
Abstract
Objectives
This study aimed to evaluate the efficacy and safety of AngioJet rheolytic thrombectomy with the adjunctive use of glycoprotein IIb/IIIa inhibitors (GPI) in the setting of ST-segment elevation myocardial infarction (STEMI).
Methods
We conducted a retrospective cohort study of 877 consecutive patients with STEMI. Propensity score matching (PSM) was employed to balance the baseline characteristics between the group receiving AngioJet rheolytic thrombectomy plus GPI (the AT + GPI group) and those receiving routine treatment (the RT group). The primary endpoint was major adverse cardiovascular and cerebrovascular events (MACCE) at 1 year. Safety endpoints comprised any bleeding and major bleeding events.
Results
Ninety-seven patients received AngioJet rheolytic thrombectomy and GPI. No significant differences were observed between the two groups regarding in-hospital mortality, reinfarction, stent thrombosis, stroke, or bleeding. After propensity-score matching, the cumulative incidence of MACCE at 1 year did not differ significantly between the AT + GPI group and the RT group (8.2% vs 9.3%; hazard ratio, 0.894; 95% CI, 0.345 to 2.318; p = 0.818). The incidence rates of all individual safety endpoints—including stroke and bleeding—showed no significant differences between the two groups.
Conclusions
In this observational cohort of STEMI patients, the strategy of combining AngioJet rheolytic thrombectomy with GPI was not associated with improved 1-year outcomes compared to routine treatment, though it did not increase bleeding or stroke risk.
Keywords
Introduction
Despite the established role of primary percutaneous coronary intervention (PCI) in restoring epicardial blood flow for patients with ST-segment elevation myocardial infarction (STEMI), a significant proportion of patients continue to experience poor myocardial perfusion and adverse clinical outcomes. 1 This discrepancy, often attributed to distal embolization and microvascular obstruction (MVO), represents a critical unresolved challenge in contemporary interventional cardiology. To address this, two adjunctive strategies have been extensively studied: thrombus aspiration to remove the embolic source and glycoprotein IIb/IIIa receptor inhibitors (GPI) to prevent downstream platelet aggregation. However, the individual application of each has yielded conflicting and often disappointing results in large-scale randomized trials.2–4 Therefore, a targeted strategy of routine thrombus aspiration, immediately followed by intracoronary GPI administration to neutralize the liberated thrombogenic debris, may synergistically protect the microvasculature and improve myocardial reperfusion.
Previous studies on the combined use of manual thrombus and GPI have reported conflicting results.5,6 As compared with manual thrombus aspiration, mechanical thrombectomy with AngioJet rheolytic is more effective in thrombus removal.7,8 Nevertheless, mechanical thrombus aspiration combined with GPI in acute myocardial infarction has not been investigated yet. This study aimed to evaluate the efficacy and safety of AngioJet rheolytic thrombectomy combined with GPI in patients with acute myocardial infarction underwent PCI.
Materials and Methods
Study Design and Population
This retrospective cohort study consecutively enrolled patients with STEMI according to predefined criteria at the Sixth Medical Center of the Chinese PLA General Hospital from October 2014 to April 2019. Acute myocardial infarction was defined as meeting all of the following criteria: elevated serum cardiac troponin I level above the 99th percentile of the upper reference limit and with at least one of following: symptoms of myocardial ischaemia; new ischaemic ECG changes; development of pathological Q waves; imaging evidence of new loss of viable myocardium or new regional wall motion abnormality in a pattern consistent with an ischaemic aetiology; identification of a coronary thrombus by angiography or autopsy. 9 Exclusion criteria were active bleeding or a known history of severe bleeding diathesis, history of ischemic stroke within the past 3 months, a rejection of invasive surgery, excessive tortuosity or severe calcification of the culprit vessel, the infarct-related artery had a reference vessel diameter of <2.5 mm.
The requirement for obtaining informed consent was specifically waived by the Ethics Committee of the Sixth Medical Center of the Chinese People's Liberation Army General Hospital on the grounds that the study solely involved analysis of anonymized data.
Cardiac Catheterization and Coronary Intervention
Following administration of a loading dose of dual antiplatelet therapy (aspirin 300 mg combined with clopidogrel 300/600 mg or ticagrelor 180 mg), subsequent management was guided by clinical needs. The administration of low molecular weight heparin, as well as the deployment of an intra-aortic balloon pump (IABP) for hemodynamic support, were utilized per operator judgment. In our cohort, all oral anticoagulants used were warfarin, with no novel oral anticoagulants administered.
The GPI tirofiban was manufactured by Grand Pharma (China) Co., Ltd (Hubei, China; National Medicine Approval Number: H20041165). For patients with STEMI undergoing PCI, tirofiban was administered intravenously in conjunction with unfractionated heparin and aspirin. The standard protocol included an initial loading infusion of 0.4 μg/kg/min for 30 min, followed by a continuous maintenance infusion of 0.1 μg/kg/min. The maintenance infusion was typically sustained for 36 h. In cases of severe renal impairment (creatinine clearance < 30 mL/min), the dosage of tirofiban was reduced by 50%. Patients also received a loading dose of clopidogrel/ticagrelor before PCI, in addition to aspirin and heparin.
In our clinical practice, the AngioJet thrombectomy is reserved for patients with large thrombus burden. The AngioJet Ultra Thrombectomy System (Boston Scientific) comprises a 4-F aspiration catheter, a pump set, and a drive unit console. Following priming of the catheter with heparinized saline (until the display read zero seconds), the activated device was advanced from at least 1 cm proximal to the thrombus through the lesion at 2 mm/s. Multiple passes were performed until angiographic thrombus resolution. Each suction period was deliberately limited to <5 s to limit hemodynamic disturbances. The procedure was repeated in cases of suboptimal TIMI flow (<3) or significant residual thrombus.
Study End Point
The primary efficacy endpoint was a composite of major adverse cardiovascular and cerebrovascular events (MACCE), including all-cause death, recurrent myocardial infarction, and stroke. Secondary efficacy endpoints included hospitalization for heart failure, rehospitalization for unstable angina, and target vessel revascularization. Safety endpoints comprised any bleeding event and major bleeding, defined as Bleeding Academic Research Consortium (BARC) types 3 to 5. 10
Prospective clinical surveillance was conducted for all patients at 1, 6, and 12 months. To overcome geographical constraints, participants from remote locales were followed up through structured telephone calls.
Statistical Analysis
The data were analyzed by SPSS version 26.0 for window (SPSS Inc., Chicago, IL, USA). Categorical variables were summarized as frequencies (percentages) and compared using the Chi-square or Fisher's exact test, as appropriate. Continuous variables were assessed for normality with the Shapiro-Wilk test and are presented as mean ± standard deviation for normally distributed data or median (IQR) for non-normally distributed data.
To minimize selection bias and control for potential confounding factors in this non-randomized observational study, we employed propensity score matching (PSM) to create comparable groups of patients who received AngioJet rheolytic thrombectomy plus GPI (the AT + GPI group) versus those who received routine treatment (the RT group). The variables used for matching included gender, age, body mass index, history of diabetes mellitus, history of hypertension, history of dyslipidemia, current smoking, previous myocardial infarction, previous PCI, killip class, delayed PCI, IABP, GPI. Patients in the AT + GPI group were matched 1:1 to patients in the RT group using nearest-neighbor matching without replacement, with a caliper width of 0.02 of the standard deviation of the logit of the propensity score.
Survival analyses were performed using Kaplan-Meier estimates with the log-rank test. To quantify the association between treatment and time-to-event outcomes, we initially calculated unadjusted hazard ratios (HRs) with 95% confidence intervals (CIs) using univariable Cox proportional hazards models. However, recognizing the potential for residual confounding even after PSM, we conducted multivariable Cox regression analyses as a prespecified sensitivity analysis. The multivariable models were adjusted for covariates that remained imbalanced after matching (standardized mean difference >10%) or were considered clinically paramount, including history of hypertension, current smoking status, Killip class, and age.”
Results
Baseline Characteristic
Between October 2014 and April 2019, a total of 877 consecutive patients with STEMI were enrolled from the Sixth Medical Center of the Chinese People's Liberation Army General Hospital. Of these, 100 patients who did not perform PCI were excluded. Five cases were lost to follow-up. Of the 772 STEMI patients, 97 were treated with AngioJet rheolytic thrombectomy and GPI. After propensity score matching, 97 well-matched patients were selected for each group. The flow of patient selection, exclusion, and the creation of the propensity-matched cohorts is detailed in Figure 1. (Figure 1).

Flow-chart of patient screening. STEMI: ST-segment elevation myocardial infarction, PCI: percutaneous coronary intervention, AT: AngioJet rheolytic thrombectomy, GPI: glycoprotein IIb/IIIa inhibitor, RT: routine treatment.
The baseline clinical characteristics of the study population, both pre- and post-propensity-score matching, are detailed in Table 1. Compared to the RT group, patients in the AT + GPI group were younger, more likely to be male, and demonstrated higher levels of admission and peak troponin and creatine kinase-MB. They also had significantly elevated hemoglobin, estimated glomerular filtration rate, and brain natriuretic peptide. Conversely, delayed PCI and IABP use were more common in the RT group. Following propensity score matching, the baseline characteristics, in-hospital laboratory profiles, and medication strategies were well-balanced between the two groups, with no statistically significant differences (Tables 1 and 2). The standardized mean differences is demonstrated in Table 3 and the accompanying balance plot (Supplementary Figure S1). Critical clinical imbalances present in the unmatched cohorts, particularly in the prevalence of delayed PCI and IABP support, were successfully corrected. The post-matching standardized mean differences were all <10%, with the exception of smoking status (12.4%) and the history of hypertension (−12.36%).
Baseline Characteristics Before and After Propensity-Score Matching.
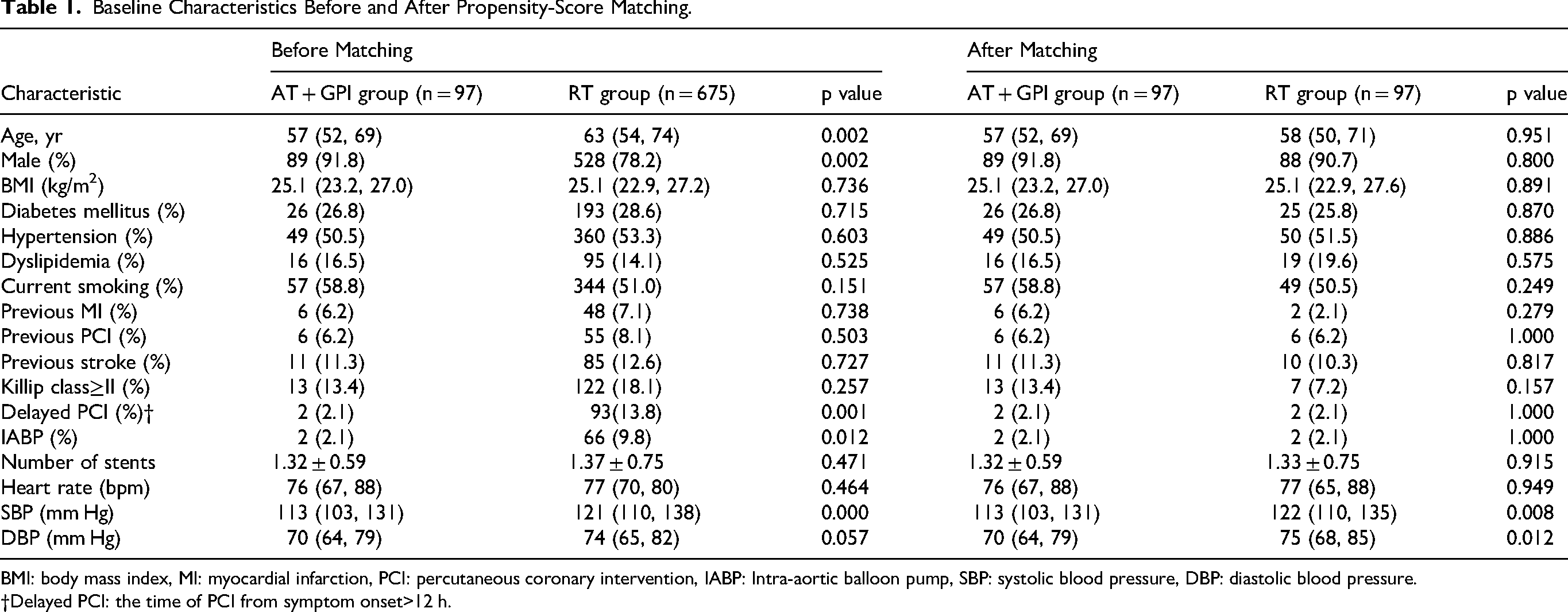
BMI: body mass index, MI: myocardial infarction, PCI: percutaneous coronary intervention, IABP: Intra-aortic balloon pump, SBP: systolic blood pressure, DBP: diastolic blood pressure.
†Delayed PCI: the time of PCI from symptom onset>12 h.
In-Hospital Data Before and After Propensity-Score Matching.

cTnI: cardiac troponin I, CK-MB: creatine kinase-MB, eGFR: estimated glomerular filtration rate, TC: total cholesterol, TG: triglyceride, HDL: high-density lipoprotein, LDL: low-density lipoprotein, INR: international normalized ratio, BNP: Brain natriuretic peptide, PPI: proton pump inhibitor, ACEi: angiotensin-converting enzyme inhibitor, ARB: angiotensin receptor, MRA: mineralocorticoid receptor antagonist, GPI: glycoprotein IIb/IIIa inhibitors, LVEF: left ventricular ejection fraction.
Standardized Mean Differences of Baseline Covariates Before and After Propensity Score Matching.

BMI: body mass index, MI: myocardial infarction, PCI: percutaneous coronary intervention, †Delayed PCI: the time of PCI from symptom onset>12 h, GPI: glycoprotein IIb/IIIa inhibitors, IABP: Intra aortic balloon pump.
Clinical Outcomes
No significant differences were observed between the two groups regarding in-hospital mortality, reinfarction, or stent thrombosis. However, the incidence of in-hospital heart failure was significantly lower in the AT + GPI group than in the RT group (7.2% vs 16.3%, p = 0.02). In terms of safety endpoints, the rates of bleeding were comparable between the groups. After propensity score matching, the balanced cohorts continued to show no significant differences in the composite of in-hospital major adverse cardiovascular events, or bleeding (Table 4).
In-Hospital Events Before and After Propensity-Score Matching.

Clinical outcomes of the 1-year follow-up before and after propensity matching are shown in Table 5. There was no significant different in the cumulative incident of MACCE between the AT + GPI group and the RT group (8.2% vs 13.3%, hazard ratio, 0.609; 95% CI, 0.295 to 1.254; P = 0.178). Similarly, the incidence rates of all individual endpoints—including death, recurrent myocardial infarction, stroke, heart failure, rehospitalization, target vessel revascularization, and bleeding—showed no significant differences between the two groups. Following propensity score matching, no significant difference in MACCE incidence was observed between the AT + GPI and RT groups (8.2% vs 9.3%; hazard ratio, 0.894; 95% CI, 0.345 to 2.318; p = 0.818).
Clinical Outcomes at 1 Year Before and After Propensity-Score Matching.

MACCE: major adverse cardiovascular and cerebrovascular events, MI: myocardial infarction, TVR: Target vessel revascularization, BARC: Bleeding Academic Research Consortium.
Kaplan–Meier Curves for Death from Any Cause are showed in the Figure 2. The survival curves demonstrated no significant difference over the 1-year follow-up period. The log-rank test showed no statistically significant difference in survival distribution between groups (χ2 = 0.736, p = 0.391). Kaplan-Meier curves for freedom from MACCE over the 1-year follow-up are presented in Figure 3. The curves showed no significant separation between groups (χ2 = 0.053, p = 0.818).
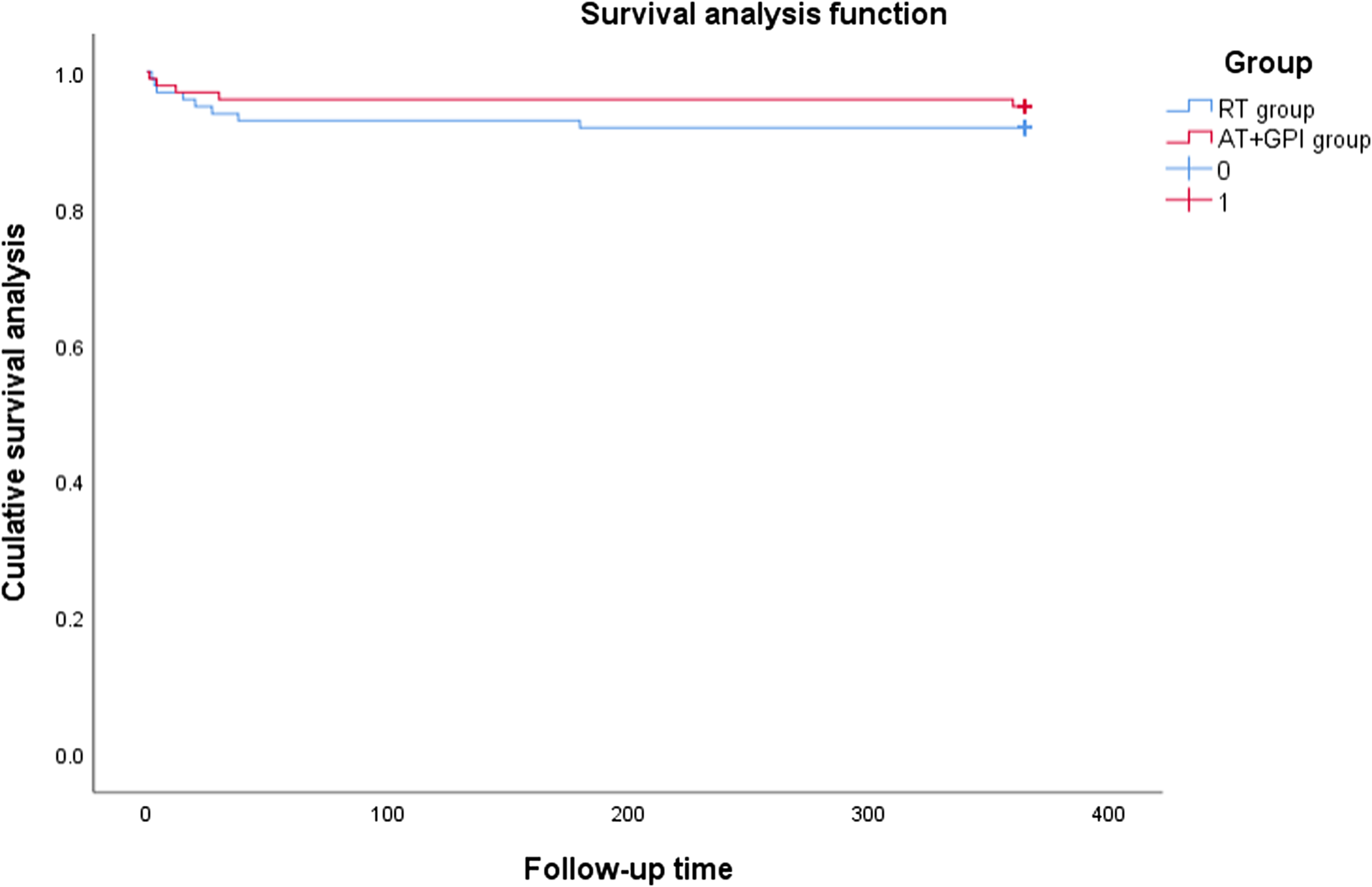
Kaplan-Meier curves for death from any cause.

Kaplan-Meier curves for MACCE.
Discussion
This propensity-matched analysis found that, among a higher-risk AMI population where thrombectomy was clinically considered, the addition of AngioJet rheolytic thrombectomy to GPI therapy was not associated with significantly better 1-year outcomes compared with routine treatment group. We observed no statistically significant differences in the rates of the composite MACCE endpoint, its individual components, or the measured safety outcomes of stroke and bleeding.
For patients with a high thrombus burden, thrombus aspiration may theoretically decrease the thrombus load, reduce distal embolization rates, and promote TIMI 3 flow restoration. However, large-scale randomized controlled trials have demonstrated that routine thrombus aspiration does not improve clinical outcomes in patients with STEMI.11,12 The TOTAL trial found that thrombus aspiration was associated with a significantly higher risk of stroke at 30 days compared with PCI alone (0.7% vs 0.3%, P = 0.02). 11 Taglieri et al conducted a meta-analysis of 25 randomized controlled trials, which revealed that thrombus aspiration combined with primary PCI was associated with an increased risk of stroke (OR 1.401, 95% CI 1.004-1.954; P = 0.047), although this association does not appear to be particularly strong. 13 Therefore, manual thrombus aspiration should not be routinely recommended during primary PCI given lack of clinical benefit (class III, 2025 American College of Cardiology/American Heart Association guidelines). 14
The increased risk of stroke associated with manual thrombus aspiration may stem from incomplete thrombus removal, which can cause thrombus fragmentation and subsequent systemic embolization. The AngioJet device employs high-velocity saline jets to fragment and aspirate thrombus. 7 The JETSTENT trial demonstrated that in patients with acute myocardial infarction and high thrombus burden, AngioJet thrombectomy prior to direct stenting improves myocardial perfusion and may lead to long-term clinical benefits. 15 Conversely, the AiMI trial demonstrated that AngioJet thrombus aspiration did not improve clinical outcomes in STEMI patients. 16 Huang et al conducted a study in patients with acute myocardial infarction characterized by TIMI thrombus grade 5, demonstrating that AngioJet thrombus aspiration combined with PCI did not improve 1-year major adverse cardiovascular events compared with PCI alone, nor did it increase the incidence of stroke. 17 The notable discrepancies in these findings may be attributable to variations in study design, limited sample sizes, operator technique, and patient selection bias. In recent years, novel mechanical thrombectomy devices have been increasingly explored in STEMI patients.18,19 The impact of these aspiration devices on clinical outcomes in STEMI warrants further validation through large-scale randomized controlled trials.
The clinical application of intravenous GPI has been downscaled despite their rapid antiplatelet effect, given the widespread use of potent P2Y12 inhibitors. The guideline recommendations now reserve their use for specific scenarios including large thrombus burden, no-reflow, or slow flow. 14 Calburean et al performed a study of 1210 STEMI patients with a median follow-up 2.78 years, demonstrating that ticagrelor consistently reduced cardiovascular and all-cause mortality, while eptifibatide reduced only cardiovascular mortality [HR = 0.72 (0.57-0.92), p = 0.002, and HR = 0.68 (0.52-0.89), p = 0.001, respectively], while manual thrombus aspiration provided no long-term benefit. 20 The CCC-ACS Project of China found that thrombus aspiration combined with GPI was associated with a reduction in ischemic events (OR: 0.27, 95% CI: 0.08 to 0.98) among patients aged < 60 years, and no significant increase in major bleeds was observed. 5 Our study found that the combination of AngioJet Rheolytic thrombectomy and GPI provided no additional benefit in STEMI patients. Whether a theoretical “ceiling effect” of potent antiplatelet therapy might limit the measurable incremental benefit of adjunctive thrombectomy is a hypothesis that requires testing in larger, targeted studies. Ahn et al evaluated the microvascular obstruction by cardiac magnetic resonance found that combination treatment using intracoronary abciximab and aspiration thrombectomy may synergistically improve myocardial perfusion in patients with STEMI. However, the sample size included in this study was relatively limited. 21 Thus, additional studies on thrombus aspiration combined with microvascular protection strategies warrant further investigation.
Regarding safety outcomes, our study revealed that AngioJet Rheolytic thrombectomy combined with GPI did not increase the risk of stroke or bleeding. The underlying mechanism likely involves its effective thrombus resolution capability, rather than physically retrieving intact thrombi like manual techniques, thereby reducing the potential for systemic embolization through thrombus fragmentation. Accordingly, future research should clarify the optimal indications and operational techniques for thrombus aspiration. Efforts could focus on specific patient populations (such as those with large thrombus burden, delayed PCI, stent thrombosis, or embolic myocardial infarction), specific procedural timing (before or after balloon angioplasty, before or after stent implantation, or following no-reflow phenomenon). The development of standardized operational procedures for thrombus aspiration, refinement of techniques, and advancement of novel thrombus aspiration devices will better improve the outcomes of patients with STEMI.
Although data on concomitant oral anticoagulant (OAC) use were captured (present in 2.1% of the AT + GPI group vs 0% in controls), its low prevalence precluded meaningful analysis. Our cohort therefore does not reflect the increasing real-world population of AMI patients on chronic OAC, a known high-bleeding-risk group, 22 and the safety of the combined regimen under triple therapy remains unaddressed.
Several limitations in our study should be acknowledged. First, this was a retrospective, non-randomized study conducted at a single center. The decision to perform AngioJet thrombectomy was based on operator judgment, which inherently introduces substantial confounding by indication. Patients selected for AngioJet likely represented a “treatment-of-last-resort” or higher-risk cohort with more severe presentations (eg, greater thrombus burden, compromised flow) that prompted the operator to adopt adjunctive therapy. Although we employed propensity score matching to balance measurable baseline characteristics, it cannot fully adjust for unmeasured or nuanced factors influencing the clinical decision, such as detailed angiographic thrombus grade, coronary anatomy complexity, and subtle hemodynamic instability. Despite matching, minimal residual imbalances persisted for hypertension history and smoking status (post-matching SMD >10%), which may represent sources of unmeasured confounding. Second, the relatively small sample size, particularly after matching, may have limited the statistical power to detect clinically relevant differences in secondary endpoints or subgroup analyses. A post-hoc power analysis for the observed difference in MACCE rates (8.2% vs 9.3%) revealed a statistical power of merely 5.8%, highlighting the study's inherent limitation in detecting small inter-group differences. This necessitates a guarded interpretation of the negative primary outcome. Third, the assessment of thrombus burden and procedural outcomes relied on operator assessment rather than core laboratory adjudication, which might have introduced assessment bias. Furthermore, we lacked objective measures of microvascular perfusion (eg, ST-segment resolution, myocardial blush grade), which are critical for evaluating the mechanistic efficacy of thrombectomy. Fourth, operator experience, a known critical factor influencing the prognosis of PCI for STEMI, 23 was not systematically collected and could represent an additional source of bias. Finally, our study period (2014-2019) spans years of ongoing evolution in STEMI care. During this time, practices such as radial artery access, potent P2Y12 inhibitor use, and refined stent techniques became more standardized and widespread. While we adjusted for some factors, the gradual improvement in overall PCI quality and peri-procedural management over time may have attenuated potential differences between the treatment strategies and limits the direct applicability of our results to contemporary practice, which may feature even more optimized background therapy.
Within the context of these limitations—including its observational design, operator-dependent intervention, and evolving treatment landscape—this analysis did not observe a clinical benefit for adjunctive AngioJet thrombectomy over routine treatment in a selected high-risk cohort. Future large-scale, randomized trials are needed to definitively assess the role of rheolytic thrombectomy in the contemporary PCI era.
Conclusion
In this observational study of STEMI patients, the strategy of combining AngioJet rheolytic thrombectomy with GPI was not associated with improved 1-year outcomes compared to routine treatment, though it did not increase stroke or bleeding risk.
Supplemental Material
sj-docx-1-cat-10.1177_10760296261439485 - Supplemental material for AngioJet Rheolytic Thrombectomy Combined with Glycoprotein IIb/IIIa Inhibitors in Acute Myocardial Infarction: An Observational Study
Supplemental material, sj-docx-1-cat-10.1177_10760296261439485 for AngioJet Rheolytic Thrombectomy Combined with Glycoprotein IIb/IIIa Inhibitors in Acute Myocardial Infarction: An Observational Study by Yi-xiong Huang, MD, Yi Cao, MD, Yu Chen, MD, PhD, Yi-gang Qiu, MD, Ying-ming Liu, MD, Jiang-chun He, MD, Li Zhao, MD, PhD, and Yong Xu, MD, PhD in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.