
Abstract
Introduction
Dysregulation of the coagulation and fibrinolytic systems has been closely linked to cancer progression and metastasis. This study investigated whether the coagulation- and fibrinolysis-related biomarkers, TAT, PIC, TM, and tPAIC, are correlated with cancer metastasis.
Methods
Plasma levels of TAT, PIC, TM, and tPAIC were measured in 240 treatment-naive patients with lung, ovarian, breast, or colorectal cancer and 120 healthy individuals. Participants were categorized into metastasis, non-metastasis and healthy groups based on clinical evaluation and imaging results. Statistical analysis and ROC curves were used to assess the performance of individual and combined biomarkers in detecting metastasis.
Results
All four biomarkers were significantly elevated in patients with metastasis (P < .001). In multivariate logistic regression analysis, PIC demonstrated the strongest association with metastasis. ROC curve analysis revealed that in lung cancer patients, a parallel test of TAT and PIC achieved a sensitivity of 93.33% and an NPV of 88.24%. In ovarian cancer, a serial test of TAT, PIC, and TM achieved a specificity of 80.00% and a PPV of 75.00%. In breast cancer, a parallel test of TAT, PIC, and tPAIC yielded a sensitivity of 93.33% and an NPV of 89.47%. In colorectal cancer, a parallel test of all four markers achieved a sensitivity of 96.67% and an NPV of 93.75%.
Conclusion
Distinct combinations of coagulation and fibrinolysis biomarkers demonstrate high diagnostic performance for detecting metastasis across different cancer types. Tailoring biomarker panels according to cancer type may provide significant clinical value in monitoring and predicting cancer metastasis.
Introduction
Metastasis is the leading cause of death in over 90% of cancer patients.1-2 Identifying reliable biomarkers associated with metastasis is crucial for monitoring treatment response and detecting disease recurrence. Growing evidence suggests a close relationship between the coagulation and fibrinolytic systems and cancer metastasis,3-7 underscoring the need to further evaluate their potential as predictive markers.
Disruption of vascular endothelial cells is a key event for tumor metastasis. Tumor cells induce breakdown of the endothelial barrier, and the resulting endothelial damage provides adhesion sites and transendothelial “windows” for circulating tumor cells to extravasate, thereby promoting tumor cell metastasis.8-9 Thrombomodulin (TM), an integral membrane glycoprotein expressed on the endothelial cell surface, is a sensitive marker of endothelial injury. Upon endothelial damage, subendothelial collagen and tissue factor (TF) become exposed. TF is a potent activator of the extrinsic coagulation pathway, leading to thrombin generation. Thrombin promotes metastasis by activating platelets and facilitating fibrin formation, thereby creating a “protective” microenvironment that enables tumor cells to evade immune surveillance and adhere to vascular endothelium. Furthermore, thrombin triggers intracellular signaling pathways, specifically the phosphoinositide 3-kinase (PI3K)/Protein kinase B (AKT) and nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) pathways, via protease-activated receptors (PARs), including PAR-1, and PAR-2. This activation promotes the epithelial-mesenchymal transition (EMT), which in turn drives tumor cell metastasis. 10 Thrombin catalyzes the conversion of fibrinogen to fibrin. Fibrin deposition provides a provisional matrix for tumor cell attachment and migration via interactions with integrins and adhesion molecules. 11 Tumor cells secrete urokinase-type plasminogen activator (uPA), while damaged endothelial cells release tissue-type plasminogen activator (tPA). Both uPA and tPA convert plasminogen to plasmin, which degrades laminin and fibrin, thereby promoting tumor invasion.12-13 Conversely, vascular endothelial cells and tumor cells secrete plasminogen activator inhibitor-1 (PAI1), which inhibits tPA and uPA, thereby suppressing fibrinolysis. tPA contribute to the extracellular matrix (ECM) degradation by activating plasminogen and MMPs. 14 PAI1 binds with high affinity to the somatomedin B domain of vitronectin, and it promotes tumor cell detachment from the ECM and enhances metastasis potential by disrupting uPAR-vitronectin interactions.11,15 PAI1 enhances circulating tumor cell adhesion to endothelium, facilitates tumor cell detachment from the ECM, stimulates tumor angiogenesis and tumor cell proliferation, ultimately promoting cancer invasion and metastasis.11,16 Thus, coagulation and fibrinolysis are intricately linked to cancer metastasis.
Under physiological conditions, thrombin has a very short half-life and rapidly binds to antithrombin to form the thrombin-antithrombin complex (TAT), a sensitive marker of coagulation activation. Similarly, plasmin is quickly neutralized by α2-antiplasmin, forming the stable plasmin-α2-antiplasmin complex (PIC), a specific marker of fibrinolytic activation. Elevated PIC levels indicate stronger fibrinolytic activity. Both tPA and its inhibitor, PAI1, are unstable in circulation and rapidly form a stable 1:1 complex, the tissue plasminogen activator-plasminogen activator inhibitor complex (tPAIC). 17 Therefore, tPAIC levels directly reflect the degree of fibrinolysis inhibition, with higher tPAIC indicating suppressed fibrinolytic function.
Collectively, TAT, PIC, TM, and tPAIC represent biomarkers of coagulation activation, fibrinolytic activation, endothelial injury, and fibrinolytic inhibition, respectively. The present study investigates the clinical significance of this biomarker panel by comparing plasma levels of these markers among patients with metastatic cancer, non-metastatic cancer, and healthy controls.
Materials and Methods
Patients and Healthy Controls
A total of 360 participants were enrolled in the study, including 240 patients with cancer and 120 healthy individuals. All of these individuals were tested for TAT, PIC, TM and tPAIC levels.
The 240 patients were recruited from Peking University Third Hospital and Beijing Haidian Hospital between April 2024 and August 2025. The inclusion criteria were as follows: patients with a histopathologically confirmed cancer diagnosis based on surgical or endoscopic specimens; those with no history of venous thromboembolism (VTE), including deep vein thrombosis or pulmonary embolism; no use of anticoagulant therapy within the past month; no surgical procedures performed within the past month; and no chemotherapy administered within the past month. Patients were excluded if they had active infections, known coagulation disorders, or concurrent malignancies.
The patient cohort comprised four cancer types: lung cancer (51 men and 9 women, mean age: 64.23 ± 10.05), ovarian cancer (60 women, mean age:57.32 ± 12.22), breast cancer (60 women, mean age:55.72 ± 9.60), and colorectal cancer (36 men and 24 women, mean age: 63.33 ± 9.60). For each type of cancer, patients were categorized into metastasis and non-metastasis groups. The presence of metastasis was initially determined via imaging examination, including computed tomography, ultrasonography, or magnetic resonance imaging, and further confirmed by pathological evaluation of metastatic lesions when tissue was accessible via biopsy or surgery.
Healthy volunteers were recruited from the physical examination centers of Peking University Third Hospital, including 30 men and 90 women with a mean age of 44.04 ± 11.81 years. Healthy controls were included if they had no history of malignancy, no long-term medication use, particularly anticoagulants, and normal results in routine blood tests, liver and kidney function tests, and coagulation profiles.
Sample and Data Collection
Venous blood samples (2 mL) were collected from all participants via antecubital venipuncture into vacuum tubes containing 0.109 mol/L sodium citrate as an anticoagulant. The samples were centrifuged at 3000 g for 15 min at 2-15 °C to obtain plasma. Samples that cannot be analyzed within 4 h were immediately stored at −80 °C until testing.
Clinical and demographic data collected from patients included age, gender, body mass index (BMI), smoking history, and comorbidities such as hyperlipidemia and diabetes mellitus. The study protocol was reviewed and approved by the Ethics Committee of the National Research Institute for Health and Family Planning. Written informed consent was obtained from all participants prior to enrollment and sample collection.
Measurement of TAT, PIC, TM, and tPAIC
The plasma levels of TAT, PIC, TM, and tPAIC were measured using the Automated Immunoassay System HISCL-5000 (Sysmex Corporation, Japan). The following reagent kits were utilized for the corresponding assays: HISCL TAT Assay Kit, HISCL PIC Assay Kit, HISCL TM Assay Kit, and HISCL tPAIC Assay Kit (Sysmex Corporation, Japan). All measurements were conducted in accordance with the manufacturer's instructions.
A single peripheral blood sample was collected from each participant, and this specimen was used to determine the plasma concentrations of all four biomarkers.
Statistical Analysis
All statistical analyses were performed using SPSS Version 27.0 and R 4.5.1.
The Shapiro-Wilk test (for sample sizes n ≤ 50) or the Kolmogorov-Smirnov test (for n > 50) was applied to assess data normality. For continuous variables following a normal distribution, data are presented as mean ± standard deviation (
Univariate logistic regression analysis was performed to identify variables associated with cancer metastasis. Variables showing significant associations were further analyzed using a multivariate logistic regression model to determine independent predictors of metastasis and to quantify metastasis risk. To assess model performance, 80% of the samples were randomly assigned to a training set for model construction, and 20% were reserved as a validation set for performance evaluation.
A nomogram was constructed using R software to translate the multivariate logistic regression model into a quantitative scoring system, in which each variable was assigned a score according to its regression coefficient. Model calibration was assessed using calibration curves and the Hosmer-Lemeshow goodness-of-fit test to evaluate agreement between predicted and observed outcomes.
Receiver operating characteristic (ROC) curve analysis was conducted to evaluate the diagnostic performance of each variable and their combinations in predicting metastasis. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated at the optimal cutoff value determined by the Youden index.
Results
Patient Characteristics
A total of 240 cancer patients were enrolled in this study, including 120 patients in the metastasis group and 120 in the non-metastasis group. As shown in Table 1, there were no statistically significant differences between the two groups in age, sex, smoking history, or the prevalence of hyperlipidemia and diabetes.
Comparison of Characteristics of Cancer Patients According to Metastasis Status.

Ages are presented as mean ± standard deviation (
Differences in Coagulation and Fibrinolysis Markers among the Metastasis, Non-Metastasis, and Healthy Groups
As shown in Table 2, the plasma levels of TAT, PIC, TM, and tPAIC differed significantly among the metastasis, non-metastasis, and healthy groups (P < .001). Within the cancer patients, the levels of TAT, PIC, TM, and tPAIC were significantly higher in the metastasis group than in the non-metastasis group (P < .001, Figure 1).

Post-Hoc pairwise comparisons of coagulation and fibrinolysis markers.
Comparison of Coagulation and Fibrinolysis Marker Levels among Metastasis, Non-Metastasis, and Healthy Control Groups.

Values are expressed as median (interquartile range, IQR; first and third quartiles).
Further subgroup analysis by cancer types, including lung, breast, ovarian, and colorectal cancers, indicated that the levels of these four markers were consistently elevated in the metastasis groups compared with their corresponding non-metastasis groups (Table 3).
Comparison of Coagulation and Fibrinolysis Marker Levels Between Metastasis and Non-Metastasis Groups Across Different Cancer Types.

Values are expressed as median (interquartile range, IQR; first and third quartiles).
Multivariate Modeling Analysis of the Association Between Coagulation and Fibrinolysis Markers and Cancer Metastasis Risk
To identify key factors associated with cancer metastasis while minimizing model overfitting due to multicollinearity, a univariate logistic regression analysis was performed to screen potential variables. As presented in Table 4, elevated plasma levels of TAT, PIC, TM, and tPAIC were significantly associated with an increased risk of cancer metastasis (P < .05).
Univariate Logistic Regression Analysis of Variables Associated with Cancer Metastasis Risk.

Subsequently, the four significant biomarkers were incorporated into a multivariate logistic regression model to further evaluate their independent effects on metastasis risk. The nomogram indicated that PIC contributed the highest weighted score, indicating its strongest discriminatory power for metastasis, followed by tPAIC, while TAT showed the relatively lowest weight (Figure 2A). The model demonstrated good discriminative performance, with an AUC of 0.735 in the training set and 0.780 in the validation set (Figure 2B). The calibration curve showed excellent agreement between predicted and observed probabilities, with a Brier score of 0.204, and the Hosmer-Lemeshow test yielded a non-significant result (P = .856), confirming adequate model fit (Figure 2C).

Development and validation of a logistic regression model for predicting cancer metastasis risk. A: Nomogram for risk prediction. B: ROC curves of the model in the training and validation sets. C: Calibration curve of the model.
ROC Analysis of Combined Coagulation and Fibrinolysis Markers for Predicting Cancer Metastasis Risk
To further assess diagnostic performance, ROC curve analysis was conducted to evaluate the sensitivity and specificity of individual and combined coagulation and fibrinolysis markers across different cancer types. As shown in Figure 3, among the individual markers, PIC exhibited the highest AUC for predicting metastasis in lung and breast cancers, whereas TAT achieved the highest AUC in ovarian and colorectal cancers.
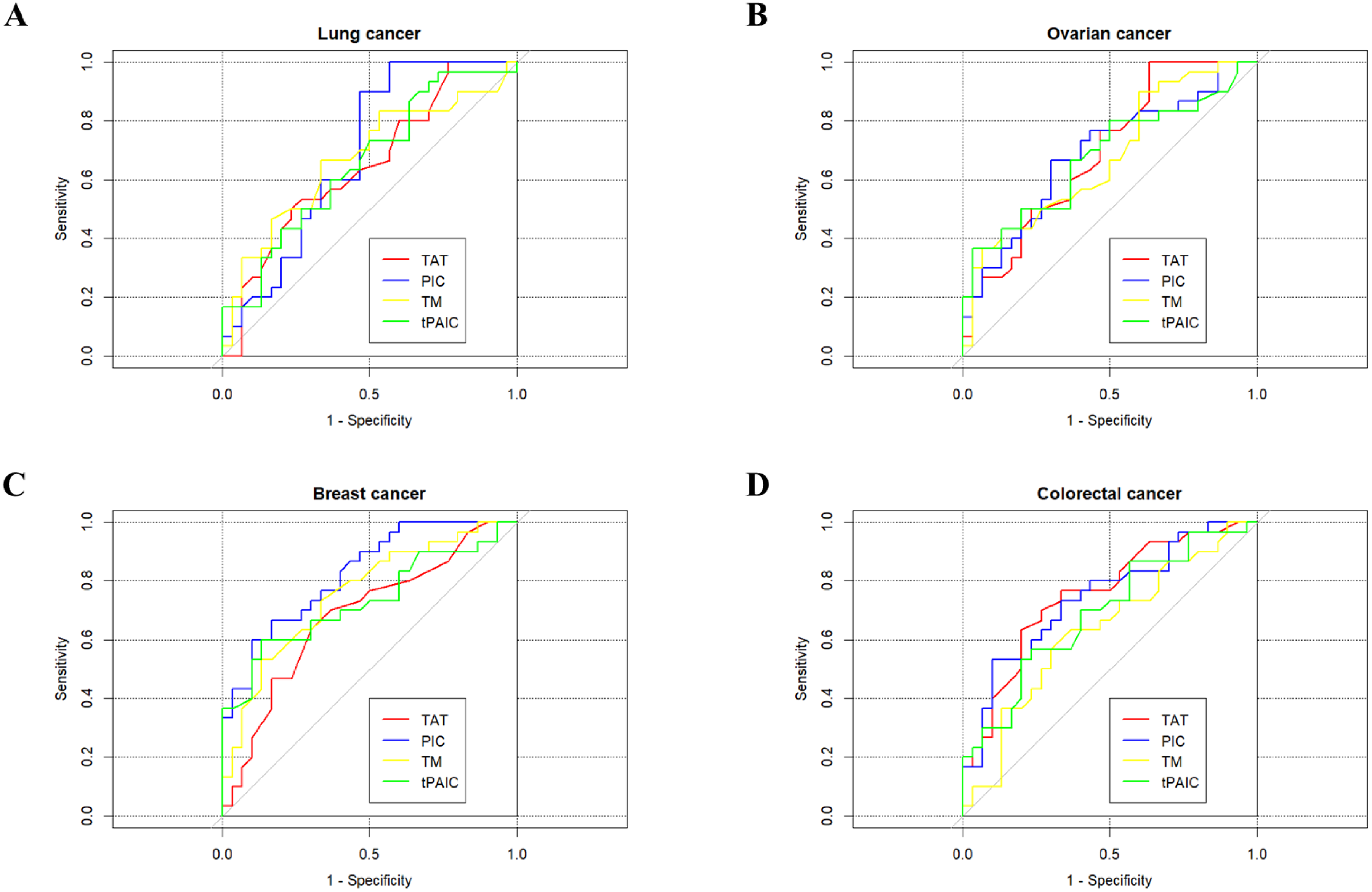
ROC curves showing the predictive performance of TAT, PIC, TM, and tPAIC for metastasis across lung, ovarian, breast, and colorectal cancers.
As shown in Table 5, Individual biomarkers exhibit distinct performance limitations. When utilized independently for lung and breast cancer, PIC demonstrates lower sensitivity and NPV compared with multi-marker panels. In ovarian cancer, TAT shows perfect sensitivity (100%) and NPV (100%), but its specificity is notably low (36.7%), resulting in a high risk of false-positive rate and making it unsuitable as a standalone tool for precise diagnosis. Similarly, when TAT is used alone in colorectal cancer, both its sensitivity and NPV are inferior to those achieved by multi-marker combinations.
Diagnostic Accuracy of Coagulation-Fibrinolysis Biomarkers and Their Combinations for Predicting Metastasis in Lung, Ovarian, Breast, and Colorectal Cancers.

Parallel tests: Metastasis was considered present if any of the four markers (TAT, PIC, TM, or tPAIC) exceeded the cutoff value. Serial tests: Metastasis was considered present only if all four markers exceeded their respective cutoff values.
The optimal biomarker combination strategy varies by cancer type to optimize the balance of diagnostic parameters. For lung and breast cancer, a parallel testing strategy (eg, TAT + PIC or TAT + PIC + tPAIC) maximizes sensitivity and NPV to minimize missed diagnoses. In ovarian cancer, TAT has high sensitivity but very low specificity, whereas tPAIC shows high specificity but very low sensitivity, using a serial combination test (TAT + PIC + TM) achieves a more balanced diagnostic profile, with all performance metrics exceeding 50%, thereby achieving a practical compromise between sensitivity and specificity. For colorectal cancer, a parallel test of incorporating all four markers (TAT, PIC, TM, and tPAIC) elevates sensitivity and NPV to their highest levels (96.67% and 93.75%), demonstrating the cumulative effect of biomarker integration in enhancing overall diagnostic performance.
Discussion
TAT, PIC, TM, and tPAIC are key molecules involved in the coagulation and fibrinolytic systems and play crucial roles in cancer metastasis. These four biomarkers are interrelated rather than independent entities. Activation of coagulation can stimulate fibrinolytic activity, endothelial injury serves as both the initiator and the site of these processes, and fibrinolytic imbalance alters the tumor microenvironment's structural and rheological properties. Collectively, they form a vicious cycle of “endothelial injury-coagulation activation-fibrinolytic imbalance”, which significantly facilitates multiple steps in the metastatic cascade. It should be noted that this is a conceptual framework and further mechanistic studies are needed to validate it.
Numerous studies have associated individual markers with cancer metastasis. TAT levels are elevated in metastatic cancers compared with non-metastatic cases. 18 PIC concentrations are significantly increased in patients with metastatic soft tissue sarcoma. 6 The relationship between TM and tumor metastasis is completely different in vivo versus in vitro. TM overexpression inhibits the migration and invasion of lung cancer cells, thereby functioning as a tumor suppressor protein. 19 Silencing TM in skHep-1 cells enhanced metastatic potential, whereas its overexpression in HepJ5 cells reduced it. 20 TM also exerts inhibitory effects on ER+ breast cancer progression and metastasis, 21 and its expression negatively correlates with the metastatic potential of melanoma cells in vitro. 22 In patients with soft tissue sarcoma, plasma TM levels were significantly higher in the metastatic group than in the non-metastatic group. 23 Elevated tPAIC levels have also been reported in patients with hematogenous metastasis of gastric cancer. 24 However, studies examining the combined diagnostic value of these four markers are limited. Our study therefore aims to assess the clinical utility and diagnostic performance of the integrated panel across four major cancers: lung, breast, ovarian, and colorectal cancers.
In our study, TAT, PIC, TM, and tPAIC levels differed significantly among the metastasis, non-metastasis, and healthy groups. Among all cancer patients, each biomarker was significantly elevated in the metastasis group compared with the non-metastasis group. This trend was consistently observed across all four cancer types, including lung, ovarian, breast, and colorectal cancers. Univariate logistic regression analysis confirmed that elevated levels of TAT, PIC, TM, and tPAIC were independently associated with an increased risk of metastasis, highlighting the potential utility of these markers in assessing metastatic risk.
ROC analysis revealed that PIC achieved the highest AUC in lung and breast cancers, while TAT showed the highest AUC in ovarian and colorectal cancers. Cancer-type-specific biomarker panels demonstrated superior diagnostic performance compared with individual markers. For example, the combined biomarker panel achieved a sensitivity of 93.33% and an NPV of 88.24% in lung cancer. In ovarian cancer, the specificity and PPV reached 80.00% and 75.00%, respectively. In breast cancer, the sensitivity was 93.33% with an NPV of 89.47%, while in colorectal cancer, the sensitivity and NPV were 96.67% and 93.75%, respectively.
These findings suggest that a tailored biomarker panel, optimized for specific cancer types, may serve as an early indicator for metastasis risk assessment and guide subsequent imaging evaluation. If biomarker levels increase during follow-up, timely imaging examination should be performed to detect potential metastasis, enabling more aggressive adjuvant therapy or closer surveillance to prevent disease progression.
This study has several limitations. First, it was a two-center, retrospective study with a relatively limited sample size, which may introduce selection bias. Future multi-center, large-sample, prospective studies are needed to validate our findings. In addition, our analysis included only four cancer types, and it remains uncertain whether these findings apply to other malignancies. Finally, although we explored clinical correlations and proposed potential mechanisms, direct in vivo or in vitro experimental evidence establishing causality is lacking and should be addressed in future research.
Conclusion
The aim of this study was to evaluate whether circulating levels of TAT, PIC, TM, and tPAIC differ among patients with metastatic cancer, non-metastatic cancer, and healthy controls, and to assess their potential clinical relevance as biomarkers of metastasis.In conclusion, our study demonstrated that the combined detection of the coagulation and fibrinolysis markers TAT, PIC, TM, and tPAIC held significant clinical value for assessing the risk of metastasis in lung, ovarian, breast, and colorectal cancers. This four biomarker panel may provide a novel and effective laboratory tool for clinical evaluation of the risk of metastasis in cancer patients. Furthermore, the optimal selection of coagulation-fibrinolysis biomarker panels should be tailored to the specific cancer type to achieve the best diagnostic performance.
Footnotes
Acknowledgements
The authors thank all participants who volunteered for this study.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the ethical standards of the National Health Commission of the People's Republic of China's Development Center for Medical Science & Technology and received formal approval from its Institutional Review Board (Ethic No. 2020024). All investigations were carried out in adherence to the principles of the Declaration of Helsinki.
Author Contributions
Huafang Gao conceived and designed the study. Yumei Zhao, Xinping Sun, and Bozhi Lin performed the data analysis and drafted the manuscript. Shiyuan Xu provided technical assistance, drafted proposals and critically revised the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
All data and figures were obtained from clinical trials in our center and are absolutely true and valid, the data that support the findings of this study are available from the corresponding author upon reasonable request.