
Abstract
Posttraumatic stress disorder (PTSD) changed substantially when Diagnostic and Statistical Manual of Mental Disorders transitioned from fourth (DSM-IV) to fifth (DSM-5) edition. Hoge et al. found that although diagnostic prevalence remained consistent across nomenclatures, diagnostic concordance was low (55%). Study goals were to examine both the generalizability of these findings and whether either diagnosis systematically excluded patients. U.S. veterans (N = 1,171) who completed the PTSD Checklist for DSM-IV (PCL-S) and DSM-5 (PCL-5) were classified as: probable PTSD on both measures; probable PTSD on PCL-S only; probable PTSD on PCL-5 only; or no PTSD on either measure. Diagnostic prevalence was equivalent. Unlike Hoge et al.’s findings, diagnostic concordance was high (91.3%). Furthermore, observed demographic and severity differences were driven by disparities between veterans in the no PTSD versus the probable PTSD groups, not diagnostic changes. Findings suggest translatability across measures and that diagnostic changes do not systematically exclude patients.
In 2013, the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association [APA], 2013) was introduced. Whereas most diagnoses remained unchanged from the fourth text-revised edition Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR; APA, 2000), posttraumatic stress disorder (PTSD) was a notable exception. Although both diagnostic nomenclatures conceptualize PTSD as a serious mental illness predicated by trauma exposure and associated with high levels of impairment and comorbidity, the two versions of PTSD differ importantly due to the substantial changes made to the operationalization of the diagnosis in DSM-5. These changes include the recategorization of PTSD from an anxiety disorder into the newly developed category of trauma- and stressor-related disorders; revisions to the stressor criterion (Criterion A); the division of the DSM-IV avoidance and numbing cluster into two separate criteria; and the addition of three new symptoms, resulting in a total symptom count of 20 (Friedman, 2013).
The distinctions between the two diagnostic criteria sets have potentially important implications for individuals with PTSD, as well as for researchers and clinicians who work with trauma-exposed individuals. Specifically, changing how PTSD is defined directly affects who is diagnosed, which can have implications on the choice and course of treatment. Furthermore, if many of those who were diagnosed with PTSD under the DSM-IV criteria are not diagnosed with PTSD under the DSM-5 criteria, work done using the DSM-IV criteria may not be translatable to a large percentage of individuals with DSM-5 PTSD (Hoge et al., 2016).
Although other studies have compared DSM-IV PTSD with DSM-5 PTSD using measures validated for DSM-IV PTSD and then modified to reflect DSM-5 PTSD criteria (e.g., Kaysen et al., 2021; Schnyder et al., 2015), only one study has directly compared the two versions of the DSM PTSD diagnosis with measures validated for each. Specifically, Hoge et al. (2014) compared probable diagnostic status using two versions of the PTSD checklist (PCL)—the DSM-IV specific stressor version (PCL-S; Weathers et al., 1994) and the DSM-5 version (PCL-5; Weathers et al., 2013)—in a sample of U.S. infantry soldiers; each participant completed both measures. Although PTSD prevalence estimates remained nearly identical (12% for DSM-IV vs. 13% for DSM-5), 45% of participants had discordant results across the DSM-IV and DSM-5 PTSD criteria.
Hoge et al.’s (2014) findings raise potential concerns about the translatability of DSM-IV research to DSM-5 PTSD patients. For example, changes to the diagnostic criteria might affect who is referred to care, despite similar levels of distress and potentially similar response to treatment. This would be particularly problematic if either version of the diagnosis systematically excluded certain trauma survivors. For these reasons, replication of the Hoge et al. findings is important.
To determine the generalizability of Hoge et al.’s (2014) findings, additional work with different trauma-exposed samples is needed. It is particularly important to understand the impact of the diagnostic shift on U.S. veterans, for whom PTSD is one of the most prevalent mental disorders (Wisco et al., 2014). Furthermore, work is needed to explore whether individuals are systematically being excluded from either diagnosis, to ensure that marginalized groups and those with high levels of comorbidity are being captured by both nomenclatures. Without this exploration, these individuals—who are already vulnerable to poor health outcomes (e.g., Baah et al., 2019; Terhaag et al., 2022)—might inadvertently be limited in their access to appropriate care. Although Hoge et al. determined that the two PCL versions were similarly associated with psychological comorbidities, they did not explore how individuals who only met criteria for one version of the diagnosis compared with those who met for the other, both, or neither version of the diagnosis across demographics or comorbidities.
In this study, we extended Hoge et al.’s (2014) work on the diagnostic discordance across the DSM-IV and DSM-5 PTSD definitions using a large sample of U.S. Operation Enduring Freedom and Operation Iraqi Freedom (OEF/OIF) veterans. We had two goals: (a) to examine whether, consistent with Hoge et al.’s findings, past month prevalence estimates remained consistent across diagnostic definitions despite high levels of diagnostic discordance and (b) to determine whether either diagnosis systematically excluded veterans as a function of demographic characteristics (i.e., education level, age, ethnicity, sex, race, and sexual orientation), comorbid psychopathology (i.e., major depressive disorder [MDD], generalized anxiety disorder [GAD], somatoform disorder, panic disorder, and alcohol use disorder), or functional impairment. Consistent with Hoge et al.’s findings, we expected prevalence estimates to remain consistent, with nearly half of the sample demonstrating discordance across diagnostic criteria. Lacking empirical findings to guide our hypotheses regarding systematic exclusion associated with the two diagnostic criteria sets, we posed no a priori hypotheses for this latter set of analyses.
Method
Participants
Participants were veterans enrolled in the Veterans After-discharge Longitudinal Registry (Project VALOR), a longitudinal national registry of Iraq and Afghanistan Army and Marine Corps veterans (Rosen et al., 2012). To be included in Project VALOR, participants must have either (a) separated from active duty after serving in OEF/OIF or (b) completed at least one Reserve/Guard deployment in support of OEF/OIF; undergone a mental health evaluation at a VA facility, as indicated by a diagnostic interview or psychotherapy procedure code, between July 2008 and December 2009; and must not currently be participating in a clinical (intervention) trial. Veterans with probable PTSD according to the electronic medical record (i.e., at least two instances of a PTSD diagnosis by a mental health professional associated with two separate visits) were oversampled at a 3:1 (probable PTSD:no PTSD) ratio, and females were oversampled at a 1:1 (female:male) ratio.
Study staff contacted 4,391 potential participants, and 2,712 consented to participate in Project VALOR. Of those participants, 1,649 completed the first assessment (Time 1; T1) and were included in Project VALOR. Participants completed the second (T2), third (T3), and fourth (T4) assessments a mean of 2.47 years (SD = 0.52), 3.47 years (SD = 0.54), and 4.64 years (SD = 0.50) following the initial assessment (T1). To ensure a head-to-head comparison between the two versions of the diagnosis, only participants who completed the measures of interest at T4 were included in analyses (including both versions of the PCL; n = 1,171). All participants were between 27 and 73 years old (M = 43.30; SD = 9.86) and approximately half were women (n = 599, 51.2%). The sample predominantly identified as White (n = 882, 75.3%); of the remaining participants, 196 identified as Black/African American (16.7%), 16 identified as American Indian/Alaska Native (1.4%), eight identified as Asian (0.7%), four identified as Native Hawaiian/Pacific Islander (0.3%), 48 identified as multiracial (4.1%), and 17 (1.5%) did not report their racial identity. One hundred and thirty-one participants identified as Hispanic (11.2%). Most participants reported either being married or living with a partner (n = 734, 62.7%), and more than half of the sample reported completing higher education (at least a Bachelor’s degree; n = 595, 50.8%).
Measures
PTSD Checklist-Specific
The PTSD Checklist-Specific (PCL-S) is a 17-item self-report measure used to assess DSM-IV PTSD symptoms (Weathers et al., 1994). Participants rate the degree to which each symptom bothered them over the past month on a 5-point Likert-type scale (1 = not at all to 5 = extremely). Total scores are computed by summing the 17 items (range, 17–85), with higher scores indicating higher PTSD symptom severity. The PCL-S has demonstrated strong psychometric properties across a range of samples (Gore et al., 2013). In this study, Cronbach’s α was .96. Participants received the following instructions prior to completing the instrument:
Below is a list of problems and complaints that people sometimes have in response to stressful life experiences. Please read each one carefully, then circle one of the numbers to the right to indicate how much you have been bothered by that problem in the past month.
PTSD Checklist for DSM-5
The PTSD Checklist for DSM-5 (PCL-5) is a 20-item self-report measure that assesses DSM-5 PTSD symptoms (Weathers et al., 2013). Participants rate the degree to which each symptom bothered them over the past month on a 5-point Likert-type scale (0 = not at all to 4 = extremely). Total severity scores are computed by summing the 20 items (range, 0–80), with higher scores indicating higher PTSD symptom severity. The PCL-5 exhibits strong psychometric properties across active-duty military and veterans (Bovin et al., 2016; Wortmann et al., 2016). Prior to completing the PCL-5, participants received identical instructions to those provided for the PCL-S; Cronbach’s α was .96.
Patient Health Questionnaire
The Patient Health Questionnaire (PHQ) is a 58-item self-report version of the Primary Care Evaluation of Mental Disorders (PRIME-MD) used to assess eight somatic diagnoses (Spitzer et al., 1999). PHQ scores possess good psychometric properties (Spitzer et al., 1999). In the present study, we examined current PHQ symptom severity scores for the four diagnostic scales administered by the parent study: MDD, panic disorder, GAD, and somatoform disorder. We calculated symptom severity scores by summing the items for each scale, with higher scores indicating higher symptom severity for each disorder. Cronbach’s α was .91, .72, .87, and .82, respectively.
Alcohol Use Disorders Identification Test
The Alcohol Use Disorders Identification Test (AUDIT) is a 10-item screening instrument used to identify current alcohol consumption patterns that are hazardous and harmful; it gathers information on amount and frequency of intake, dependence, and issues associated with consumption (Saunders et al., 1993). Total scores are calculated by summing the 10 items (range, 0–40). The AUDIT has demonstrated strong psychometric properties in a sample of combat veterans (Berke et al., 2019). In the present study, Cronbach’s α was .87.
Inventory of Psychosocial Functioning
The Inventory of Psychosocial Functioning (IPF) is an 80-item self-report measure of past month psychosocial functioning that allows for the assessment of overall functioning and functioning across seven domains (romantic, family, parenting, friendship, work, education, and self-care; Marx et al., 2019). Each item is scored on a 7-point Likert-type scale (0 = never to 6 = always). The overall impairment score is calculated by summing the domain impairment scores, dividing by the number of domains to which the participant responded, and multiplying by 100 (range, 0–100), with higher scores suggesting a higher level of impairment. The IPF has demonstrated strong psychometric properties among veterans (Bovin et al., 2018). In this study, participants completed an average of 4.83 (SD = 1.21) domain scales, with Cronbach’s α ranging from .80 to .90 across scales.
Demographics Questionnaire
Participants completed a questionnaire in which they reported age, sex, race, ethnicity, sexual orientation, and highest level of education.
Procedure
Participants completed study measures of interest as part of a larger battery of questionnaires. All participants completed the T1 assessment for Project VALOR approximately 5 years prior to the T4 assessment. Except for sex (collected at T1 only), all the data used in the current study were from T4 (collected from September 2015 to January 2017) because it was the only study time point during which we administered both versions of the PCL. To help minimize re-administration effects, the two versions of the PCL were separated in the questionnaire battery by nine measures (i.e., more than 125 unrelated items). Participants were compensated US$150 for completing T4 of Project VALOR. All study procedures were approved by the local Institutional Review Board and the Human Research Protection Office of the U.S. Army Medical Research and Material Command.
Data Analytic Plan
We conducted all analyses using SPSS version 25. We first dichotomized five of the six demographic variables; age was left as a continuous variable. Sex was dichotomized into female (n = 599) and male (n = 572); race was dichotomized into White (n = 882) and Black (n = 196; individual groups of other races included fewer than 16 participants each, which precluded additional comparisons); sexual orientation was dichotomized into heterosexual (n = 1,090) and sexual minority (n = 78; individual groups included fewer than 45 participants which precluded comparisons; three participants had missing data); ethnicity was dichotomized into Hispanic (n = 131) and non-Hispanic (n = 1,031; nine participants had missing data); and education was dichotomized into no advanced degree (n = 569) and advanced degree (Bachelor’s degree or higher; n = 595; seven participants had missing data).
Next, using an appropriate cutoff score, we dichotomized the PCL-S and the PCL-5 into two groups: probable PTSD and no PTSD. As discussed above, both the PCL-S and PCL-5 assessed symptomatology in the past month; therefore, our groups reflected current probable PTSD status. As the best cutoff score for any given sample is a product of both diagnostic prevalence and the purpose of the measure, we would have ideally conducted diagnostic utility analyses to determine the best cutoff score for this sample. However, in the absence of clinical interviews to validate a cutoff score on each of the two versions of the PCL, we relied on pre-established cutoff scores. There are many cutoff scores proposed to estimate probable PTSD with the PCL-S, ranging from 30 to 60 (see McDonald & Calhoun, 2010, for a review). For this study, we chose to use a cutoff score of 50 on the PCL-S because, in addition demonstrating good diagnostic accuracy across myriad studies (e.g., Andrykowski et al., 1998; Weathers et al., 1993; κs = .65), a cutoff score of 50 is conventionally recommended to be used among veterans (e.g., McDonald & Calhoun, 2010), thereby increasing the applicability of our findings. For the PCL-5, we used a cutoff score of 33. This cutoff score was validated among veterans, demonstrating adequate diagnostic accuracy (κ = .58; Bovin et al., 2016), and is recommended for use in veterans by the Veterans Health Administration (e.g., Franklin et al., 2018). For participants with missing data on either measure (n = 210), analyses were conducted to determine whether the missing data would influence categorization based on the pre-established cutoff scores. If missingness did not influence categorization (i.e., participants had severity scores above the required cutoff score for probable diagnosis even with missing data or participants would not be above the required cutoff score even if they had the highest possible scores on the items missing), they were included in analyses (n = 138). The remaining participants were excluded from analyses, leaving a final sample of 1,171 veterans.
Participants were then classified into one of four groups based on the concordance of their probable PTSD diagnosis across the two measures: (a) no PTSD diagnosis on either measure; (b) probable PTSD diagnosis according to the PCL-5 but not the PCL-S; (c) probable PTSD diagnosis according to the PCL-S but not the PCL-5; and (d) probable PTSD diagnosis on both measures. We collapsed these groups into a single variable with four levels. After examining descriptive statistics for each group, we tested differences between groups. We used chi-square analyses and one-way analyses of variance (ANOVAs) to identify potential differences between the four groups across demographic characteristics (i.e., sex, race, sexual orientation, ethnicity, education level, and age), measures of current psychopathology (i.e., MDD, panic, GAD, somatoform, and alcohol use severity), and psychosocial functioning. We calculated standardized residuals (std res) to determine chi-square simple effects, with those ≥|1.96| interpreted as significant at the p < .05 level. We used least significant difference (LSD) tests to evaluate ANOVA simple effects, with significance evaluated at the p < .05 level. We used a Bonferroni correction for the omnibus test (i.e., chi-square test or F-test) to protect against type I error given the 12 analyses conducted.
Results
Group Categorization
Of the 1,171 total participants, 602 veterans (51.4%) screened positive for probable DSM-IV PTSD according to the PCL-S, and 638 veterans (54.5%) screened positive for probable DSM-5 PTSD according to the PCL-5. Concordance across the two measures was high (91.3%), with 500 veterans (42.7%) not meeting the criteria for probable PTSD on either the PCL-S or the PCL-5 (no PTSD group); 33 veterans (2.8%) meeting the criteria for probable PTSD on the PCL-S only (probable DSM-IV PTSD group); 69 veterans (5.9%) meeting the criteria for probable PTSD on the PCL-5 only (probable DSM-5 PTSD group); and 569 veterans (48.6%) meeting the criteria for probable PTSD on both measures (probable both PTSD group). 1
Demographic Comparisons
Results identified three significant demographic differences across probable PTSD groups that met the adjusted Bonferroni criterion for statistical significance (p < .004). Groups differed significantly on education level, with veterans in the no PTSD group being significantly more likely to have an advanced degree (std res = 2.3), and veterans in the probable both PTSD group being significantly more likely to not have an advanced degree (std res = 2.2). Groups also differed on ethnicity, with veterans in the no PTSD group being significantly less likely to identify as Hispanic (std res = −3.0) and veterans in the probable both PTSD group being significantly more likely to identify as Hispanic (std res = 2.7). In addition, groups differed significantly on age, with veterans in the no PTSD group being significantly younger than those in the probable DSM-IV PTSD group (p < .05) and those in the probable both PTSD group (p < .05). Furthermore, veterans in the probable DSM-IV PTSD only group were significantly older than veterans in the other three groups (all ps < .05). No significant group differences were found across sex, race, or sexual orientation (see Table 1).
Omnibus Comparisons of Demographic Variables Across Four PTSD Diagnostic Categories.
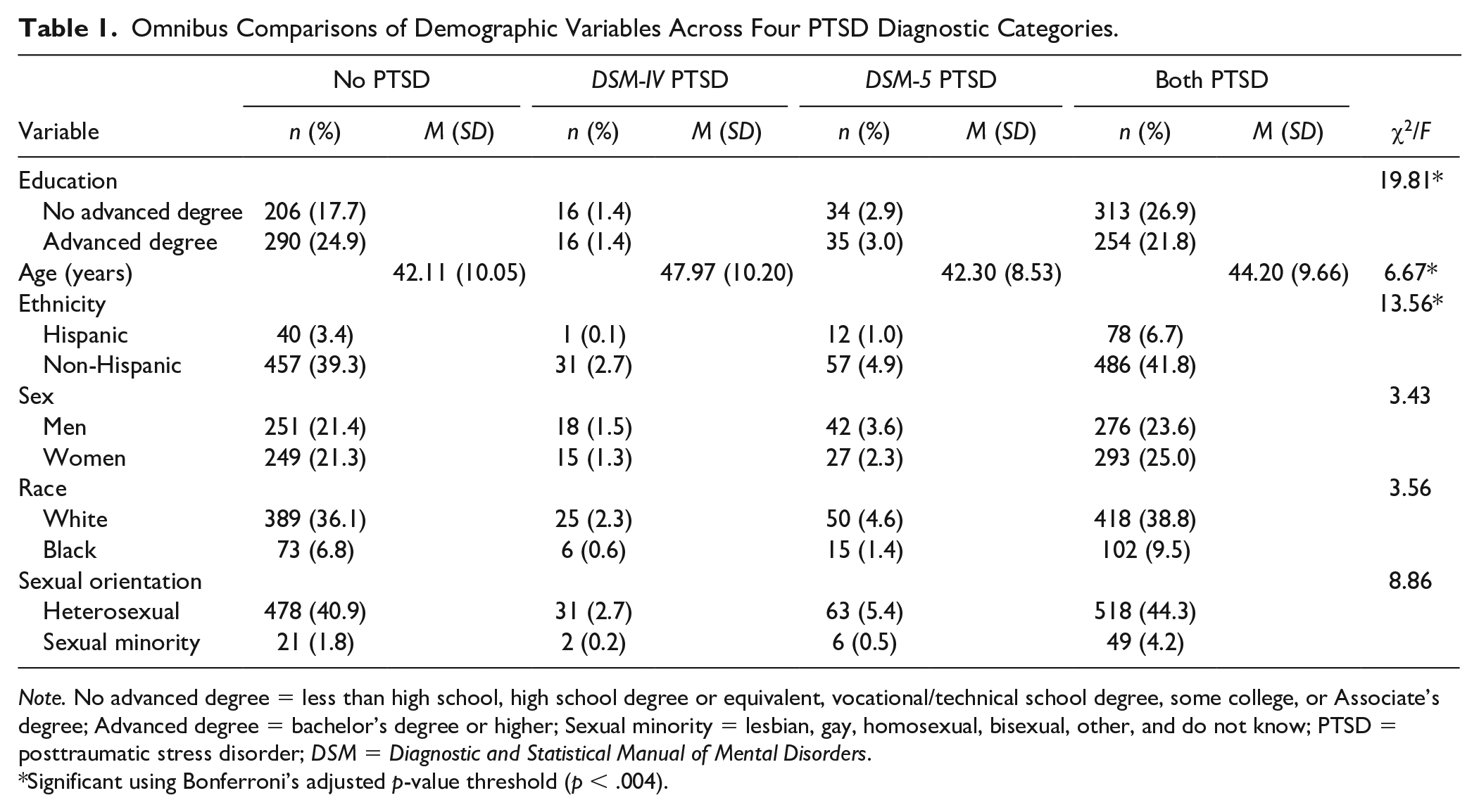
Note. No advanced degree = less than high school, high school degree or equivalent, vocational/technical school degree, some college, or Associate’s degree; Advanced degree = bachelor’s degree or higher; Sexual minority = lesbian, gay, homosexual, bisexual, other, and do not know; PTSD = posttraumatic stress disorder; DSM = Diagnostic and Statistical Manual of Mental Disorders.
Significant using Bonferroni’s adjusted p-value threshold (p < .004).
Psychopathology and Impairment Comparisons
For all ANOVAs examining psychopathology and impairment, the overall F-test met the adjusted Bonferroni criterion for statistical significance (all ps < .004). For MDD severity, GAD severity, panic disorder severity, somatoform disorder severity, and psychosocial functioning, post hoc tests indicated that veterans in the no PTSD group had significantly lower severity scores and lower functioning scores than veterans in the other three groups (all ps < .01). Furthermore, veterans in the probable both PTSD group had significantly greater MDD severity scores, GAD severity scores, panic disorder severity scores, somatoform disorder severity scores, and functioning scores than veterans in the other three groups (all ps < .01; see Table 2).
Omnibus Comparisons of Psychopathology Severity and Psychological Functioning Variables Across Four PTSD Diagnostic Categories.
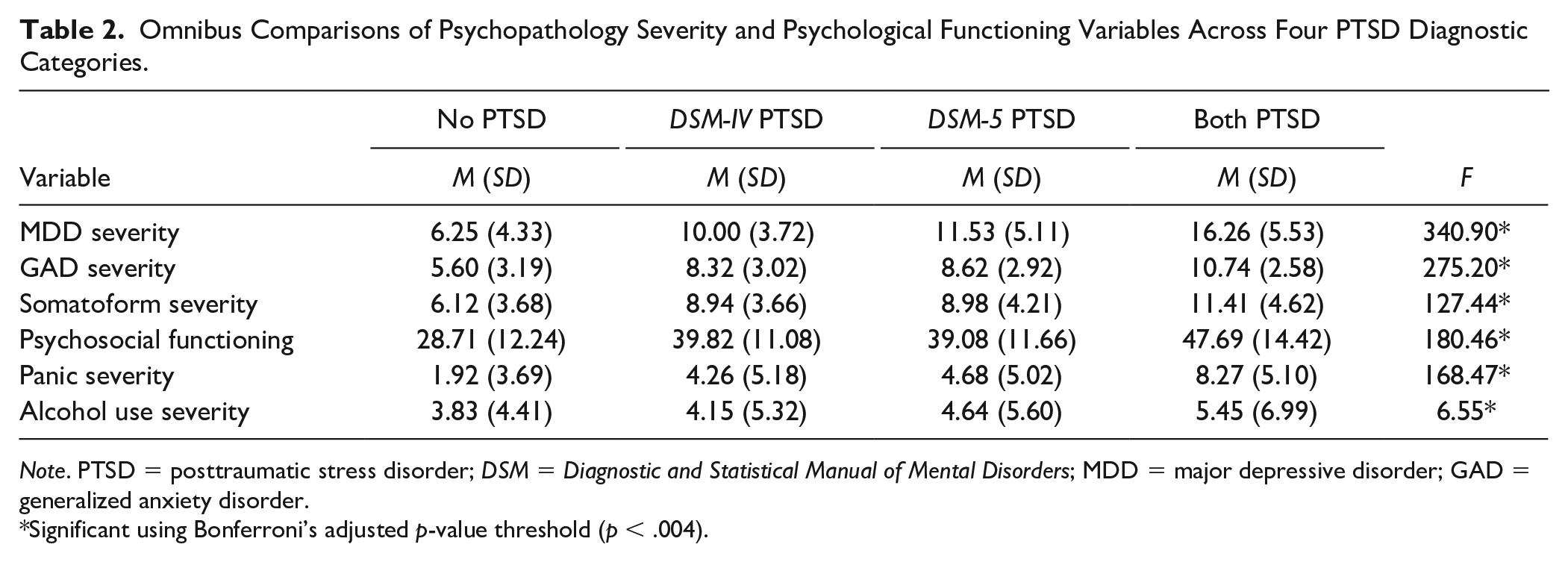
Note. PTSD = posttraumatic stress disorder; DSM = Diagnostic and Statistical Manual of Mental Disorders; MDD = major depressive disorder; GAD = generalized anxiety disorder.
Significant using Bonferroni’s adjusted p-value threshold (p < .004).
Alcohol use severity scores demonstrated a different pattern across groups. Veterans in the no PTSD group had significantly lower severity scores than veterans in the probable both PTSD group (p < .01). However, there were no other differences observed across groups (all ps > .05; see Table 2).
Discussion
Consistent with work conducted among active-duty military personnel (Hoge et al., 2014), our results indicated that probable PTSD prevalence as measured by self-report measures was not significantly affected by the shift from DSM-IV to DSM-5. However, unlike Hoge et al.’s findings, our results indicated that despite the differences associated with the two nomenclatures, the two diagnoses were highly concordant in classification across probable PTSD status at both the group and individual levels of analysis. Furthermore, in general, there were no systematic differences across diagnostic groups. Probable PTSD status was not affected by veteran sex, racial identity, or sexual orientation, and both diagnoses captured veterans with the highest levels of both symptom severity and functional impairment.
Taken together, our findings indicate that veterans who meet the criteria for probable PTSD according to one DSM taxonomy will also meet the criteria on the other. For the small number of cases in which diagnostic status is discordant, our findings suggest that this discordance cannot be explained by any systematic demographic or psychosocial differences. Furthermore, rather than one set of diagnostic criteria being associated with a more severe presentation than the other, our results suggest that veterans with the most severe presentations will be captured by both definitions of PTSD.
Our findings have important clinical implications. First, our results suggest that the field can have confidence that research operationalizing probable PTSD according to the DSM-IV definition will still be relevant for veterans with probable PTSD according to the DSM-5, as only a small number of veterans who meet the criteria for probable DSM-IV PTSD will not meet for probable DSM-5 PTSD (and vice versa), and the two groups of veterans are not systematically different from one another. Second, regardless of which diagnosis is employed, the veterans with the highest self-reported comorbid distress and functional impairment will be captured. This somewhat alleviates safety concerns that might otherwise emerged as a function of differing diagnoses on the respective measures; our findings suggest that the most symptomatic veterans—and likely those with the most imminent need for treatment—will be identified as having probable PTSD regardless of the version of the PCL used.
Despite these findings, our results should not be interpreted to imply that the DSM-IV and DSM-5 versions of PTSD are identical, nor that the two versions of the PCL are interchangeable. Each iteration of the DSM builds on empirical work which provides additional insight into the diagnosis, and the success of each iteration cannot be tested without measures that reflect each version of the diagnosis. Therefore, while the development and validation of new metrics is resource and time intensive, such efforts are crucial to moving the field forward.
Although the change in the PTSD diagnosis occurred nearly a decade ago, this work remains important for examination and dissemination even now. Following diagnostic changes, rigorous validation can take several years following the development of new instruments; in the case of the PCL, although the instrument was published in 2013 (Weathers et al., 2013), the first validation paper among veterans did not occur until several years later (Bovin et al., 2016), and new validation papers are continuing to be published to examine the utility of the instrument among different samples and settings (e.g., Carvalho et al., 2020; Van Praag et al., 2020). Thus, it is likely that while the most recent version of the PCL is widely utilized in some settings, other settings may be slower to adopt due to limited resources and psychometric information. Importantly, our findings suggest that among veterans, both versions of the PCL will capture the most symptomatic individuals with probable PTSD.
The current study addresses only one aspect of a larger consideration in the field—namely, the existence of multiple legitimate definitions for conferring a PTSD diagnosis. Even under the same diagnostic set, there is a lack of consensus in how the PTSD definition should be applied. Multiple scoring rules exist for even the most rigorous diagnostic interviews (e.g., Weathers et al., 1999), creating potential heterogeneity across populations, trauma types, and studies. Additional work is needed to explore the existence of systematic exclusion across these scoring rules to have confidence that the findings predicated on these rules are translatable. Future endeavors can use this study as a guide for investigating this important question.
Several strengths of this study should be noted. First, this research was conducted with a large sample of returning combat veterans, a demographic group that is at elevated risk for trauma exposure and PTSD (e.g., Sundin et al., 2010). Second, all participants completed both DSM-IV and DSM-5 versions of the PCL, allowing for direct comparisons across classification schemes. Third, by comparing four groups across multiple outcomes, our approach provided a robust examination of the implications of the two diagnoses on veterans with and without PTSD.
Like all studies, our project is not without limitations. First, our examination of U.S. veterans suggests that our findings may not generalize to all trauma-exposed populations; additional research is needed to explore this possibility. Relatedly, although our findings diverged from Hoge et al.’s (2014), it is unclear how much of this discrepancy was driven by the differences across the samples. Whereas Hoge et al. examined a sample of active-duty U.S. infantry soldiers that were mostly male (~10% women) and for whom PTSD diagnostic status was allowed to vary naturally (~16% of participants met the criteria for PTSD on at least one version of the PCL), we examined a sample of U.S. veterans that were oversampled for both women (~51% women) and for PTSD diagnostic status (~57% of participants met the criteria for probable PTSD on at least one version of the PCL). Due to the substantial sampling differences between the two studies, additional work is needed to understand how the varying sampling approaches may have influenced the findings. Second, this study (like Hoge et al.’s) used self-report measures of PTSD rather than clinical interviews. Although both measures have been validated against structured clinical interviews, additional work is needed to determine whether our findings are replicable when interview measures are used, as these will not only provide more definitive information about diagnostic status but also allow for response bias indicators to be considered. This was not possible in the current study, as we only administered a clinical interview that reflected DSM-5 criteria. Third, we used pre-established cutoff scores to operationalize probable PTSD, which may not have ideally fit the data. However, our use of conventionally accepted cutoff scores for both measures increases the chances that these findings will replicate in practice. Fourth, we standardized the order of administration in this study and accordingly may have introduced order effects by not counterbalancing.
Results of the current study provide evidence of high levels of PTSD diagnostic concordance across DSM definitions. This suggests that most veterans who meet the criteria for probable PTSD on the PCL-S will also meet the criteria on the PCL-5, and vice versa. Furthermore, the diagnoses demonstrate no systematic differences in classification, and both diagnoses capture veterans with the highest levels of functional impairment and comorbid symptom severity. Our findings suggest that the large body of work conducted using DSM-IV PTSD criteria has direct implications for veterans who meet the criteria for PTSD according to DSM-5. Furthermore, the high level of overlap suggests that both diagnoses are capturing important aspects of latent construct of PTSD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the U.S. Department of Defense Awards W81XWH-08-2-0102 and W81XWH-08-2-0100. Colin T. Mahoney was supported by National Institute of Mental Health Award 5T32MH019836-16 to Terence M. Keane, PhD.