
Abstract
Establishing normative data for questionnaires is essential for the accurate interpretation of scores, given that these norms can vary according to different subpopulations and treatment contexts. The purpose of this study was to establish norms for the Eating Disorder Examination-Questionnaire (EDE-Q) among adults receiving higher levels of care (HLOCs) for the treatment of eating disorders. Participants were 2,283 people receiving treatment at the inpatient, residential, partial hospitalization, or intensive outpatient levels of care. The EDE-Q was completed at admission. Patients with anorexia nervosa—restricting subtype (AN-R) had the lowest EDE-Q Global scores when compared with all other eating disorder diagnoses. When compared with intensive outpatient care, only those in residential treatment had higher EDE-Q Global scores. This study is among the first to describe norms for the EDE-Q in a large sample of adults receiving various HLOCs. Programs utilizing the EDE-Q to assess treatment outcomes can use these findings to aid people in interpreting their scores.
This study established Eating Disorder Examination-Questionnaire (EDE-Q) norms for a large transdiagnostic sample of adults receiving treatment for an eating disorder at a higher level of care (HLOC). As norms can vary depending on the subpopulation examined, this study will enable HLOC treatment programs utilizing the EDE-Q to interpret and contextualize people’s scores.
Higher levels of care (HLOCs) for eating disorders (EDs), including inpatient (IP) medical hospitals, residential (RES), partial hospitalization, and intensive outpatient programs (IOP), augment treatment options for those who are medically compromised due to their EDs, those who have been unsuccessful in outpatient treatment, or those in need of more intensive treatment than what is typically offered in outpatient practices. Although the number of RES programs has grown over the past 25 years (Guarda & Attia, 2018), most research on EDs has been at the IP mental health or outpatient levels of care. More information on the presentation and outcome of people with EDs in HLOCs, such as RES, will help to determine the effectiveness of these programs.
One of the most used measures for assessing ED pathology and determining treatment effectiveness is the Eating Disorder Examination-Questionnaire (EDE-Q) (Fairburn & Beglin, 1994, 2008), a self-report measure assessing both cognitive and behavioral features of EDs, based on the Eating Disorder Examination interview (Cooper & Fairburn, 1987). To accurately interpret the EDE-Q and to determine the presence of clinically significant change, establishing normative data is essential, as norms can vary depending on the subpopulation examined (Aardoom et al., 2012). Several studies have examined EDE-Q norms among adults. However, many of these studies have been conducted with nonclinical populations, such as community samples or university students (e.g., Carey et al., 2019; Hilbert et al., 2012; Mond et al., 2006; Reas et al., 2012). Clinical studies completed heretofore have included male IPs (Jennings & Phillips, 2017a; n = 38), combined IP and outpatient samples (Dahlgren et al., 2017; n = 667), combined RES and outpatient samples (Aardoom et al., 2012; n = 935), a clinical sample of females without a description of the levels of care included (Welch et al., 2011; n = 2,383), and outpatients (Brewin et al., 2014; n = 932). Only one study has examined EDE-Q norms among those receiving RES or partial hospitalization levels of care, and this study included only males (Smith et al., 2017; n = 373). Thus, there is a dearth of information on EDE-Q norms among clinical samples of adults across all levels of HLOC treatment.
The purpose of this study was to establish EDE-Q norms for a large transdiagnostic ED sample of adults receiving treatment at IP, RES, partial hospitalization program (PHP), or IOP levels of care. Norms will be examined separately by ED diagnosis and by HLOCs.
Method
Participants and Procedure
Participants were 2,283 adults with a diagnosis of an ED receiving treatment at Eating Recovery Center (ERC), a multisite treatment facility in the United States offering HLOCs for those with EDs. Participants had been admitted to treatment between October 2020 and October 2022. Diagnoses were made by licensed clinicians conducting semi-structured interviews based on the Diagnostic and Statistical Manual of Mental Disorders–Fifth Edition (DSM-5; American Psychiatric Association [APA], 2013), and included anorexia nervosa—restricting subtype (AN-R), anorexia nervosa—binge/purge subtype (AN-BP), bulimia nervosa (BN), binge eating disorder (BED), and other specified feeding or eating disorder (OSFED). All participants who provided informed consent and completed self-report measures at admission were eligible for the study. This study was approved by Salus Institutional Review Board.
Treatment
Treatment at the IP, RES, and PHP levels includes individual therapy twice a week, weekly family therapy, twice weekly medical provider visits (daily for IPs), weekly sessions with registered dietitians, and 3 to 4 hours of evidence-based skills groups per day. Groups include interventions based on exposure and response prevention, acceptance and commitment therapy, and dialectical behavior therapy. Patients eat three supervised meals and two to three supervised snacks per day. IPs see a psychiatrist daily, while RES and PHP patients see a psychiatrist twice weekly for medication and psychiatric comorbidity monitoring. Treatment at the IOP level includes one therapy session and one dietary session per week, a supervised meal each day, and 3 hours of group therapy per day, 3 to 5 days per week. Patients in IOP do not see a psychiatrist as part of their ERC treatment.
Level of care criteria are based on medical stability, weight, and intensity of ED behaviors, and decisions regarding the level of care are based on the American Psychiatric Association Practice Guideline for the Treatment of Patients With Eating Disorders, Third Edition (Yager et al., 2006), and Fourth Edition (Crone et al., 2023), and the DSM-5 (APA, 2013) severity index, which delineate appropriate criteria for various levels of care. Individuals with medical instability are typically admitted for medical IP treatment; those who are medically stable but at a very low body weight or have severe ED behaviors are generally admitted to RES treatment. PHP is recommended for those needing some weight restoration or moderate behavior containment, while IOP is typically recommended for those not requiring significant monitoring.
Measures
The EDE-Q (Fairburn & Beglin, 1994, 2008) is a widely used 28-item self-report measure of the cognitive and behavioral psychopathology of patients with EDs that was completed at admission and discharge. For purposes of this study, only admission scores are considered here. The measure has four subscales: Restraint, Eating Concern, Shape Concern, and Weight Concern. Items are scored from 0 to 6, with higher scores indicating more severe psychopathology, and averaged to obtain the subscale scores. No items are reverse scored. In addition, there is a Global Score obtained by averaging the scores of the four subscales. The EDE-Q has been found to have acceptable internal consistency, discriminant validity, and construct validity (Berg et al., 2012). For the current sample, all subscales and the Global Score demonstrated high internal consistency (Restraint α = .90, 95% confidence interval [CI] = [0.89, 0.90]; Eating Concerns α = .77, 95% CI = [0.76, 0.78]; Shape Concerns α = .93, 95% CI = [0.93, 0.94]; Weight Concerns α = .87, 95% CI = [0.86, 0.87]; Global Score α = .96, 95% CI = [0.96, 0.96]). Previous studies have used a cutoff of 4 to indicate clinical significance (e.g., Jennings & Phillips, 2017b).
Statistical Analyses
Means, standard deviations, and percentiles were computed for the EDE-Q Global score and each subscale across the entire sample, and within diagnosis and level of care. Chi-square tests of independence were used for all comparisons of dichotomous proportions. Generalized linear models with dummy coding were used for all comparisons, with a Gaussian distribution for continuous outcomes and a binomial distribution for dichotomous outcomes. AN-R is the reference group for comparisons across diagnoses, and IOP is the reference group for comparisons across levels of care. For the EDE-Q behavioral items, frequencies are presented but no inferential comparisons were performed to minimize the study-wise error rate and need for a multiple comparison correction.
Results
Table 1 presents characteristics for the overall sample. Most were diagnosed with OSFED (39.2%), identified as female (88.5%), and were White (78.0%). The EDE-Q Global score for the sample was 3.92 (SD = 1.46). The EDE-Q Global score was significantly higher in female (M = 3.97, SD = 1.44) than in male participants (M = 3.26, SD = 1.62; t = 5.16, p < .001).
Patient Characteristics by Level of Care.
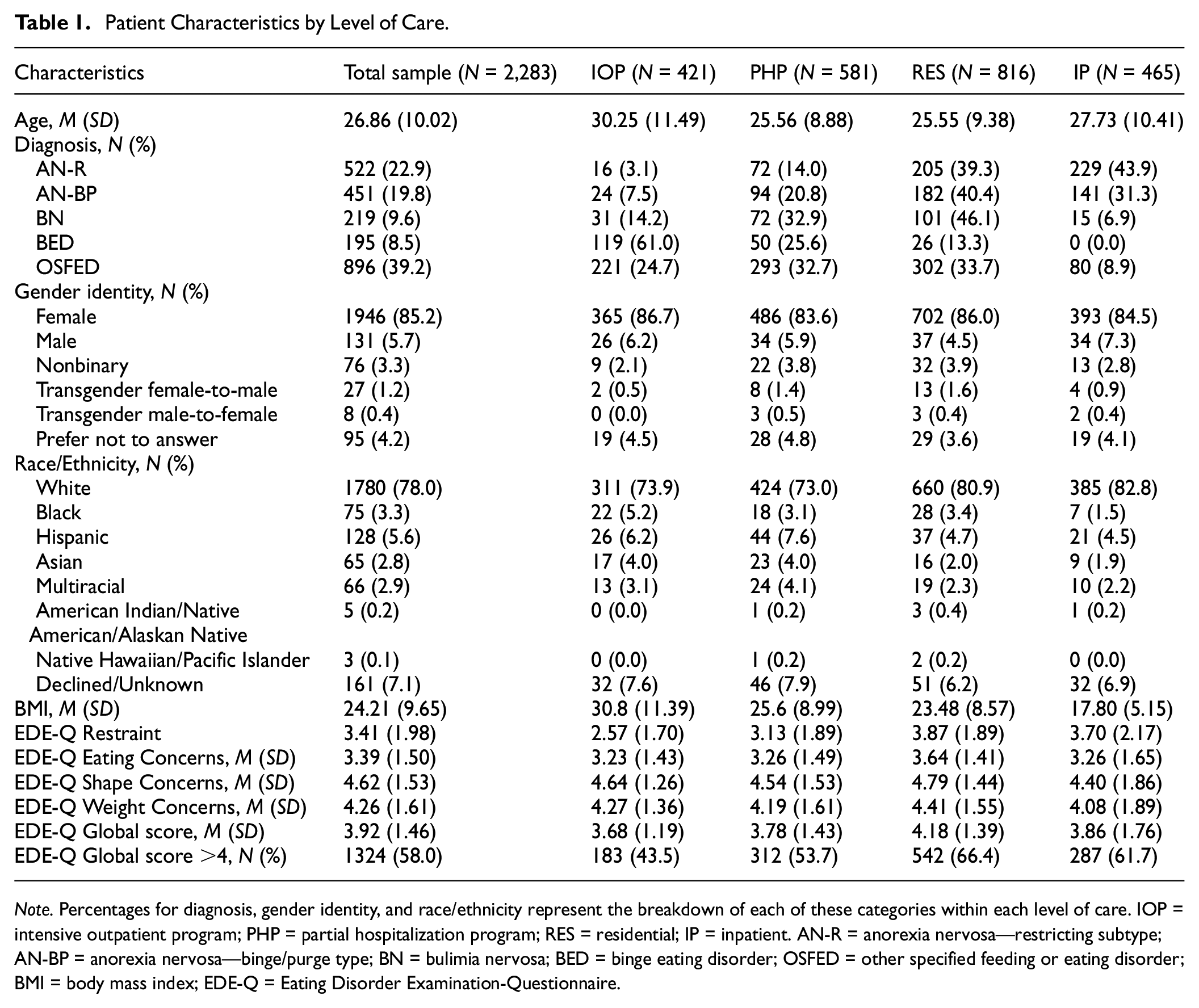
Note. Percentages for diagnosis, gender identity, and race/ethnicity represent the breakdown of each of these categories within each level of care. IOP = intensive outpatient program; PHP = partial hospitalization program; RES = residential; IP = inpatient. AN-R = anorexia nervosa—restricting subtype; AN-BP = anorexia nervosa—binge/purge type; BN = bulimia nervosa; BED = binge eating disorder; OSFED = other specified feeding or eating disorder; BMI = body mass index; EDE-Q = Eating Disorder Examination-Questionnaire.
Table 2 presents the percentile ranks for the EDE-Q Global and subscale scores. More than half of the participants scored >4 on the EDE-Q Global (N = 1,324, 58.0%). On the EDE-Q Shape subscale (N = 1,674, 73.3%) and the EDE-Q Weight subscale (N = 1,445, 63.3%), more than half of the participants scored >4. Less than half of the participants scored >4 on the EDE-Q Eating Concerns subscale (N = 846, 37.1%) and EDE-Q Restraint subscale (N = 1,032, 45.2%).
EDE-Q T Scores and Raw Percentile Scores.
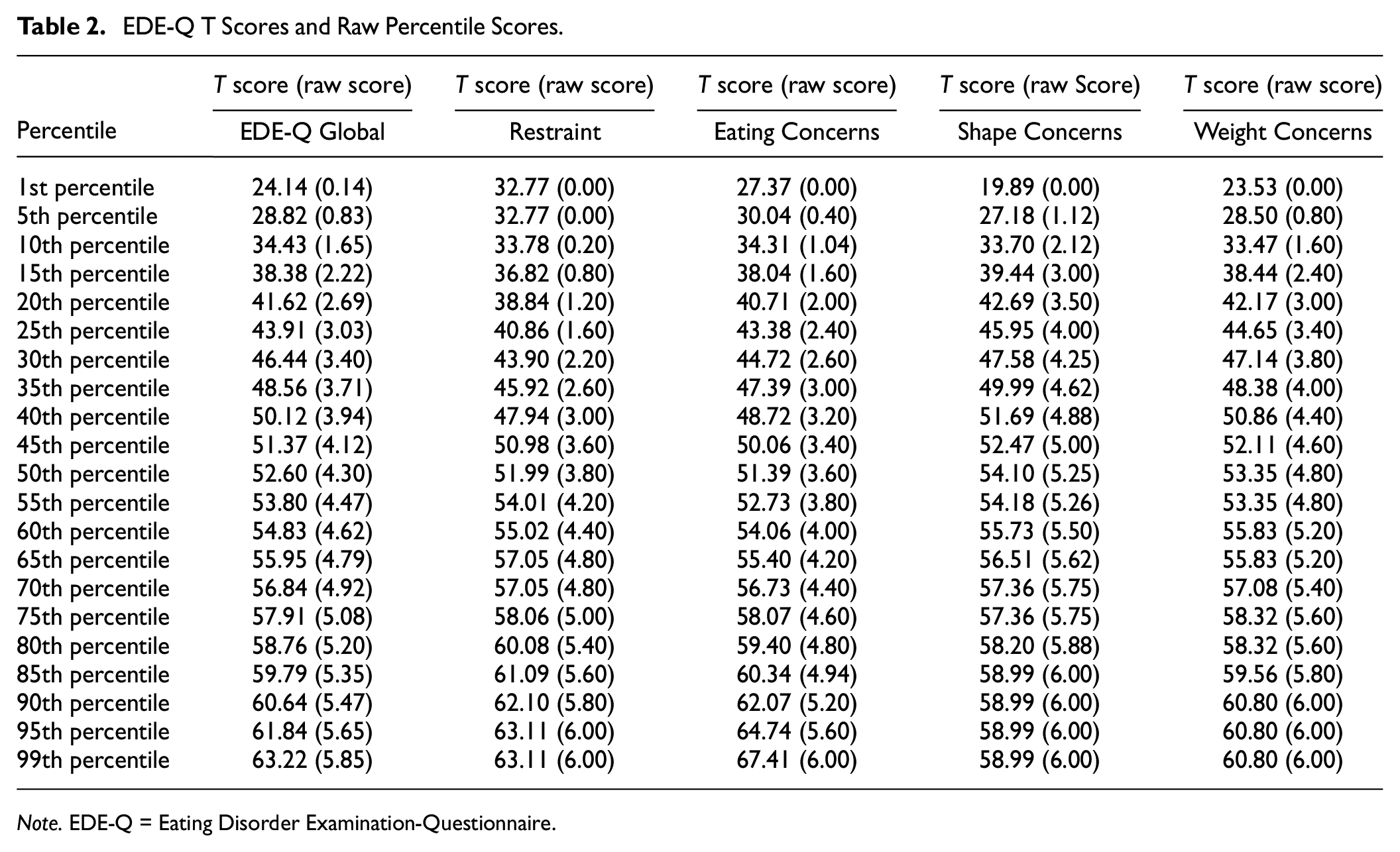
Note. EDE-Q = Eating Disorder Examination-Questionnaire.
There was a significant variation in the EDE-Q Global score by diagnosis, F(4,2278) = 22.63, p < .001. When compared with those with AN-R, significantly higher EDE-Q Global scores were found for those with AN-BP (b = 0.83, t = 8.95, p < .001, β = .56, 95% CI = [0.44, 0.69]), BN (b = 0.64, t = 5.52, p < .001, β = .21, 95% CI = [0.05, 0.37]), BED (b = 0.31, t = 2.55, p = .01, β = .44, 95% CI = [0.28, 0.59]), and OSFED (b = 0.53, t = 6.68, p < .001, β = .36, 95% CI = [0.26, 0.47]) (see Table 3).
EDE-Q Scores and BMI by Diagnosis.
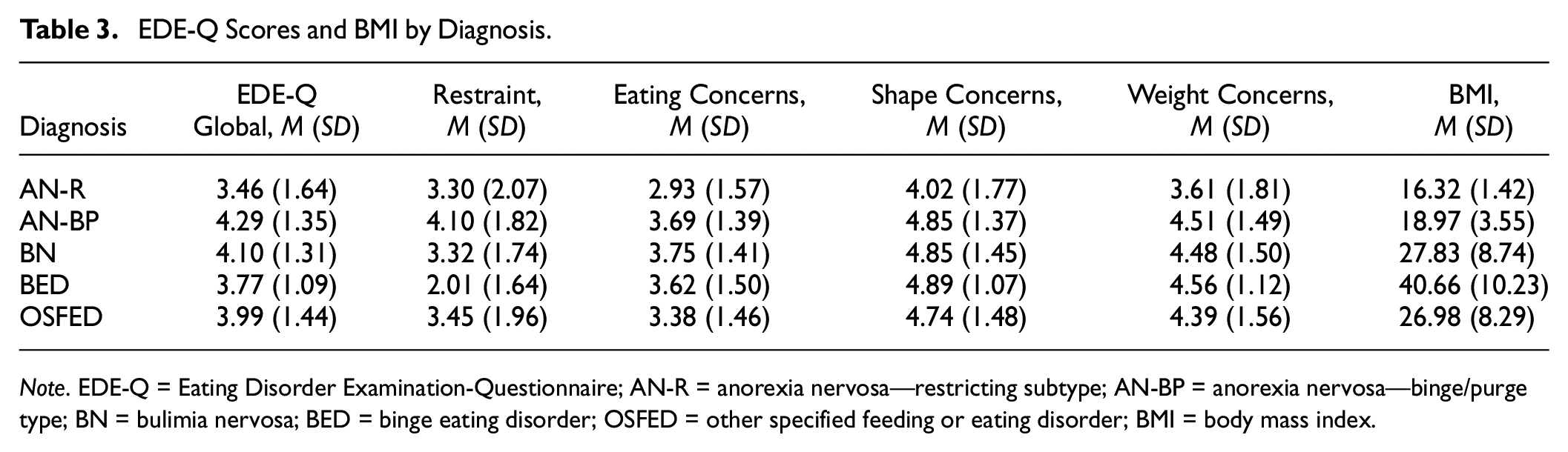
Note. EDE-Q = Eating Disorder Examination-Questionnaire; AN-R = anorexia nervosa—restricting subtype; AN-BP = anorexia nervosa—binge/purge type; BN = bulimia nervosa; BED = binge eating disorder; OSFED = other specified feeding or eating disorder; BMI = body mass index.
There was a significant variation in the EDE-Q Global score by HLOCs, F(3,2279) = 14.45, p < .001. When compared with IOP, only RES had a significantly higher EDE-Q Global score (b = 0.50, t = 5.74, p < .001). Table 4 presents EDE-Q Global percentile scores by HLOCs. The proportion of people with an EDE-Q Global score >4 also differed significantly by LOCs (χ2 = 67.30, p < .001). When compared with IOP, PHP (b = 0.41, t = 3.19, p < .01, odds ratio [OR] = 1.51, 95% CI = [1.17, 1.94]), RES (b = 0.94, t = 7.67, p < .001, OR = 2.57, 95% CI = [2.02, 3.28]), and IP (b = 0.74, t = 5.41, p < .001, OR = 2.10, 95% CI = [1.60, 2.75]) all had significantly higher odds of EDE-Q Global score >4 (see Table 1).
EDE-Q Global T Scores and Raw Percentile Scores by HLOCs.
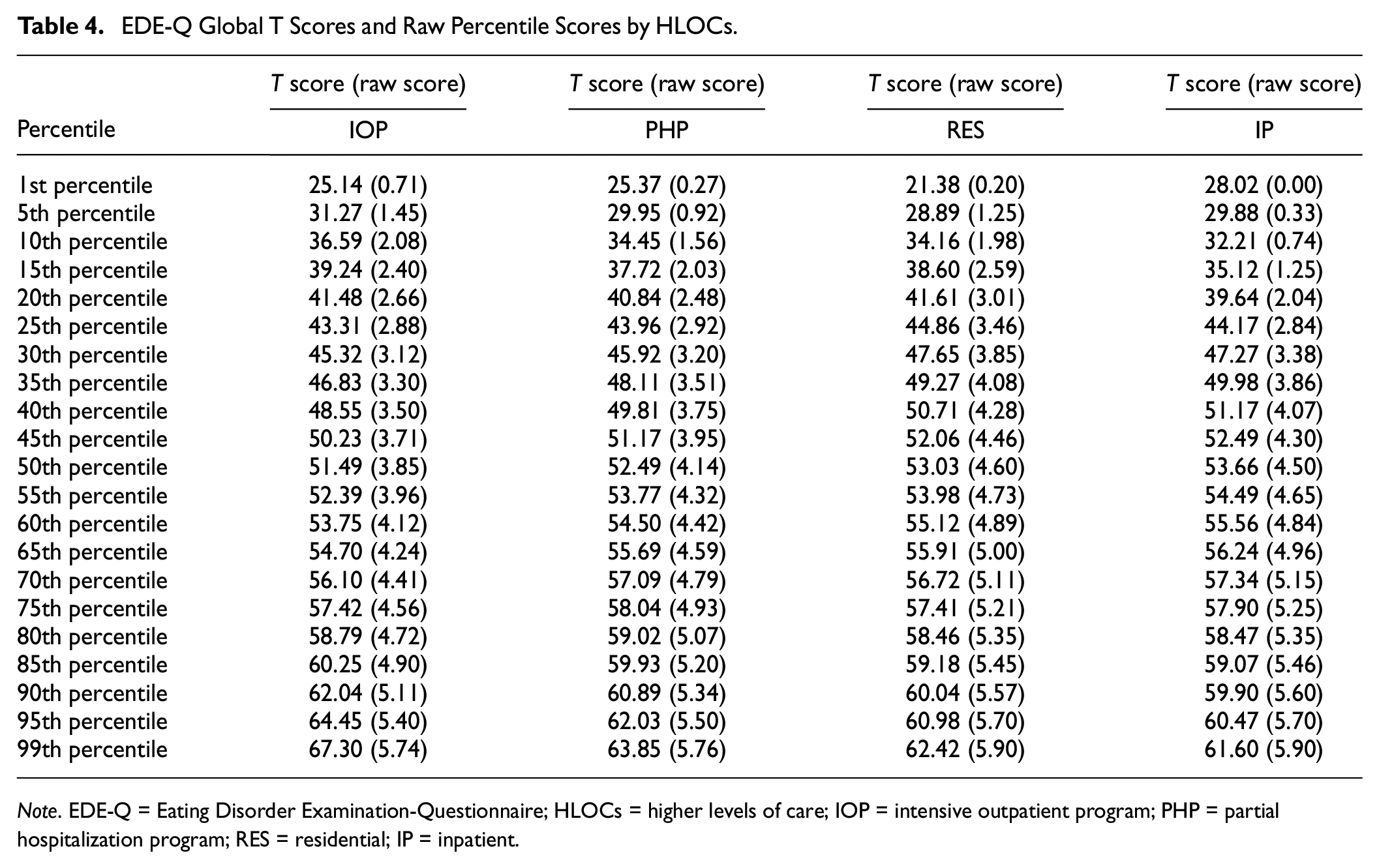
Note. EDE-Q = Eating Disorder Examination-Questionnaire; HLOCs = higher levels of care; IOP = intensive outpatient program; PHP = partial hospitalization program; RES = residential; IP = inpatient.
Table 5 presents the frequency of the EDE-Q behavioral items (objective binge episodes, self-induced vomiting, laxative misuse, and driven exercise) by diagnosis and HLOCs. Table 6 presents EDE-Q subscale T scores and raw percentile scores by HLOC.
Frequency of EDE-Q Behavioral Items by Diagnosis and HLOCs.
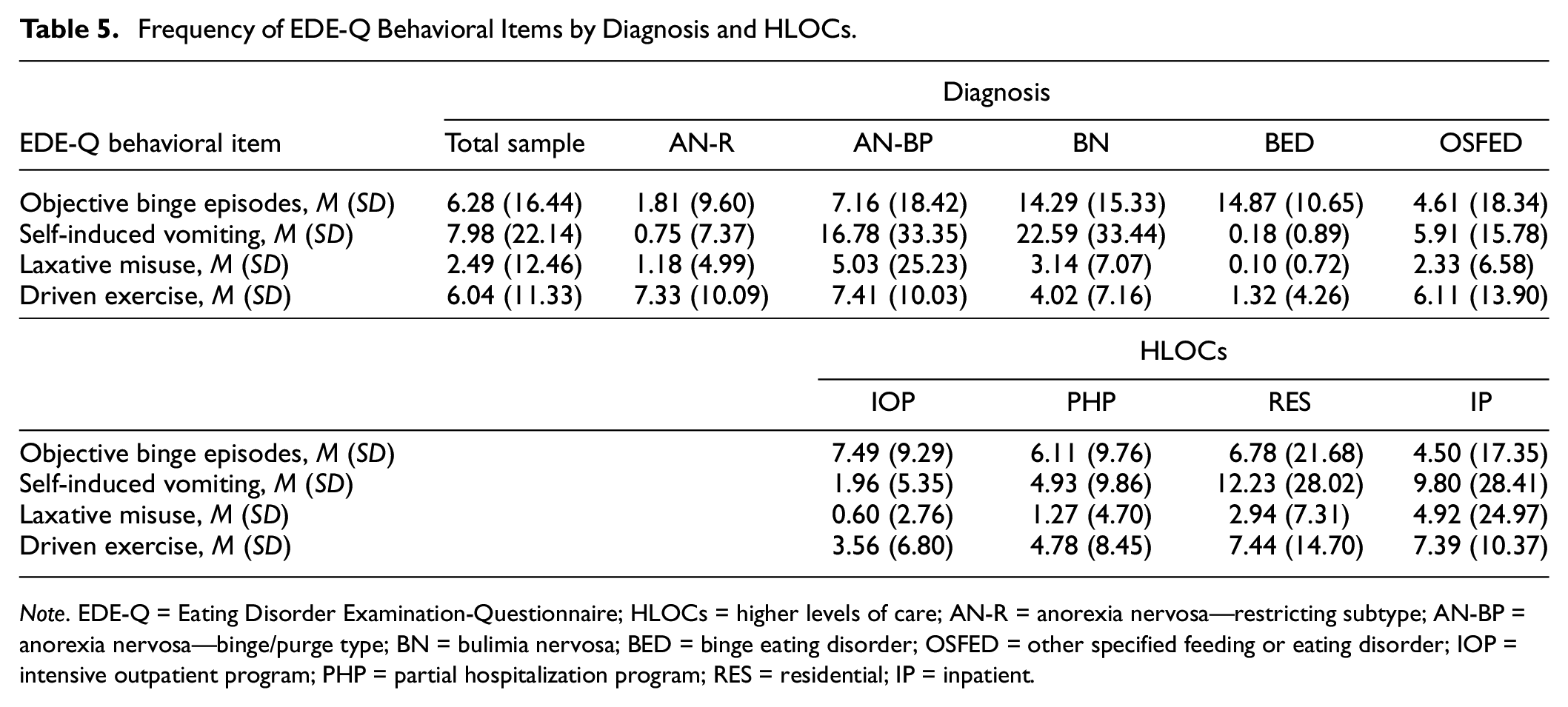
Note. EDE-Q = Eating Disorder Examination-Questionnaire; HLOCs = higher levels of care; AN-R = anorexia nervosa—restricting subtype; AN-BP = anorexia nervosa—binge/purge type; BN = bulimia nervosa; BED = binge eating disorder; OSFED = other specified feeding or eating disorder; IOP = intensive outpatient program; PHP = partial hospitalization program; RES = residential; IP = inpatient.
EDE-Q Subscale T Scores and Raw Percentile Scores by HLOCs
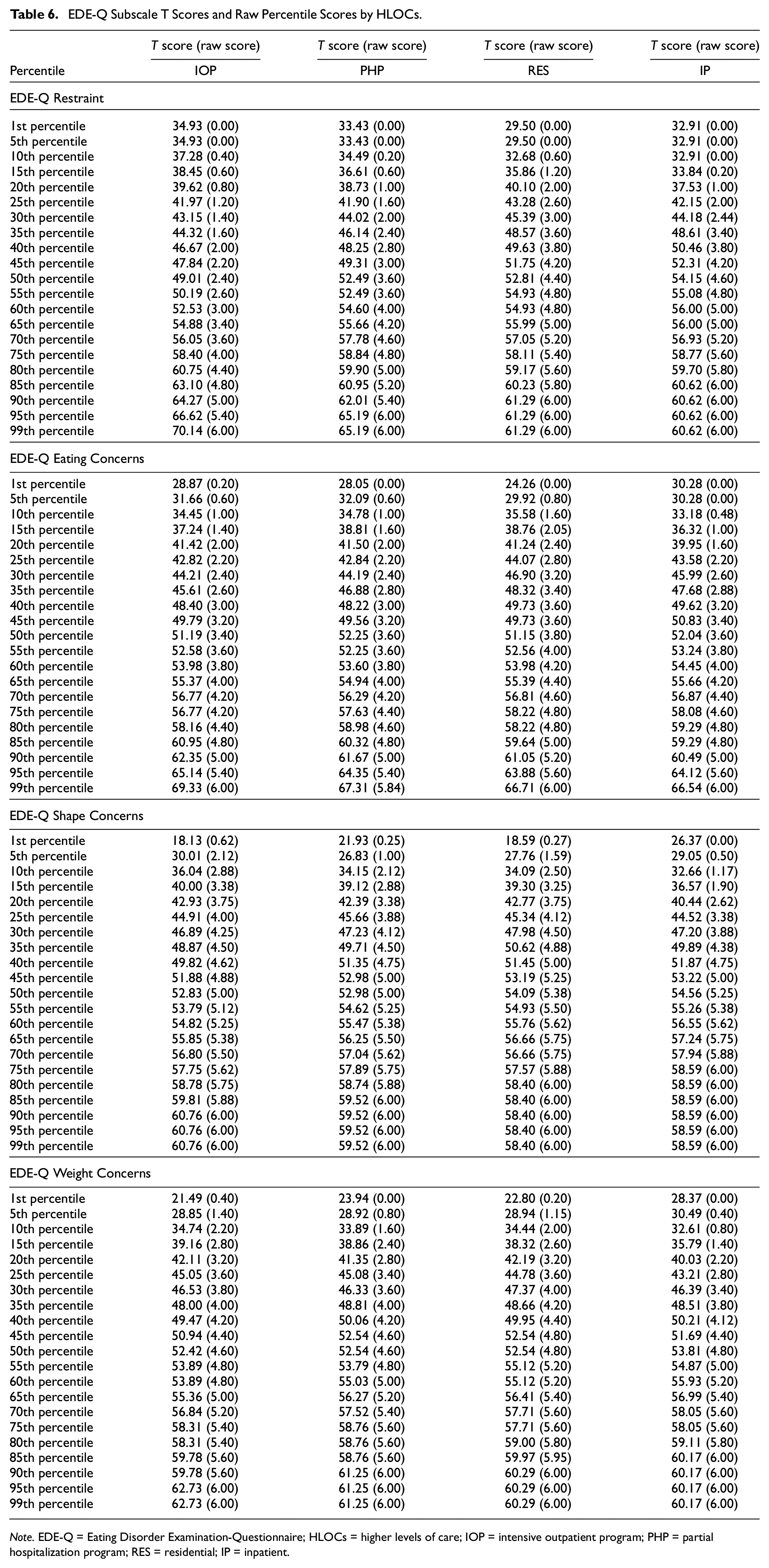
Note. EDE-Q = Eating Disorder Examination-Questionnaire; HLOCs = higher levels of care; IOP = intensive outpatient program; PHP = partial hospitalization program; RES = residential; IP = inpatient.
Discussion
With the largest norms sample to date of adults in HLOCs, this study established EDE-Q norms for adults seeking treatment for an ED at HLOCs. Consistent with previous research, females reported higher EDE-Q Global scores than males (Dahlgren et al., 2017; Smith et al., 2017). Scores in this study are similar to Global scores reported for males and females in PHP and RES HLOCs (Smith et al., 2017), and to a small IP sample of males (Jennings & Phillips, 2017a). Scores are higher than those found in nonclinical samples. For example, Mond et al.’s (2006) study of a general population sample of Australian adult women found a Global EDE-Q score of 1.52. Quick and Byrd-Bredbenner (2013) found a mean Global score of 1.65 for college women and 0.95 for college men in the United States.
Also consistent with previous research, those with AN-R scored lower on the EDE-Q Global score than other diagnostic groups (Smith et al., 2017). This is likely multifactorial, as many of the items on the EDE-Q are more relevant for BN than for AN. For example, questions about restricting one’s food intake “whether or not you have succeeded” seem to be more relevant for BN than for AN (Thomas et al., 2014). In addition, the EDE, upon which the EDE-Q is based, was developed with the cognitive behavioral theory of BN in mind (Thomas et al., 2014). Lower scores may also be due to the minimization of symptoms often seen in AN (APA, 2013; Couturier & Lock, 2006), and also perhaps as a result of the cognitive impairment caused by chronic malnutrition. Although the EDE-Q is arguably the most widely used self-report ED measure, it may not be the best suited for assessing AN symptoms. Having Global EDE or EDE-Q scores within 1 SD of community norms has been used as an indicator of remission in several ED treatment studies (e.g., Lock et al., 2010). Thomas et al. (2014) point out that in a treatment study of adults with AN, 33% of patients scored within 1 SD of community norms on the EDE-Q before treatment even began (Fairburn et al., 2013), further calling into question the accuracy with which the EDE-Q assesses AN symptoms.
This study is among the first to provide normative data on the EDE-Q across the spectrum of HLOCs. The Global score was lowest at IOP, was slightly higher at PHP, and higher at the RES LOC. It was somewhat lower at the IP level, although only RES was significantly higher than IOP. Those receiving treatment at the IP level did not report the highest EDE-Q scores. This finding could be due to malnutrition-induced cognitive impairment, lack of insight, or because of more medical comorbidity or metabolic aberrations found in individuals needing this level of intensive treatment. One study examining cognitive impairment among adolescents receiving IP treatment for AN or BN did not find correlations between cognitive functioning and clinical parameters (Remberk et al., 2011), but it is possible that this relationship is more pronounced among adults who may have longer durations of illness and more brain atrophy. Possibly providing support for this hypothesis, a study of female adolescents admitted to IP reported higher mean EDE-Q Global scores than those found for IPs in the current adult sample (AN-R M score: 3.71; AN-BP M score: 4.71) (Jennings & Phillips, 2017b).
There are several limitations to the current investigation. First, all data are from questionnaires collected at admission to an HLOC, which can be a very stressful time, and may have affected the accuracy of participants’ reporting. Future studies should seek to examine fluctuations in scores before, during, and immediately after completion of an admission to an HLOC, and capture additional information relevant to participants’ EDs, such as duration of illness, which was not available for the current sample. Future research should replicate findings from this study, as well as determine the complexity of responses within settings and the impact of treatment-specific contextual factors, such as stress related to the admission process, on EDE-Q scores. An additional limitation is that all data were collected from one treatment program, and that patients seeking treatment from this program must use private insurance or pay out-of-pocket, which may limit the generalizability of these findings. However, data were collected from multiple sites across the United States that were all part of the same treatment program, and the payor model utilized at ERC is similar to most other HLOC sites in its inclusivity, thus likely mitigating this shortcoming. In addition, although the focus of this study was not on the utility of using a cutoff score of 4 to establish clinical significance, it has been argued that cutoff scores should not be used with the EDE-Q, as they may only be relevant for the population that was included in the original study (Meule, 2021). The decision to use a cutoff score of 4 was based on Fairburn and Cooper’s (1993) suggestion, as well as its use in other treatment studies (e.g., Carter et al., 2001; Jennings & Phillips, 2017b). However, three of the five diagnostic groups scored under 4.0 in this study. Future research should determine whether another cutoff is more appropriate for patients in HLOCs, for patients with AN-R, and for those with the most extreme forms of AN, that is, with body mass indices (BMIs) <14. Finally, although the sample size is large, there are many chronically underrepresented subpopulations (such as noncisgender patients) and intersectional identities (such as Black men) that were unable to be captured in a large enough number to examine. Future studies should seek to oversample these subpopulations. Future research may also seek to establish norms for the EDE-Q using factor structures other than the four subscales that were originally proposed and are arguably the most widely used. A systematic review found that the four-factor structure of the EDE-Q received little empirical support (Jenkins & Rienecke, 2022) and that a brief, 7-item version (Grilo et al., 2010, 2013) may be preferable.
This study provides a comprehensive overview of normative EDE-Q data among a large sample of adults seeking treatment for an ED in HLOCs. In addition to contributing to the limited literature on EDE-Q norms in HLOCs, the current findings have clinical utility. Programs utilizing the EDE-Q to assess treatment outcomes can use these findings to help patients interpret and provide context for their scores.
Footnotes
Author Contributions
Renee D. Rienecke helped in conceptualization and writing—original draft. Philip S. Mehler, Carol B. Peterson, and Daniel Le Grange helped in writing—review and editing. Alan Duffy helped in data curation and writing—review and editing. Dan V. Blalock helped in formal analysis and writing—original draft.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Renee D. Rienecke receives consulting fees from the Training Institute for Child and Adolescent Eating Disorders, LLC, and royalties from Routledge. Daniel Le Grange receives royalties from Guilford Press and Routledge, is the Co-Director of the Training Institute for Child and Adolescent Eating Disorders, LLC, and is a member of the Clinical Advisory Board of Equip Health. Dan V. Blalock receives consulting fees from Eating Recovery Center. All other authors report no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dan V. Blalock is supported by Career Development Award 19–035 (IK2HX003085-01A2) from the U.S. Department of Veterans Affairs Health Services Research and Development Service (HSR&D).
Data Availability Statement
Data will be made available upon reasonable request.