
Abstract
The Social and Emotional Assets and Resilience Scale (SEARS) is a promising instrument for prediction of resilience in youth; however, there is limited data to support its use. The purpose of the current study was to examine the factor structure, measurement invariance, internal consistency, and validity of the SEARS-Adolescent Report in youth 8 to 20 years of age. Two hundred and twenty-five childhood cancer survivors (Mage = 15.9, SD = 4.2; 51.4% male; 74.5% White) and 122 student controls without history of significant health problems (Mage = 14.2, SD = 3.5; 54.1% female; 79.5% White) 8 to 20 years of age completed the SEARS-A. The SEARS-A was found to have an adequate factor structure and model fit (χ2 = 1215.5, p < .001; root mean square error of approximation = .057; comparative fit index = .95; standardized root mean square residual = .06) and demonstrated invariance across domains of age, health status, gender, race, and socioeconomic status (Δ comparative fit index < −0.01). It also demonstrated excellent internal reliability, criterion validity, and current validity when compared with another well-established measure of psychological adjustment. As such, the SEARS-A has potential to be a useful, valid, and psychometrically sound tool for predicting social–emotional adjustment outcomes among at-risk youth 8 to 20 years of age.
Resilience has been conceptualized in many ways including as a trait, a process, and an outcome (Southwick et al., 2014). There may be validity to all of these approaches, but as outlined in a recent American Psychological Association (APA) monograph, there is some consensus developing regarding the advantage of operationalizing resilience in terms of positive outcomes in the face of adversity or significant sources of stress. In supporting the view of resilience as an outcome, Bonanno (2004) defines it as a stable trajectory of healthy psychological functioning following exposure to adversity or potentially traumatic events. Although the APA monograph states explicitly that resilience is not a trait, it is also clear that there are numerous personal factors that may be associated with more or less resilient outcomes. Research has identified a number of social–emotional strengths that may serve as predictors of resilience in youth who have endured challenging events, such as close interpersonal relationships, self-regulation, self-efficacy, agency, and conscientiousness (Alvord & Grados, 2005; Masten, 2015).
Social competence and self-regulation have been conceptualized as central components of fostering and facilitating close interpersonal relationships, as children who demonstrate high social competence and greater self-regulation are more likely to have closer social relationships and to exhibit better psychosocial functioning (Buckner et al., 2003; Eisenberg et al., 2003; Werner, 1993). Agency and conscientiousness have also been shown to be associated with healthy psychological adjustment among youth who have experienced hardship, as those who take responsibility for themselves and empathize with others are more likely to demonstrate greater self-efficacy, self-awareness, and self-esteem (Southwick et al., 2014). As such, the assessment of social–emotional strengths provides a potentially important approach to our understanding and prediction of resilience in youth who have endured hardship.
The Social and Emotional Assets and Resilience Scale (SEARS) was developed as an assessment of social–emotional predictors of resilience (Cohn et al., 2009). It is a cross-informant assessment system designed to assess social–emotional strengths in children 5 to 18 years of age. These strengths include social competence, peer relations, coping and self-regulation skills, problem solving abilities, agency, and empathy (Merrell, 2011). The SEARS consists of four rating forms: two separate self-report forms, the child self-report (SEARS-C) for children 8 to 12 years and the adolescent–self- report (SEARS-A) for adolescents 13 to 18 years, and a parent- (SEARS-P) and teacher-report (SEARS-T) for youth 5 to 18 years (Merrell, 2011). All four rating forms contain similar item content; however, items have been slightly tailored to fit the developmental level of the child and the context of the informant (Cohn et al., 2009; Merrell, 2011).
The SEARS was originally created to serve as a screening tool to identify students within the school system who may benefit from intervention aimed to enhance their social, emotional, and academic development (Ysseldyke et al., 2008). Unlike other behavior rating systems which primarily focus on problem behaviors, the SEARS identifies specific social–emotional strengths that may serve as protective factors that promote psychological well-being and academic success (Merrell, 2011). It has been suggested that such strength-based assessments may be a superior method of identifying psychosocial risk in youth as these measures tend have higher social validity among raters and be less stigmatizing than traditional behavior rating scales and mental health screeners (Dowdy et al., 2010).
Despite the availability of the SEARS and its potential utility, questions regarding its psychometric properties have been raised (Cohn et al., 2009). Based on factor analytic studies, the developers created separate versions of the youth report measure: a unidimensional measure for children 8 to 12 years of age (SEARS-C) and a measure with four separate factors for adolescents ages 13 years and older (SEARS-A), although the item content is similar in both instruments. However, Cohn et al. (2009) found that items on the SEARS-C cluster into the same four-factor structure of the SEARS-A. Both the SEARS-C and SEARS-A contain 35 items, 25 of which are identical or near identical in wording, with only 10 items unique to each, but still covering similar content. Thus, it may be possible that a single instrument could be used with children as young as 8 years of age. A single instrument that could reliably measure the same constructs across this age range would be advantageous for both cross-sectional and longitudinal studies. However, additional research is needed to determine whether a single instrument, the SEARS-A, demonstrates factorial invariance across the full age range, as well as other important demographic factors, including race, SES, and health status. Furthermore, a thorough investigation of its reliability, validity, and utility as a measure of social–emotional strengths among both normative and at-risk youth is warranted.
Authors of the SEARS have demonstrated that it correlates highly with other strength-based social rating scales, including the Social Skills Rating Scale (Gresham & Elliott, 1990), the Positive Affect Scale of the Internalizing Symptoms Scales for Children (Merrell & Walters, 1998), and the Student Life Satisfaction Scale (Huebner, 1991). However, it has yet to be tested against other well-developed and widely used behavior rating scales of psychological adjustment. Additionally, parent–child correlations between the adolescent or child and parent versions of the SEARS have yet to be reported and are not mentioned in the SEARS manual (Merrell, 2011), nor is information provided regarding age, gender, or other demographic influences. As such, further examination of the SEARS is warranted to make meaningful comparisons across informants and demographic groups.
A final reservation of the SEARS, given the need to assess resilience in the context of adversity or stress, is that there has been little examination of the measure within established at-risk populations. Youth with chronic health conditions have been established as an at-risk population, as these individuals often experience a number of treatment- and illness-related stressors. Pediatric cancer is a chronic health condition that is associated with a variety of complex physical and psychosocial challenges, including demanding treatment regimens, painful medical procedures, treatment side effects, disruptions to everyday functioning and interpersonal relationships, and threat of death (Hildenbrand et al., 2014). Despite these challenges, patients with cancer and childhood cancer survivors tend to report low levels of posttraumatic stress and internalizing symptoms and high levels of posttraumatic growth, suggesting the presence of resilience promoting factors (Brinkman et al., 2018; Gerhardt et al., 2007; Phipps et al., 2014). Previous research has identified several social–emotional strengths among youth with cancer, such as social support and social connectedness, as predictors of healthy psychological functioning and resilience (Howard Sharp et al., 2015; Tillery et al., 2017; Trask et al., 2003; Van Schoors et al., 2017). As such, the SEARS may be a particularly useful measure of social–emotional predictors of resilience in youth with cancer.
Given the potential utility of the SEARS-A as a measure of resilience in the context of adversity or stress, the purpose of this study was to (a) evaluate the factor structure of the SEARS-A using the original factor structure proposed by Merrell (2011) in youth 8 to 20 years of age; (b) evaluate measurement invariance of the SEARS-A across domains of age, health status (youth with cancer vs. control), gender, race, and SES; (c) examine internal consistency, concurrent validity, and criterion validity of the SEARS-A; and (d) examine the utility of the SEARS-A in predicting common outcomes of psychological adjustment in comparison to a widely used evidence-based behavior rating scale (the Behavior Assessment System for Children, Second Edition; BASC 2) among a sample of youth with and without a history of pediatric cancer. Further examination of the psychometric properties of the SEARS-A, as well as confirmation of its utility among a sample of youth with cancer, will provide needed support for the use of this measure as a means of assessing constructs associated with resilience.
Method
Participants and Procedures
Data were collected from (a) 225 childhood cancer survivors (Mage = 15.9, SD = 4.2; 51.4% male; 74.5% White) and their primary caregiver and (b) 122 student controls without history of significant health problems (Mage = 14.2, SD = 3.5; 54.1% female; 79.5% White) and their primary caregiver, as part of a larger longitudinal study examining stress and adjustment in youth diagnosed with pediatric cancer and their families (see Table 1 for demographic and disease characteristics).
Demographic and Disease Characteristics Across Study Groups.
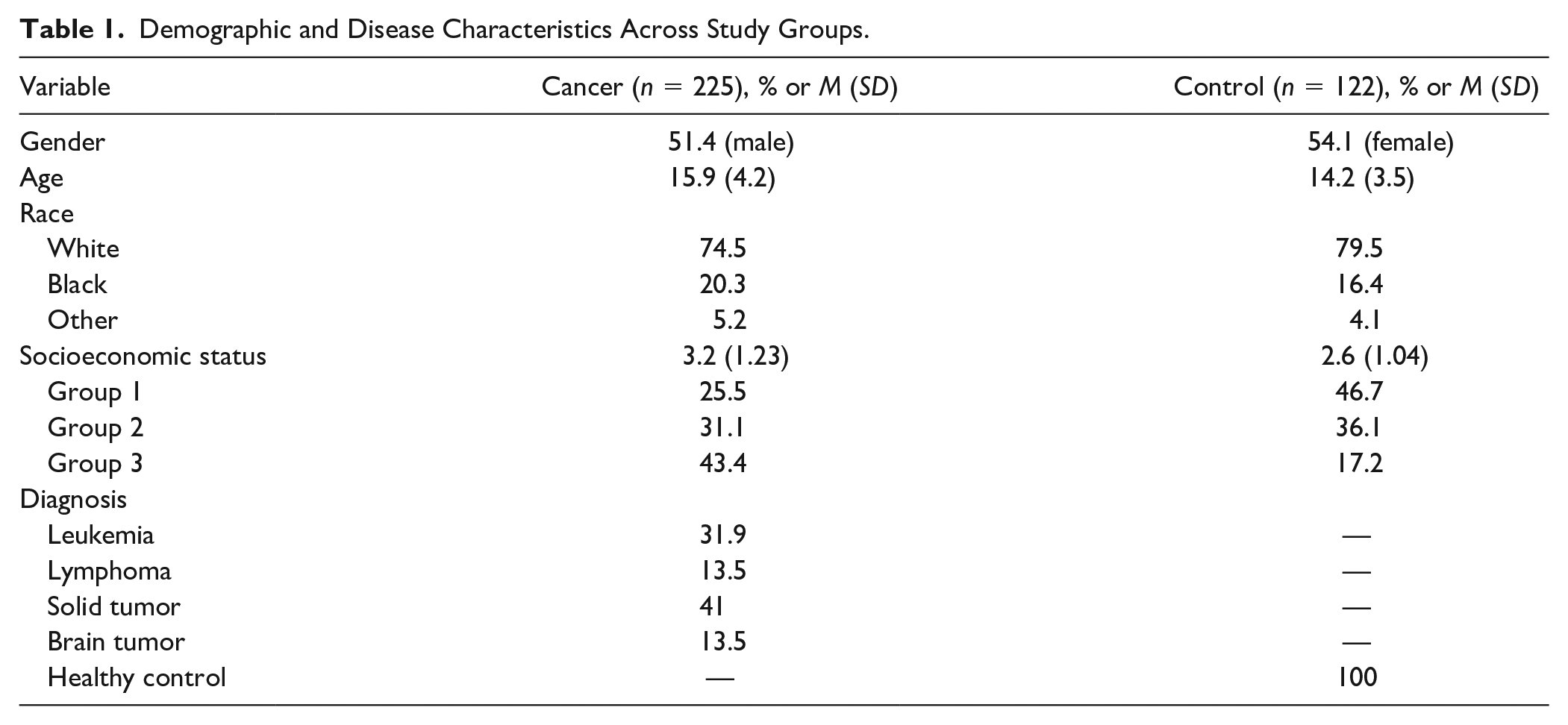
For participants with a history of pediatric cancer, eligible caregiver–child dyads were approached during their routine care visit to outpatient clinics at a large pediatric medical center devoted to the care of children with cancer. At baseline, patients were included if they were (a) English-speaking, (b) at least 1-month post diagnosis, (c) did not have any significant cognitive or sensory impairments, and (d) had a parent/legal guardian who was willing to participate and provide consent for their child. The current data were obtained at the third-year follow-up of the longitudinal study.
A comparison group of children without history of cancer or other serious illness was obtained from the community. Comparison participants were included in the present study if they (a) did not have a history of chronic or life-threatening illness, (b) did not have any significant cognitive or sensory impairments, (c) spoke English, and (d) had a parent/legal guardian who was willing to participate and provide consent for their child. Participants in the healthy comparison group were recruited from public and private schools within the surrounding three-state area of the hospital. Permission slips were distributed to students through administrative staff at their school. Returned permission slips were collected from administrative staff and used to create a pool of potential control participants, which included information regarding youths’ age, gender, race/ethnicity, and parental education and occupation. Participants in this pool were subsequently contacted to participate if their demographics were similar to a participant in the cancer group.
Data collection procedures were conducted with approval from the institutional review board. All participants and caregivers met with a trained psychology staff member in the hospital’s outpatient psychology clinic. Caregivers provided written consent for themselves and for youth to participate; youth provided additional assent.
Measures
Demographic and Clinical Variables
Parents and youth reported on their own sociodemographic information respectively, including age, race, gender, education, and occupation. Socioeconomic status (SES) was measured using the Barratt Simplified Measure of Social Status (Barratt, 2006). Participants’ medical diagnosis, date of diagnosis, and treatment information was systematically collected through medical record review.
Social and Emotional Assets and Resilience Scale
Youth and caregivers completed the SEARS (Merrell, 2011). The SEARS system has been designed to measure social–emotional strengths in youth across four global domains: self-regulation, empathy, responsibility, and social competence. Adolescent (SEARS-A) and parent-report (SEARS-P) versions of the SEARS were used in the current study. Items on the SEARS-A reflect characteristics of these subscales and include statements such as “I know how to calm down when I am upset,” “My friends come to me for help,” and “I know when other people are upset, even when they do not talk about it.” The SEARS-P consists of 39 items and three subscales: Self-Regulation/Responsibility, Social Competence, and Empathy. Example items include statements about their child, such as “[My child] Knows when people are upset,” “Expresses disagreement with others without fighting or arguing,” and “Makes good decisions.” For the current study, the SEARS-P was obtained only as an indicator of concurrent validity, as the examination of its factor structure is beyond the scope of the current study. Teacher report (SEARS-T) was not collected.
All youth (8-20 years of age) in the current study completed the SEARS-A. Caregivers completed the 39-item parent version of the SEARS (SEARS-P; Self-Regulation/Responsibility, α = .95; Social Competence, α = .93; Empathy, α = .87, for the current study). Youth and caregivers respond to items using a 4-point Likert-type scale (0 = never, 1 = sometimes, 2 = often, 3 = always). All 35 items on the SEARS-A can be summed to create scores for each subscale or a combined total score. Tables are available to convert raw scores to T-scores (neither age nor gender corrected), with higher scores indicating greater social–emotional strengths. Reliability and validity with other well-known measures of social functioning (e.g., Social Skills Rating System) has been demonstrated.
Behavior Assessment System for Children, Second Edition
Youth and caregivers also completed BASC 2 (Reynolds & Kamphaus, 2004). The BASC 2 is a widely used, multidimensional clinical assessment system that measures behavioral, emotional, and adaptive functioning of children and individuals between 4 and 21 years of age. The BASC-2 includes youth self-report (BASC 2-SRP), parent (BASC 2-PRS), and teacher rating scales; however, only self-report and parent rating scales were utilized in the current study. The BASC 2-SRP has two different versions, one for children 8 to 11 years of age (Child Form) and one for adolescents 12 to 21 years of age (Adolescent Form). Both self-report versions consist of 16 subscales (i.e., Anxiety, Attention Problems, Attitude to School, Attitude to Teachers, Atypicality, Depression, Hyperactivity, Interpersonal Relations, Locus of Control, Relations with Parents, Self-Esteem, Self-Reliance, Sensation Seeking, Sense of Inadequacy, Social Stress, and Somatization) and four composite scales (i.e., Internalizing Problems, School Problems, Personal Adjustment, and Inattention/Hyperactivity). The BASC 2-PRS consists of nine clinical scales (i.e., Aggression, Anxiety, Attention Problems, Atypicality, Conduct Problems, Depression, Hyperactivity, Somatization, and Withdrawal) and five adaptive scales (i.e., Activities of Daily Living, Adaptability, Functional Communication, Leadership, and Social Skills). The clinical and adaptive scales are used to generate four composite scores: Internalizing Problems, Externalizing Problems, Behavioral Symptoms Index, and Adaptive Skills. Additional content scales, including Ego Strength and Resiliency, were added to the BASC 2-SRP and BASC 2-PRS, respectively, to assist professionals administering the BASC 2 in determining differences in social maladjustment and emotional disturbances (Reynolds & Kamphaus, 2004). The format of items on the BASC 2-SRP consists of a combination of True/False (or T/F) responses and a 4-point Likert-type response scale (0 = never; 1 = sometimes; 2 = often; 3 = almost always). All responses on the BASC 2-PRS consist of the same 4-point Likert-type scale. Items on the BASC 2-SRP reflect characteristics of these subscales and include statements such as “I am good at things,” “I feel sad,” and “I get nervous.” Example items on the BASC 2-PRS include statements that may or may not apply to their child, such as “[My child] Adjusts well to changes in family plans,” “Cries easily,” and “Makes friends easily.” The BASC 2-SRP takes approximately 20 to 30 minutes for youth to complete and the BASC 20-PRS takes approximately 10 to 20 minutes for caregivers to complete.
The current study used self-report Internalizing Problems, Personal Adjustment, and Ego Strength scales and parent-report Internalizing Problems, Externalizing Problems, Adaptive Skills, and Resiliency scales as an overall assessment of youth’s psychosocial functioning. Item raw scores are summed and converted to age- and gender-normed T-scores (M = 50, SD = 10), with scores below 60 indicating normal functioning, scores between 60 and 69 indicating “at-risk” behavior implying mild to moderate impairment, and scores above 70 indicating “significant risk” requiring follow-up. The BASC-2 has been shown to be internally consistent (α = .80-.90) and has demonstrated good test-retest reliability (average r = .80, for composite scores and between .70 and .80, for individual scales) and interrater reliability (median r = .70 across composite and individual scales; Reynolds & Kamphaus, 2004).
Statistical Analysis
Data analyses occurred in two distinct phases, a factor analytic phase and a validation phase. First, confirmatory factor analyses (CFAs) were used to examine the factor structure of the SEARS-A in a sample of 8- to 20-year-olds with and without a history of pediatric cancer using the original factor structures proposed by Merrell (2011). Multigroup CFA was then used to test invariance of the SEARS-A across age, gender, race, health status, and SES. To investigate invariance across these demographics, the following groups were used: age (8-12 or ≥ 13), gender (male/female), race/ethnicity (minority/nonminority), health status (cancer diagnosis or comparison), and SES (high, medium, or low). Invariance analyses proceeded in three stages, from configural to metric to scalar, for all group invariance analyses, as recommended by Gregorich (2006). Configural invariance was tested by (a) freeing all factor loadings for each item across groups, (b) freeing thresholds for each item across groups, (c) fixing scale factor means for each item at 1 across the groups, (d) fixing factor means at 0 for each item across groups, and then (e) freeing factor variances for each item across the groups in comparison (Kamody et al., 2014; Millsap & Yun-Tein, 2004; Muthén & Muthén, 1998-2012). Metric invariance assumes configural invariance and establishes that the factor loadings are equal across the groups. Scalar invariance assumes metric invariance and establishes that the indicator thresholds are equal across the groups.
CFAs were conducted using mean- and variance-adjusted weighted least squares estimation (Asparouhov & Muthén, 2010) to account for missing data and the ordinal response format. Model fit was evaluated using the model chi-square (Browne & Cudeck, 1993), the root mean square error of approximation (RMSEA; Steiger, 1990), the standardized root mean square residual (SRMR; Hu & Bentler, 1999), and the comparative fit index (CFI; Bentler, 1990). In general, higher chi-square values indicate worse model fit; however, this value is less informative compared with RMSEA, SRMR, and CFI values as it is more sensitive to slight misspecifications in model structure and sample size (Bollen & Long, 1993). RMSEA values less than .05 are interpreted as good, and values between .05 and .08 are interpreted as acceptable (Hu & Bentler, 1999). SRMR values of .08 or lower indicate good model fit (Hu & Bentler, 1999). CFI values range from 0 to 1, with values above 0.9 representing adequate model fit (Bollen, 1989). For invariance testing, invariance is supported at the metric and scalar levels if the model fit is not worse than the previous level of invariance (metric compared against configural, scalar compared against metric) based on the change in CFI values (Gregorich, 2006; Kamody et al., 2014; Kline, 2015; Muthén & Muthén, 1998-2015). To be considered invariant across groups, the change in CFI must be ≤ −0.01. Furthermore, it is also recommended to use RMSEA and SRMR values to compare model fit when assessing measurement invariance as these values are less sensitive to model complexity and sample size (Chen, 2007).
In the second phase of analyses, internal reliability and validity analyses were conducted. Internal reliability was assessed via Cronbach’s alpha (α). Concurrent validity of the SEARS-A was determined by comparing the subscales of the SEARS-A with one another and comparing the subscales of the SEARS-A with subscales of the SEARS-P across the cancer and control group via bivariate correlations. Criterion validity of the SEARS-A was determined in a similar fashion by comparing the SEARS-A and self- and parent-report subscales of the BASC-2 (BASC-2 SRP and BASC-2 PRS, respectively) across both groups. CFA and invariance analyses were conducted in Mplus version 8.4 and reliability and validity analyses were conducted using SPSS 25 (IMB, 2017).
Results
Confirmatory Factor Analysis
CFA was used to examine the factor structure of the SEARS-A for 8- to 20-year-olds using the original factor structures proposed by Merrell (2011). The SEARS-A yielded adequate model fit (χ2 = 1215.46, p < .001; RMSEA = .057, 90% confidence interval [.05, .06]; CFI = .95; SRMR = .06; see Figure 1 for the factor structure of the SEARS-A in youth 8- to 20-years-old).

Factor structure of the Social and Emotional Assets and Resilience Scale–Adolescent in youth 8- to 20-years-old.
Measurement Invariance
As shown in Table 2, the SEARS-A was found to be invariant across age, health status (cancer or comparison), gender, race, and SES. Demonstrating configural invariance, all models at the configural level demonstrated acceptable model fit. At the metric and scalar levels, all models demonstrated invariance as evidenced by nonsignificant changes in chi-square and changes in CFI that were less than −0.01.Table 2.
Overall Model Fit and Invariance Testing of the SEARS-A.
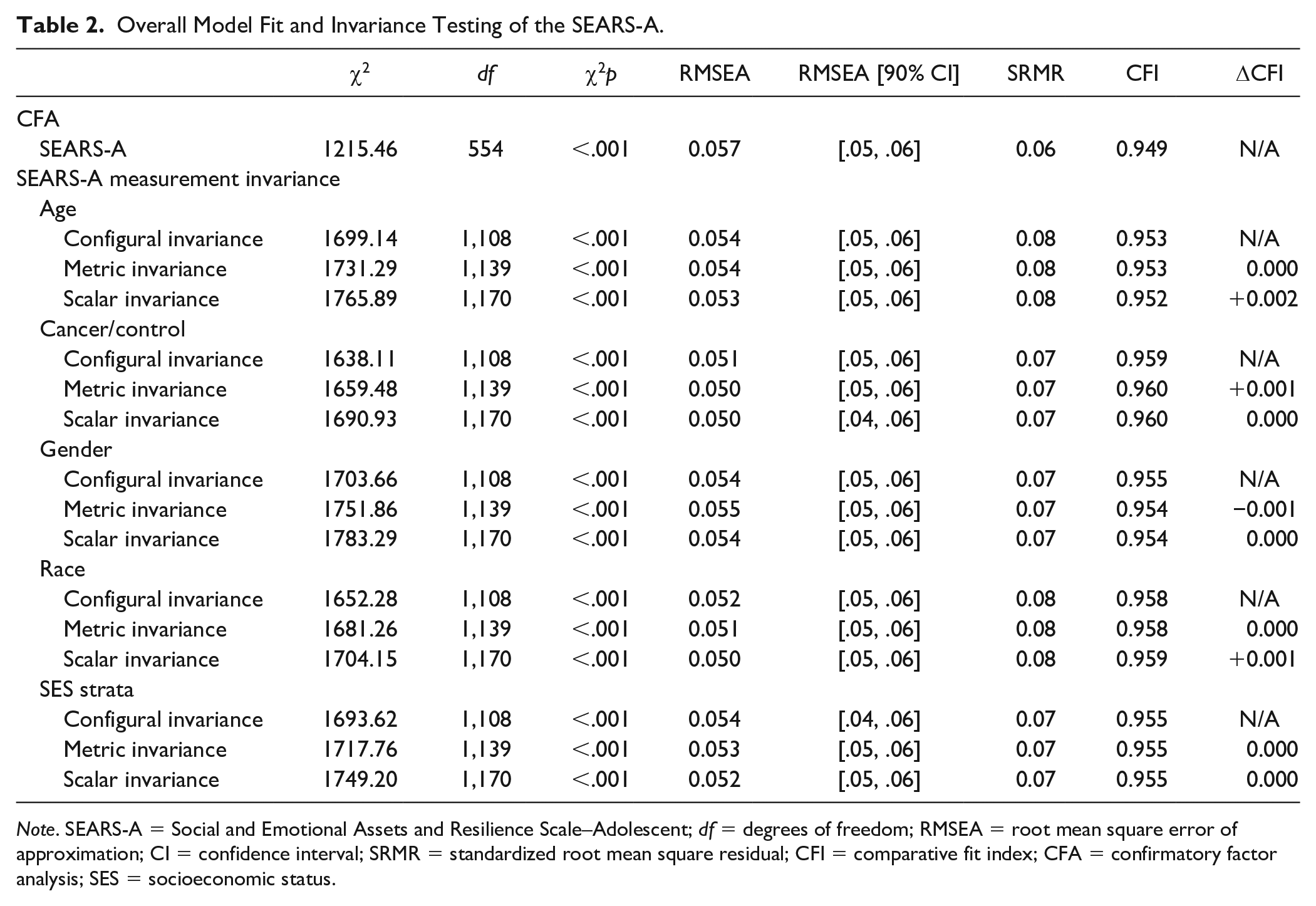
Note. SEARS-A = Social and Emotional Assets and Resilience Scale–Adolescent; df = degrees of freedom; RMSEA = root mean square error of approximation; CI = confidence interval; SRMR = standardized root mean square residual; CFI = comparative fit index; CFA = confirmatory factor analysis; SES = socioeconomic status.
Internal Reliability
Following demonstration of factorial invariance across age groups, we then examined internal reliabilities (α) of the four SEARS-A factors across the entire sample, and across the subsample of those aged 8 to 12 years. For the entire sample, reliabilities for Self-Regulation, Social Competence, Empathy, and Responsibility were, respectively, .872, .892, .895, and .821; for those aged 8 to 12 years they were .888, .878, .886, and .820.
Concurrent Validity
Having demonstrated factorial invariance and equivalent reliabilities across the full age range, the SEARS-A was used for all subsequent analyses of correlations and group differences between cancer and healthy comparison samples. In the cancer group, all correlations between the SEARS-A and SEARS-P were significant, generally in the small to moderate range (r = .24-.46). In contrast, in the healthy comparison group, parent–child correlations were much smaller, reaching significance only on the social competence subscales (r = .04-.21).
Criterion Validity
Within both groups, the subscales of SEARS correlated highly with subscales on the BASC 2 in the expected directions. Correlations were higher when from the same informant than cross-informant. Generally, correlations of SEARS subscales with strength-based scales of the BASC 2 (BASC 2-SRP Personal Adjustment: r = .52-.65, for the cancer group and r = .60-.73, for the comparison group Ego Strength: r = .43-.60, for the cancer group, and r = .48-.67, for the comparison group; BASC 2-PRS Adaptive Skills: r = .30-.80, for the caner group and r = .14-.78, for the comparison group, and Resiliency: r = .27-.72, for the cancer group and r = .19-.74, for the comparison group) were larger than were the inverse correlations with the problem behavior scales (BASC 2-SRP Internalizing Problems: r = .25-.37, for the cancer group, and .11-.53, for the comparison group; BASC 2-PRS Internalizing Problems: r = .02-.14, for the cancer group and r = .24-.38, for the comparison group, Externalizing Problems: r = .14-.31, for the cancer group and r = .14-.34, for the comparison group).
As mentioned previously, T-scores of the SEARS were utilized in the current study. While T-scores of the SEARS are not age or gender corrected, we chose to run additional analyses to further evaluate correlations and group differences between raw subscale scores of the SEARS-A and demographic factors. A small, yet significant correlation was found between age and the Empathy raw subscale score of the SEARS-A (r = .176, p < .01). All other subscales are nonsignificant, and correlations are essentially identical whether using raw scores or T-scores. A significant difference was found between males and females on the Empathy raw subscale of the SEARS-A, with higher ratings among females compared with males (t = 3.74, p < .001, raw scores; t = 3.77, p < .001, T-scores).
Discussion
The SEARS assessment system was originally developed as a measure of social–emotional predictors of resilience among school-aged children and adolescents (Merrell, 2011). The purpose of the present study was to evaluate psychometric prosperities of the SEARS-A in youth across a broader age range (8-20 years of age) and to examine the utility of the SEARS instruments in comparison with another well-established measure of psychological adjustment. The four-factor structure of the SEARS-A (i.e., self-regulation, social competence, empathy, and responsibility) was found to have an adequate factor structure and demonstrated invariance across domains of age, health status, gender, race, and SES. The internal reliabilities of the four factors were excellent across the full age range and were nearly identical in the subsample of those 8 to 12 years old. Taken together, our results suggest that for youth self-report, a single measure, the SEARS-A, can be used with children as young as 8 years, and has the potential to be a useful tool for predicting social–emotional adjustment outcomes in the context of adversity or stress.
In considering the utility of the SEARS multi-informant system, a shortcoming of prior work is the absence of any data regarding interrater or cross-informant reliability. It is curious that the SEARS manual, which describes youth, parent, and teacher report versions, does not mention anything about parent–child, parent–teacher, or teacher–child correlations. The current data from our community comparison group showed generally poor parent–child correlations between SEARS-A and SEARS-P subscales, reaching a marginal level of significance only on the common social competence scales. Although low to moderate parent–child correlations on measures of youth mental health and psychosocial functioning have long been recognized (Achenbach, 2011; De Los Reyes et al., 2015; De Los Reyes & Kazdin, 2005), the near zero correlations observed here are concerning, particularly given the conceptual similarity of the subscales and overlapping item content. It is not clear why cross-informant ratings in domains such as self-regulation, responsibility, and empathy would be less consistent than those typically seen with ratings of internalizing/externalizing behaviors or adaptive skills, but this is an apparent shortcoming of the measure that will require further examination. With that said, the factor structure of the two versions is different—three factors for the parent, four for the adolescent—so it may be that these respondents are considering these items differently. However, a complete examination of the factor structure of the SEARS-P was beyond the scope of this study. Given that the other psychometric properties of the SEARS were adequate, this lack of concordance between parent- and self-report should not dissuade others from use of the measure, but it is a noteworthy limitation of the scale, and needs to be examined in future work.
In contrast, parent–youth correlations in the cancer group were all statistically significant, in the low to moderate range, and comparable to what is commonly seen in widely used behavioral scales such as the BASC-2. Perhaps there are elements of the childhood cancer experience that facilitate parents becoming more attuned to their child’s emotional strengths and weaknesses. Certainly, during the child’s active cancer treatment, parents may have more opportunities to observe their child manage daily stressors related to their cancer experience, and thus become more aware of their child’s assets for resilience in the face of challenge. It will be important for future research to continue to examine concordance between self- and proxy-ratings on the SEARS, and to do so in other populations that face adversity, whether that be other serious illness populations or some other sort of challenge.
Although parent–child correlations were higher in the cancer group, correlations of the SEARS subscales with outcomes on the BASC-2 were observed similarly in both groups. Not surprisingly, correlations within the same informant, that is, SEARS-A with BASC-2 SRP and SEARS-P with BASC-2 PRS, were substantially higher than across informants. In general, the within informant correlations of the SEARS subscales were greater with the strength-based outcomes of the BASC, than were the inverse correlations with the problem behavior scales; this was true for both youth and parent report, and in cancer and comparison groups. These findings add to the incremental validity of the SEARS scales and are among the first to demonstrate predictive validity with commonly used behavioral outcomes.
Findings from this articles must be interpreted in light of limitations. First, authors of the present study chose to examine the published factor structure of the SEARS-A (Merrell, 2011) instead of using exploratory methods to systematically evaluate the underlying theoretical structure of the SEARS-A. The factor structure was retained as it has previously validated in student populations (Cohn et al., 2009). Second, with the inclusion of 8-year-old to 12-year-old and 19- and 20-year-old participants, we were forced to extend T-score conversions on the SEARS to ages that were not available within the manual. As such, it is possible that the resulting scores for these youth were either over- or underestimated. However, given that values do not appear to vary considerably by age, per the manual and our own analyses, we felt comfortable making this choice, and in using T-scores rather than raw scores. Future work will be needed to determine appropriate T-scores for older and younger respondents on the SEARS. Third, while this study was able to extend knowledge on many psychometric properties, we were not able to examine test-retest reliability or stability. As such, future work will be needed to examine these factors, and especially to do so in an illness or other challenge sample. Finally, while we were able to obtain both self- and parent-report assessments, we did not include teacher reports. It will be important for future studies to confirm the psychometric properties of the teacher-report version of the SEARS, and to examine concordance with parent- and self-report, particularly given the near zero associations found between parent- and adolescent-report in this sample.
Ultimately, findings from this study provide support for the use of the SEARS assessment system as a means of assessing the social–emotional predictors of resilience. Indeed, we were able to provide support for the four-factor solution of the self-report version to be applicable for the full range of respondents—8 to 20 years—which will increase the utility of the SEARS in both wide age range cross-sectional studies, as well as longitudinal reports. Furthermore, we demonstrated that the psychometric properties of the SEARS remain intact within a childhood cancer sample, providing support for its use within at-risk populations, such as youth who have experienced a challenge such as a serious illness. Results of this study suggest that the SEARS-A has the potential to be a useful tool to identify specific social–emotional strengths among at-risk youth. Information from the SEARS-A can be used by clinicians to provide targeted interventions that bolster youths’ strengths that promote healthy psychological adjustment and resilience. It will be beneficial for future work to determine the clinical utility of the SEARS-A, as well as its potential as a means of assessing change in the context of intervention.
Supplemental Material
sj-docx-1-asm-10.1177_10731911211022844 – Supplemental material for Examination of the Social Emotional Assets and Resilience Scales (SEARS) Youth Report: Factor Structure, Measurement Invariance, and Validity
Supplemental material, sj-docx-1-asm-10.1177_10731911211022844 for Examination of the Social Emotional Assets and Resilience Scales (SEARS) Youth Report: Factor Structure, Measurement Invariance, and Validity by Kimberly L. Klages, Richard F. Ittenbach, Alanna Long, Victoria W. Willard and Sean Phipps in Assessment
Supplemental Material
sj-docx-2-asm-10.1177_10731911211022844 – Supplemental material for Examination of the Social Emotional Assets and Resilience Scales (SEARS) Youth Report: Factor Structure, Measurement Invariance, and Validity
Supplemental material, sj-docx-2-asm-10.1177_10731911211022844 for Examination of the Social Emotional Assets and Resilience Scales (SEARS) Youth Report: Factor Structure, Measurement Invariance, and Validity by Kimberly L. Klages, Richard F. Ittenbach, Alanna Long, Victoria W. Willard and Sean Phipps in Assessment
Supplemental Material
sj-docx-3-asm-10.1177_10731911211022844 – Supplemental material for Examination of the Social Emotional Assets and Resilience Scales (SEARS) Youth Report: Factor Structure, Measurement Invariance, and Validity
Supplemental material, sj-docx-3-asm-10.1177_10731911211022844 for Examination of the Social Emotional Assets and Resilience Scales (SEARS) Youth Report: Factor Structure, Measurement Invariance, and Validity by Kimberly L. Klages, Richard F. Ittenbach, Alanna Long, Victoria W. Willard and Sean Phipps in Assessment
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.