
Abstract
This study examined the reliability and validity of scores from questionnaires assessing compensatory cognitive strategy use by young adults. Participants (N = 783; 79.6% women; 77.4% White; Age: M = 18.7 ± 0.9 years) completed the Compensatory Cognitive Strategies Scale (CCSS), Multifactorial Memory Questionnaire–Strategies (MMQ-S), Neuro-Quality of Life (Neuro-QoL) v2.0 Short Form–Cognitive Function, and Difficulties in Emotion Regulation Scale (DERS). Reliability estimates were acceptable for the CCSS (α = .85) and MMQ-S (α = .86) in the full sample and comparable in subsamples stratified by gender and self-reported mental health conditions. The CCSS and MMQ-S scores showed evidence for convergent validity (r range: .60 to .70) and discriminant validity in the full sample and subsamples (r with DERS range: .13 to .33). Greater compensatory strategy use had small-to-medium associations with greater subjective cognitive concerns on the Neuro-QOL for the full sample and subsamples (r range: −.19 to −.49). The CCSS and MMQ-S scores showed acceptable properties for use with young adults.
Keywords
Researchers have conducted intervention studies examining the efficacy of compensatory cognitive strategies at reducing subjective cognitive concerns in patients with neurological conditions (e.g., multiple sclerosis, dementia; Becker et al., 2019; Troyer, 2001), psychiatric disorders (e.g., psychosis, posttraumatic stress disorder, anxiety, or mood disorders; Jak et al., 2019; Mullen et al., 2017; Twamley et al., 2012), and traumatic brain injuries (Huckans et al., 2010; Jak et al., 2019; Storzbach et al., 2017; Twamley et al., 2015). The outcomes for these trials have included objective cognitive performances, subjective cognitive complaints, and the self-reported implementation of cognitive strategies into the everyday lives of participants. Whereas many prior studies have examined the psychometric properties of neuropsychological tests (Lezak et al., 2012; Strauss et al., 2006) and self-report cognitive symptom questionnaires (Cella et al., 2012; Gershon et al., 2012; Lai et al., 2014; Roth et al., 2014), fewer studies have examined the psychometric properties of questionnaires on compensatory cognitive strategy use (Becker et al., 2019; Dixon & Hultsch, 1983; Troyer & Rich, 2002).
These existing studies have specifically focused on patients with neurological, neurodegenerative, or psychiatric conditions. The assessment of compensatory cognitive strategy use may also be helpful for clinicians working with college students. College students experience significant cognitive demands in their coursework. They have high rates of mental and behavioral health problems (e.g., depression, alcohol use disorders; Auerbach et al., 2016; Blanco et al., 2008) that may adversely affect cognitive functioning (McDermott & Ebmeier, 2009; Semkovska et al., 2019; Stephan et al., 2017). Furthermore, they may acquire conditions or injuries that could affect their cognitive functioning during their studies (e.g., sport-related concussion; Belanger & Vanderploeg, 2005; Dougan et al., 2014; Karr et al., 2014). Successful academic performance requires the use of cognitive strategies, such as planning, notetaking, and developing study strategies to remember important material. For those with and without cognitive weakness or impairment, compensatory cognitive strategy use can be helpful for successful academic performance during postsecondary studies.
Compensatory cognitive strategies have been taught in interventions for many populations with conditions that can affect cognitive functioning (Becker et al., 2019; Jak et al., 2019; Troyer, 2001; Twamley et al., 2012) including college students with psychiatric conditions, which resulted in increased frequency of compensatory cognitive strategy use (Mullen et al., 2017). A clinician working with a college student struggling in their courses may consider possible modes of intervention, which could include addressing mental health problems, recommending academic accommodations, or providing psychoeducation on compensatory cognitive strategy use to support academic performance. Clinicians educating patients on compensatory cognitive strategies as part of their intervention would benefit from having an instrument that quantified current strategy use. Such an instrument would allow them to gauge whether psychoeducation was necessary (i.e., determine if the student is or is not currently using strategies in their everyday life) and track changes in strategy use over the course of the intervention. They may also benefit from reference data among college-aged peers in terms of how often students implement compensatory cognitive strategies in their everyday lives.
This study examined the psychometric properties of two compensatory cognitive strategy scales in a college student sample: the Compensatory Cognitive Strategies Scale (CCSS; Becker et al., 2019) and the Multifactorial Memory Questionnaire–Strategies (MMQ-S; Troyer & Rich, 2002), which have previously been examined for use in samples with multiple sclerosis and dementia, respectively. Prior researchers have not examined the psychometric properties of published scales on compensatory cognitive strategy use among college students. The CCSS and MMQ-S were selected because (a) they are brief and have known psychometric properties (i.e., evidence of reliability, convergent validity, and discriminant validity with different populations); (b) the CCSS was recently developed and involved technology use in its item content, which is pertinent to current college education; and (c) the MMQ-S assesses learning and memory strategies highly relevant for successful academic performance, such as making a to-do list, taking notes, using mnemonics, and practicing spaced retrieval (i.e., effortful recall of information without reference to the source material over increasingly longer spaced time intervals).
For the CCSS and MMQ-S, reliability, convergent validity, and discriminant validity were evaluated, along with the correspondence between compensatory strategy use and subjective cognitive concerns. Reliability was assessed by calculating internal consistency for each scale, hypothesizing that the CCSS and MMQ-S scores would show acceptable reliability among a college student sample. Convergent validity was assessed by calculating the correlation between the CCSS and MMQ-S, hypothesizing that—consistent with previous findings (Becker et al., 2019)—these scales would have a moderate and positive correlation. Discriminant validity was assessed by calculating the correlation between the CCSS and MMQ-S and a measure of emotional regulation, hypothesizing that these scales would correlate, at most, modestly. The relationship between compensatory cognitive strategy use and subjective cognitive concerns was also evaluated as a criterion index for concurrent validity, hypothesizing that—consistent with previous findings (Becker et al., 2019; Troyer & Rich, 2002)—the CCSS and MMQ-S would have a small, negative correlation with cognitive complaints (i.e., those with stronger confidence in their cognitive abilities would report less compensatory strategy use). Last, the assessment of reliability and validity for the CCSS and MMQ-S scores was stratified by gender and preexisting self-reported mental health conditions. Prior research on compensatory cognitive strategy training among college students focused specifically on participants with psychiatric conditions (Mullen et al., 2017); and as such, the current study sought to determine whether the psychometric properties of the scales were comparable between those with and without self-reported mental health conditions.
Method
Participants
Of 1,457 eligible students enrolled in one of three low-level undergraduate psychology courses (i.e., Intro to Psychology, Experimental Psychology, or Statistics in Psychology) at a public university in the United States, 977 college-aged participants completed an online survey as a screener for participation in departmental research (i.e., response rate of 67.1%). For inclusion in analysis, participants needed to meet preestablished inclusion criteria. Participants were excluded from analyses if they (a) reported a history of a neurological condition (e.g., brain tumor, stroke; n = 23); (b) reported a diagnosis of a neurodevelopmental disorder other than attention-deficit/hyperactivity disorder (ADHD), such as autism spectrum disorder (n = 4); and/or (c) reported a traumatic brain injury, not including concussion (n = 9). Among those who met inclusion criteria, participants were further removed from analysis if they provided an incorrect response to either of two embedded validity questions (n = 158), which are described in the Measures section below. This resulted in a final sample of 783 participants included in analysis, with demographic characteristics reported in Table 1.
Sample Characteristics.

The final sample was an average of 18.7 years old (SD = 0.9, range: 18-22), with 79.6% identifying as women (n = 623; Age: M = 18.6, SD = 0.9; 78.8% White), 20.1% identifying as men (n = 157; Age: M = 18.9, SD = 1.0; 72.6% White), and 0.3% identifying as genderqueer/nonconforming or declining to answer (n = 3). The majority of the sample were freshmen (58.5%; n = 458) or sophomores (26.3%; n = 206) in college, with 30.4% (n = 238) declaring a psychology major. In terms of racial and ethnic identity, 77.4% identified as White (n = 606), 9.2% as Black or African American (n = 72), 5.2% as multiracial (n = 41), 4.0% as Latinx (n = 31), 3.2% as Asian (n = 25), 0.3% as Native American or Pacific Islander (n = 2), and 0.8% as another identity or declined to answer (n = 6). In terms of preexisting mental health conditions not used as exclusion criteria, subsamples of participants self-reported a prior diagnosis of depression (21.8%; n = 171; 83.6% women, 84.2% White), an anxiety disorder (28.7%; n = 225; 84.9% women, 83.1% White), ADHD (12.9%; n = 101; 70.3% women, 88.1% White), or another unspecified mental health diagnosis (8.6%; n = 67; 94.0% women, 89.6% White). There was overlap between these samples of participants, with 22.9% reporting a personal history of two or more comorbid diagnoses (n = 179; 84.9% women, 83.8% White). A subsample also reported no preexisting mental health conditions (n = 491; 79.4% women, 73.7% White). Because of the substantial representation of women and preexisting mental health conditions, each analysis was run for the full sample, men, women, the subsample reporting no prior diagnoses of mental health conditions, and the subsamples reporting prior diagnoses of depression, an anxiety disorder, ADHD, and two or more comorbid mental health conditions.
Measures
The questionnaires included as variables in this study included the CCSS (Becker et al., 2019), the MMQ-S (Troyer & Rich, 2002), the Neuro–Quality of Life (Neuro-QoL) Short Form v2.0–Cognitive Function (Cella et al., 2012; Gershon et al., 2012), and the Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2008). A pair of embedded validity assessment questions were included in the CCSS and MMQ-S, informing participants that the question was a validity question and asking them to respond by selecting a specific rating on the item scale (e.g., This is a validity question to check that you are paying attention. Please respond by selecting Often as your response). Prior researchers have recommended face valid instructed response items for online survey data collection as a method for detecting careless and invalid responding (Meade & Craig, 2012).
CCSS
This measure is a 24-item questionnaire querying how frequently participants use compensatory cognitive strategies in their everyday life, including strategies related to processing speed and attention, memory, and executive functions. The questionnaire builds from prior assessments of cognitive strategies by incorporating items on strategies that involve the use of technology. Participants are instructed as follows: “Please rate how frequently you use each strategy to complete cognitive tasks (e.g., those involving thinking, attention, memory) in your daily life.” They respond to each item by rating their frequency of use on a 5-point Likert-type scale: never (0), rarely (1), sometimes (2), often (3), and all the time (4). All items were summed to arrive at the CCSS total score used in analysis, with possible scores ranging from 0 to 96. In patients with multiple sclerosis, previous research has shown acceptable internal consistency for the CCSS total score (α = .90), along with evidence for convergent and discriminant validity (Becker et al., 2019).
MMQ-S
This measure is a 19-item questionnaire that queries about how frequently participants use specific metamemory strategies in their everyday life. Participants are instructed to “Please rate how frequently you use each strategy to help with memory in your daily life,” rating their frequency of use on a 5-point Likert-type scale: never (0), rarely (1), sometimes (2), often (3), and all the time (4). All items are summed to arrive at the MMQ-S total score used in analysis, with possible scores ranging from 0 to 76. Among older adults, the MMQ-S total score has shown acceptable test–retest reliability (r = .88) and evidence for convergent and discriminant validity (Troyer & Rich, 2002).
Neuro-QoL Short Form v2.0–Cognitive Function
This measure is an 8-item questionnaire on subjective cognitive functioning, through which participants rate how much difficulty they have had with cognitive functioning and engagement in different cognitive tasks both currently and over the previous 7 days. Participants rate each item on a 5-point Likert-type scale. The item ratings are summed to arrive a total raw score, with possible values ranging from 8 to 40. Per recommendation by the test developers, the raw scores for the Neuro-QoL are converted to norm-referenced T scores (M = 50, SD = 10) based on comparison with the general United States population (Hanmer et al., 2020). In the general population, the total score for the questionnaire has shown acceptable reliability (α = .92) and evidence for convergent and discriminant validity (Cella et al., 2012).
DERS
The DERS is a 36-item questionnaire that asks about emotional regulation, understanding, and awareness. Participants are instructed to indicate how often the items apply to them on a 5-point Likert-type scale: almost never (1), sometimes (2), about half the time (3), most of the time (4), and almost always (5). All items are summed to arrive at a total score, with possible scores ranging from 36 to 180. This questionnaire has shown acceptable reliability for the total score (α = .93) in a sample of undergraduate students (Gratz & Roemer, 2004). Previous research has shown good fit for a bifactor model of the DERS including a general factor on which all items loaded (Hallion et al., 2018), which supports the use of a total sum score for the measure.
Procedure
Participants completed the questionnaires online via Sona Systems® participant pool management software as part of a screener for participation in research within a university psychology department. The survey is advertised to students enrolled in the three aforementioned undergraduate psychology courses as a way to earn course credit (i.e., Intro to Psychology, Experimental Psychology, and Statistics in Psychology). Participants provided informed consent for their data to be included in this study, and received course credit for participation in the survey. All questionnaires were administered in the same order: a demographic and health history questionnaire, the Neuro-QoL, CCSS, MMQ-S, and the DERS. This study protocol received ethical approval from a university institutional review board.
Statistical Analysis
Missing Data
Less than 2% of cases were missing data for each item on the Neuro-QoL, CCSS, MMQ-S, and DERS, with data missing completely at random per Little’s (1988) test, χ2(5,022) = 5,160, p = .084. Missing data were handled via the expectation–maximization method (Enders, 2010), which retained 80 cases with partial missing data by imputing expected values for individual items on each scale.
Reliability and Validity Assessment
Internal consistency (α) was calculated as an estimate of reliability for each test score (Cronbach, 1951). Convergent validity was assessed by calculating the correlation (r) between the CCSS and the MMQ-S. Discriminant validity was assessed by calculating the correlations between the CCSS and MMQ-S and the DERS. The correlation coefficients from the convergent and discriminant validity analyses were compared (Meng et al., 1992), hypothesizing that the correlation between the CCSS and MMQ-S would be significantly greater than the correlations between either of these scales and the DERS. The relationship between compensatory cognitive strategy use and subjective cognitive concerns was assessed by calculating the correlations between the CCSS and MMQ-S and the Neuro-QoL. All descriptive and inferential statistics were calculated using IBM SPSS version 27.
Factor Analysis
The dimensionality of the CCSS and MMQ-S were evaluated via confirmatory factor analysis using Mplus v.7.3. The items for both the CCSS and MMQ-S are on Likert-type scales and were considered polytomous indicators in the factor model, which requires an alternative estimator in Mplus called weighted least squares with mean and variance adjusted. Multiple fit indices were calculated, including the χ2 goodness-of-fit test, the comparative fit index (CFI), the Tucker–Lewis index (TLI), and the root mean square error of approximation (RMSEA). For the χ2 test, an insignificant p value suggests adequate model fit; however, with large sample sizes, this test has increased power to reject the null hypothesis (Tanaka, 1987). With the large sample size for the current study (N = 783), alternative fit indices were interpreted to determine model fit. For the CFI and TLI, values ≥.90 or ≥.95 were considered indicative of adequate and optimal fit, respectively (Bentler & Bonett, 1980; Hu & Bentler, 1999). For the RMSEA, values ≤.08 and ≤.06 were considered indicative of adequate and optimal fit, respectively (Browne & Cudeck, 1993; Hu & Bentler, 1999). The RMSEA is presented with an accompanying 95% confidence interval (CI).
Because the MMQ-S assesses a single common construct of metamemory strategy use and has evidenced unidimensionality in a prior principal components analysis (Troyer & Rich, 2002), a one-factor model was examined for this scale. No prior research has examined the factor structure of the CCSS; although the original development study of the CCSS examined a single total sum score for the items (Becker et al., 2019), implying a unidimensional structure. When examining the factor structure of the CCSS, the use of a confirmatory approach was preferred over an exploratory approach to (a) examine the fit of a one-factor model, which was implied by prior research using a total score; and (b) compare this model with an alternative multidimensional factor model, with individual items categorized based on an examination of item content. As such, a one-factor model was examined for the CCSS, in addition to a multidimensional model that separated item content by different abilities associated with different strategies (i.e., attention and processing speed, memory, and executive functions).
Power Analysis
An a priori power analysis was conducted using G*Power 3.1 (Erdfelder et al., 2009). Based on previous findings, a medium positive correlation (r = .65) between the CCSS and MMQ-S was anticipated (Becker et al., 2019), requiring a sample size of 16 for power of .80 with α of .05; and smaller negative correlations (r = −.20) between the cognitive strategy questionnaires and the Neuro-QoL were anticipated (Becker et al., 2019; Troyer & Rich, 2002), requiring a sample size of 153 for power of .80 with α of .05. A very small correlation was hypothesized between the cognitive strategy questionnaires and the DERS (r < .10); but considering the large sample size, there was power to detect a significant finding for even a very small effect. An additional analysis examined whether the correlations between the CCSS and MMQ-S differed from the correlations between the DERS and each of these scales. With a hypothesized convergent correlation of .65 and hypothesized discriminant correlations of .10, a sample size of 35 was required for a z test comparing two correlations to achieve power of .80 with an α of .05. For the confirmatory factor analysis, a priori power analysis was conducted to determine the necessary sample size based on a conservative hypothesized RMSEA of .04 (Hancock & Freeman, 2001). The required sample size to achieve .80 power predicting a RMSEA of .04 for the MMQ-S one-factor model (degrees of freedom [df] = 152) was 600. For the CCSS, again predicting a RMSEA of .04, the sample size required to achieve .80 power for the one-factor model (df = 252) and the three-factor model (df = 249) was 400.
Results
Descriptive Statistics for Full Sample and Subsamples
Descriptive statistics for the CCSS, MMQ-S, Neuro-QoL, and DERS are reported in Table 2 for the full sample, men, women, and for subsamples of participants with and without self-reported diagnoses of mental health conditions. All variables were normally distributed, with skewness and kurtosis values for each variable approximating zero. Descriptive statistics for individual items on the CCSS and MMQ-S for the full sample are reported in Tables 3 and 4, respectively. The frequencies of self-reported compensatory cognitive strategy use (i.e., using the strategy sometimes, often, or all the time) for the full sample are also reported in Tables 3 and 4 for the CCSS and MMQ-S, respectively.
Descriptive Statistics for the Full Sample and Subsamples Stratified by Gender and Self-Reported Diagnoses of Mental Health Conditions.
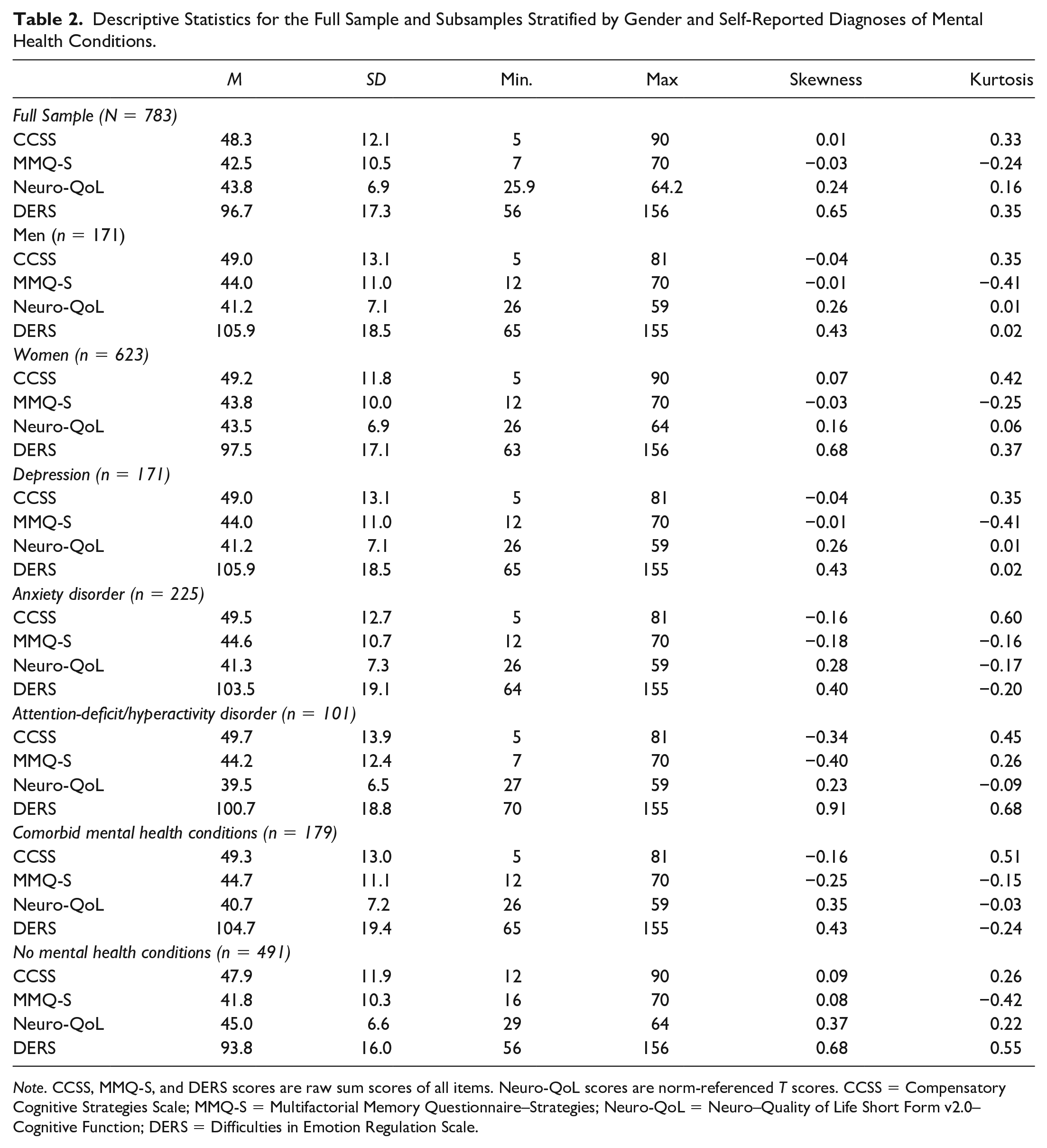
Note. CCSS, MMQ-S, and DERS scores are raw sum scores of all items. Neuro-QoL scores are norm-referenced T scores. CCSS = Compensatory Cognitive Strategies Scale; MMQ-S = Multifactorial Memory Questionnaire–Strategies; Neuro-QoL = Neuro–Quality of Life Short Form v2.0–Cognitive Function; DERS = Difficulties in Emotion Regulation Scale.
The Compensatory Cognitive Strategies Scale: Descriptive Statistics of Self-reported Engagement in Compensatory Cognitive Strategies and Factor Loadings for One-Factor and Three-Factor Measurement Models.
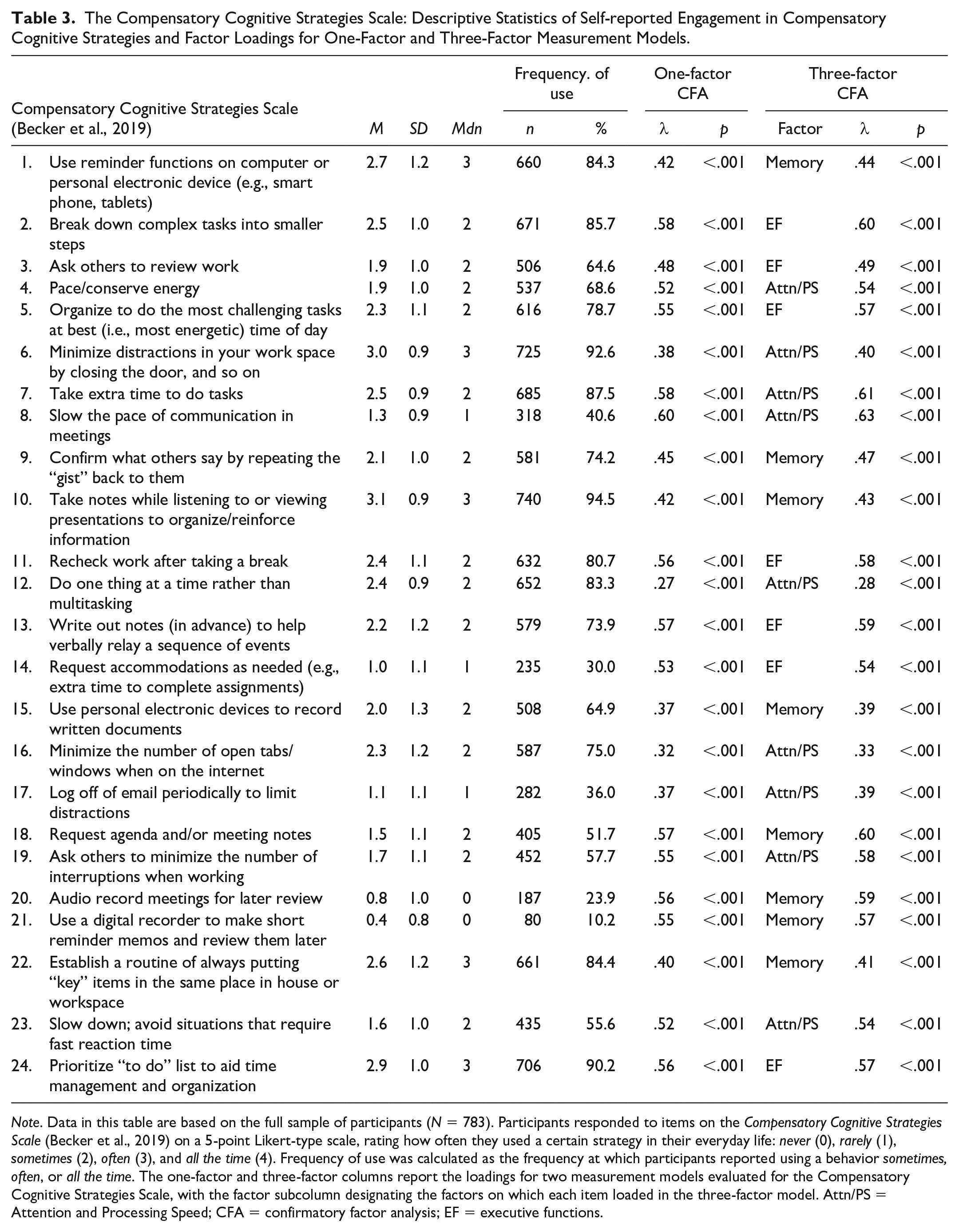
Note. Data in this table are based on the full sample of participants (N = 783). Participants responded to items on the Compensatory Cognitive Strategies Scale (Becker et al., 2019) on a 5-point Likert-type scale, rating how often they used a certain strategy in their everyday life: never (0), rarely (1), sometimes (2), often (3), and all the time (4). Frequency of use was calculated as the frequency at which participants reported using a behavior sometimes, often, or all the time. The one-factor and three-factor columns report the loadings for two measurement models evaluated for the Compensatory Cognitive Strategies Scale, with the factor subcolumn designating the factors on which each item loaded in the three-factor model. Attn/PS = Attention and Processing Speed; CFA = confirmatory factor analysis; EF = executive functions.
The Multifactorial Memory Questionnaire–Strategies Subscale: Descriptive Statistics of Self-Reported Engagement in Compensatory Cognitive Strategies and Factor Loadings for a One-Factor Measurement Model.
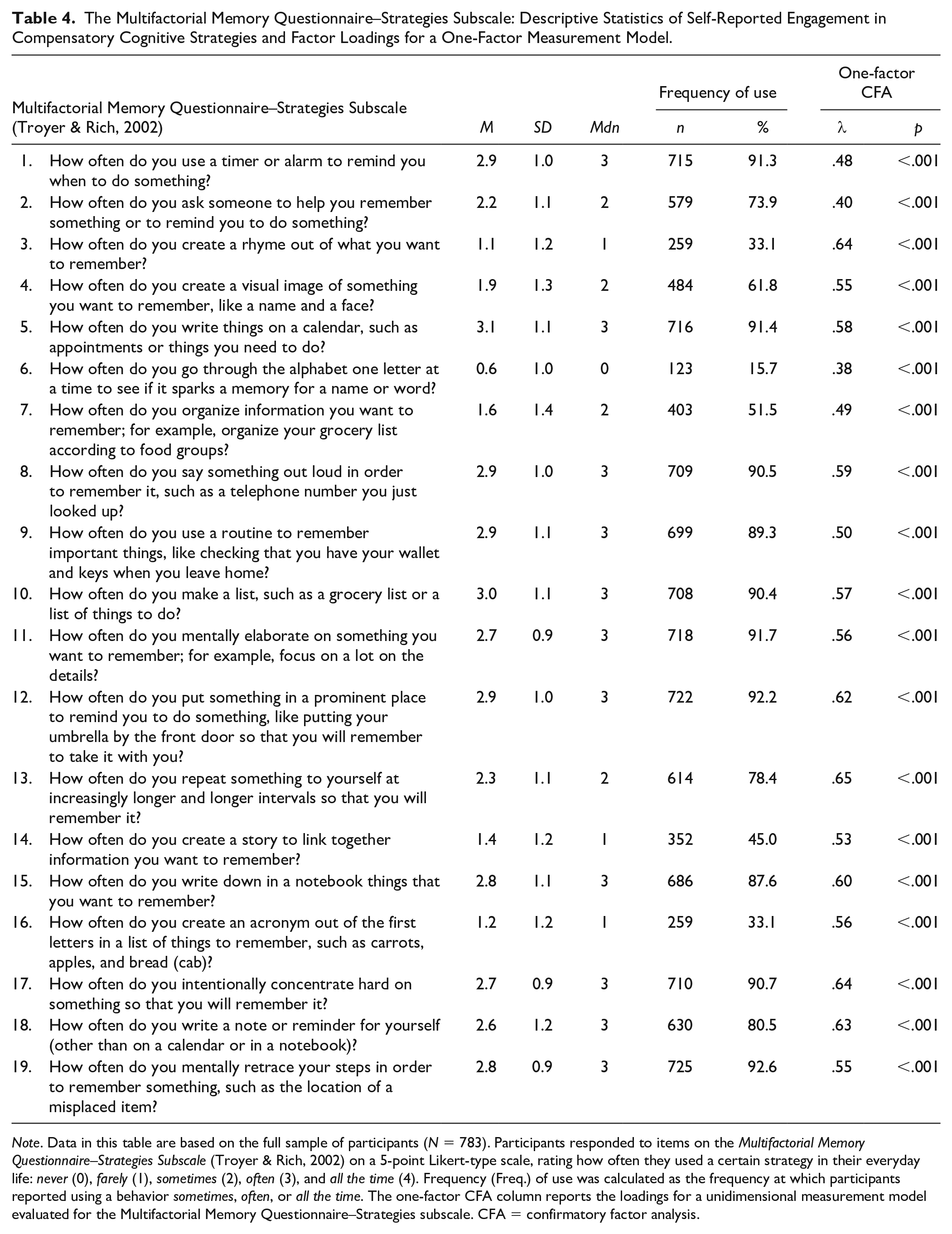
Note. Data in this table are based on the full sample of participants (N = 783). Participants responded to items on the Multifactorial Memory Questionnaire–Strategies Subscale (Troyer & Rich, 2002) on a 5-point Likert-type scale, rating how often they used a certain strategy in their everyday life: never (0), farely (1), sometimes (2), often (3), and all the time (4). Frequency (Freq.) of use was calculated as the frequency at which participants reported using a behavior sometimes, often, or all the time. The one-factor CFA column reports the loadings for a unidimensional measurement model evaluated for the Multifactorial Memory Questionnaire–Strategies subscale. CFA = confirmatory factor analysis.
The most frequently used compensatory cognitive strategies on the CCSS included taking notes during presentations (94.5% of participants reported using this strategy), minimizing distractions in their workspace (92.6%), using a to-do list to aide with time management and organization (90.2%), and taking extra time to do tasks (87.5%). The least frequently used strategies endorsed on the CCSS included using a digital recorder to make short reminders to review later (10.2%), audio recording meetings (23.9%), requesting accommodations (e.g., more time for assignments; 30.0%), and logging off email to reduce distractions (36.0%). On the MMQ-S, the most frequently used compensatory strategies reported by participants included mentally retracing steps in order to remember something (92.6%), placing something in a prominent place as a reminder (92.2%), mentally elaborating on something to support memory (e.g., focusing on details; 91.7%), using a calendar to document appointments and tasks that need completion (91.4%), and using a timer or an alarm as a reminder (91.3%). The least frequently used strategies on the MMQ-S included going through the alphabet a letter at a time to spark a memory (15.7%), using a rhyme to help remember (33.1%), creating an acronym to help remember (33.1%), creating a story to link together information (45.0%), and organizing information to aide with memory (51.5%).
Reliability Estimates
The internal consistency for the CCSS (α = .85), MMQ-S (α = .86), Neuro-QOL (α = .88), and DERS (α = .86) were acceptable in the full sample, as well as men (CCSS: α = .86; MMQ-S: α = 0.87; Neuro-QOL: α = .88; and DERS: α = .86) and women (CCSS: α = .85; MMQ-S: α = .85; Neuro-QOL: α = .88; and DERS: α = .86) analyzed separately. The internal consistency for each measures was also examined in subsamples of participants reporting prior diagnoses of mental health conditions, including depression (CCSS: α = .86; MMQ-S: α = .87; Neuro-QOL: α = .88; and DERS: α = .86), anxiety (CCSS: α = .86; MMQ-S: α = .86; Neuro-QOL: α = .89; and DERS: α = .87), ADHD (CCSS: α = .88; MMQ-S: α = .90; Neuro-QOL: α = .87; and DERS: α = .86), or two or more comorbid mental health conditions (CCSS: α = .88; MMQ-S: α = .90; Neuro-QOL: α = .87; and DERS: α = .86). Internal consistency was also examined in participants who reported no prior diagnoses of mental health conditions (CCSS: α = .86; MMQ-S: α = 0.87; Neuro-QOL: α = .88; and DERS: α = .88). Consistent with the full sample, internal consistency was acceptable for all scales for each subsample of participants.
Convergent and Discriminant Validity Assessment
The Pearson r correlations between the CCSS, MMQ-S, Neuro-QoL, and DERS are presented in Table 5. The correlations between the CCSS and MMQ-S were calculated to gauge the convergent validity of the scales, hypothesizing that the scales would be positively correlated with a medium effect size. Confirming this hypothesis, the correlational analyses indicated that the CCSS and MMQ-S correlated positively and at a moderate magnitude for the full sample (r = .63, p < .01) and at a comparable magnitude for the subsamples stratified by gender and self-reported diagnoses of mental health conditions (r range: .60 to .70, p < .01, for all correlations).
Convergent and Discriminant Validity Analyses for the Full Sample and Subsamples Stratified by Gender and Self-Reported Diagnoses of Mental Health Conditions.
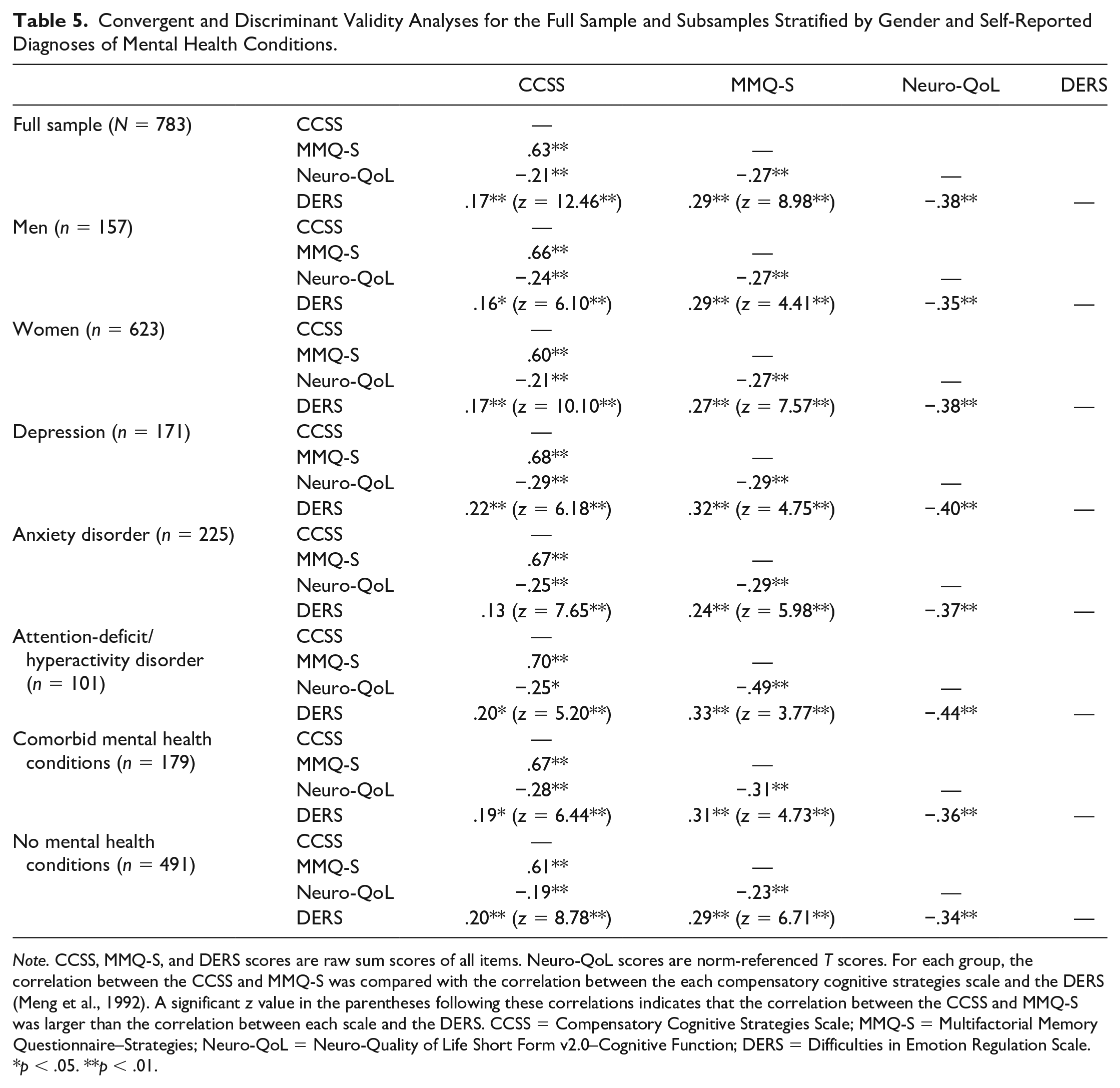
Note. CCSS, MMQ-S, and DERS scores are raw sum scores of all items. Neuro-QoL scores are norm-referenced T scores. For each group, the correlation between the CCSS and MMQ-S was compared with the correlation between the each compensatory cognitive strategies scale and the DERS (Meng et al., 1992). A significant z value in the parentheses following these correlations indicates that the correlation between the CCSS and MMQ-S was larger than the correlation between each scale and the DERS. CCSS = Compensatory Cognitive Strategies Scale; MMQ-S = Multifactorial Memory Questionnaire–Strategies; Neuro-QoL = Neuro-Quality of Life Short Form v2.0–Cognitive Function; DERS = Difficulties in Emotion Regulation Scale.
p < .05. **p < .01.
The correlations between the compensatory cognitive strategy scales and the DERS were examined to evaluate discriminant validity, hypothesizing that these scales would have low correlations as measures of separate largely unrelated constructs. Again, confirming this hypothesis, the correlations between the DERS and the CCSS (r = .17, p < .01) and the MMQ-S (r = .29, p < .01) were small, albeit significant considering the well-powered sample size. Within the subsamples with and without self-reported diagnoses of mental health conditions, the correlations between the DERS and the CCSS were of similar magnitude, but varied in their absolute value (r range: .13 to .22). The correlation between the DERS and CCSS was nonsignificant in the subsample with anxiety disorders, but significant in the subsamples with depression (p < .01), ADHD (p < .05), comorbid mental health conditions (p < .05), and no mental health conditions (p < .01). The DERS correlated significantly with the MMQ-S for all subsamples at a similar magnitude to the full sample (r range: .24 to .33, p < .01 for all correlations). The correlations between the CCSS and the MMQ-S were compared with the correlations between each scale and the DERS for the full sample and each subsample. For the full sample and all subsamples, the correlation between the CCSS and MMQ-S was significantly higher than the correlation of the CCSS with the DERS (all p values <.01) and the MMQ-S with the DERS (all p values <.01).
Subjective Cognitive Concerns and Compensatory Cognitive Strategy Use
The Neuro-QoL was the only norm-referenced questionnaire used in the current study, and a sizeable minority of the full sample (30.5%) reported moderate subjective cognitive complaints (i.e., T < 40). This sizeable minority was still greater than expectation based on normative comparisons (i.e., T = 40 corresponds to the 16th percentile) even when removing participants with self-reported diagnoses of mental health conditions: 23.8% of the sample without any reported mental health condition endorsed moderate cognitive symptom severity.
The correlation between the compensatory cognitive strategy scales and the Neuro-QoL were examined to determine how closely compensatory cognitive strategy use corresponded to subjective cognitive concerns in everyday life. The correlation between the CCSS and Neuro-QoL was r = −.21 (p < .01), and was similar for subsamples of participants stratified by gender or self-reported diagnoses of mental health conditions (r range: −.21 to −.29, p < .05, for subsample with ADHD, and p < .01, for all other subsamples). The correlation between the MMQ-S and Neuro-QoL was r = −.27 (p < .01) for the full sample. This correlation was moderate for the subsample with ADHD (r = −.49, p < .01), but comparable to the full sample for subsamples stratified by gender and other self-reported diagnoses (r range: −.23 to −.31, p < .01, for all correlations). As hypothesized, the observed correlations aligned with the small negative correlations observed in previous literature.
Factor Analysis
The one-factor CCSS model failed to meet criteria for adequate model fit, χ2 = 1,605.80 (p < .0001), df = 252, CFI = 0.805, TLI = 0.787, RMSEA = 0.083 (95% CI [0.079, 0.087]), albeit the RMSEA approached an upper-bound threshold for acceptable fit. The factor loadings for this model are presented in Table 3. The CCSS items were categorized under three factors: attention and processing speed, memory, and executive functions. The item assignments and factor loadings for the three-factor model are provided in Table 3. The three-factor CCSS model showed comparable fit to the one-factor model, χ2 = 1,574.66 (p < .0001), df = 249, CFI = 0.809, TLI = 0.789, RMSEA = 0.082 (95% CI [0.079, 0.086]). The attention and processing speed factor correlated highly with the memory factor (r = .88) and the executive functions factor (r = .90). The memory factor and executive functions factor also correlated highly (r = .91). The one-factor MMQ-S model did not meet criteria for adequate model fit, χ2 = 1,795.09, df = 152, p < .0001; CFI = 0.777, TLI = 0.749, RMSEA = 0.117 (95% CI [0.113, 0.122]). The factor loadings for this model are presented in Table 4.
Discussion
The CCSS and MMQ-S total scores showed evidence for acceptable reliability and convergent and discriminant validity in a sample of young adults with and without self-reported mental health conditions attending college in the United States. The observed internal consistency for each scale and the correlation between the CCSS and MMQ-S were consistent with prior estimates in samples of older adults and patients with multiple sclerosis (Becker et al., 2019; Troyer & Rich, 2002). Evidence for discriminant validity was also apparent, in that the correlations between compensatory cognitive strategy use and emotional regulation were significantly smaller than the correlations between the CCSS and MMQ-S. The correspondence between compensatory cognitive strategy use and subjective cognitive concerns was also similar to prior studies, with small negative correlations observed for the current sample. These negative correlations provide evidence for concurrent validity, in that participants with greater cognitive concerns use compensatory cognitive strategies at a greater frequency in their everyday life.
A confirmatory factor analysis was run to examine the internal structure of the CCSS and MMQ-S, hypothesizing a one-factor structure for each based on prior use of the total score for the CCSS (Becker et al., 2019) and a previous principal components analysis for the MMQ-S (Troyer & Rich, 2002). The one-factor models did not meet most criteria for adequate fit for either scale. For the CCSS, fit was not improved when an alternative three-factor model was examined, and the three factors (i.e., attention and processing speed, memory, and executive functions) correlated highly with one another (r range: .88 to .91). The strongest evidence supported the one-factor CCSS model, which was parsimonious and had a RMSEA that approximated the lenient threshold for acceptable fit. However, overall, these findings show weak evidence for any of the scale structures evaluated.
Clinical Implications
A sizeable minority of participants reported a moderate severity of subjective cognitive concerns, even after excluding participants with self-reported mental health conditions that may affect cognitive functioning. Even without any neurological or psychiatric conditions, young adults may struggle to engage in cognitively demanding tasks, and subjectively notice personal difficulties with their cognitive functioning that may go undetected by objective neuropsychological tests. Prior research has shown that subjective cognitive concerns tend to be more related to mental health symptoms than objective cognitive functioning (Serra-Blasco et al., 2019; Srisurapanont et al., 2017), and underlying symptoms of depression could explain the high frequency of elevated cognitive concerns observed in the current sample. Of note, both participants who did and did not have prior diagnoses of mental health conditions reported elevated cognitive concerns, but the severity of current symptoms was not directly measured. Considering the significant stress of postsecondary education (Robotham & Julian, 2006) and the mental health problems experienced by college students (Auerbach et al., 2016; Blanco et al., 2008), cognitive remediation may be a helpful style of intervention for clinicians in college counseling centers seeking to support students managing many personal and academic demands.
Compensatory cognitive strategy use was quite common in the current sample. Nearly all participants reported using some strategies (e.g., taking notes, keeping a to-do list, or maintaining a calendar), whereas other strategies were implemented less often, such as spaced retrieval. Some students may not be familiar with spaced retrieval, but this learning strategy has led to success in college math courses (Hopkins et al., 2016); and increased use could lead to greater academic success. Compensatory cognitive strategies have been used by high-functioning students with learning disabilities to support success in postsecondary education (Reis et al., 2000), and a compensatory cognitive training intervention led to reduced academic difficulties in college students with mental health conditions (Mullen et al., 2017). A clinician could apply such an intervention independent of, or supplemental to, more traditional mental health treatment to support academic functioning, potentially using the CCSS or MMQ-S to assess baseline use of compensatory cognitive strategies and monitor change posttreatment.
Limitations
This study had limitations that affect the generalizability of the findings. Although embedded validity questions addressed careless responding during survey administration, other threats to validity were not evaluated, such as social desirability. Participants were current college students; and, for this population, it may be desirable to report, or at least self-perceive, a greater use of strategies that would help with academic performance. However, the survey responses were nonidentifiable and unrelated to the allocation course credit, which both reduce the risk for a social desirable response pattern affecting the validity of responses. The study was also limited by its cross-sectional design, meaning estimates of test–retest reliability could not be estimated. A test–retest estimate of reliability may be helpful for researchers and practitioners who readminister the CCSS or MMQ-S on multiple occasions, such as those who conduct interventions. The availability of a test–retest reliability estimate would also be useful for calculating a reliable change index to determine if an individual participant or patient improved with intervention. A future investigation examining the test–retest reliability for the CCSS, MMQ-S, or another scale assessing compensatory cognitive strategy use would be beneficial for cognitive rehabilitation research and clinical practice.
Another limitation pertains to participant recruitment, which occurred at a single university psychology department. Although the sample included participants of diverse identities, they identified predominantly as White, with an overrepresentation of women. This sample is not necessarily representative of young adults from different states, regions, or countries, or those who do not attend college or university. The enrollment of participants in college may contribute to greater self-perceived cognitive problems and a greater recruitment of cognitive strategies, considering the high cognitive demands associated with college coursework.
The CCSS and MMQ-S are not the only measures available to evaluate compensatory cognitive strategy use. Other assessment instruments, such as the Cognitive Problems and Strategies Assessment (Twamley et al., 2012) and the Metamemory in Adulthood Questionnaire–Strategy subscale (Dixon & Hultsch, 1983), may have valuable items that address compensatory cognitive strategies not included in the CCSS and MMQ-S. However, these additional measures were not administered in the current study. The relationships between these measures, the CCSS, and the MMQ-S remain unknown and could be the focus of future research on the convergent validity of these scales among young adults.
Future Directions
The CCSS and MMQ-S show many sound psychometric properties for use with young adults based on the current findings, but prior researchers did not design these measures for use with healthy young adults. The cognitive strategies applicable to a young adult may not align with those applicable to an older adult. Whereas a college student may need strategies to focus while studying for a test or manage a busy schedule (e.g., sports or exercise, classes, and work), a retired older adult may need strategies to help remember a phone number, a grocery list, or a doctor’s appointment. Compared with the MMQ-S, some added strengths of the CCSS are its recent development and inclusion of items pertaining to technology use (Becker et al., 2019), which may make this scale more appropriate for use with college students. However, both scales showed comparable psychometric properties, including acceptable reliability and evidence for convergent validity and discriminant validity. This study adds to existing research on the psychometric properties of instruments assessing compensatory cognitive strategy use in various populations, and provides evidence for the reliability and validity of the CCSS and MMQ-S for use with college students with and without mental health conditions. The findings do not indicate a preference for either scale; and the absence of a clear factor structure for both scales may suggest that future researchers could further refine these instruments by modifying their content, combining items from different scales, or including new items specifically pertinent to college students.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.