
Abstract
Background
Cardiogenic shock remains a life-threatening condition with persistently high mortality. Norepinephrine and dopamine are commonly used vasoactive agents; however, comparative data on clinical outcomes remain limited.
Methods
This retrospective cohort study included 388 adults with cardiogenic shock treated with norepinephrine (n = 72) or dopamine (n = 316) at King Chulalongkorn Memorial Hospital, Thailand. The primary outcome was 28-day mortality. Survival was evaluated using Kaplan–Meier analysis and Cox proportional hazards regression. Inverse probability of treatment weighting (IPTW) was applied to adjust for confounding by indication.
Results
Mortality at 28 days occurred in 30.6% and 25.9% of the norepinephrine and dopamine groups, respectively. No statistically significant difference in 28-day mortality was observed in either the unadjusted (HR 0.84, 95% CI 0.52-1.34; P = .463) or IPTW-adjusted Cox proportional hazards model (HR 1.10, 95% CI 0.64-1.88; P = .725). Epinephrine rescue rates were comparable between groups (27.7% vs 24.2%; P = .551). Independent predictors of 28-day mortality included age ≥65 years, cardiopulmonary resuscitation, and epinephrine use (P < .001 for all), as well as renal replacement therapy and endotracheal intubation (P = .003 for both).
Conclusion
The present study did not demonstrate a significant difference in 28-day mortality between norepinephrine and dopamine; however, dopamine was associated with a significantly higher incidence of arrhythmias.
Introduction
Cardiogenic shock (CS) is a life-threatening condition characterized by low cardiac output and inadequate tissue perfusion, typically accompanied by a mean arterial pressure <65 mm Hg or a systolic blood pressure <90 mm Hg.1–4 The most common cause of CS is acute myocardial infarction with left ventricular dysfunction. 4 Although reperfusion strategies and supportive care have advanced considerably over recent decades, the incidence of CS continues to rise, and in-hospital mortality remains as high as 40% to 60%.5,6
Current management guidelines from the Heart Failure Council of Thailand, the American Heart Association, and the European Society of Cardiology recommend the use of inotropic agents in patients with CS and evidence of hypoperfusion despite adequate volume status.1,2,7 Vasopressors, including norepinephrine and dopamine, are commonly used to restore blood pressure and maintain vital organ function. 2 However, both agents can increase myocardial oxygen demand and have been associated with an increased risk of arrhythmias and myocardial ischemia.8,9
De Backer et al conducted a multicenter randomized trial and reported a significantly higher 28-day mortality rate among a predefined subgroup of patients with CS who received dopamine, as well as a higher rate of arrhythmic events compared with those receiving norepinephrine. 10 Nevertheless, direct evidence comparing these agents in CS derives largely from a prespecified subgroup analysis of a single multicenter randomized trial, while real-world comparative data from routine clinical practice remain limited. Therefore, this study aimed to compare 28-day mortality between patients with CS receiving norepinephrine and those receiving dopamine.
Ethics Approval
This retrospective study followed the Helsinki Declaration and received Institutional Review Board approval from the Faculty of Medicine, Chulalongkorn University (IRB No. 531/64).
Methods
Study Design and Patient Population
The researchers conducted an analytical, retrospective cohort chart review of patients diagnosed with cardiogenic shock who received either norepinephrine or dopamine as initial vasoactive agents at the Coronary Care Unit (CCU) or the Intermediate Coronary Care Unit (ICCU) at King Chulalongkorn Memorial Hospital, a public tertiary care hospital in Thailand. Data were collected from January 1, 2014 to September 30, 2022. Patients were identified using either medication dispensing records for norepinephrine or dopamine, or the International Classification of Diseases, 10th Revision (ICD-10) diagnostic codes for cardiogenic shock.
Patients were eligible for inclusion if they met all the following criteria: (1) age ≥18 years; (2) admitted to the CCU or ICCU with cardiogenic shock requiring either norepinephrine or dopamine therapy; and (3) cardiogenic shock confirmed despite adequate fluid resuscitation, defined by at least one of the following:
At least one clinical or laboratory sign of tissue hypoperfusion with systolic blood pressure <90 mm Hg for ≥30 min. Clinical signs included altered mental status, cold extremities, oliguria (<0.5 mL/kg/h, <30 mL/h, or <500 mL/day), or narrow pulse pressure. Laboratory signs included arterial pH <7.35, lactate ≥2 mmol/L, or an increase in serum creatinine of ≥0.3 mg/dL or ≥1.5 times the baseline value. Hemodynamic criteria, defined as systolic blood pressure <90 mm Hg for ≥30 min with cardiac index ≤2.2 L/min/m2 and pulmonary capillary wedge pressure (PCWP) ≥15 mm Hg. Diagnostic code criteria, defined by a documented diagnosis of cardiogenic shock according to ICD-10.
Patients were excluded if any of the following conditions applied: (1) suspected shock of another etiology, including septic, anaphylactic, hypovolemic, or neurogenic shock, occurring within 24–48 h prior to norepinephrine or dopamine initiation; (2) concomitant use of both norepinephrine and dopamine for cardiogenic shock management; or (3) cardiogenic shock not being the first presenting shock episode.
Data Collection
Baseline characteristics and hemodynamic parameters were extracted from electronic medical records for all eligible patients. Maximum vasopressor doses and total treatment durations were recorded for each agent. Serial vasopressor doses were extracted at prespecified time points (0, 6, 12, 24, 48, and 72 h after initiation) to characterize dose trajectories. Arrhythmia events were ascertained from physician-documented diagnoses and continuous cardiac telemetry records; telemetry was performed at intervals of no greater than one hour for all patients in both groups, who were managed exclusively in the CCU and ICCU throughout the study period.
Objectives
The primary outcome was 28-day mortality, defined as all-cause mortality within 28 days of cardiogenic shock diagnosis. Secondary outcomes included the requirement for epinephrine as rescue therapy after norepinephrine or dopamine failure, and the incidence of arrhythmias.
A prespecified multivariable analysis was performed to identify baseline characteristics independently associated with 28-day mortality, including age ≥65 years, diabetes mellitus, hypertension, obesity, multivessel coronary artery disease (≥2 vessels), elevated systemic vascular resistance, endotracheal intubation, cardiopulmonary resuscitation, renal replacement therapy, and mechanical circulatory support.
In addition, post hoc exploratory analyses examined the association of 28-day mortality with acute coronary syndrome (ACS) etiology of shock, initial mean arterial pressure, elevated lactate, left ventricular ejection fraction (LVEF) < 40% at the time of diagnosis, transfer status, and concomitant use of other vasoactive agents, including dobutamine, milrinone, and epinephrine.
Statistical Analysis
Continuous variables are presented as median (IQR), and categorical variables as frequency (percentage). Between-group comparisons were performed using the Wilcoxon rank-sum test for continuous variables, and the chi-square test or Fisher's exact test for categorical variables, as appropriate.
Missing data in continuous baseline variables (left ventricular ejection fraction (LVEF), mean arterial pressure at diagnosis, and serum lactate) were handled using multiple imputation by chained equations (MICE) with predictive mean matching (k = 5 nearest neighbors). Forty imputed datasets were generated using a fixed random seed (12345) to ensure reproducibility. Convergence was assessed using trace plots of posterior means and standard deviations across iterations; all variables demonstrated stable mixing without systematic trends. Adequacy was further confirmed by comparing the distributions of imputed values against observed data. The imputation model included all covariates in the propensity score model (age ≥ 65 years, resuscitation status, endotracheal intubation, renal replacement therapy, mechanical circulatory support, epinephrine use, and dobutamine use), treatment group, 28-day mortality, and follow-up time.
To address confounding by indication, propensity scores were estimated using multivariable logistic regression. Candidate covariates were identified based on clinical relevance, informed by the published literature, and driven by significant baseline imbalance between groups. These candidates were then examined using univariable logistic regression, and variables with P < .10 were subsequently included in the propensity score model. Stabilized inverse probability of treatment weights (IPTW) were derived from the propensity scores and applied to create a weighted pseudo-population. Covariate balance before and after weighting was assessed using standardized mean differences (SMDs), with an SMD <0.10 considered indicative of adequate balance.
The primary outcome (28-day mortality) was analyzed using Cox proportional hazards regression. Unadjusted and multivariable-adjusted Cox models were first conducted, followed by an IPTW-weighted Cox model with robust variance estimation as the primary analysis. Results are expressed as hazard ratios (HRs) with 95% confidence intervals (CIs). Kaplan–Meier survival curves were constructed to illustrate survival over the 28-day follow-up. A sensitivity analysis was performed using complete-case data, restricted to patients with available baseline lactate and LVEF measurements (n = 192).
Secondary outcomes were analyzed using unadjusted logistic regression for epinephrine rescue therapy and the chi-square test for arrhythmia incidence. Results are expressed as odds ratios (ORs) with 95% CIs where applicable.
Changes in hemodynamic parameters over time were analyzed using linear mixed-effects models with treatment group, time, and their interaction as fixed effects, and patient as a random effect to account for repeated measurements. Estimated marginal means were compared between groups at each time point with Bonferroni correction for multiple comparisons. Vasopressor dose trajectories from hour 0 (H0) to hour 72 (H72) are summarized descriptively, with mean (± standard error) doses graphed for each treatment group, without formal statistical comparisons.
Post-hoc subgroup analyses were performed within the IPTW-weighted population to examine the association between vasopressor type and 28-day mortality among patients stratified by cardiogenic shock etiology (ACS-related vs non-ACS-related), prior cardiopulmonary resuscitation, and mechanical circulatory support use. Interaction terms between treatment assignment and each subgroup variable were incorporated into the IPTW-adjusted Cox model to formally test for effect modification. These analyses were exploratory in nature and should be interpreted accordingly.
All analyses were performed using Stata version 19.5 (StataCorp LLC, College Station, TX, USA). A two-sided P < .050 was considered statistically significant.
Results
Patient Characteristics
A total of 831 patients with a recorded history of norepinephrine or dopamine use or an ICD-10 diagnostic code for cardiogenic shock were identified from admissions to the CCU or ICCU. Of these, 388 patients met the eligibility criteria and were assigned to the norepinephrine group (n = 72) or dopamine group (n = 316). A total of 443 patients were excluded, mainly due to suspected shock of another etiology or mixed shock (n = 221), concomitant use of both norepinephrine and dopamine (n = 194), or cardiogenic shock not being the first presenting shock episode (n = 11) (Figure 1).

Flowchart of patient inclusion.
Among the 388 patients included in the study, the majority (85.1%) met the inclusion criterion (a). Clinical signs of hypoperfusion were present in 71.9% of patients, and laboratory signs were observed in 58.5%. Invasive hemodynamic monitoring using Swan–Ganz catheterization was performed in 64 of 388 patients (16.5%) and was more frequent in the norepinephrine group than in the dopamine group (31.9% vs 13.0%; P < .001). Among patients who underwent Swan–Ganz catheterization, 5.9% fulfilled criterion (b). The mean cardiac index and PCWP among these patients were 1.52 ± 0.46 L/min/m2 and 24 ± 6 mm Hg, respectively, with no statistically significant difference between groups (PCWP: P = .897; cardiac index: P = .179). Criterion (c) was met by 68.8% of patients (Table 1).
Inclusion Criteria.

Note: Inclusion criteria were defined as meeting either criterion (a), (b), or (c). All continuous variables are reported as median (interquartile range) and categorical variables as frequency (%). P values are from the chi-square test.
Abbreviations: CI, Cardiac Index; ICD-10, International Classification of Diseases, 10th Revision; PCWP, Pulmonary Capillary Wedge Pressure; SBP, Systolic Blood Pressure; SVR, Systemic Vascular Resistance.
The baseline characteristics of the enrolled patients are shown in Table 2. The median age of all included patients was 64 years, and 61.6% were male. Most patients were admitted to the CCU, with 40.2% transferred from other hospitals. The most common etiology of cardiogenic shock was acute coronary syndrome (59.0%; 43.1% in the norepinephrine group vs 62.7% in the dopamine group; P = .002), of which 78.2% were ST-elevation myocardial infarction (STEMI) and 21.8% non-ST-elevation myocardial infarction (NSTEMI) or unstable angina (UA). Other etiologies included congestive heart failure (17.8%), arrhythmia (11.1%), valvular heart disease (5.4%), myocarditis or pericarditis (2.1%), pulmonary embolism (1.3%), and others (3.4%). Median LVEF at the time of diagnosis was 38% (n = 222); the proportion of patients with LVEF <40% was 51.8% overall (62.3% in the norepinephrine group vs 49.4% in the dopamine group; P = .070). Baseline comorbidities and prior beta-blocker use were similar between groups. Cardiopulmonary resuscitation prior to vasoactive agent initiation, endotracheal intubation, and renal replacement therapy were all significantly more frequent in the norepinephrine group (33.3% vs 21.5%, P = .033; 72.2% vs 46.8%, P < .001; and 31.9% vs 16.8%, P = .003, respectively).
Baseline Patient Characteristics.

Note: All continuous variables are reported as median (interquartile range) and categorical variables as frequency (%).
Abbreviations: ACS, Acute Coronary Syndrome; ALT, Alanine Aminotransferase; AST, Aspartate Aminotransferase; CAD, Coronary Artery Disease; CI, Cardiac Index; COPD, Chronic Obstructive Pulmonary Disease; CVP, Central Venous Pressure; DVD, Double Vessel Disease; Hb, Hemoglobin; HFmrEF, Heart Failure with Mildly Reduced Ejection Fraction; HFpEF, Heart Failure with Preserved Ejection Fraction; HFrEF, Heart Failure with Reduced Ejection Fraction; HR, Heart Rate; LVEF, Left Ventricular Ejection Fraction; MAP, Mean Arterial Pressure; NSTEMI, Non-ST-Elevation Myocardial Infarction; PCWP, Pulmonary Capillary Wedge Pressure; SBP, Systolic Blood Pressure; STEMI, ST-Elevation Myocardial Infarction; SVD, Single Vessel Disease; SVR, Systemic Vascular Resistance; TB, Total Bilirubin; TVD, Triple Vessel Disease; UA, Unstable Angina.
The Fisher's exact test was used instead of the chi-square test when the expected count in any cell was <5.
Variables with missing values.
28-Day Mortality
The overall 28-day mortality rate was 26.8%; 22 patients (30.6%) in the norepinephrine group and 82 patients (25.9%) in the dopamine group died within 28 days (Table 3). In the unadjusted Cox proportional hazards model, dopamine was not significantly associated with 28-day mortality compared with norepinephrine (HR 0.84, 95% CI 0.52-1.34; P = .463) (Table 4 and Supplement S1). After multivariable adjustment for age ≥65 years, cardiopulmonary resuscitation, endotracheal intubation, renal replacement therapy, mechanical circulatory support, lactate ≥2 mmol/L, LVEF <40% at the time of diagnosis, dobutamine use, and epinephrine use, the association remained nonsignificant (adjusted HR 1.25, 95% CI 0.79-1.98; P = .336) (Table 4 and Figure 2).

Kaplan–Meier survival curve with multivariable-adjusted HR.
Clinical Outcomes.
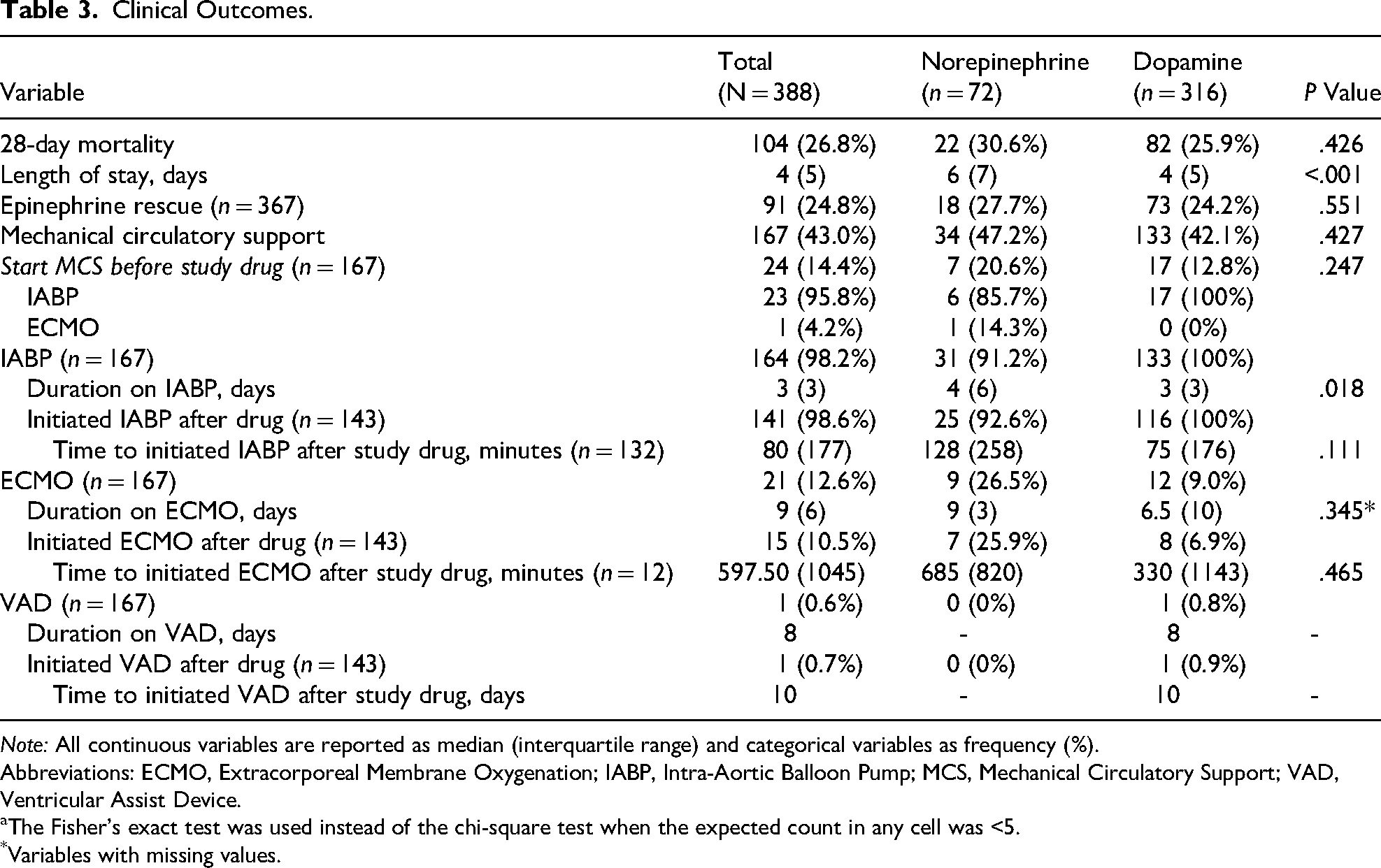
Note: All continuous variables are reported as median (interquartile range) and categorical variables as frequency (%).
Abbreviations: ECMO, Extracorporeal Membrane Oxygenation; IABP, Intra-Aortic Balloon Pump; MCS, Mechanical Circulatory Support; VAD, Ventricular Assist Device.
The Fisher's exact test was used instead of the chi-square test when the expected count in any cell was <5.
Variables with missing values.
Association Between Dopamine Versus Norepinephrine and 28-Day Mortality Across Analytical Approaches.
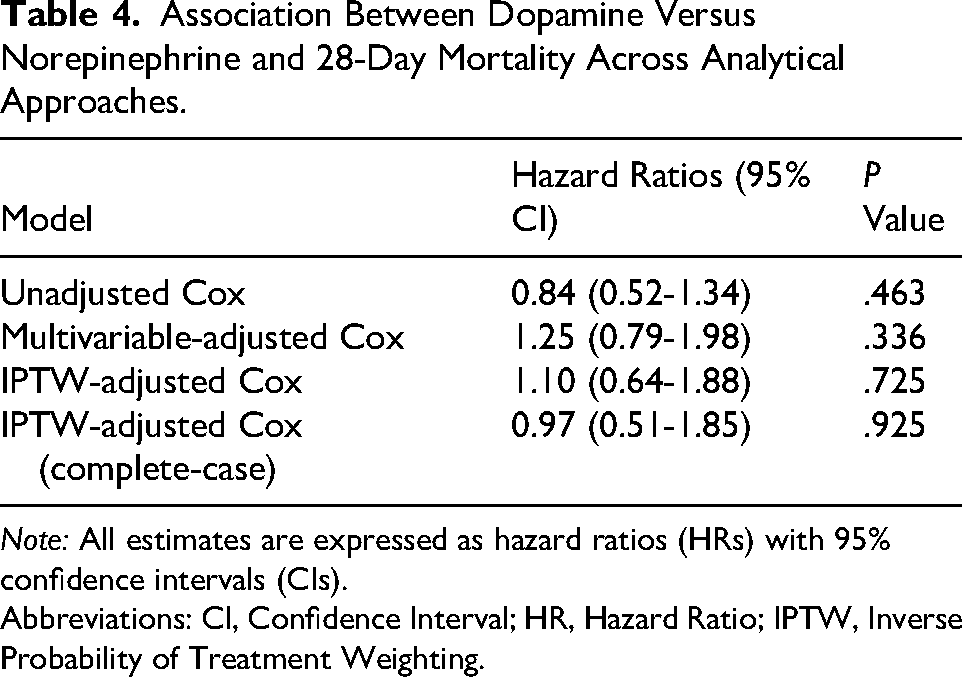
Note: All estimates are expressed as hazard ratios (HRs) with 95% confidence intervals (CIs).
Abbreviations: CI, Confidence Interval; HR, Hazard Ratio; IPTW, Inverse Probability of Treatment Weighting.
Propensity Score Weighting
To further address confounding by indication, stabilized inverse probability of treatment weighting (IPTW) based on propensity scores was applied. Missing baseline values, including lactate, LVEF, and mean arterial pressure, were handled using multiple imputation by chained equations under the missing-at-random assumption. The propensity score model was estimated using multivariable logistic regression incorporating age ≥65 years, cardiopulmonary resuscitation, endotracheal intubation, renal replacement therapy, mechanical circulatory support, lactate ≥2 mmol/L, LVEF <40% at the time of diagnosis, dobutamine use, and epinephrine use. The propensity score model demonstrated moderate discrimination (C-statistic 0.70, 95% CI 0.63-0.77); model adequacy was primarily assessed through postweighting covariate balance, consistent with established IPTW practice. After applying stabilized IPTW, all nine covariates achieved absolute SMDs <0.10, confirming adequate balance in the weighted pseudo-population (Supplementary S2-S3). In the IPTW-adjusted Cox proportional hazards model, dopamine was not significantly associated with 28-day mortality compared with norepinephrine (IPTW-adjusted HR 1.10, 95% CI 0.64-1.88; P = .725) (Table 4 and Figure 3).

IPTW-adjusted Kaplan–Meier survival curves.
Sensitivity Analysis
As a sensitivity analysis, the IPTW-adjusted Cox proportional hazards model was repeated using complete-case data restricted to the 192 patients with available baseline lactate and LVEF measurements. The propensity score model in this subset achieved adequate covariate balance after weighting (all SMDs <0.10) (Supplementary S4). Results were consistent with the primary analysis (IPTW-adjusted HR 0.97, 95% CI 0.51-1.85; P = .925) (Table 4 and Supplementary S5).
Predictors of 28-Day Mortality
On univariable analysis, the following factors were significantly associated with 28-day mortality: age ≥65 years (OR 1.99, 95% CI 1.26-3.14; P = .003), cardiopulmonary resuscitation (OR 8.63, 95% CI 5.11-14.57; P < .001), endotracheal intubation (OR 9.25, 95% CI 5.09-16.79; P < .001), renal replacement therapy (OR 4.98, 95% CI 2.93-8.47; P < .001), mechanical circulatory support (OR 1.82, 95% CI 1.16-2.86; P = .010), lactate ≥2 mmol/L (OR 4.58, 95% CI 2.28-9.19; P < .001), LVEF <40% at the time of diagnosis (OR 1.89, 95% CI 1.19-3.00; P = .007), dobutamine use (OR 1.50, 95% CI 0.93-2.44; P = .099), and epinephrine use (OR 8.40, 95% CI 5.07-13.93; P < .001).
On multivariable analysis, age ≥65 years (OR 3.05, 95% CI 1.68-5.57; P < .001), cardiopulmonary resuscitation (OR 3.59, 95% CI 1.90-6.77; P < .001), endotracheal intubation (OR 2.98, 95% CI 1.44-6.20; P = .003), renal replacement therapy (OR 2.68, 95% CI 1.41-5.10; P = .003), and epinephrine use (OR 3.55, 95% CI 1.83-6.87; P < .001) remained independent predictors of 28-day mortality. Other variables, including mechanical circulatory support, diabetes mellitus, hypertension, obesity, multivessel coronary artery disease (≥2 vessels), elevated systemic vascular resistance (>1600 dynes-sec/cm5), lactate ≥2 mmol/L, LVEF <40% at the time of diagnosis, and dobutamine use, were not independently associated with mortality after multivariable adjustment (Table 5).
Univariable Analysis and Multivariable Analysis for Predictors of 28-Day Mortality in Patients With Cardiogenic Shock.
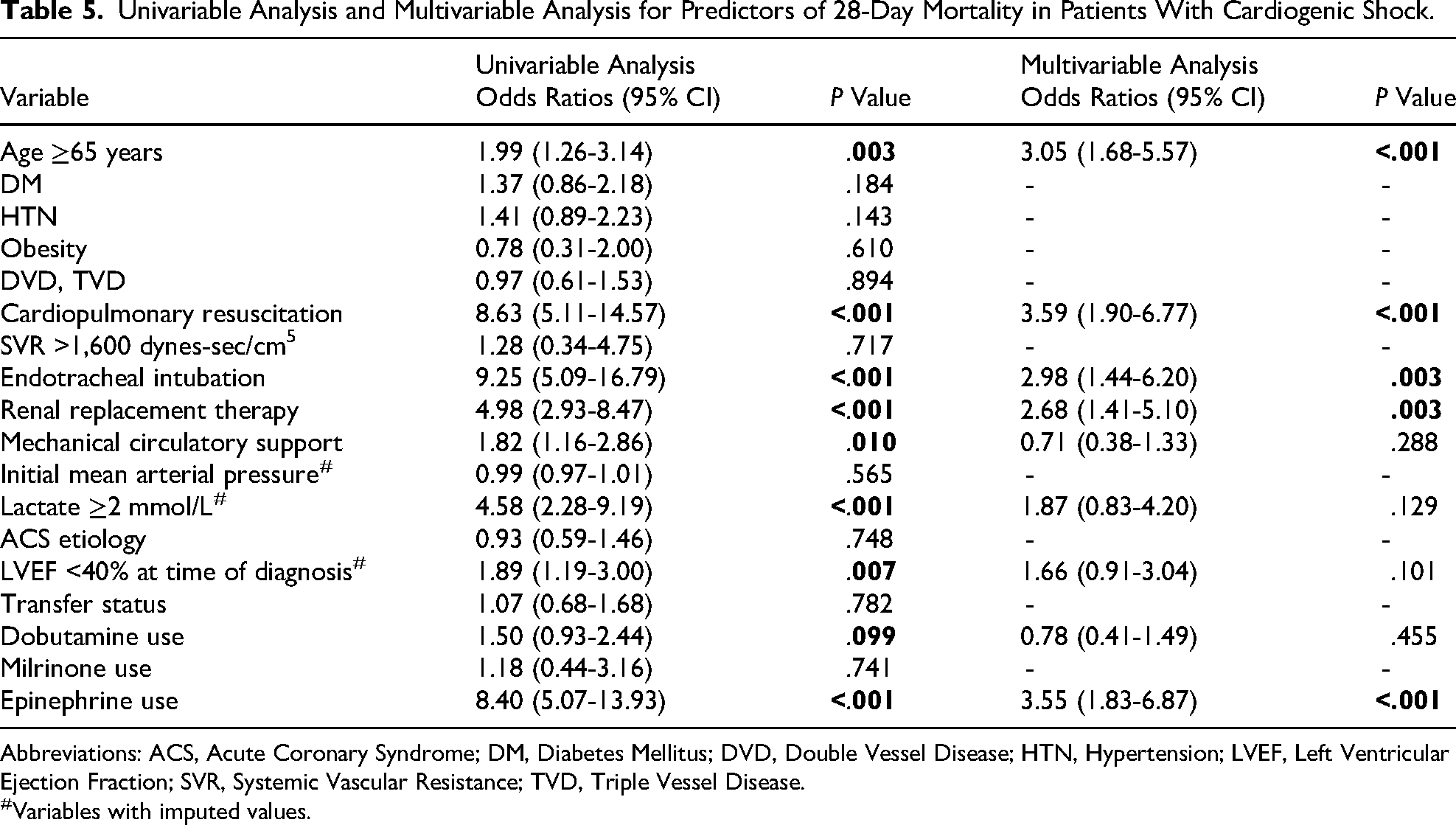
Abbreviations: ACS, Acute Coronary Syndrome; DM, Diabetes Mellitus; DVD, Double Vessel Disease; HTN, Hypertension; LVEF, Left Ventricular Ejection Fraction; SVR, Systemic Vascular Resistance; TVD, Triple Vessel Disease.
Variables with imputed values.
Hemodynamic Parameters
Among patients actively receiving vasopressor therapy, norepinephrine doses showed a gradual increasing trend, rising from 0.11 mcg/kg/min (SD 0.24) at H0 to 0.41 mcg/kg/min (SD 0.23) at H72; however, the number of patients remaining on norepinephrine declined markedly from 71 at H0 to only 3 at H72, and therefore the H72 estimate should be interpreted with considerable caution. Dopamine doses followed a different pattern, with the highest mean dose recorded at H6 (8.58 mcg/kg/min, SD 5.69), declining to a nadir at H48 (6.94 mcg/kg/min, SD 5.25), before rising again at H72 (8.46 mcg/kg/min, SD 5.86), with the number of patients on dopamine declining from 314 at H0 to 35 at H72. No formal statistical comparison between groups was performed, as the two agents differ substantially in dosing units and pharmacological profiles; descriptive data are presented in Supplement S7, and dose trajectories based on model-estimated means (± SE) are shown graphically in Supplement S6. Overall, the median maximum dose was 0.3 mcg/kg/min for norepinephrine and 11.5 mcg/kg/min for dopamine, with a median treatment duration of 2 days for both agents.
Mean Arterial Pressure
Mean arterial pressure (MAP) trajectories over 72 h were similar between the norepinephrine and dopamine groups. Mixed-effects analysis showed no significant treatment-by-time interaction (P for interaction = .968). MAP increased significantly from baseline to 6 h in both groups and remained stable thereafter. No significant between-group differences in MAP were observed at any time point, including baseline (all P > .05) (Supplement S8).
Heart Rate
Heart rate trajectories over 72 h differed significantly between the norepinephrine and dopamine groups (P for interaction <.001). At baseline, patients receiving norepinephrine had a significantly higher mean heart rate than those receiving dopamine (94.6 beats/min [95% CI 89.3-99.9] vs 75.0 beats/min [95% CI 72.5-77.5]; P < .001). Within the norepinephrine group, heart rate did not change significantly over the 72-h observation period. In contrast, heart rate in the dopamine group decreased significantly from baseline to 6 h and remained stable thereafter. Despite the higher baseline heart rate in the norepinephrine group, no statistically significant between-group differences in heart rate were observed at 6, 12, 24, 48, or 72 h after treatment initiation (all P > .05), although a numerical difference persisted throughout the observation period (Supplement S9).
Epinephrine Rescue Therapy
Epinephrine rescue therapy, administered when norepinephrine or dopamine failed to maintain hemodynamic stability, was required in 91 of 367 patients (24.8%), with comparable rates between the norepinephrine and dopamine groups (27.7% vs 24.2%; OR 0.83, 95% CI 0.46-1.52; P = .551). Of the 388 patients, 21 (5.4%) had initiated epinephrine prior to study vasopressor initiation and were therefore excluded from the rescue analysis (Table 3).
Among all 388 patients, 112 (28.9%) received epinephrine at any point during the treatment course, including for cardiopulmonary resuscitation, with no significant difference between groups (34.7% vs 27.5%; P = .224). Median epinephrine duration was 2 days in both groups (P = .708). However, the maximum epinephrine dose was significantly higher in the dopamine group (0.75 (IQR 0.95) versus 0.35 (IQR 0.70) mcg/kg/min; P = .019) (Supplement S10).
Safety Outcomes
Arrhythmias occurred in 96 patients (24.7%), with a significantly higher incidence in the dopamine group than in the norepinephrine group (28.2% vs 9.7%; P = .001). Atrial fibrillation and ventricular tachycardia were each significantly more frequent with dopamine (11.7% vs 2.8%; P = .027, and 21.2% vs 6.9%; P = .005, respectively), with nonsustained ventricular tachycardia (including short-run) being the most prevalent subtype. Ventricular fibrillation occurred in only three patients (0.8%), all of whom were in the dopamine group. Among patients who developed arrhythmias, amiodarone was the most frequently used antiarrhythmic agent (49%), with no significant difference between groups (P = .436).
Baseline serum potassium was comparable between groups (norepinephrine 4.00 [IQR 0.82] vs dopamine 3.90 [IQR 0.80] mmol/L; P = .765; n = 353). However, baseline serum magnesium was significantly higher in the norepinephrine group than in the dopamine group (0.98 [IQR 0.41] vs 0.86 [IQR 0.23] mmol/L; P = .011; n = 293) (Table 6).
Safety Outcomes.
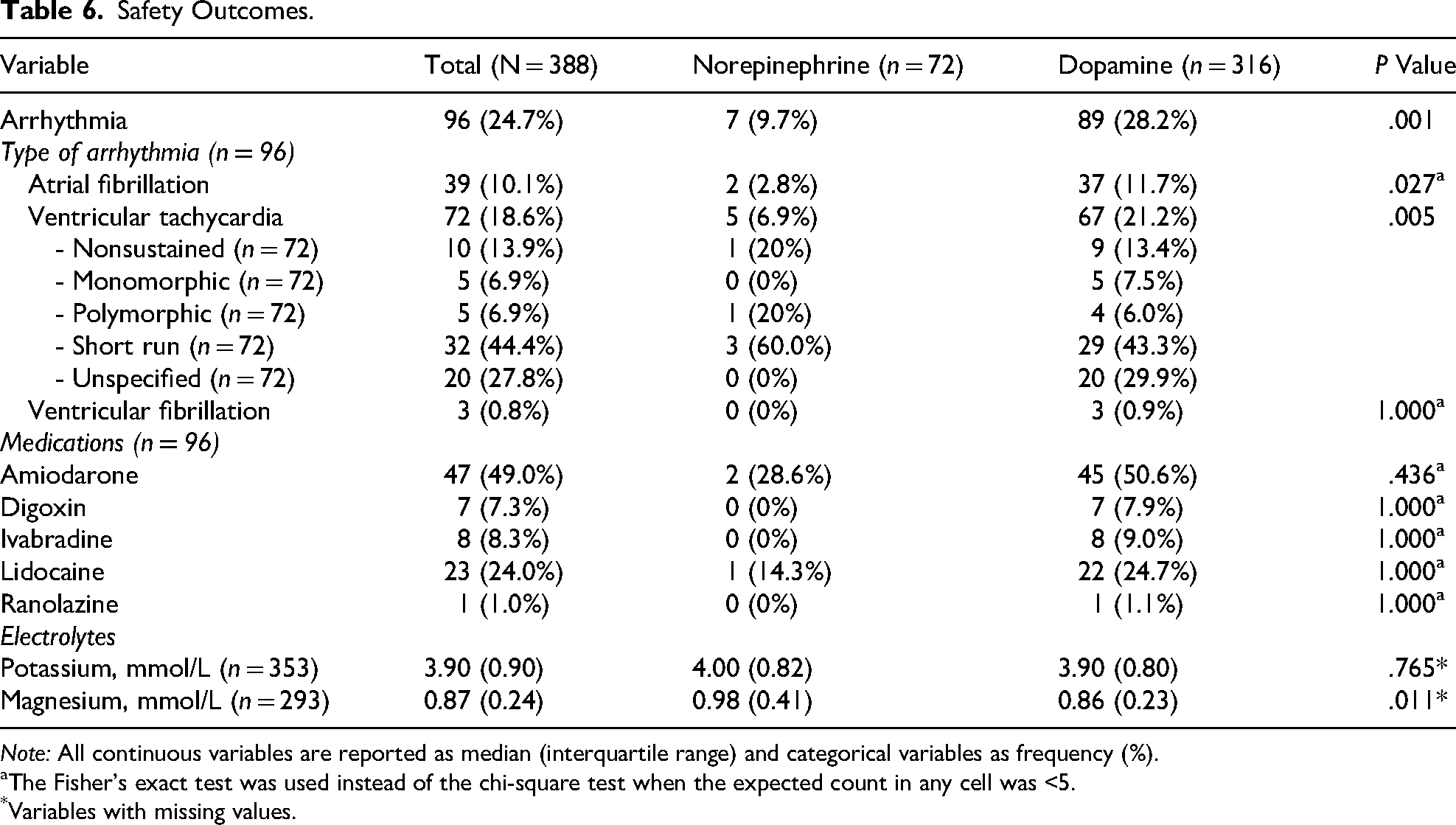
Note: All continuous variables are reported as median (interquartile range) and categorical variables as frequency (%).
The Fisher's exact test was used instead of the chi-square test when the expected count in any cell was <5.
Variables with missing values.
Post Hoc Subgroup Analyses
In post hoc subgroup analyses, the association between vasoactive agent type and 28-day mortality was generally consistent across clinically relevant subgroups, with no statistically significant effect modification by prior cardiopulmonary resuscitation or mechanical circulatory support. However, a significant treatment-by-etiology interaction was identified when patients were stratified by shock etiology (P for interaction = .002). Among patients with ACS-related cardiogenic shock (n = 229), 28-day mortality did not differ significantly between the dopamine and norepinephrine groups (IPTW-adjusted HR 0.53, 95% CI 0.27-1.04; P = .064). In contrast, among patients with non-ACS cardiogenic shock (n = 159), dopamine use was associated with significantly higher 28-day mortality compared with norepinephrine (IPTW-adjusted HR 2.89, 95% CI 1.26-6.62; P = .012) (Figure 4).

Post hoc subgroup analyses.
Discussion
This study examined the clinical outcomes associated with norepinephrine and dopamine as initial vasoactive therapy in patients with cardiogenic shock. In the predefined cardiogenic shock subgroup (n = 280) of the SOAP II trial, a multicenter randomized study by De Backer et al., norepinephrine was associated with a lower 28-day mortality rate than dopamine. However, dopamine was associated with a higher risk of arrhythmias. 10 In contrast, the present study, which included only patients with cardiogenic shock, observed no statistically significant difference in 28-day mortality between those receiving norepinephrine and those receiving dopamine. Of note, the unadjusted Cox model suggested a lower mortality risk with dopamine (HR 0.84, 95% CI 0.52-1.34), whereas both the multivariable-adjusted and IPTW-adjusted models yielded HRs in the opposite direction (1.25 and 1.10, respectively). This reversal is consistent with confounding by indication, as norepinephrine was preferentially prescribed to more severely ill patients, as evidenced by significantly higher rates of cardiopulmonary resuscitation, endotracheal intubation, renal replacement therapy, higher baseline lactate levels, and a higher rate of dobutamine use in the norepinephrine group. Consistent with greater illness severity, the norepinephrine group also had a significantly longer hospital stay (6 vs 4 days; P < .001), likely reflecting prolonged mechanical circulatory support requirements, including longer IABP (4 vs 3 days) and ECMO support (9 vs 6.5 days). The unadjusted estimate may therefore reflect baseline imbalance rather than a true pharmacological difference between agents. Baseline imbalance and confounding by indication are inherent limitations of observational studies. To address these sources of bias, stabilized IPTW was applied. Covariate balance improved substantially after weighting, with all nine covariates achieving absolute SMDs <0.10, indicating adequate balance in the weighted pseudo-population. The sensitivity analysis, restricted to patients with available lactate and LVEF measurements (n = 192), yielded an IPTW-adjusted HR of 0.97 (95% CI 0.51-1.85; P = .925), consistent with the primary analysis and without a statistically significant difference.
Dopamine use was associated with a significantly higher incidence of atrial fibrillation and ventricular tachycardia, consistent with its dose-dependent receptor activity. At intermediate doses of 3–10 mcg/kg/min, dopamine agonizes β1-adrenergic receptors and promotes norepinephrine release by inhibiting its reuptake at presynaptic nerve terminals, 8 which may increase myocardial excitability and trigger arrhythmias. At higher doses exceeding 10 mcg/kg/min, α1-adrenergic receptor stimulation predominates, producing vasoconstriction and increased systemic vascular resistance, effects that parallel those of norepinephrine. 8 In the present study, the mean dopamine dose at H6 was 8.58 mcg/kg/min, placing most patients within the β1-dominant range, while the median maximum dose of 11.5 mcg/kg/min—consistent with the mean maintenance dose of approximately 9 mcg/kg/min reported in surviving patients with cardiogenic shock by Karliner et al 11 —suggests that a substantial proportion were also exposed to high-dose dopamine at some point during their treatment course. Since arrhythmia onset was not recorded relative to specific dose levels, a direct relationship between dose range and arrhythmia incidence cannot be established from the present data. Nevertheless, the overall dopamine exposure pattern is consistent with a pharmacological profile with higher arrhythmogenic potential than norepinephrine.
The higher arrhythmia burden observed with dopamine is likely due to a combination of factors. Although baseline serum magnesium was significantly lower in the dopamine group (0.86 vs 0.98 mmol/L; P = .011), both values fell within the normal reference range, and the clinical significance of this difference in the context of arrhythmia risk remains uncertain. Among patients who received epinephrine or dobutamine, those in the dopamine group received significantly higher maximum doses of both epinephrine (0.75 vs 0.35 mcg/kg/min; P = .019) and dobutamine (10.0 vs 5.50 mcg/kg/min; P = .006) (Supplement S10), which independently carry arrhythmogenic potential. This is consistent with findings from a randomized pilot study by Levy et al, in which patients who switched from dopamine–dobutamine therapy to epinephrine experienced new supraventricular arrhythmias, sustained ventricular tachycardia, and transient lactic acidosis, whereas those receiving norepinephrine–dobutamine had fewer arrhythmic complications, 12 further supporting the role of concomitant vasoactive agent selection in determining arrhythmia risk. In contrast, dobutamine and levosimendan were more frequently used in combination with norepinephrine in the present study, potentially augmenting inotropic and vasodilatory effects through β1-adrenergic stimulation and calcium sensitization, respectively. 8 The elevated baseline heart rate in the norepinephrine group more likely reflects greater illness severity at the time of vasopressor initiation rather than a drug-mediated effect, and is therefore unlikely to account for the higher arrhythmia incidence observed with dopamine. Residual confounding, however, cannot be fully excluded.
The most common etiology of cardiogenic shock in the present cohort was acute coronary syndrome, accounting for 59% of cases, of which 78.2% were due to STEMI. Among patients with ACS-related cardiogenic shock, 28-day mortality did not differ significantly between groups (IPTW-adjusted HR 0.53, 95% CI 0.27-1.04; P = .064), whereas dopamine was associated with significantly higher 28-day mortality in the non-ACS subgroup (IPTW-adjusted HR 2.89, 95% CI 1.26-6.62; P = .012). This different effect may reflect dopamine's chronotropic and arrhythmogenic properties, which could contribute to worse outcomes in non-ACS etiologies characterized by pre-existing electrical instability. These results are hypothesis-generating and warrant prospective validation. However, several limitations of this subgroup analysis should be acknowledged. Within the non-ACS subgroup, dopamine was used by 74.2% of patients (n = 118 of 159), resulting in a substantially smaller norepinephrine group for comparison. This disproportion may limit the reliability of IPTW estimation within this subgroup. Furthermore, the non-ACS group comprised diverse etiologies, including acute decompensated heart failure, arrhythmia-related shock, and valvular heart disease, and the observed findings may not apply equally to each individual etiology. Regarding epinephrine rescue, the OptimaCC trial reported comparable hemodynamic effects between epinephrine and norepinephrine in ACS-related cardiogenic shock, though norepinephrine was favored owing to a lower incidence of refractory shock. 13
Mechanical circulatory support was used by 43% of patients in the present study, with IABP being the most commonly used device. The IABP-SHOCK II trial reported no significant reduction in 30-day mortality with IABP in patients with cardiogenic shock complicating acute myocardial infarction treated with early revascularisation. 14 Furthermore, 21 of 388 patients in the present study received ECMO support, with significantly higher use in the norepinephrine group. Similarly, the ECLS-SHOCK trial reported no mortality benefit of ECMO over medical therapy in patients with acute myocardial infarction and cardiogenic shock undergoing early revascularisation. 15 MCS use was therefore considered unlikely to have substantially confounded the primary mortality findings.
A meta-analysis by Rui Qing et al, encompassing 7 studies, reported lower 28-day mortality (P < .001) and fewer arrhythmic events (P < .001) among patients receiving norepinephrine. 16 However, the present study observed no significant difference in 28-day mortality between the two agents, consistent with the retrospective study by Na SJ et al, which included 520 patients with cardiogenic shock treated with either dopamine or norepinephrine. That study also found no mortality difference but reported a greater need for additional vasoactive agents in the dopamine group, with norepinephrine as the most common second agent (93.5%). 17
Multivariable analysis identified age ≥65 years, cardiopulmonary resuscitation, endotracheal intubation, renal replacement therapy, and epinephrine use as independent predictors of 28-day mortality. These factors collectively reflect disease severity and the extent of organ failure at presentation. Epinephrine use in this analysis captured administration at any point during the admission, including for cardiopulmonary resuscitation, and therefore likely reflects overall hemodynamic instability and illness severity rather than a direct pharmacological effect of epinephrine. Lactate was additionally included as a covariate given its established prognostic role in cardiogenic shock; a pooled analysis by Zeymer et al reported that higher arterial lactate levels were associated with 30-day and 1-year mortality regardless of shock status, supporting its inclusion in the multivariable model. 18
Although no statistically significant difference in 28-day mortality was observed between groups, the higher arrhythmia burden with dopamine is consistent with its established pharmacological profile and with current guideline recommendations favoring norepinephrine in cardiogenic shock. These findings contribute real-world evidence from a contemporary tertiary care center in Thailand. The large sample size, comprehensive clinical data, and consistency with prior randomized evidence support the validity of the present findings; multicenter prospective studies are warranted to further evaluate optimal vasoactive agent strategies in cardiogenic shock.
Limitations
Several limitations should be acknowledged. This was a single-center retrospective study, which may introduce selection bias and limit causal interpretation despite multivariable adjustment and IPTW. Treatment allocation likely reflected clinician judgment and underlying shock phenotype, factors that cannot be fully captured despite IPTW adjustment. The choice of vasopressor and dosing was at clinicians’ discretion, and approximately 40% of patients were transferred from other hospitals, which may have influenced early outcomes. Only 28-day mortality was evaluated, and invasive hemodynamic data were available only for a limited subset.
Although the propensity score model incorporated nine covariates (c-statistic 0.70), residual confounding from unmeasured variables cannot be excluded. Baseline lactate and LVEF were missing in 42.8% and 15.5% of patients, respectively, likely reflecting selective measurement in more critically ill individuals. Multiple imputations under the missing-at-random assumption were applied; however, residual bias from informative missingness cannot be fully excluded. Furthermore, a single imputed dataset was used for propensity score estimation and inverse probability of treatment weighting, potentially underestimating the uncertainty attributable to missing data.
The complete case sensitivity analysis was restricted to the 192 patients with available lactate and LVEF measurements. These patients were systematically more severely ill than the remaining 196 patients with missing data, with notably higher rates of endotracheal intubation (70.3% vs 33.2%), renal replacement therapy (28.7% vs 10.7%), epinephrine use (38.5% vs 19.4%), and mechanical circulatory support (52.1% vs 34.2%). This case-mix difference may have influenced propensity score estimation within the complete-case subset and contributed to the modest reversal in point estimate observed in the sensitivity analysis. Overall mortality did not differ significantly between patients with and without complete data (26.6% vs 27.0%; P = .915), which supports, but does not confirm, the missing-at-random assumption.
Finally, concomitant vasoactive agent use could not be fully incorporated into the primary model, and as arrhythmia onset was not recorded relative to specific dose levels, a direct relationship between dopamine dose and arrhythmia incidence cannot be established. Arrhythmia ascertainment relied on physician-documented diagnoses and telemetry records rather than systematic prospective adjudication; transient self-terminating events may therefore have been under-reported. Nevertheless, given that all patients were monitored under identical CCU/ICCU protocols, differential under-ascertainment between groups is unlikely.
Conclusion
In this retrospective cohort study, dopamine and norepinephrine did not demonstrate a statistically significant difference in 28-day mortality in patients with cardiogenic shock. However, dopamine was associated with a significantly higher incidence of arrhythmias. Independent predictors of 28-day mortality included endotracheal intubation, renal replacement therapy, cardiopulmonary resuscitation, epinephrine use, and age ≥65 years, underscoring that prognosis in cardiogenic shock is primarily driven by illness severity and organ dysfunction at presentation.
Supplemental Material
sj-docx-1-cpt-10.1177_10742484261456161 - Supplemental material for Norepinephrine Versus Dopamine as Vasoactive Therapy in Cardiogenic Shock: Association With 28-Day Mortality in a Retrospective Cohort Study
Supplemental material, sj-docx-1-cpt-10.1177_10742484261456161 for Norepinephrine Versus Dopamine as Vasoactive Therapy in Cardiogenic Shock: Association With 28-Day Mortality in a Retrospective Cohort Study by Suthida Chanchenchop, PharmD, Supanee Sinphurmsukskul, MD, and Krittin Bunditanukul, PharmD, PhD, BCPS in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Author Contributions
SC and KB: conceptualization. SC: methodology. SC: investigation. SC: resources. SC: data curation. SC: formal analysis. KB and SS: project administration. KB and SS: supervision. KB: validation. SC and KB: visualization. SC: writing—original draft. KB and SS: writing—review and editing. All authors approved the final version of the manuscript.
Funding
The Ajarn Kasem Pangsriwong Foundation funded this study. The funder had no role in the study design, data collection, data analysis, interpretation of the results, or manuscript writing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.