
Abstract
Introduction
Cervical cancer prevalence and incidence are high in sub-Saharan Africa, especially in Uganda, where screening rates are low, despite government policy recommending screening for all women aged 25-49 every three years. Most prior research focuses on client-related barriers to screening, including women’s fears about the screening procedure, lack of partner support, and community-level stigma. Fewer studies elaborate on inner context factors related to health care systems, facilities, and providers. The aim of this study was to use qualitative methods to explore inner context factors that may affect cervical cancer screening in Uganda.
Methods
We recruited 20 health care facility administrators, 6 providers of cervical cancer screening, 2 district health officers, 2 division medical officers, and one government health official for key informant interviews, and 69 women (31 screened and 38 not screened for cervical cancer) for focus group discussions. Participants were recruited from four health care facilities that varied by urbanicity and funding source: one urban public facility, one urban private non-profit facility, one rural public facility, and one rural private non-profit facility.
Results
Inner context themes emerged around infrastructure needs (insufficient space, equipment, and supplies) and staffing issues (inadequate staff quantity and training), which contributed to lower quality of care (e.g., long wait-times; painful, rushed exams). Women described privacy concerns as well as discomfort with male and young providers. Women with HIV were prioritized for screening based on funding streams and inability to serve all women given infrastructure and staffing issues. Despite barriers, many stakeholders were committed to providing cervical cancer screening services, and many women saw the value of screening.
Conclusion
This study identified inner context barriers related to resource shortfalls, which affected quality of care. Low cost solutions are needed to improve health care readiness and increase reach of cervical cancer screening in Uganda.
Keywords
Introduction
In sub-Saharan Africa, prevalence and incidence of cervical cancer are among the highest globally1-3: In 2022, multiple countries across the continent—in Eastern (Burundi, Tanzania, Uganda), Western (Guinea), and Southern (Eswatini, Lesotho, Mozembique, Zambia, Zimbabwe) Africa showed the highest level of standardized incidence rates worldwide (from 45.3-95.9 per 100,000). In Uganda in particular, cervical cancer is the leading cause of cancer-related deaths among women; the age-standardized incidence and mortality rates are 53.8 and 40.6 per 100,000, respectively. 4 Ugandan government policy states that all women aged 25 to 49 years-old should be screened for cervical cancer every 3 years. 5 Evidence-based visual inspection with acetic acid (VIA) screening and thermal cryotherapy for pre-cancerous lesions are available at low or no cost to women, mostly through midwives and nurses in health care facilities. 6 However, a minority of women in sub-Saharan Africa are estimated to have ever screened for cervical cancer,7,8 and late-stage presentation for screening is common. 9 In a five-country analysis of data from 2011 to 2018 across sub-Saharan African regions (Benin, Ivory Coast, Kenya, Namibia, Zimbabwe), 19% of women on average (95% confidence interval = 18.5% to 19.5%) were estimated to have ever screened for cervical cancer. 8 In Uganda, across different samples, an estimated 5-35% of women have been screened, and an estimated 80% have advanced cancer when initiating care.6,10 Moreover, most women diagnosed with cervical cancer cannot afford treatment and do not live near treatment centers. Thus, early detection and prevention through screening are critical.
Consistent with the implementation science literature suggesting that inner context factors (within clinics) and outer context (extra-clinic) factors (e.g., policy, community norms, client attitudes) impact implementation of evidence-based practices,11,12 research has identified factors at multiple levels that affect cervical cancer screening implementation in sub-Sanahan Africa.13-15 Prior research across sub-Saharan African has primarily focused on outer context factors related to client barriers to cervical cancer screening, including low knowledge and awareness, misconceptions and fear regarding cervical cancer screening (e.g., perceptions that it damages the uterus, causes infertility, and is painful), stigma around cervical cancer and the screening process, and lack of partner support.13,14,16-23 Stigma can stem from fear of having cancer (and anticipated cancer stigma), shame around having symptoms of a sexually transmitted infection and advanced disease (e.g., bleeding, discharge), as well as embarrassment from the screening procedure itself (including disrobing), especially with male providers. Women may need to get permission for screening and treatment from male partners, who may be unsupportive, especially if the woman needs to abstain from sexual intercourse when healing after treatment.
Socio-demographic outer context factors at the client level, such as poverty and geographic location also may hinder screening in Uganda as well as sub-Saharan Africa as a whole: those who live far from screening facilities, who do not have access to financial support for medical care, and who live in rural areas are less likely to get screened,13,14,16,17,22,24 suggesting that transport costs are a barrier. In sub-Saharan Africa, women with HIV also have been more likely to be screened, potentially because some donor and partner organizations provide funds for services for people with HIV only.16,17,25,26 In addition, insufficient funding for cervical cancer screening and management overall greatly hinders implementation in sub-Saharan Africa. 13
Relatively less research in sub-Saharan Africa has described organizational barriers to cervical cancer screening in the inner context (i.e., at the health care facility and provider levels).13,24 In sub-Saharan Africa as well as Uganda specifically, inner context factors at the organizational level include insufficient or lack of resources and equipment, long wait-times, and staffing shortages.13,14,17,24,25,27 At the provider level, studies have identified inadequate knowledge and skills, in part due to high staff turn-over and lack of training opportunities, as well as lack of recommendation or encouragement to screen.13,18,28,29 Research in several sub-Saharan African countries also has found poor patient experience to be an issue13,14; for example, in a focus group study of screening-eligible women in Uganda, some participants noted that screened women’s stories of providers causing pain or being rude during the screening process deterred other women in the community from getting screened. 20
In sum, prior research on barriers to cervical cancer screening implementation in sub-Saharan Africa has mainly focused on outer context factors related to client characteristics. Thus, the purpose of the present paper was to explore implementation factors at the inner context health care system, facility, and provider levels that contribute to low cervical cancer screening levels in Uganda. We collected data across multiple levels of stakeholders: health care facility administrators, screening providers, government officials, women who had been screened for cervical cancer, and women who had not been screened.
Methods
Setting
This study was conducted in four health care facilities offering cervical cancer screening that varied by urbanicity and funding source: two urban clinics, one public and one private non-profit, in Kampala, Uganda, and two rural clinics, one public and one private non-profit, near Jinja, Uganda. A substantial percentage of the Ugandan population utilizes public and private non-profit facilities (about 40% each), increasing this study’s external validity. 30
Study Design and Implementation Framework
We conducted a cross-sectional qualitative study in four health care facilities that used key informant interviews with health care workers and policymakers, and separate focus groups with female clients who had and had not been screened for cervical cancer. Our research was guided by the Exploration, Preparation, Implementation and Sustainability (EPIS) implementation framework, 11 which highlights inner and outer contextual factors and dynamic phases of implementation; this qualitative study, which was conducted under the Preparation phase of EPIS, aimed to identify inner context barriers to easy access to and delivery of CC screening. This qualitative analysis represents the first step of a larger study on a social network intervention to increase cervical cancer screening demand among women in Uganda. 31 After this qualitative phase, following EPIS’s dynamic phases, the team remediated barriers uncovered in the qualitative analysis in Plan-Do-Check-Act (PDCA) cycles, 32 evaluated intervention implementation, and then observed sustainment of the social network intervention in the same four facilities.
Participants and Procedures
A total of 31 individuals participated in 60-minute audio-recorded qualitative key informant interviews; individuals were eligible if they were a healthcare administrator or provider in one of the study clinics, or a relevant government health official. A total of 20 health care facility administrators, including directors, department heads, and managers (4-6 per facility; physician specialists, nurses, and other types of senior managers), 6 providers of cervical cancer screening (1-2 per facility; 5 midwives, 1 assistant nursing officer), 2 district health officers, 2 division medical officers, and one government health official. The majority of interview participants were women (n = 17, 56.7%), and their average age was 45.7 years (SD = 8.5, range = 32-63); they had worked in health care an average of 14.8 years (SD = 9.8, range = 1-36).
Using a purposive (selective) sampling method, study team members attended health care facility staff meetings and offered participation to staff; the government official was known by members of the research team and thus called directly. Interview participants were told that the purpose of the study was “to explore how to best ensure that women have access to and are utilizing cervical cancer screening services here at the clinic.” All interviews were conducted in English in a private facility space or office by trained local Ugandan Co-Investigators with MDs, PhDs, or both (one man and four women). Participants were given the equivalent of $8 cash (in Ugandan Shillings). Interviews took place from October, 2023-January2024.
A total of 69 women were recruited across the targeted health care facilities to participate in focus group discussions in October, 2023: 31 women who were screened for cervical cancer (range = 6-9 per facility) and 38 women who were not screened for cervical cancer (range = 8-11 per facility). Individuals were eligible for the focus groups if they were a woman aged 25 years-old or older and a client at the health care facility. Using a convenience sampling strategy, providers of gynecological care, HIV care treatment and support, and family planning services told clients who had never been screened about the study, and providers of cervical cancer screening told clients who were recently screened for cervical cancer (who screened negative as well as those who were treated for pre-cancerous lesions) about the study. They were told that the purpose of the study was “to explore how to best ensure that women get periodically screened for cervical cancer risk.” Interested women were contacted and offered participation by the local study coordinator. Two focus group discussions by two local team Co-Investigators (both women, one with MD/MPH training and one with PhD training) were conducted in a private room at each facility (eight total): Four focus groups with women who had been screened for cervical cancer and four different focus groups with women who had not been screened. The 60-minute focus groups were audio-recorded and conducted in Luganda by trained bilingual local staff. Women were provided with refreshments during the discussion and the equivalent of $8 in transport reimbursement.
The team did not conduct interim analyses to inform saturation and sample size; instead, the team pre-determined sample sizes based on standard guidance for code and meaning saturation in qualitative research,33,34 as well as the number of relevant health care workers at each facility who served unique roles in the cervical cancer screening process.
Qualitative Guides
Example Qualitative Questions to Elicit Information About Health Care System, Facility, and Provider Factors in Cervical Cancer Screening, by EPIS Subdomain

Qualitative Data Collection, Management, and Analysis
The team used a deductive directed content analysis strategy, in which broad categories of inner context factors affecting implementation under the EPIS framework (facility organizational characteristics, organizational staffing processes, individual characteristics) guided construction of the codebook and the analysis. 35 Members of the Uganda team transcribed the interviews and focus groups, and used standard methods to translate and back-translate focus group discussions into English. Two members of the US team (PhD Co-Principal Investigator and MPH Project Coordinator, both women) first read all transcripts, and then, with input from a Ugandan Co-Investigator (a woman), wrote preliminary summaries of overall and health care facility-specific results. These summaries were refined with Uganda team input, after which Ugandan and U.S. study team co-authors discussed and refined the facility-specific results with administrators and providers in all four facilities in separate in-person meetings.
After the health care facility meetings, the PhD Co-Principal Investigator and MPH Project Coordinator from the U.S. developed a codebook, which was refined iteratively with two non-Ugandan graduate students in public policy (who served as coders) and then uploaded along with all transcripts into Dedoose 36 (qualitative data management software). The coding team met to refine the codebook, iteratively coding transcripts and revising the codebook as needed. Once the codebook was fully refined, the two coders coded approximately 13% of the transcripts (n = 3 or 10% of interviews; n = 2 or 25% of focus groups), randomly selected by Microsoft Excel random function. After satisfactory interrater reliability was established (Cohen’s Kappa = 0.774), 37 the two coders reviewed and updated all previously coded transcripts to align with the final codebook, and then divided the coding between the remaining transcripts. The coders continued to meet weekly, with the PhD Co-Principal Investigator and MPH Project Coordinator resolving any coding differences as needed. The PhD Co-Principal Investigator reviewed all final codes, after which the MPH Project Coordinator reviewed coded transcripts and updated the preliminary summary, focusing on key themes that strongly emerged across participant groups and facilities. Because no clear differences in themes emerged by type of facility, and to preserve confidentiality and reduce potential for identifiability in urban and rural locations, specific quotations are identified by facility funding source only rather than the cross of urbanicity by funding source.
All participant details have been de-identified. The reporting of this study conforms to the COREQ guidelines. 38 The team ensured trustworthiness,39,40 including: credibility through triangulating themes across multiple data sources (i.e., different types of stakeholders) and methods (key informant interviews and focus groups), and validating findings (i.e., presenting and discussing results) in meetings with health care workers at the facilities where data collection occurred; transferability through comprehensive description of the methods (participants, setting, procedures), such that applicability of the results to other contexts can be determined; dependability through documentation of all research steps (e.g., qualitative analysis, interrater reliability) with a standards of procedures manual and weekly study updates; and confirmability through discussions about data interpretation with multiple levels of relevant stakeholders in Uganda (e.g., policymakers, health care providers, local community advisory board members) and the Uganda study team.
Ethical Approvals
Study procedures were approved by the RAND Human Subjects Protection Committee (HSPC#2023-N0111; May 4, 2023) in the U.S., and Makerere University School of Public Health Higher Degrees, Research, and Ethics Committee (HDREC#SPH-2023-412; May 26, 2023) and the Ugandan National Council of Science and Technology (HS SS1873ES; July 13, 2023) in Uganda. The study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2024. Interview participants provided verbal informed consent and focus group participants provided written informed consent.
Results
Overview
Exemplary Quotes by Theme and Subtheme Representing Inner Context Implementation Factors in Cervical Cancer Screening in Uganda
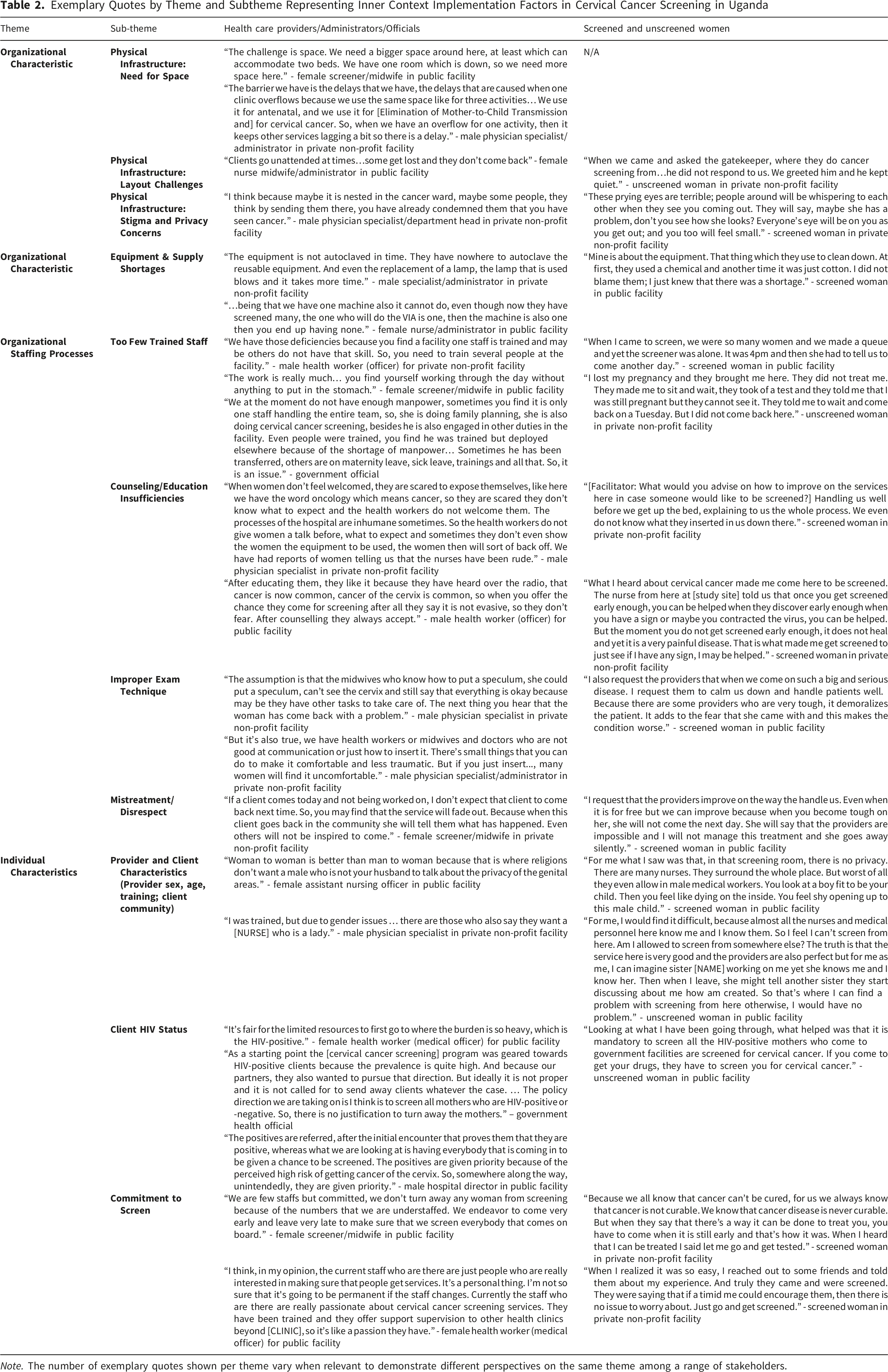
Note. The number of exemplary quotes shown per theme vary when relevant to demonstrate different perspectives on the same theme among a range of stakeholders.
Organizational Characteristics
Inadequate equipment and supplies affected clients negatively. Screened women in two focus groups in public clinics commented on the effects of equipment and supply shortages on the screening experience. Some providers discussed turning clients away or long wait times, if there was insufficient time to sterilize speculums in between screenings. A screener mentioned that facilities tend to stock one standard speculum size only, which could lead to discomfort and pain, such as if the speculums were too large for nulliparous women.
Clients complained of discomfort, and staff said that discomfort can be a training issue, because some staff do not employ correct techniques. For example, some screeners do not prepare speculums appropriately (to be correct size, warmed, and lubricated)—although, as noted above, some facilities stocked only one speculum size. Low skill or lack of proper attention could result in painful screening. Moreover, women who experienced pain or who felt disrespected might not return for screening or treatment, or might discourage other women from screening.
Individual Characteristics
Discussion
This qualitative study in a low-income country with high cervical cancer prevalence and low screening rates uncovered inner context health care system, facility, and provider challenges to screening implementation. Across urban and rural public and private non-profit facilities, multiple types of stakeholders described how resource issues related to space, equipment, supplies, and staffing (in the inner context) could lead to inability to screen all women aged 25-49 every three years, per government policy. In most clinics, stakeholders noted that the demand for screening sometimes exceeded available staffing and infrastructure resources, consistent with prior research in sub-Saharan Africa.13,14,24 Our research extends prior studies in Uganda and sub-Saharan Africa as a whole,14,17,24 which have established client-related (outer context) barriers such as misconceptions and fears about the screening process, community stigma around cancer, and male partner barriers, and rarely include perspectives of health care providers, administrators, and policymakers.
Prior research in sub-Saharan Africa, including in Uganda, has found that women may be reluctant to be screened because they are concerned about discomfort and pain, as well as long wait times; they also may have misconceptions and lack of awareness about the procedure.14,16-23 Our research indicates that such client fears may have some basis in truth. Screeners may rush through examinations and not have time to provide sufficient counseling or to warm instruments; screeners also may not have access to resources that would allow them to serve more women, including additional equipment to sterilize more speculums, or access to different size speculums to lower the discomfort of the procedure. Such resource limitations may reduce providers’ motivation to offer screening and increase their workload. 13
Our research suggests cause for optimism in overcoming barriers. Despite substantial inner context barriers to cervical cancer screening, policymakers, administrators, and providers persevered, supporting screening for as many women as resources would allow. Women too believed in overcoming their fears and navigating difficult clinic experiences to get screened. Across narratives, stakeholders shared their commitment to improving the screening process, given the high rates of cervical cancer, combined with few treatment options for advanced disease, in the country.
Based on our results, we propose several specific recommendations for increasing cervical cancer screening in this low-resource environment. As prior qualitative research suggests that compassionate, respectful care facilitates retention,41,42 policymakers and health care administrators could require trainings for cervical cancer screening providers to improve their skills and to practice client-centered care; such training seems critical to increase demand for screening, given the inherent discomfort of the screening procedure. Training could include preparing clients by telling them what to expect, ensuring that speculums are warmed and available in different sizes; clinics could also stock plastic disposable speculums (that do not need to be sterilized in between clients) as a back-up, to decrease waiting time or ability to serve all clients. Moreover, improved infrastructure and greater resources (i.e., expanding space, increasing staff, and ensuring sufficient supplies and equipment) from public and private funders would address many of the barriers detailed in the present study, but such changes can be unrealistic for low-resource settings if cost is prohibitive and supply stockouts are beyond the control of individual facilities. Creative, cost-effective solutions could include reconfiguring space and adding appropriate signage for easier navigation to screening rooms, and training more clinic staff on screening procedures, even if their daily responsibilities are in other departments, so that more staff are available when demand is high.
Consistent with prior research,23,25 stakeholders mentioned the need for community sensitization about cervical cancer and screening, to raise awareness, overcome misconceptions, and convince male partners of the high need—which in turn would help women to feel more prepared and knowledgeable about the screening process prior to the clinic visit. However, standard community education strategies have not consistently increased screening uptake. 43 Social network interventions, in which pre-existing social ties with known others in the community are leveraged to diffuse health information in communities, have shown promise for cervical cancer prevention.44,45 For example, in the Game Changers for Cervical Cancer Prevention group-based intervention, originally developed for HIV and adapted for cervical cancer,31,46,47 women who have been screened for cervical cancer are trained to engage in peer advocacy. Results of a pilot study showed significantly increased cervical cancer knowledge and uptake of cervical cancer screening among social network members. 47 Although such community-based interventions can be effective, local health care facilities first need to be prepared for the surge in demand for screening that result from such interventions, by addressing the inner context factors described above. 31
Limitations of this study include qualitative data collection in only four clinics in a lower-income country—one of each type representing the cross of urbanicity and funding source. Results may not be generalizable to other countries, especially those of higher income, or other health care facilities. We triangulated results across data collection sources at multiple levels, reducing the likelihood of bias from any one individual source. Moreover, we did not systematically collect facility-level quantitative data on the number of health facilities providing cervical cancer screening services in the study areas or on the number of women screened for cervical cancer in the clinic catchment areas, which would have provided useful contextual information for our analysis.
Conclusion
In this qualitative study of cervical cancer screening implementation factors in Uganda, multiple types of stakeholders were engaged, including at the national policy level. The similarity of our findings with other studies on cervical cancer screening barriers in Uganda and sub-Saharan Africa lends credence to our results. Furthermore, by elucidating the inner context factors that can impede smooth cervical cancer screening, our research can help to determine solutions to address outer-setting factors related to lack of community demand for screening.
Footnotes
Acknowledgments
We are grateful for the participants who shared their stories and the community advisory boards who contributed their insights.
Ethical Considerations
Study procedures were approved by the RAND Human Subjects Protection Committee (HSPC#2023-N0111; May 4, 2023), Makerere University School of Public Health Higher Degrees, Research, and Ethics Committee (HDREC#SPH-2023-412; May 26, 2023), and the Ugandan National Council of Science and Technology (HS SS1873ES; July 13, 2023).
Consent to Participate
Interview participants provided verbal informed consent and focus group participants provided written informed consent.
Author contributions
Conceptualization (Bogart, Beyeza-Kashesya, Gwokyalya, Ober, Wagner, Wanyenze), Methodology (Bogart, Ober, Wagner), Validation (Bogart, Rukundo, Timmins, Whitaker), Formal Analysis (Bogart, Rukundo, Timmins, Whitaker), Investigation (Beyeza-Kashesya, Gwokyalya, Matovu, Nakami, Namisango), Data Curation (Gwokyalya, Whitaker), Funding Acquisition (Bogart, Wagner, Wanyenze), Project Administration (Gwokyalya, Nakami, Namisango, Whitaker), Writing – Original Draft (Bogart, Whitaker), Writing – Review & Editing (Bogart, Beyeza-Kashesya, Green, Gwokyalya, Matovu, Nakami, Namisango, Ober, Timmins, Rukundo, Wagner, Wanyenze, Whitaker).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Cancer Institute of the U.S. National Institutes of Health (Grant # R01CA282284).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.