
Abstract
This study assessed the feasibility of a multi-domain measure of the occurrence, impact, and timing of childhood/adolescent psychological adversity exposure, the Subjective Impact and Timing of Adversity Scale (SITA). Participants were from among those who had previously participated in two waves of data collection when aged approximately 14 and 21 years. Internal consistency estimates at both online and interview stages were acceptable for all SITA domains (with the exception of parental loss). SITA domain scores correlated meaningfully with scores on other scales and psychological measures, supporting convergent validity. Those with lifetime psychiatric diagnoses scored significantly higher on SITA domains than those not meeting diagnostic threshold. There was evidence of the importance of both the subjective impact and timing of adversity with regard to psychiatric diagnoses. The study demonstrates the viability of the SITA; however, further studies are required to substantiate these findings in larger samples.
Since the landmark adverse childhood experiences (ACEs) study (Felitti et al., 1998), a large number of studies and meta-analytical reviews have demonstrated a link between adversity and negative health outcomes, particularly in the area of psychiatry (e.g., Li et al., 2016; Varese et al., 2012). Measuring childhood adversity is complex (Danese, 2020), with terms such as adverse childhood experience, childhood trauma, childhood adversity, and childhood maltreatment used interchangeably (Petruccelli et al., 2019). The experience of childhood adversity deleteriously affects development (Jaffee et al., 2018; McKay, Cannon et al., 2021) and can negatively impact health and well-being into adulthood (Agnew-Blais & Danese, 2016; Anda et al., 2009; Hughes et al., 2017). A lot of the adversity literature relies on retrospective recall (Danese, 2020), with potential biases resulting from memory difficulties, confusion about past events, and bias owing to concurrent health issues (Monroe, 2008). Therefore, because the majority of studies examining the relationship between adversity and psychiatric disorder do so retrospectively, it is important that adversity is assessed in as complete (in terms of occurrence, timing, and impact) a way as possible, using multiple items to try to capture the deleterious impact of adversity in different domains. For example, to only assess sibling bullying could be potentially to miss the negative experience of having been bullied by peers at school.
The number and extent of adversities being assessed have increased over the years (Bethell et al., 2017; Cronholm et al., 2015; Felitti et al., 1998) and a recent scoping review of ACE screening tools (SmithBattle et al., 2022) supported the expansion of these to include a wider range of adversities, particularly beyond family and household adversities. However, and of note, these authors also stressed the need for screening tools that are brief, and easy-to-complete, if they are to be clinically useful and acceptable to patients. Given the difficulty in attempting to measure the breadth of adversity in a user-friendly way, SmithBattle et al. (2022) suggested that any given ACE screening tool is unlikely to exhaust the totality of childhood adversity exposures. The present study reports on the feasibility of a measure of childhood adversity that may be particularly useful in the area of psychiatry, and more broadly, mental well-being.
Given that there is a wide (and increasing) spectrum of possible childhood adversities, knowing which to assess in a given sample can be difficult. A recent systematic review and meta-analysis (McKay, Cannon et al., 2021) reported a significant relationship between nine forms of adversity exposure and adult-diagnosed psychiatric disorder, namely, bullying victim, bullying perpetrator, being both a victim and a perpetrator, frequency of bullying, emotional abuse, physical neglect, maltreatment (not specified), multiple maltreatment, and parental loss. Of note, there was a nonsignificant association between both sexual abuse, and physical abuse, and adult psychiatric diagnoses. The authors attributed this to the nature of the studies meeting inclusion criteria. In short, the adversities that emerged as important for the development of psychiatric disorder clustered around the household/family and peer environments. Accordingly, the development of the present tool was in line with the outcomes of the McKay, Cannon et al. (2021) review and was with specific focus on the potential relationship between the experience of adversity and subsequent psychiatric morbidity.
Some have reported poor concordance between prospectively and retrospectively reported exposure to childhood adversities (Baldwin et al., 2019; Latham et al., 2021) with greater concordance being found where interviews were used rather than questionnaires, and also in studies with smaller sample sizes (Danese, 2020). However, the extant literature is replete with studies assessing adversity retrospectively with tools such as the Childhood Trauma Questionnaire (CTQ; Bernstein et al., 1997) or the Traumatic Life Events Questionnaire (TLEQ; Kubany et al., 2000). These measures are not without limitations. While the CTQ assesses the occurrence of adversity experienced in childhood in five domains (physical abuse/neglect, emotional abuse/neglect, and sexual abuse), the TLEQ assesses a wide range of adversities experienced across the life span, ranging from natural disasters, to experience of combat, to adult physical or sexual assault. In research examining the specific impact of childhood adversity on adult psychiatric disorder, instruments such as the TLEQ provide limited utility. In a systematic review of tools used to measure ACEs, Bethell et al. (2017) reported that of the 14 assessment tools meeting their review criteria, between six and 20 different constructs were assessed, with only four common across all measures, namely, domestic violence, parental incarceration, household mental illness/suicide, and household substance abuse. In short, there are a wide variety of scales currently in existence, all measuring various elements of childhood adversity. A key rationale for the development of the scale reported here is the focus on early life adversities that have the strongest associations with psychiatric disorder in adulthood.
Specifically, the present study was motivated by a number of key factors: first, the results of the McKay, Cannon et al.’s 2021 systematic review and meta-analysis, pointing to key childhood adversities that have lasting psychiatric impact into adulthood. Accordingly, a psychometrically sound tool assessing these adversities in early life may have the potential to be able to identify those at particular risk of future psychiatric disorder. Second, we were keen to develop a measure that would not merely provide a count of adversities experienced, but which would also assess the subjective impact of those adversity forms. We contend that merely counting how many forms of adversity have been experienced implies that all adversities experienced are appraised to an equally deleterious or negative degree. Finally, we were keen to include a third element, namely, the timing of the exposure, in an attempt to ascertain if this contributed negatively to outcomes resulting from exposure to adversity. It is noteworthy that in their review of ACEs tools, Bethell et al. (2017) reported that only a small minority of tools assess any degree of age, frequency, intensity, or effect of adversity exposure.
The majority of those experiencing adult psychopathology did not experience childhood adversity and not all individuals who experience adversity go on to develop psychopathology (Baldwin et al., 2021; Baldwin & Danese, 2021; Danese, 2020). Therefore, the subjective experience of the adversity and the wider environmental context likely contribute to the development of psychopathology. The idea that there is an interplay between risk and resilience in the development of disorders is not new (Bonanno et al., 2011; Rutter, 2013). However, still, the vast majority of assessment of childhood adversities assesses only the occurrence and not the impact of such adversity. In the development of the five-item Subjective Trauma Outlook (STO; Palgi et al., 2017), authors differentiated between two trauma-related layers that they called the phenomenological-external layer (the observed trauma response used for diagnostic purposes) and the inner psychological layer (an internal and subjective response to trauma). The STO assesses the subjective impact of traumatic experiences, with items examining psychological impact, the “control” of trauma over life, and the “fracturing” of life and experience as a result of trauma exposure.
It has further been suggested that the overall number of ACEs is directly related to health outcomes (Baldwin et al., 2021; Hughes et al., 2017). In a practitioners review article, Lacey and Minnis (2020) recently underlined a number of considerations and made a number of recommendations for future research. Among these were that research should be conducted on the clustering of ACEs and their relative prognostic significance, both individually and in combination; that researchers consider including information on the perceived severity or effect of experience; and that the timing and duration of the experience be taken into account when assessing adversity. Based on all of this, we aimed to examine the feasibility of a measure of childhood adversity, based on the risk factors for adult-diagnosed psychiatric disorder identified by McKay, Cannon et al. (2021), a first step in the development of a potentially useful risk assessment tool.
The Present Study
The present study is a direct response to the issues delineated above. (a) Adversity domains assessed: In the first instance, and based on the literature broadly, but on the McKay, Cannon et al. (2021) review more specifically, items were purposively chosen to enquire about the adversity domains which that particular meta-analysis revealed had the strongest evidence for an association with adverse mental health outcomes in adulthood. (b) Subjective impact: The present study included an assessment of the subjective impact of adversities experienced. This is an important element in adversity exposure, namely, the fact that different people react to similar exposures in very different ways and that the impact of a particular form of adversity (e.g., emotional abuse) may be experienced to varying degrees in different individuals. (c) Finally, and in line with the recommendation of Lacey and Minnis (2020), the present study examined in which developmental periods specific adversities were experienced.
Method
Participants
The study population comprised individuals who had previously taken part in the first two waves of the Challenging Times Study (for study details see Lynch et al., 2006), which had initially been established to investigate the prevalence of psychiatric disorders among Irish adolescents aged 12 to 15 years at Wave 1 (N = 723; Mage = 13.4 years, 53% female). Those who participated at the second wave of data collection and who had given consent to be recontacted (N = 169; Mage = 20.8 years, 53.8% female) were telephoned and or/emailed, and where necessary, letters were sent to the last known domiciliary address. In the majority of these cases, contact was not made. Four previous participants were reported to have died in the interim by a relative. Finally, a number of individuals reported themselves unable to participate owing to current life stresses. Participants at this wave received €50 in shopping vouchers in return for participation.
There were three elements to the present study. First, participants completed an online questionnaire using the Qualtrics platform. Approximately 3 weeks later, a large proportion of these individuals took part in a structured interview with one of the authors (M.T.M.). The third element of the study was to link the responses given at these two times, to data previously gathered.
Materials—Online Questionnaire
The Subjective Impact and Timing of Adversity Scale (SITA)
Items were first generated by two individuals (M.T.M. and L.O.) and assessed by a third individual (M.C.C.). Items were generated ex nihilo with a background knowledge of the ACEs literature, and knowledge of other preexisting measures, but without direct recourse to these. Items were in domains that reflected the findings of the systematic review of McKay, Cannon et al. (2021), namely, physical abuse and neglect, emotional abuse and neglect, sexual abuse, parental loss, and bullying (both perpetration and victimhood). The parental loss domain included items enquiring about parental death, separation, divorce, incarceration, and parents/children spending “long periods of time” away from home. All items were assessed by a variety of psychiatrists, educational psychologists, and schoolteachers for readability, and content appropriateness. Items were modified, combined, or dropped based on these assessments. Items were assessed for readability using the online Flesch–Kincaid tool and language was modified in order that readability was determined to be appropriate for those in Grade 7 of the U.S. educational system. This process yielded a questionnaire consisting of 79 items.
Assessment of the Occurrence of Adversity
The SITA assesses adversity experience in eight domains. Bullying victimhood was measured using 10 items (e.g., “I was bullied by other children when I was growing up”), bullying perpetration (six items, for example, “When I was growing up I made fun of how other children looked or sounded”), emotional abuse (EA; 18 items, for example, “When I was growing up my Mam or Dad called me mean or hurtful names”), emotional neglect (EN; five items, for example, “When I was growing up my Mum or Dad did not celebrate my birthday”), physical abuse (PA; seven items, for example, “I remember being hit so hard by my Mum or Dad that it hurt”), physical neglect (PN; 11 items, for example, “Growing up my clothes were smelly and not clean”), sexual abuse (SA; nine items, for example, “Growing up, someone whom I didn’t know touched my private parts”), and parental loss (PL; nine items, for example, “Growing up I lived away from my Mum or Dad for what seemed like a long time,” or “When I was growing up my Mum or Dad spent time in prison”). All items are displayed in Supplemental Table S1. Four items were filler items (e.g., “I would not wish my childhood on other children”). Items were scored 1 = never through 5 = all the time. Items with a binary response option (e.g., “One or both of my parents died before I turned 18”) were scored 1 = no and 5 = yes. Cronbach’s alpha estimates in the present study were as follows for online/interview administration, respectively: bully victim = .90/.92; bully perpetrator = .75/.83; emotional abuse = .91/.89; emotional neglect = .81/.82; physical abuse = .87/.90; physical neglect = .76/.71; sexual abuse = .81/.82; and parental loss = .67/.61. Regarding the lower-than-ideal internal consistency for parental loss, please see Supplemental Section B for a discussion of this.
Assessment of the Subjective Impact of Trauma
Additional to the assessment of adversity itself, participants also completed a modified version of the STO (Palgi et al., 2017). Subjective traumatic outlook is defined as people’s evaluation of themselves as traumatized when comparing their pre- and postevent conditions. Participants were asked to reflect on each of the adversity domains where they had endorsed any item (e.g., sexual abuse) and to respond to five questions (e.g., Looking at your life now, do you feel that you suffer psychologically as a result of having experienced sexual abuse?). Original response options (NA = 1; not at all = 2; a little = 3; moderately = 4; much = 5; very much = 6) were recoded as follows: NA or not at all = 0; a little = 1; moderately = 2; much = 3; very Much = 4). Subjective impact degree was determined by totaling the responses to the five items within each domain. Subjective impact was assessed for bullying victimhood, EA, PA, PN, SA, and PL. The scale has previously shown good psychometric, convergent, and discriminant validity (Mahat-Shamir et al., 2019; Palgi et al., 2017). Cronbach’s alpha estimates in the present study were as follows for online/interview, respectively: bullying victim = .86/.65, emotional abuse = .91/.92, physical abuse = .82/.91, physical neglect = .90/.95, sexual abuse = .98/.98, and parental loss = .93/.68.
Assessment of the Timing of Adversity Exposure
Participants were asked to indicate at what point in their lives they had been exposed to the adversity. For each domain, participants were asked to indicate yes/no for the period: birth to age 6, 7 to 11 years, and 12 to 17 years. These temporal bands were purposively chosen in an attempt to aid recall, as they broadly correspond to preschool, primary school, and secondary school historical periods.
The CTQ
The CTQ (Bernstein et al., 1997; Bernstein & Fink, 1998) is widely used to measure childhood maltreatment. The CTQ uses five items each to assess five types of maltreatment: EA, EN, PA, PN, and SA. Each item is scored on a 5-point Likert-type scale (ranging from never true to very often true). The instrument includes a three-item minimization scale (e.g., “best family in the world”) that gives an estimate of response validity (the tendency to idealize one’s family). A total severity score can be obtained by summing the scores for the 25 items (three minimization items excluded). Subscale scores can be created in the same manner. In addition, a multiplicity score is generated based on scores above cutoff on the five subscales (Bernstein & Fink, 1998). In the present analyses, mean CTQ domain scores were computed in order that scores on this measure and the SITA could be compared. Cronbach’s alpha estimates in the present study were as follows: CTQ-EA = .80, CTQ-EN = .90, CTQ-PA = .68, CTQ-PN = .44, and CTQ-SA = 95.
The Adolescent and Adult Time Inventory–Time Attitudes Scale
We assessed how individuals felt about the past, present, and future, using the Adolescent and Adult Time Inventory–Time Attitudes Scale (AATI-TA; Mello et al., 2016; Mello & Worrell, 2007). This is constituted of 30 items, with six latent factors, each evaluated on a 5-point Likert-type scale ranging from 1 (totally disagree) to 5 (totally agree). The factors are as follows: past negative (five items; for example, “My past is a time in my life that I would like to forget”), past positive (five items; for example, “I have very happy memories of my childhood”), present negative (five items; for example, “I am not satisfied with my life right now”), present positive (five items; for example, “I am happy with my current life”), future negative (five items; for example, “I doubt I will make something of myself”), and future positive (five items; “My future makes me happy”). For each subscale, the score is computed by summing the responses and dividing the sum by the number of items for each subscale. A recent comprehensive review of the psychometric properties of the scale showed scores to be psychometrically valid and internally consistent in both adolescents and adults (McKay, Healy, & O’Donnell, 2021). Cronbach’s alpha estimates in the present study were as follows: past positive = .87; past negative = .92; present positive = .95; present negative = .87; future positive = .93; and future negative = .84.
Materials—Telephone Interviews
Approximately 3 weeks after completing the online questionnaire, participants were invited to take part in a telephone interview. Interviews were conducted by telephone as a result of Covid-19 lockdowns prohibiting the use of university facilities. This allowed comparison of scoring on the SITA domains not only across time but also across different administration forms (online platform vs. telephone interview).
The Structured Clinical Interview for DSM -5 Disorders–Research Version (SCID-5-RV)
The SCID-5-RV (American Psychiatric Association, 2015) is a comprehensive semi-structured psychiatric interview guide that includes diagnostic assessment of all major Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) disorders, including subtypes, severity, and course specifiers. The Research Version allows for the customization of the interview to the specific needs of a study. It was designed for administration by a clinician or a trained mental health professional familiar with the DSM-5 diagnostic system. However, nonclinicians can administer the SCID-5-RV with appropriate training and supervision (First et al., 2015). In the current study, the SCID-5-RV was administered by a trained postdoctoral researcher. Training included receiving in-person instruction from researchers with specialized SCID training, viewing instructional videos, and participating in role-plays and mock interviews. The interviewer also received ongoing support from a psychiatrist. The SITA, including subjective impact and age of exposures, was also readministered during the telephone interview.
Materials—Longitudinal Analyses
We were able to analyze the association between current reports of adverse experiences with previously reported stressful life experiences as well as with previous reports of psychological, social, and occupational functioning. These assessment were carried out at previous waves of data collection.
The Strengths and Difficulties Questionnaire (SDQ; R. Goodman, 1987, administered at Wave 1) is a brief behavioral screening questionnaire, which asks about 25 positive and negative personal attributes. The 25 items are divided into five scales, namely, conduct, hyperactivity, emotional, peer problems and pro-social, with five items in each scale. All but the pro-social scale is summed to generate a total difficulties score. Internal consistency has been found to be to be acceptable (R. Goodman et al., 2000) with Cronbach’s alpha yielding a coefficient of .73.
The Stressful Life Events Screening Questionnaire (SLESQ; L. Goodman et al., 1998, Wave 2) is a 13-item self-report measure for nontreatment-seeking samples that assesses lifetime exposure to traumatic events. Eleven specific and two general categories of events, such as a life-threatening accident, physical and sexual abuse, and witness to another person being killed or assaulted, are examined. For each event, respondents are asked to indicate whether the event occurred (“yes” or “no”), their age at the time of the event, and other specific items related to the event, such as the frequency, duration, whether anyone died, or was hospitalization. The SLESQ is recommended for research and general screening purposes.
The Children’s Global Assessment Scale (CGAS; Shaffer et al., 1983, Wave 1) was originally created as an adaptation of the Global Assessment Scale for adults (Endicott et al., 1976) and designed to reflect the lowest level of functioning for children during a specified time period. It has values from 1, representing the lowest level of functioning, to 100, representing the highest. Scores above 70 represent normal functioning. The questionnaire is divided into different categories of impairment every 10 points, which the rater first decides on (e.g., 31–40: Serious Problems), before assigning a score within the category. The CGAS has been used extensively in clinical and research settings.
Psychological, social, and occupational functioning were assessed with the Global Assessment of Functioning Scale (GAF), a numerical rating scale from 1 to 100 usually reported on the Axis V of the multiaxial diagnostic system in Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV, American Psychiatric Association, 1994). A higher rating indicates better current psychosocial functioning.
Statistical Analyses
Internal consistency scores (α) were computed for all SITA domains. In addition, individual item mean (+standard deviation), skew and kurtosis values were computed for all items. To give an indication of the stability of SITA scores, correlations were computed between SITA scores at the online questionnaire and the structured interview (at +3 weeks). Convergent validity of SITA scores was examined by comparing SITA domain scores with equivalent scores on the CTQ (for the domains of PA, PN, EA, EN, and SA). Convergent validity was also examined by comparing SITA mean scores with scores on the AATI-TA domains. Here, higher adversity scores would be expected to be associated with higher scores on past negative and lower scores on past positive. Mean SITA domain scores were examined against results on the SCID-5-RV (disorder yes/no). Here, Hedges’s g values (rather that p value) were used to interpret results. This was because of the small sample size, and Hedges’s g is a sample-size-adjusted equivalent of Cohen’s d. To examine the potential combined influence of adversity experience and subjective impact (for the domains of bullying victimhood, EA, PA, Neglect, SA and PL), participants were allocated to one of three categories: (a) no adversity, no impact; (b) adversity, no impact; and (c) both adversity and impact. The proportion of participants in these categories was then examined against lifetime SCID-5-RV diagnoses.
Because the timing of adversity was related to subjective impact, these same adversity domains were used to examine the relationship between SCID-5-RV lifetime diagnoses and the timing of adversity. Timing was assessed as “in primary school only” (birth to age 11), “in secondary school only” (age 12–17), or both. In addition, scores from this wave of data collection were examined against responses given for both adversity exposure in the past (at ages 14 and 20) and also for scores on the SDQ, SLE questionnaire, CGAS, and the GAF questionnaire at previous waves of data collection.
Given the small sample size, we employed the guidelines recommended by Funder and Ozer (2019) for the interpretation of effect sizes. Accordingly, these were as follows: small effect = .10; medium effect = .20; and large effect ≥ .30.
Results
Results presented in the main text relate to the SCID-5-RV lifetime diagnoses and criterion variables gathered at the online questionnaire. Additional results are detailed in Supplemental Materials. There were no missing data as the online platform was designed in such a way that participants could not proceed to the next page without full completion of the current one.
Descriptive Results
A total of N = 68 individuals of a possible 169 (40.2%; females = 43 [63.2%]; Mage = 33.43 [SD = 0.92]) participated. All participants were of White Irish ethnicity, with 23% reporting themselves to be married, 47% reporting themselves to have an undergraduate degree, and 78% reporting themselves to be in full-time employment.
Supplemental Table S1 shows the individual item mean (+standard deviation), variance, skew and kurtosis values for all SITA items. Results suggest that some items were redundant in this particular sample and that others offered little in terms of explanation of the SITA domains (low variance scores). Supplemental Table S2 shows the mean scores (+ standard errors) and the 95% confidence intervals for scores on all measures used at the online part of the study. Comparing mean CTQ and SITA scores was instructive. Mean SITA-EA score (d = .05), and SITA-PA (d = .54) were higher than their CTQ equivalent. Conversely, mean SITA-EN (d = .25), SITA-PN (d = .12), and SITA-SA (d = .11) were lower than their CTQ equivalent. Using Funder and Ozer’s (2019) guidelines, all but one of these effect sizes was interpretable. In sum, these results suggest that results on both the SITA and CTQ were closely aligned, and therefore that the SITA assessed exposure to adversity to a similar degree as the CTQ.
Internal Consistency and Consistency of Scores Across Time and Methodology
Figure 1 is a heat plot displaying correlation coefficients between scores on the SITA employed online and at telephone interview. Correlations between scores on the SITA administered in different ways at 3-week follow-up ranged from r = .51 to r = .83, indicating a large effect size (Funder & Ozer, 2019). These values do not represent classic test–retest reliability, given the differences in form of administration (online platform vs. telephone interview). The heat plot suggests that scores for bully perpetration, physical neglect, sexual abuse, and parental loss were particularly stable across time (+3 weeks) and methodology. In sum, this suggests that the SITA items functioned well, with acceptable internal consistency estimates.
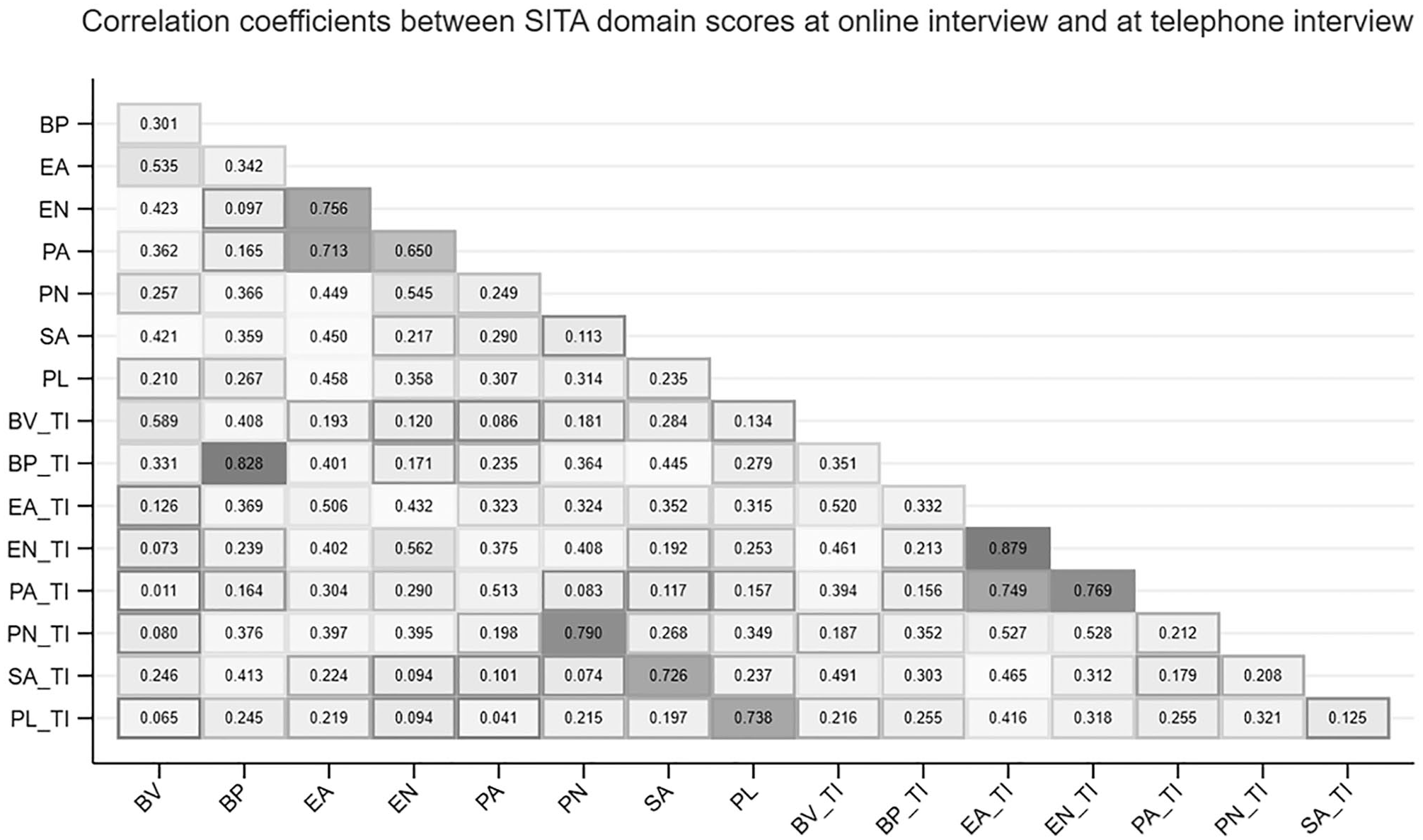
Pearson’s Correlations Between Scores on the Subjective Impact and Timing of Adversity Scale at Online Questionnaire and at the TI.
Convergent Validity
Figure 2 displays a heat map showing Pearson’s correlations between scores on the SITA, the CTQ, and the AATI-TA domains (all completed online). Comparable results comparing SITA interview scores, CTQ scores (online), and AATI-TI scores (online) are displayed in Supplemental Figure 1. The direction and magnitude of these correlations suggest adequate convergent validity between SITA and CTQ scores (.88 ≥ r ≥ .67; with an outlier for PN, r = .46). The magnitude of these relationships showed a substantial reduction when comparing SITA scores derived from telephone interviews and online CTQ scores (.55 < r > .26, see Supplemental Figure 1). Elsewhere in Figures 2 and S1, correlation coefficients between both SITA and CTQ scores, and scores on the AATI-TA suggest that higher self-reported levels of adversity were associated with higher past negative time attitudes and lower past positive time attitudes. An exception to this pattern was seen for physical neglect, where correlations with past, present, and future time attitudes were of a similar magnitude. These results suggest that higher levels of past adverse experience are related to how people feel about the past, more so than how they feel about the present, or the future, broadly speaking.
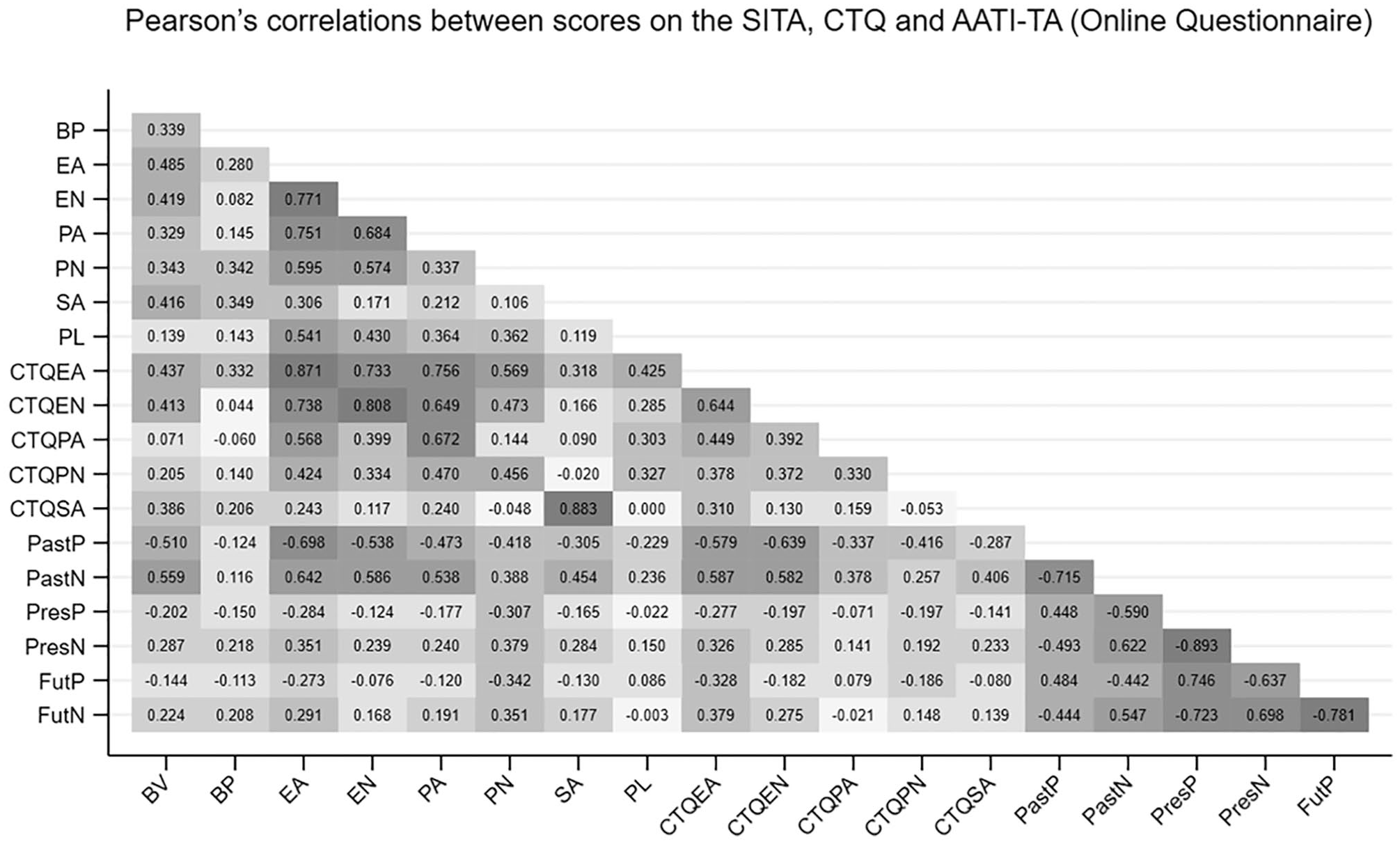
Pearson’s Correlations Between Scores on the Subjective Impact and Timing of Adversity Scale, the CTQ, and the Adolescent and Adult Time Inventory–Time Attitudes Scale.
To further examine the relationship between SITA domain scores and their equivalent CTQ score, planned contrasts based on procedures outlined by Meng and colleagues (1992) were used. In each case, the correlation coefficient between SITA domain and its CTQ equivalent was compared with the next highest (or higher) coefficient between that SITA domain and other CTQ domains. Results at the online questionnaire indicated that SITA-SA (Z = 8.40, p < .05) and SITA-EA (Z = 3.04, p < .05) were more strongly related to CTQ-SA and CTQ-EA, respectively, than any other CTQ domain. No other comparisons using the online data were statistically significant. Using SITA data gathered at the telephone interview indicated that SITA-SA (Z = 3.21, p < .05), and SITA-EN (Z = 2.11, p < .05) were more strongly related to CTQ-SA and CTQ-EN, respectively, than any other CTQ domain. Again, there were no other statistically significant findings.
Results Using Lifetime Disorder Diagnoses
Given the small number of participants, mental disorders were analyzed as follows: (a) mood disorders, (b) mood or anxiety disorders, and (c) any disorders. Table 1 displays differences in mean adversity score (SITA and CTQ) between individuals meeting threshold for disorders on the SCID-5-RV and those not. Results for all individual disorder categories are displayed in Supplemental Table S3. A discussion of the difference between adversity scores at online questionnaire and at telephone interview is also contained in Supplemental Materials. The majority of comparisons attained a large-sized threshold (Funder & Ozer, 2019), with higher mean adversity scores observed in those reporting lifetime disorder in the three categories of disorder.
Scores on the SITA, and the CTQ, by Disorder Categories.

Note. Shown are means (+SD) and Hedges’s g effect sizes. SITA = Subjective Impact and Timing of Adversity Scale; CTQ = Childhood Trauma Questionnaire.
Adversity Plus Subjective Impact
Table 2 displays results of a cross-tabulation for lifetime SCID-5-RV disorder and the categories of (a) no adversity/no subjective impact, (b) adversity/no subjective impact, and (c) adversity plus self-reported subjective impact. Full results comparing SITA administered online and at telephone interview are displayed in Supplemental Table S4, and full comparable results by individual disorder in Supplemental Table S5. Confining results to those where the Fisher’s exact test yielded a statistically significant result (Table 3, shaded) is instructive. Results point to a relationship between adversity and subjective impact being particularly relevant in the domains of EA and PA. However, while statistical significance was not always attained, in all cases, the majority of individuals reporting both adversity and impact also met threshold for lifetime SCID-5-RV diagnosis. For example, of the 24 individuals reporting both EA and EA-subjective impact, 22 also met threshold for either a lifetime mood or anxiety disorder.
Proportions of Individuals in Adversity/Impact Categories.
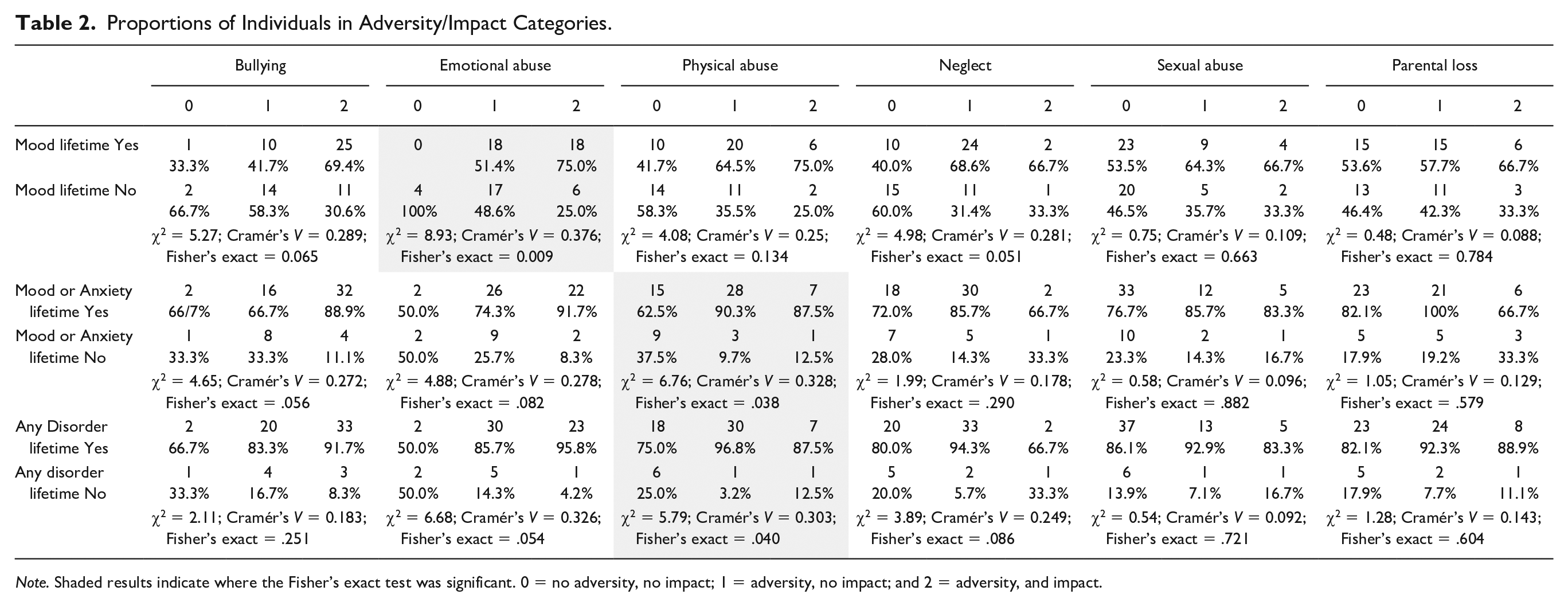
Note. Shaded results indicate where the Fisher’s exact test was significant. 0 = no adversity, no impact; 1 = adversity, no impact; and 2 = adversity, and impact.
Comparison of Proportions of Individuals With/Without Lifetime Mental Disorder and Adversity/Timing Categories.
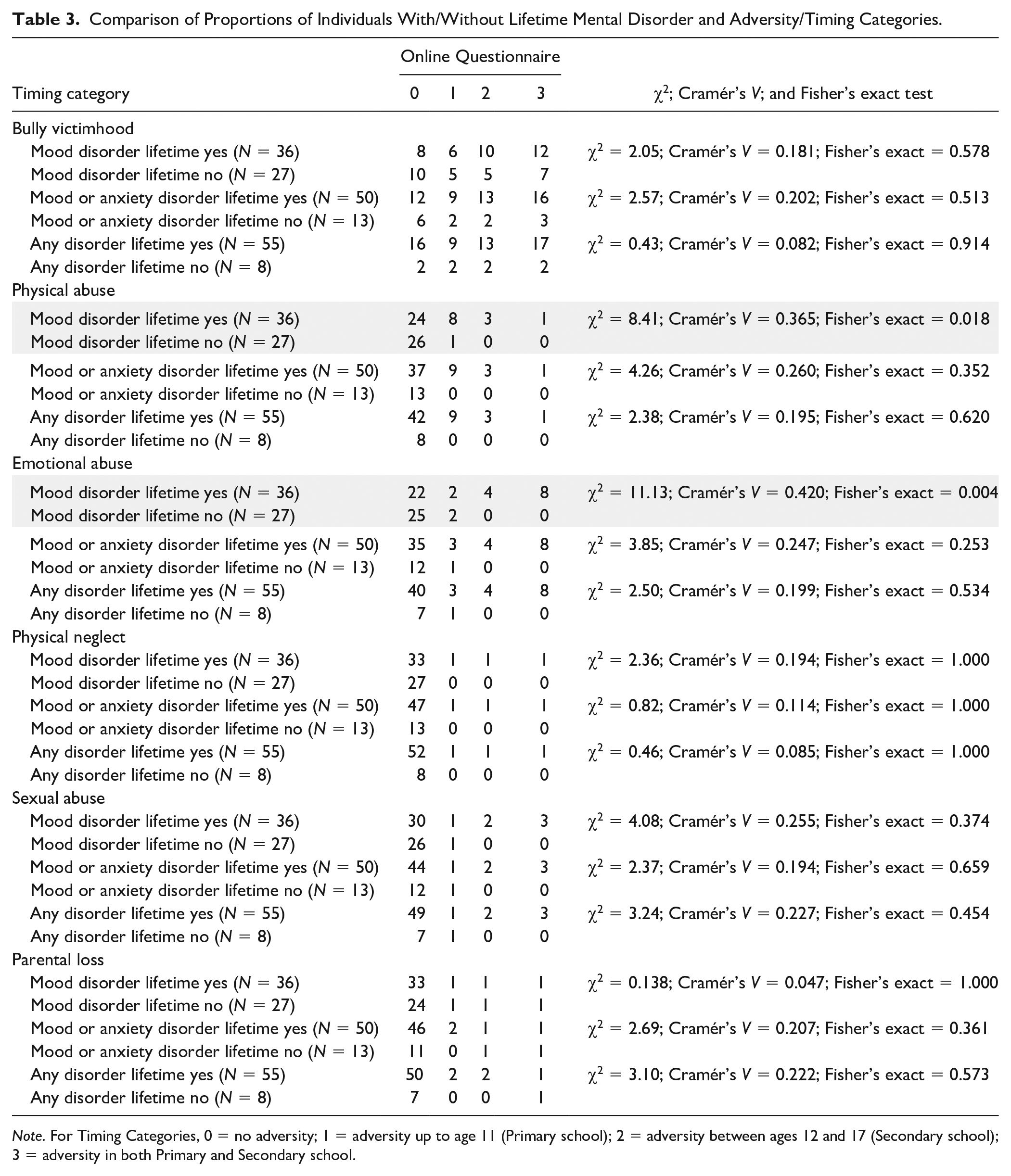
Note. For Timing Categories, 0 = no adversity; 1 = adversity up to age 11 (Primary school); 2 = adversity between ages 12 and 17 (Secondary school); 3 = adversity in both Primary and Secondary school.
Finally (Table 3), we examined the relationship between SCID-5-RV lifetime diagnoses and the timing of self-reported adversity exposure (for results comparing online and telephone interview responses, see Supplemental Table S6, and additionally for results by specific disorders, see Supplemental S7a–S7f). The timing categories of birth to age 6 and age 7 to 11 were collapsed owing to the relatively low amount of adversity indicated in the period up to age 6, and additionally to the fact that in interviews, many participants struggled to be sure of the timing of events in the early Primary school period (ages 5–8). Descriptive statistics point to a potentially important relationship between disorder, adversity, and timing. Taking PA as an example, results show that of the nine individuals reporting PA up to and including age 11, eight met the criteria for lifetime mood disorder and all met the criteria for any lifetime disorder. Again, looking at EA, of the eight individuals reporting this throughout their childhood, all met the criteria for lifetime mental disorder. In terms of the relationship between self-reported adversity (by domain) and number of lifetime disorders, the following Pearson’s correlation coefficients were observed: bully victim, r = .30; EA, r = .30; EN, r = .27; PA, r = .28, PN, r = .35, SA, r = .37, and PL, r = .07.
For longitudinal results, see Supplemental Section C. These results demonstrated adequate convergent validity of SITA scores against variables of consequence assessed some 12 and 18 (approximately) years earlier. As an example, we report two results here. As participants had also participated in two previous waves of data collection, it was possible to compare scores on the SITA with data reported previously. At Wave 2 (age ≈ 20 years), participants were asked whether there had been a split between the parents in their family. Those who said no at Wave 2 (N = 51) reported a lower SITA-PL score (Mparental loss = 1.139, .242) than those who had reported yes (N = 17; Mparental loss = 1.876, .517), Hedges’s g = 2.23. Similar analyses were undertaken for self-reported bullying victimhood. Exposure to bullying had been assessed at Wave 1 (age ≈ 14). Those reporting no to bullying at age 14 (N = 37) reported an SITA Mbully victim score = 1.936 (.097), whereas those who had said yes to bullying at age 14 reported an SITA Mbully victim score = 2.215 (.143), Hedges’s g = 2.39.
Discussion
The present study aimed to examine the feasibility, validity, and reliability of the SITA, using participants from an existing longitudinal cohort. The study is limited as a result of the small sample size; however, this is a feasibility study. We primarily aimed to assess the SITA in terms of ease of administration/completion, internal consistency of items, convergent validity of factors/domains, and an examination of the utility of adding subjective impact and timing of exposure components to the assessment of the relationship between lifetime psychiatric disorder, and adversity. At a macro level, the study is also limited by the fact that some forms of adversity are experienced more chronically than acutely, for example, war or civil unrest, neighborhood disorganization, or indeed poverty-related adversity. To the extent that the SITA does not assess every possible adverse experience, results overall are limited. However, this is a limitation of many ACEs assessment tools. Results must also be interpreted in light of the fact that all interviews were conducted remotely by the same interviewer, during a Covid-19 lockdown. These interviews were not digitally recorded, so the lack of interrater reliability is a limitation of the study.
The SITA assesses not only adversity exposure, but additionally the subjective impact and timing of the exposure. In this sense, it is a welcome addition to the ACEs’ assessment portfolio. Additional to the importance of psychometric robustness, SmithBattle et al. (2022) pointed to the importance of tools being easy-to-administer and interpret, whereas Bethell et al. (2017) demonstrated that few existing tools include any aspect of timing or impact of adversity. We believe that these are important considerations as it has been recently demonstrated that although, at a population level, the number of ACEs reported was negatively related to mental and physical health, this relationship did not hold at the level of the individual (Baldwin et al., 2021). In other words, a count of adversity alone was not related to deleterious outcomes in individuals. Therefore, it is likely that the way in which the adversity is experienced and when exactly in childhood it is experienced are important considerations. Rutter (2016) highlighted the difference between objective stress (e.g., did it happen, yes/no?) and subjective stress (e.g., how did it make me feel?). Indeed, some research has shown that subjective measures have better been able to predict health impact than objective ones. For example, regarding social standing, a number of studies (Cohen et al., 2008; Gianaros et al., 2007) showed the importance of the personal appraisal and processing of experiences, additional to their factual occurrence. There is also evidence of the relationship between maternal stress subjectively experienced in pregnancy and deleterious psychiatric outcomes in offspring (Brannigan et al., 2019, 2020).
At a macro level, the evidence presented here suggests that the SITA is a viable measure. First, at an item level, internal consistency estimates at both the online questionnaire and interview stages were largely acceptable (α > .70), with the exception of the PL domain. This indicates that items together are appropriately and consistently assessing their particular hypothesized domain (for example, sexual abuse). The correlation coefficients between SITA scores obtained using the online platform and the telephone interview (at +3 weeks) show variation in scores. This is an important consideration for future assessment of the properties and feasibility of this measure. Individuals engaged in a process of negotiation at the interviews, querying the appropriateness of responses to items and clarifying what was intended by “bullying” or “loss” in particular. As this was a feasibility study in a small cohort, we would be reluctant to suggest that the present results are a sound basis for the reduction of numbers of SITA items. Although SmithBattle et al. (2022) stress the importance of ease-of-completion of ACEs tools, a larger sample(s) will be required to justify the dropping of items. For example, a visual inspection of the Supplemental Materials suggests that (for example) parental incarceration and the lack of provision of regular meals were not particularly relevant in this sample. However, these might be important variables of consequence in other samples, and eliminating them for convenience alone based on this study, would not be methodologically sound.
In addition to this methodological issue, is the fact that differences in administration format across the 3-week follow-up (online vs. interview) mean that it is not possible to establish test–retest reliability in the widely understood sense of that term. The fact that the assessment format was different at both times will have affected the results (see Supplemental Section B). For example, there were a number of participants who modified their responses to “bullying” in the negotiated context of a telephone interview, providing a follow-up interpretation of the putative adverse event(s) as being on a normal spectrum. Relatedly, it is possible that different modes of administration of the questionnaire could ultimately yield different results. Although Supplemental Tables show overlap in “significant” findings across online and interview methodologies, there are also some cases where results were “significant” at online, but not at interview. However, method-specific results are not unique to this study, or to adversity research. For example, studies have shown relatively poor concordance in prospectively reported and retrospectively reported traumatic experience (e.g., Baldwin et al., 2019). It will be for future and better powered studies to determine the impact of SITA delivery mode or context on outcomes.
Convergent validity results point to the SITA domains functioning similarly to the widely used CTQ. Furthermore, results comparing SCID-5-RV lifetime diagnoses with mean adversity scores (Table 1 and Supplemental Table S3) suggest that in many cases the SITA scores were more strongly related to lifetime diagnosis than the CTQ. Results using the AATI-TA point to convergent validity insofar as they clearly demonstrated a substantively higher past negative, and lower past positive score was related to SITA domain score. In other words, attitudes to the past were more strongly related to experience of adversity, something that seems very plausible.
Results comparing SCID-5-RV lifetime diagnoses and both SITA mean scores and CTQ mean scores were also instructive and suggested a pattern of higher adversity scores in cases where lifetime diagnosis was positive. Results also suggest that the SITA scores were more consistently related to lifetime disorder outcomes than scores on the CTQ. With regard to the timing of adversity experience, there is already a literature showing the negative impact of trauma or adversity on the developing brain, which potentially leaves it susceptible to the effects of stress later in life, including the development of psychiatric disorders (Ho, 2019; McLaughlin et al., 2017). The hypothesis that there are “critical windows” or “sensitive periods” of neurodevelopment in early life during which exposure to adversity has a bigger impact than exposure later on in life is supported by the neuroscience literature (Gee & Casey, 2015; Ho, 2019).
To facilitate early intervention in mental disorders, we need to understand more about their complex etiology. A large part of this challenge is understanding how genetic and environmental risk influences each other. To effectively study environmental risk factors, we need better measurement of them than we currently have. The measurement of adverse experiences is an important part of understanding the environmental contributors to the etiology of mental disorders and potential targets for early intervention. Increasingly, trauma-focused interventions are being offered in circumstances where individuals have experienced adversities earlier in life (Bryant et al., 2021; Schuler & Boals, 2016). This is in keeping with emerging approaches in mental health policy, which specifies trauma-informed care as a key service delivery principle (Government of Ireland, 2020). The SITA has relevant research potential but also has a potential clinical utility, following further validity and reliability studies. These further studies can help reduce the number of items to produce a more easy-to-administer/interpret tool, and importantly in studies with much larger sample sizes, consideration can be given to the latent structure of this adversity screening tool to facilitate its use in examining risk for future psychiatric disorder.
Supplemental Material
sj-docx-1-asm-10.1177_10731911221116573 – Supplemental material for The Subjective Impact and Timing of Adversity Scale: A Feasibility Study Using Cross-Sectional and Longitudinal Data
Supplemental material, sj-docx-1-asm-10.1177_10731911221116573 for The Subjective Impact and Timing of Adversity Scale: A Feasibility Study Using Cross-Sectional and Longitudinal Data by Michel McKay, Colm Healy, Derek Chambers, Philip Dodd, Laurie O’Donnell, Mary Cannon and Mary C. Clarke in Assessment
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by the Irish Research Council, Grant number: COALESCE/2019/61.
Ethical Approval
The study was approved by the ethics committee at the RCSI, and has therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.