQ can be useful for researchers who are interested in studying the origins and correlates of different forms of risky behavior with a comprehensive, yet efficient, assessment tool.
Footnotes
Authors’ Note
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the U.S. Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by grants through the American Psychological Foundation and the American Psychology-Law Society. Additionally, this research was supported by the National Center for PTSD, Behavioral Science Division at VA Boston Healthcare System.