
Abstract
According to research, as many as 68% of students have experienced at least some form of trauma (Cavanaugh, 2016). Yet, most educators report feeling inadequate about understanding trauma-informed practice, including understanding how trauma can impact student behavior in the classroom. This article provides a primer about trauma that can allow educators to unpack the definition, understanding, identification, and the impact traumatic experiences can have on students in today’s schools.
Ashra is a third-grade student identified as having an emotional and behavioral disorder who recently moved to Bishop Elementary School. Before Ashra’s first day at Bishop, the school social worker, Mrs. Baskin, received a phone call from a school professional at Ashra’s previous school to update her on Ashra’s needs. The school professional shared that through talking with Ashra, her mother, and direct observations of Ashra during the school day, they were able to successfully reduce her challenging behaviors through a behavior intervention plan (BIP) that addressed her emotional outbursts which included yelling at her teacher or other students, throwing items such as pencils or crayons, and leaving the classroom without permission that manifested from chronic trauma.
Mrs. Baskin learned about the complex trauma Ashra experienced due to years of domestic violence exposure in the home. Ashra’s father was recently found guilty and sentenced to time in prison for physically and sexually abusing Ashra and her siblings. The children in the home also frequently witnessed Ashra’s father’s explosive temper that included tearing apart the house while screaming obscenities and emotionally abusive slurs toward Ashra’s mother.
Mrs. Baskin also learned that Ashra and her siblings had at one time lived in several shelters and a car with their mother when they left Ashra’s abusive father. The family experienced homelessness, poverty, and exposure to drug use through both parents who frequently used illicit drugs. Mrs. Baskin had worked with students who experienced trauma in the past, and she knew this was information that would be important for Ashra’s new teachers to know, including understanding how Ashra’s previous trauma might impact her academic, behavioral, and social performance in school.
Ashra is one of thousands of students in the United States who show up to learn in schools every day and struggle with trauma they have or continue to experience. Approximately 20% of youth, or the equivalent of six pupils in every U.S. classroom, have experienced trauma (Spence et al., 2021). Meanwhile, nearly half of all U.S. children in today’s schools have reported at least one adverse childhood experience (ACE; Brown et al., 2020). Approximately 10% of those children report three or more ACEs.
Adverse childhood experiences describe types of abuse, neglect, and other childhood experiences that are potentially traumatic experiences or environments that can lead to long-term physical and mental health challenges and can negatively impact the overall well-being for the individual involved (Sciaraffa et al., 2018; Van der Kolk, 2014). Adverse childhood experiences consist of seven different categories: psychological, physical, or sexual abuse, exposure to substance abuse, mental illness, witnessing violent treatment of parent, and criminal behavior (Felitti et al., 1998). According to the U.S. Centers for Disease Control and Prevention (CDC, 2019), at least two-thirds of adults surveyed reported experiencing at least one ACE during childhood. More than one in five adults reported experiencing three or more ACEs during childhood (Jennings, 2019).
Common across all race and ethnicity groups, ACEs are somewhat disproportionately lower for White, non-Hispanic children and lowest for Asian children. Over six in 10 Black children have ACEs, representing 17.4% of all children in the United States (Bethell et al., 2017). Adverse childhood experiences are also often associated with social, emotional, and cognitive impairments; engaging in high-risk behaviors; disabilities; and social problems (Cavanaugh, 2016).
Empirical research has consistently linked ACEs with negative health outcomes and a range of mental health difficulties through the lifespan (Pataky et al., 2019). For example, beginning early in life, ACEs can negatively impact the development of biological regulatory systems and may even lead to an increase in a person’s physiological and reactive response to stressors (Sheffler et al., 2019). Consequently, students who have experienced ACEs are often in great need of developing the social–emotional knowledge required to process their traumas and the necessary skills to address any potential challenges or triggers that are associated with childhood traumas. Because neurobiological research indicates that exposure to repeated and chronic trauma can negatively impact the brain, it is common for students to have trouble accessing higher order cognitive processes, which are critical to learning, social, and emotional regulation (Brown et al., 2020).
Despite such a large population of students with a history of trauma in today’s classrooms, when it comes to supporting such students, most teachers report feeling inexperienced. Reinke et al. (2011) conducted a survey and found that 75% of teachers agreed that schools should be involved in addressing the mental health needs of students. Yet only 34% of those teachers felt as if they had the necessary skills to address those concerns.
To retain quality educators, it is necessary to provide them with the knowledge, skills, and resources needed to effectively understand and address student needs related to trauma. Specifically, it is important to provide educators with a better understanding of possible unseen reasons behind student problem behavior linked with a history of trauma. Consequently, the purpose of this article is to (a) provide a foundational knowledge on trauma for educators in schools, (b) identify how trauma can affect brain development and processing, (c) recognize student challenging behaviors that may stem from a history of trauma, and (d) identify universal and targeted trauma-informed practices. We want educators to be aware of trauma considerations when advocating for students’ needs.
Understanding Trauma
The American Psychological Association (APA, 2015) defines trauma as “an emotional response to a terrible event.” The most common types of trauma experienced by students in schools include physical or sexual abuse, emotional and physical neglect, and witnessing or experiencing domestic violence. Of these traumatic events, physical abuse has the highest prevalence rate (28.3%). Other prevalence rates include sexual abuse (20.7%), emotional neglect (14.8%), physical neglect (9.9%), and domestic violence (12.7%) (Cavanaugh, 2016). Furthermore, child abuse and neglect, also referred to as child maltreatment, is identified as one of the country’s most serious problems (Chitiyo & Pietrantoni, 2019).
In such cases, students are often perpetrated by parents, primary caregivers, or close family members. Thus, these students are likely to experience ongoing traumatization because they lack the social and emotional support that is needed to cope and be removed from such abuse (Chitiyo & Pietrantoni, 2019). Meanwhile, less known events can also be linked with trauma, including the sudden and unexpected loss of a loved one, natural disasters (e.g., hurricanes, tornadoes, earthquakes), or man-made disasters, such as war or domestic and international terrorism (Cavanaugh, 2016), and even the global COVID-19 pandemic.
Indeed, exposure to aversive events can lead to trauma. However, the impact of the event leading to experiencing trauma lies within the perspective of the individual. In other words, not all ACEs are perceived by individuals as traumatic. According to Black et al. (2012), for an event to be labeled as traumatic, the events should be perceived by the individual as aversive, terrifying, shocking, sudden, or potentially pose a threat to one’s safety or personal integrity. Consequently, teachers cannot assume all students will respond similarly to all events.
To better explain this phenomenon, consider the example of how two brothers, both of whom experienced a traumatic event together, manifested the aversive incident differently. Jordan and Jaden both experienced a house fire that resulted in the loss of their home and belongings. The fire occurred while the boys and their parents were asleep. The family woke up to the fire alarm beeping. The boys were able to crawl out the window, along with their family, to find safety outside. Fortunately, no family members were injured, but the family did lose all belongings and their home. Even after 2 years, the parents shared with his teacher that Jordan still had nightmares about the house fire and often experienced insomnia.
Jordan’s dreams consisted of re-experiencing the awful events of that night. At times, Jordan suddenly woke up believing he heard the fire alarm beeping. This caused him to panic and begin crying for his mom. Meanwhile, Jaden did not display any signs of stress regarding the night of the fire and did not display any behaviors that were connected to re-experiencing the events of that night. In fact, even if the fire alarm in the house beeped, Jaden simply covered his ears due to the loud noise without crying or displaying panic. In this example, both brothers experienced and processed the house fire differently.
Types of Traumas Observed in Schools
It is estimated that about 30% of U.S. students with emotional and behavioral disorders have experienced trauma or show signs of post-traumatic stress disorder (PTSD; Cavanaugh, 2016). Consequently, negative outcomes for these students can include social challenges, emotional and cognitive impairments, and high-risk behaviors. Meanwhile, students with intellectual and developmental disabilities (IDDs) are 4.3 times more likely to experience trauma from maltreatment than students without disabilities, and they are at a greater risk for other potentially traumatic experiences, such as sexual, physical, and emotional abuse (Keesler, 2020; Mevissen & de Jongh, 2010; Thomas-Skaf & Jenney, 2021).
There are several factors contributing to this statistic, including student deficits in language and an inability to provide verbal descriptions of their experiences and emotional states due to impairments in receptive and expressive language (Mevissen & de Jongh, 2010). Individuals with IDD, particularly those with autism, may also be at a greater risk for more intense stress responses to traumatic events because of their neurobiological differences (Keesler, 2020). These differences can also lead to more opportunities for the student to be victimized due to stigmas of being vulnerable. For example, a student with IDD can sometimes be perceived as more gullible or trusting of others (Thomas-Skaf & Jenney, 2021). It is also important to note that students with disabilities are at a greater risk for trauma due to abuse by caregivers. One reason for this risk is explained by an increase in caregiver strain because students with disabilities require more care than those without disabilities, which can lead to an increase in stress (Thomas-Skaf & Jenney, 2021).
Trauma can be experienced in multiple forms. Table 1lists and describes the following types: secondary, acute, chronic, complex, developmental, secondary, and collective trauma. Acute trauma is described as a short-term, unexpected, single incident (Keller-Dupree, 2013). Examples of acute trauma may include experiencing an automobile accident, the sudden loss of a family member, or survival of a natural disaster event, such as a tornado. In a school setting, acute trauma can also include the seclusion and/or restraint of a student, school violence, such as shootings, or even the unexpected loss of a classmate.
Types of Trauma, Descriptions, and Possible Impacts.
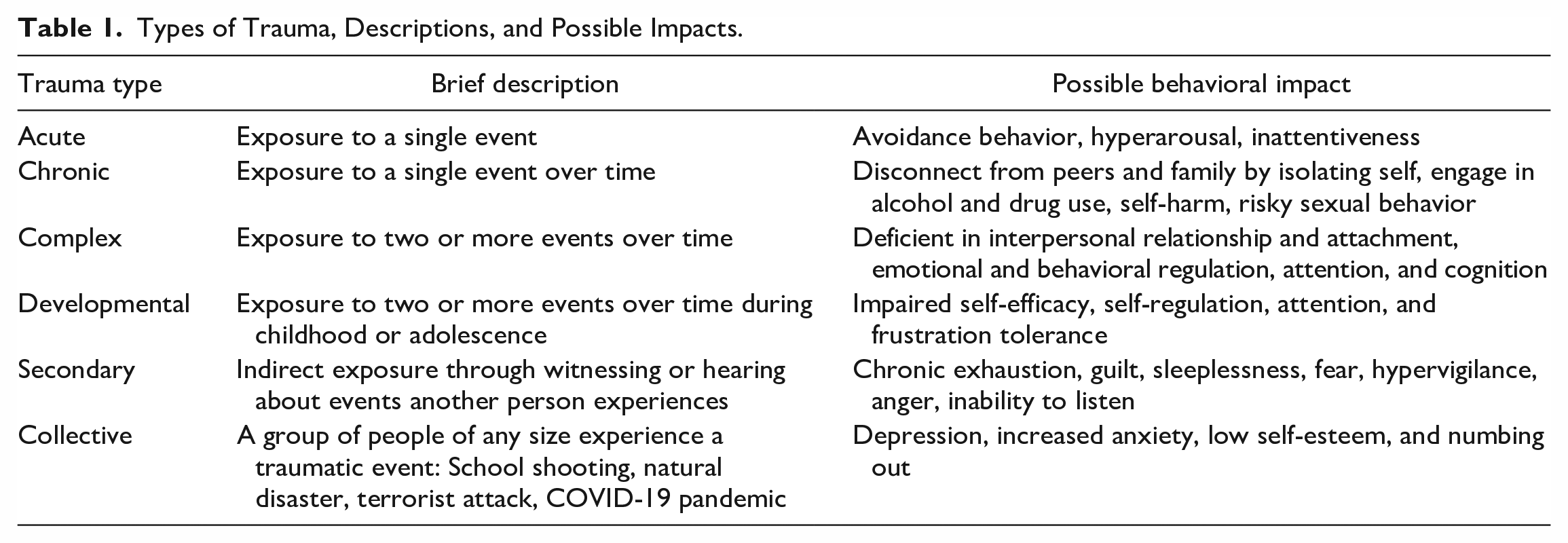
By contrast, chronic trauma includes repeated and prolonged exposure to traumatic incidents (Keller-Dupree, 2013), for example, a student who is continuously subjected to domestic violence in the home, including abuse, neglect, homelessness, or continuous starvation. In a chronic trauma situation, such aversive events occur more than once and over time, sometimes spanning years.
In addition to these types of traumas, when an individual is exposed to varied and repeated traumatic events, it is known as complex trauma (Deutsch et al., 2020). According to Kliethermes et al. (2014), complex trauma events include repetitive physical, sexual, or emotional abuse, neglect, witnessing domestic violence, exposure to community violence, and medical trauma that occurs over an extended time period. In the case of Ashra, she experienced complex trauma because she was repeatedly exposed to domestic violence and physical and emotional abuse.
Developmental trauma can be acute, complex, or chronic. The main criterion for developmental trauma is the effect the trauma has on the child’s developmental processes. This form of trauma can impact a child in several different areas, including—but not limited to—interference with peer relationships, social skills, school success, and a sense of self (Deutsch et al., 2020). During the developmental years of childhood, such chronic childhood traumatic stress can also have profound consequences on attachment, emotional, and behavioral regulation, and cognition and learning (Brown et al., 2020).
Meanwhile secondary trauma, also referred to as vicarious trauma, includes traumatic stresses found to impact those who have indirectly experienced the traumatic event. This can include events, such as an individual witnessing a traumatic event (e.g., car accident), one who experiences the behaviors or emotions exhibited by the trauma survivor (e.g., consoling a victim crying in pain when triggered by memories of previous abuse, listening to a student share stories of physical abuse endured), or if the individual provides assistance to the survivor in the midst of trauma that results in similar stress reactions as the trauma survivor (e.g., rescuing a victim after a large tornado swept through the city; Wiest-Stevenson & Lee, 2016).
Notably, it is common for educators to experience secondary trauma. Teachers typically encounter students who have experienced trauma more so than most other professionals, such as therapists, because these students are often not diagnosed, identified, or treated. Because teachers work consistently and directly with students who have likely experienced trauma, they are more susceptible to developing secondary trauma. Secondary trauma can occur when responding to a students’ emotional and behavioral crisis, as well as hearing about trauma experienced by the student. Not surprisingly, this type of trauma contributes to reported emotional burden, stress, and anxiety among teachers (Christian-Brandt et al., 2020).
Finally, collective trauma includes instances where a group of people of any size experience a traumatic event at the same time, but not necessarily when they are directly together. Examples may include a school shooting, natural disaster (e.g., hurricane or earthquake), terrorist attack, or violent crime. The impact of the COVID-19 pandemic has created significant socioemotional and financial stress for many families across the country leading to a collective traumatic experience (Phelps & Sperry, 2020). Google searches were also another indicator of significant socioemotional stress as there was an increase in phrases, such as, “My mom beat me,” “My dad hit me,” and searches about how to report and identify child abuse (Bryant et al., 2020). This form or trauma may impact students, teachers, and families for years to come.
Trauma and Connection to PTSD
The greatest difference between trauma and PTSD, or even how trauma may lead to PTSD, lies within the responses or behaviors exhibited by the individual who experienced trauma. The Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev.; DSM-5-TR; APA, 2022) identified the primary symptoms of PTSD to include history of an identifiable traumatic event, re-experiencing of the trauma, avoidance of cues associated with the trauma or emotional numbing, and symptoms of increased arousal. Another criterion is experiencing stressors related to the traumatic events for more than 6 months that are disruptive to normal functioning. Therefore, trauma could be viewed as an event that can trigger PTSD.
Post-traumatic stress disorder can take various forms, including the spontaneous triggering of any unwanted images, flashbacks, nightmares, distress, and physiological reactions (Ehlers et al., 2004). The onset of these reactions can be triggered for many different reasons and are often activated through the five senses: hearing, seeing, smelling, touching, and tasting. This trigger could immediately take a student back to the emotional responses associated with the trauma. Examples may include but are not limited to (a) sounds, such as songs or outside noises, (b) sights, such as colors, physical features of a person, or external features, (c) smells like perfume or alcohol), (d) touch sensations, such as concrete or fabric, and (e) the tastes of certain foods or drinks. In some cases, a student may re-experience the emotions or sensations of the traumatic event without even being aware of them. This is further explained in the next section, which addresses how trauma impacts the brain.
The following is an example of PTSD in a student named Jonah who was in a head-on car collision that took his mother’s life when he was 5 years old. As a result of this trauma, Jonah developed PTSD. Directly before the accident, Jonah saw headlights of another car coming directly toward him and his mom. Three years later, Jonah continues to periodically re-experience seeing those headlights. At times it occurs even while sitting in his classroom when a bright classroom light is unexpectedly turned on. As a result, Jonah will run from the classroom to escape the vision of the headlights. Without having such background knowledge about Jonah, educators may limit their interpretation to why Jonah is leaving the classroom.
Because not all traumas are equal in their impact and can vary greatly in the amount of stress they impose on an individual (Agaibi & Wilson, 2005), not all trauma leads to the development of PTSD. In fact, Wiest-Stevenson and Lee (2016) reported that one in three children exposed to trauma exhibit symptoms of PTSD. Resilience has been named as a potential contributing factor for this low percentage of PTSD because it is related to one’s ability to self-regulate, cope with, and manage stressful situations (Sciaraffa et al., 2018).
According to Agaibi and Wilson (2005), resilience is described as having the ability to overcome large amounts of stressful events and is strongly associated with positive outcomes, fewer PTSD symptoms, and better overall health. There are a few protective factors that can result in a greater likelihood of resilience from experiencing trauma, including a healthy recovery from stress; curiosity and intellectual mastery; the ability to detach and conceptualize problems; and the intensity, duration, and frequency of traumatic events (Agaibi & Wilson, 2005). It is also important to note that positive teacher–child relationships, as well as the provision of a safe, predictable, and stimulating environment, can also build resilience for students who have experienced trauma (Sciaraffa et al., 2018). These protective factors are extremely important considerations, especially regarding the impact trauma can have on the brain.
Recognizing How Trauma Affects the Brain
When the brain is triggered by a threat or the perception of a threat that can be related to re-experiencing trauma, the autonomic nervous system (ANS), specifically the sympathetic nervous system (SNS), reacts by releasing chemicals into the body that allow individuals to “survive” those states of stress through “fight or flight” responses (Harris, 2021). When these chemicals are released in large doses, and over long periods of time, they can become toxic to the body and create significant impairment in a child’s development (Souers & Hall, 2016). In fact, preclinical and clinical studies have shown that alterations in memory function and changes in a circuit of brain areas can take place following a traumatic event that triggers stress responses (Bremner, 2006). By contrast, when individuals are under no threat, the parasympathetic nervous system (PNS) is in effect, often referred to as the “rest and digest” state (Harris, 2021). These ANS responses can be further explained through understanding how the brain responds to triggers that are related to trauma.
Neuroscientist Paul MacLean (1990) introduced the Triune brain, a model dividing the brain into three major structural parts, each presented sequentially according to the development of the area of the brain from the oldest to newest area (brain stem to prefrontal cortex). The oldest and lowest region of the brain located in the brain stem, often referred to as the reptilian or primitive brain, is responsible for basic human survival skills, including maintaining all physical functions, such as heart rate, breathing, sleeping, feeling pain, eating, drinking, and defecating.
Just above this region of the brain lies the limbic system, referred to as the emotional part of the brain, whereby individuals begin to interpret their experiences, interactions, and emotions within this area of the brain. This is also where the amygdala, often referred to as the body’s built-in “emergency alarm,” is housed. This area of the brain is responsible for receiving and delivering sensory input for anything that appears to be a threat, and it consequently leads to emotionally reacting to an event, including sometimes displaying a lack of behavioral control through verbal and physical aggression (Van der Kolk, 2014).
Essentially, when something is presented to an individual that is perceived as alarming, stressful, or threatening, the amygdala triggers the SNS into a “fight or flight” response as a form of protection (Bremner, 2006; Harris, 2021). During this stage, physical symptoms through the SNS include an increase in alertness, adrenaline, and heart rate; an agitated state; muscle stiffness; and the ability to take immediate physical action in response to stress (Harris, 2021).
Some individual students may even describe feeling an out-of-body experience referred to as disassociation, which is also described as a “freeze” response, whereby the SNS has become so overloaded with emotional responses that the individual is overwhelmed to a state of immobility and helplessness (Van der Kolk, 2014). Greene (2014) further describes this phenomenon as “vapor lock,” likening an individual who is at this stage (fight, flight, or freeze) to an overheated car that is incapable of any intervention beyond allowing it to simply “cool down.” For students, this means they need to regulate the SNS system and regain emotional and behavioral composure. During this stage, educators should only provide a safe space for the student and should not provide any directives to the student until they have had a chance to regain self-control (Greene, 2014).
Some researchers have also recently defined a “fawn” response to trauma, described as an individual who may respond to a trauma trigger by utilizing a protective strategy, whereby the individual attempts to please and appease others through extreme people-pleasing behaviors that may include neglecting their own values, needs, and boundaries (Harris, 2021). The “fawn” response is not derived from the SNS, as seen with fight, flight, or freeze responses, and is therefore not an automatic uncontrolled physical reaction to triggers.
The inability for the amygdala to recognize a real versus false alarm can be further explained by a disconnect between the limbic brain and the last region of the Triune brain model, the neocortex region (Bremner, 2006). The neocortex, described as “the executive” of the brain, is in the upper region of the brain and responsible for rational interpretation of outside stimuli and overall behavioral control, including logical thinking, problem-solving, judgment, emotional expression, emotional regulation, creativity, planning and organizing, processing, attention, working memory, and overall effort (MacLean, 1990).
Perhaps, the most important component of understanding the rational brain when considering trauma triggers is the medial prefrontal cortex (MPFC), which is described as a “watchtower.” Its major role is to process input from the limbic brain (emotional part of the brain) to interpret input (e.g., trauma triggers) and act accordingly (Pittman & Karle, 2015; Van der Kolk, 2014). The neocortex region of the brain provides individuals with the ability to identify a real versus a false threat and consequently access self-regulation skills to address the trigger (Harris, 2021).
Students who have experienced trauma often have long-term deficits in these processing skills and emotional regulation, which affects a student’s ability to interpret trauma triggers while managing strong emotions, engaging in learning, sustaining attention to learning and problem-solving, and controlling impulses that could interfere with learning (Harris, 2021; Jennings, 2019; Van der Kolk, 2014). Essentially, when the amygdala triggers an emergency signal, the neocortex area of the brain that is needed to provide rational thought often takes longer to respond or may be impaired due to age, ability level, and previous trauma (Van der Kolk, 2014).
Students who have experienced trauma may regularly experience a heightened state of arousal, meaning their SNS is always running in overdrive (Van der Kolk, 2014). It is common for students who have experienced trauma to misinterpret input, assign it to traumatic memories, and then react in harmful ways (Harris, 2021). Consequently, students who are triggered by trauma are likely to demonstrate poor impulse control, have difficulty in recognizing the emotional signals of classmates and educators, and are often uncertain about trusting peers and adults (Jennings, 2019). In many cases, students who have experienced trauma may develop an impaired view of their external and internal perceptions (Pittman & Karle, 2015). Van der Kolk (2014) describes this phenomenon best: “After trauma the world is experienced with a different nervous system. The survivor’s energy now becomes focused on suppressing inner chaos, at the expense of spontaneous involvement in their life” (p. 53).
Understanding How Trauma Affects Student Performance in School
When the brain processes trauma, stress and trauma exposure can impair emotional regulation and executive functioning accessed through executive high-order reasoning. For students in schools, this means there are likely many instances where inadvertent exposure to trauma-related triggers can result in student behavior challenges, including demonstrating an inability to follow directions, participate in learning opportunities, pay attention, and work with others, and challenges with retaining/recalling information. Students who have experienced trauma may instead display challenging behaviors, such as verbal and physical aggression, attendance problems, difficulties in developing and maintaining peer relationships, and deficits in self-regulation. These issues contribute to the prevalence of academic and behavior challenges in schools, often leading to school dropout among adolescents in low-resource, high-crime neighborhoods (Mendelson et al., 2015).
Students who live in stressful family environments are also more likely to exhibit avoidant behavior (e.g., elopement, noncompliance) and are less likely to engage in problem-focused coping strategies (e.g., deep breathing, positive self-talk; Sheffler et al., 2019). Such students who experience severe and ongoing trauma may also have trouble accessing and identifying emotions, coping with emotions, and tolerating emotional expression. They will often demonstrate an impaired ability to regulate their impulses (Kliethermes et al., 2014). This can lead to difficulty in developing and maintaining peer relationships, responding appropriately to disappointment or failures, and identifying the emotions of peers and teachers. Returning to Ashra, we provide an example of how trauma can lead to responding to triggers through avoidance behaviors due to a fear of re-experiencing disappointments or failures.
After Ashra’s team discovered she had previous traumatic experiences and developed a BIP to address her challenging behaviors, she began to demonstrate significant progress. Her grades were improving, the frequency of her challenging behaviors was decreasing, and her overall affect seemed to be improving. One day, Ashra’s teacher was absent and she had a substitute. The school administrators, counselor, and social worker were called several times to the classroom due to Ashra’s behaviors. She was yelling and screaming at the substitute, running out of the classroom, and throwing classroom materials, such as school boxes, pencils, and notebooks.
Eventually, the team had Ashra finish her school day by working in one of her reading teachers’ rooms. Her behaviors immediately stopped. After school, the team met to debrief the situation to determine the reason behind Ashra’s behavior. Initially, the team thought it was because the substitute was a male. However, there had been other male substitutes in the classroom and she did not demonstrate those behaviors in the past. One of the administrators called Ashra’s mom to discuss the incident with her and seek her input as to why Ashra’s challenging behaviors had resurfaced. Ashra’s mom was unsure, but she said that she would talk to Ashra that night. The next day, Ashra’s mom brought her to school. She explained to the school team that Ashra told her that the male substitute teacher smelled like her dad and “creeped her out.” She thought her dad was disguised as the substitute so he could find and hurt her.
For students who have experienced complex trauma, behaviors displayed can also include maintaining a state of hyperarousal or hypervigilance, with a tendency to overreact to stimuli that may go unnoticed by others (Razuri et al., 2016). This is because their amygdala is continuing to send warning signals to the brain, thereby activating the SNS (Van der Kolk, 2014). Hyperarousal can include symptoms of sleeping, hypervigilance, and irritability (Ehlers et al., 2004). Sympathetic nervous system hyperarousal often extends to conditions that are not necessarily consistent with the trauma that occurred (Friman et al., 1998). For example, hyperarousal can include fear, panic, and uncontrolled anger that seems to be disconnected from any observed triggers (Spence et al., 2021). At times, it can also be confused with attention-deficit/hyperactivity disorder (ADHD).
Moving From Trauma Awareness to Universal and Targeted Trauma-Informed Practice
Once educators understand how trauma may impact their students academically, emotionally, socially, and behaviorally, they are encouraged to implement a multi-tiered system of trauma-informed practices in accordance with the Substance Abuse and Mental Health Services Administration (SAMHSA) guidance that emphasizes (a) the importance of providing students who have experienced trauma with the appropriate individual supports necessary to address their needs and (b) suggestions for the development of a trauma-sensitive classroom that include a “trauma-sensitive de-escalation protocol” for crisis related to trauma (Hanover Research, 2019).
However, perhaps the most simple and key trauma-informed practice begins first with educators actively developing a rapport with their students and creating a safe and supportive learning environment. Research has consistently demonstrated that resilient outcomes are associated with students who have a meaningful connection with at least one safe adult who is trusting and provides unconditional support (Van der Kolk, 2014).
Universal Trauma-Informed Practice
Universal schoolwide positive behavioral interventions and supports (SWPBIS) can be helpful in establishing a trauma-informed classroom that prevents and addresses several social and behavioral challenges commonly experienced by children who have a history of trauma (Cavanaugh, 2016). Such universal supports are provided to all students in the school regardless of whether they have experienced trauma. This approach is especially pragmatic given the large number of undisclosed cases of trauma that continue to exist.
Schoolwide positive behavioral interventions and supports practices focus on the importance of integrating learning, social and emotional functioning, mental and physical health, and the overall well-being of students for all areas of the school and child (Rossen & Cowan, 2013). Through SWPBIS, a safe and predictable learning environment is created by developing, teaching, and reinforcing three to five schoolwide expectations (Horner et al., 2010). These expectations include universal routines, procedures, and behavior interventions that are taught and reinforced throughout the school environment and schedule. It is important to note, however, that students who have experienced trauma may need additional reminders or specific prompts when there are to be changes within their routine (Cavanaugh, 2016). For example, if a fire or tornado drill is scheduled to occur within the school day, it may be essential to provide visual and/or verbal reminders about the upcoming drill to individual students. Other events to consider providing additional reminders can include upcoming substitutes, assemblies, or early release schedules.
Targeted and Individualized Trauma-Informed Practice
Before providing any targeted or individualized supports in the classroom, a critical element of effective implementation is an accurate identification of student needs (Jennings, 2019). To do this, educators are encouraged to adopt a trauma-sensitive screener used for the purposes of identifying challenging behaviors that may be associated with trauma. These screeners should use a trauma-sensitive approach by screening both internalizing (i.e., anxiety, depression, dissociation) and externalizing (i.e., aggression, defiance, disruptive) behaviors (Cavanaugh, 2016; Jennings, 2019). Once students have been identified through universal screening, more individualized interventions can be provided based on identified student need(s).
Table 2 provides descriptions of common challenging behaviors resulting from trauma and accompanying trauma-informed practices to use in the classroom. The practices described in the table can be used universally (whole class/whole school), targeted (small group), or individually (student only) to address the social, emotional, behavioral, and academic needs of students. It is important to note that any new skill should always be taught through explicit instruction, modeling, and practicing skills with feedback and ongoing positive reinforcement. Each area of need is described below.
Trauma-Informed Practices According to Student Need.
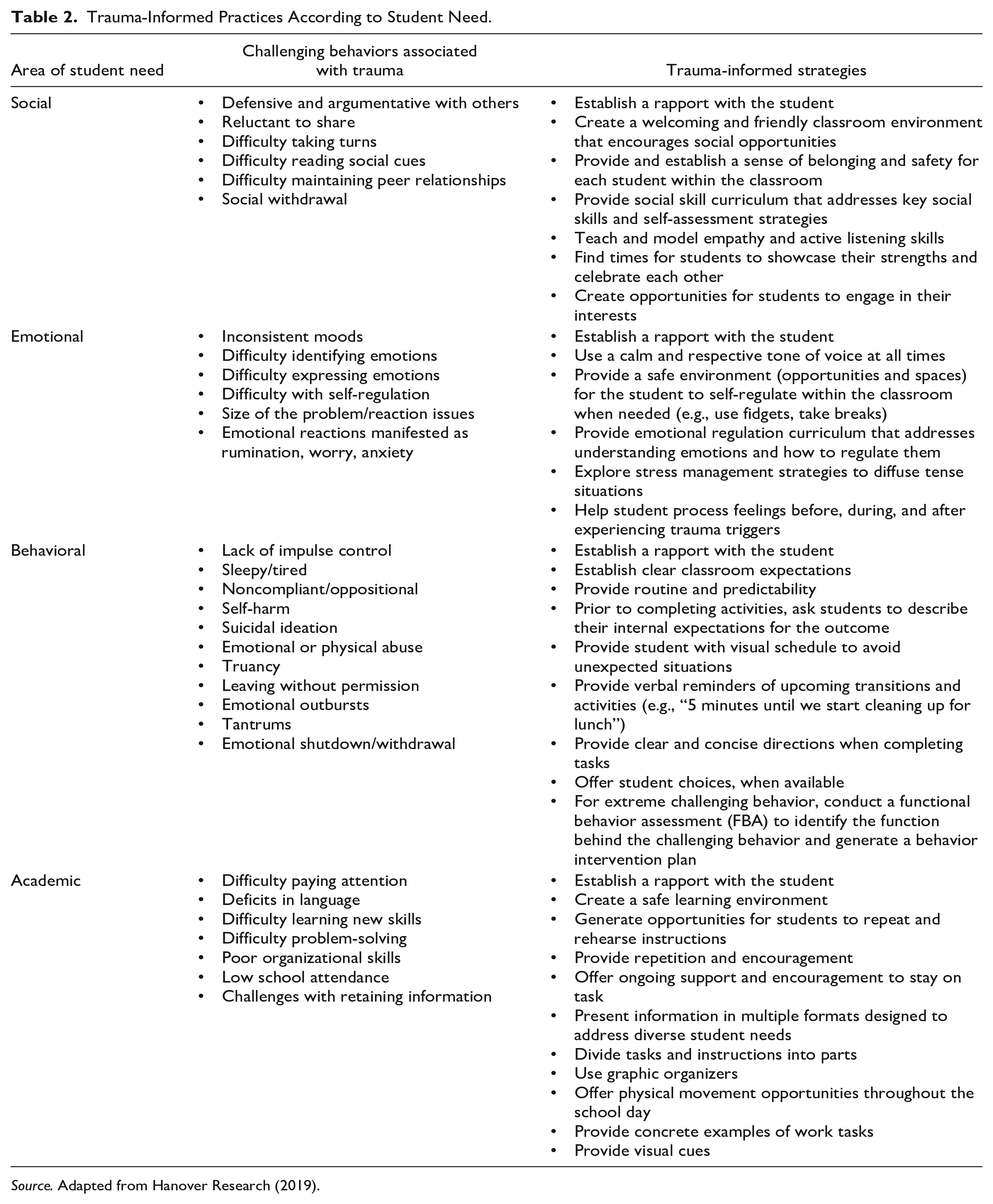
Source. Adapted from Hanover Research (2019).
Social challenges
Students who have experienced trauma may exhibit social challenges that include but are not limited to defensive and argumentative actions with others, reluctance to share, difficulty taking turns, difficulty reading social cues, social withdrawal, and difficulty maintaining peer relationships. Some potential interventions for social skill challenges may include providing the student with a targeted or personalized social skill curriculum that addresses key social skills and self-assessment strategies, teaching and modeling empathy, and active listening skills for the student, providing opportunities for students to showcase their strengths, celebrate each other, and engage in their interests together (Hanover Research, 2019). For example, students who struggle with anger management or problem-solving skills may benefit from targeted social skills instruction delivered in a small-group format.
Emotional challenges
Emotional challenges exhibited by students who have experienced trauma can include inconsistent moods, difficulty expressing emotions, and difficulty with self-regulation. These students may also display emotional responses that are not consistent with the size of a problem. For example, a student may display overreaction by crying and fretting over a missing pencil. Most students would see this as a small problem and solve it by getting another pencil from their school box. These students may also exhibit emotional reactions manifested as rumination, worry, or anxiety.
Potential interventions include always using a calm and respectful tone of voice, teaching and practicing mindfulness, providing an area in the classroom where the student can self-regulate when needed, and helping the student process feelings before, during, and after experiencing triggers leading to retraumatization (Hanover Research, 2019). For example, if a student is having a hard time losing at a small-group game, the teacher may support the student by helping the student to (a) practice mindfulness by naming the emotions and feelings they are experiencing at the time and (b) experience the disappointment of losing at the game without the problem behavior.
Behavioral challenges
Students who have experienced trauma may also display internal and external behavioral challenges. Examples of challenging behaviors can include a lack of impulse control, tantrum, emotional shutdown, emotional outbursts, and noncompliance. For these behaviors, interventions could include providing a predictable routine, establishing clear classroom expectations, offering choices, and providing clear and concise directions when completing tasks (Hanover Research, 2019).
Students may also engage in self-harming behaviors, suicide ideation, and emotional or physical abuse. In this case, it is important to establish a meaningful rapport with the student. It will also be beneficial to consult with the school counselor or social worker to ensure safety plans are developed if needed. For extreme challenging behaviors, it is important to identify the function of the behavior through a functional behavior assessment aimed identifying the trauma trigger(s) and purpose(s) of the behavior in order to develop an informed plan for how to successfully respond. Data collected can inform the comprehensive BIP, which will be designed to prevent the occurrence of the trauma trigger(s), neutralize the impact of the trauma trigger(s) on student behavior, and, in cases where a student is re-experiencing trauma, generate a plan for providing the student with safety and support.
Academic challenges
Academic challenges experienced by students who have a history of trauma often include deficits in language, problem-solving difficulties, poor organization skills, difficulty learning new skills, and challenges with retaining information. Some interventions to consider for these academic challenges include preteaching skills, presenting information in multiple formats, dividing tasks and instructions into parts, providing opportunities for the students to repeat and rehearse instructions, and providing students opportunities to complete major assignments and tests in private settings, if needed (Hanover Research, 2019). It is also important to offer ongoing support and encouragement for students to remain on task. Therefore, educators are encouraged to provide students with ongoing positive reinforcement opportunities to encourage on-task behavior.
While constructing her BIP, Ashra’s team made sure to address her social, emotional, behavioral, and academic needs. Socially, Ashra seemed to be withdrawn. She would typically avoid peer interactions and frequently isolated herself. To address this concern, Ashra’s teacher worked to create a welcoming and friendly classroom environment that encouraged social opportunities. She often used cooperative learning strategies and had her class engage in several community-building activities. Within her BIP, the team addressed concerns regarding Ashra’s difficulty in identifying and expressing emotions, including frequent exhibitions of emotional reactions that were inconsistent with the size of the problem. The team included information within the BIP about incorporating frequent breaks within her schedule as well as discussing the need for staff to help her process her feelings before, during, and after she experienced any type of emotional trigger.
Behaviorally, Ashra would have emotional outbursts that included yelling at her teacher or other students, throwing items, such as pencils or crayons, and leaving the classroom without permission. To address these behaviors, the team specified within the BIP the importance of providing clear and concise directions for tasks, visual and verbal reminders of upcoming transitions to activities, and offering Ashra choices of where she wanted to complete her work or what tool she used to record her answers (e.g., pencil, colored pencil, typing answers).
Finally, the team addressed Ashra’s academic needs within the BIP as well.
With academics, Ashra demonstrated difficulty problem-solving, poor organizational skills, and challenges with retaining information. Interventions for these areas of need included generating opportunities for Ashra to repeat the directions back to the teacher, dividing assignments into smaller segments, allowing Ashra to take movement breaks, and providing visual cues, such as checklists to assist with her organizational skills. The team reviewed the BIP regularly to determine whether the interventions were increasing Ashra’s work completion while also decreasing emotional outbursts.
Conclusion
Every day, students who have experienced trauma enter our schools. Most of these students are often misdiagnosed as having oppositional defiant disorder, ADHD, or they are judged as being hyperactive, elusive, or noncompliant, when the underlying reasons behind these behaviors are associated with trauma (Van der Kolk, 2014). It is our hope that this article provided a primer about trauma for educators to understand the definition and impact traumatic experiences can have on students in today’s schools.
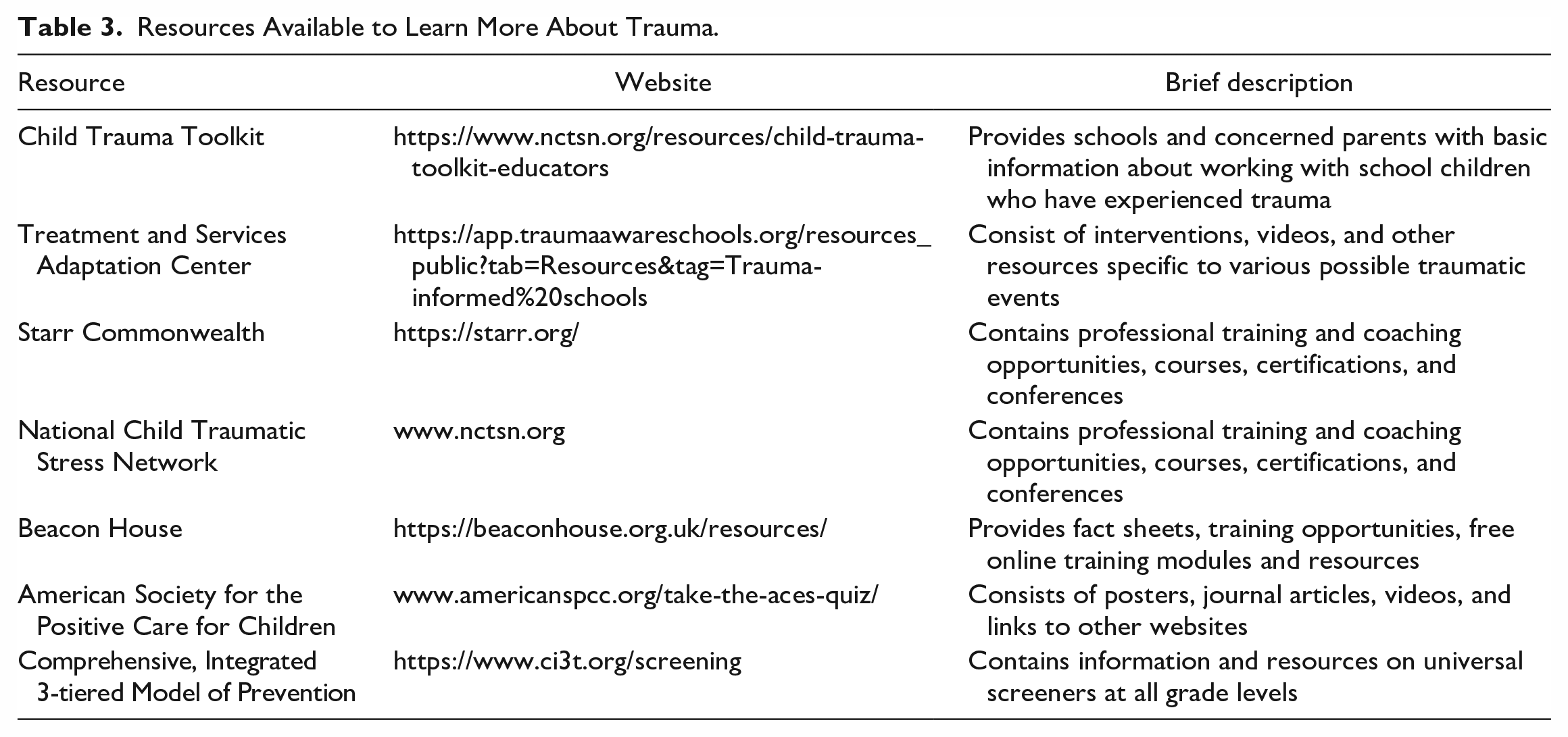
Teachers are not expected to act as licensed counselors. However, understanding trauma, the types of traumas, and the emotional, social, behavioral, and academic impact trauma can have on students are important considerations before responding to student challenging behavior(s). Furthermore, understanding how the brain processes trauma and events related to trauma can provide educators with more background knowledge and an explanation for why some students may exhibit challenging behaviors “out of the blue” or in response to identified triggers that are related to a traumatic event. Table 3 lists resources that are available for educators to pursue a deeper understanding about trauma. Until we can regularly consider trauma when working with students, it is possible that these students may go unnoticed, be misdiagnosed, or inadvertently be retraumatized through aversive behavioral consequences.
Resources Available to Learn More About Trauma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.