
Abstract
Background
Oral anticoagulants (OACs) remain the standard strategy for stroke prevention in atrial fibrillation (AF) but are limited by bleeding risk, intolerance, and long-term adherence challenges. Left atrial appendage closure (LAAC) has emerged as a catheter-based alternative for thromboembolic prevention in non-valvular AF. This systematic review evaluated the comparative efficacy and safety of LAAC versus OAC therapy in patients with AF.
Methods
PubMed and Embase were systematically searched for randomized controlled trials (RCTs) comparing percutaneous LAAC with OACs, including direct oral anticoagulants (DOACs) and warfarin, in patients with AF.
Results
Four pivotal randomized trials (PROTECT AF, PREVAIL, PRAGUE-17, and OPTION) were included. Compared with DOAC therapy, LAAC demonstrated non-inferiority for the composite endpoint of all-cause death, stroke, or systemic embolism in OPTION and for the primary composite outcome in PRAGUE-17. LAAC was associated with significantly lower non-procedural bleeding compared with DOACs in OPTION and PRAGUE-17. Compared with warfarin, LAAC achieved non-inferiority for ischemic stroke or systemic embolism beyond 7 days after randomization in PREVAIL and reduced long-term cardiovascular mortality in PROTECT AF. Procedure-related complications declined with increasing operator experience.
Conclusion
LAAC provides non-inferior thromboembolic protection compared with OAC therapy while reducing long-term bleeding events in selected patients with AF. LAAC represents an important alternative for patients at elevated bleeding risk or with contraindications to long-term anticoagulation.
Introduction
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia worldwide and is associated with a substantially increased risk of thromboembolic complications, particularly ischemic stroke and systemic embolism. 1 Oral anticoagulants (OACs), including vitamin K antagonists (VKAs) and direct oral anticoagulants (DOACs), constitute the cornerstone of stroke prevention in patients with AF and are strongly recommended by contemporary international guidelines.2-4 Despite their proven efficacy, long-term OAC therapy is constrained by several clinically important limitations, including an increased risk of major and clinically relevant non-major bleeding, drug–drug and drug–food interactions, the requirement for routine monitoring with VKAs, and suboptimal long-term adherence associated with treatment burden and adverse effects. Moreover, a considerable proportion of patients with AF either have contraindications to chronic anticoagulation or discontinue therapy prematurely because of bleeding concerns or intolerance, thereby remaining insufficiently protected against thromboembolic events. These challenges are particularly relevant in patients with concomitantly elevated thromboembolic and bleeding risks and have stimulated growing interest in alternative non-pharmacological approaches for stroke prevention in AF.
Left atrial appendage closure (LAAC) has emerged as a non-pharmacological, mechanical alternative to OAC therapy by targeting the left atrial appendage (LAA), the predominant site of thrombus formation in non-valvular AF. Early randomized controlled trials (RCTs), including PROTECT AF and PREVAIL,5-7 demonstrated that percutaneous LAAC using the Watchman device was non-inferior to warfarin for the prevention of stroke, systemic embolism, and cardiovascular death. Long-term follow-up analyses further suggested reductions in hemorrhagic stroke, disabling or fatal bleeding, and cardiovascular mortality with LAAC compared with warfarin therapy. These pivotal studies established the initial evidence base supporting LAAC as a therapeutic option for selected patients with AF, particularly those considered unsuitable for long-term anticoagulation or at increased risk of bleeding complications.
Subsequent advances in device technology, procedural techniques, and post-procedural antithrombotic strategies have substantially expanded the role of LAAC in contemporary clinical practice. More recent RCTs,8-10 including PRAGUE-17 and OPTION, have directly compared LAAC with contemporary medical therapy based predominantly on DOACs. Nevertheless, uncertainties persist regarding the relative efficacy and safety of LAAC compared with OACs across heterogeneous patient populations, evolving procedural techniques, and different device platforms. Therefore, the present systematic review aims to integrate evidence from pivotal RCTs to critically evaluate the clinical outcomes of LAAC versus OAC therapy in patients with AF.
Methods
Literature Search
A comprehensive search was systematically performed in PubMed and Embase up to January 2026 without language restrictions. The search strategy combined Medical Subject Headings (MeSH) terms and free-text keywords related to atrial fibrillation, left atrial appendage closure, oral anticoagulants, direct oral anticoagulants, vitamin K antagonists, and randomized controlled trials. The detailed search strategy was developed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations to maximize sensitivity and minimize the risk of missing relevant studies. Additionally, reference lists of relevant reviews11-15 and eligible studies were manually screened to identify potentially eligible publications not captured through the electronic database search.
Eligibility Criteria
Studies were selected based on the following criteria: 1) Population: Adult patients with non-valvular AF, regardless of AF subtype (paroxysmal, persistent, or permanent). 2) Intervention: LAAC using commercially available or clinically approved devices, including but not limited to the Watchman, Watchman FLX, Amulet, or other contemporary LAAC systems. 3) Comparison: OAC therapy, including DOACs (e.g., apixaban, rivaroxaban, dabigatran, edoxaban)16-21 or VKAs such as warfarin. 4) Outcomes: clinically relevant efficacy and/or safety outcomes, such as stroke, systemic embolism, cardiovascular death, all-cause mortality, major bleeding, or clinically relevant non-major bleeding. 4) Study Design: RCTs.
Studies were excluded if they were observational cohort studies, case reports, case series, reviews, meta-analyses, editorials, letters, conference abstracts without full peer-reviewed publication, or studies lacking a direct comparison between LAAC and OAC therapy. When multiple publications originated from the same trial population, the report with the longest follow-up duration, most comprehensive outcome data, or largest sample size was retained to avoid duplication of data.
Study Selection and Data Extraction
Study selection was independently performed by two reviewers in a two-stage process consisting of title/abstract screening followed by full-text assessment of potentially eligible articles. Disagreements regarding study eligibility were resolved through consensus discussion, and a third reviewer was consulted when necessary.
Extracted variables included study characteristics (trial name, publication year, study design, sample size, and follow-up duration), baseline patient demographics (mean age, sex distribution, CHA2DS2-VASc score, HAS-BLED score, AF subtype, prior stroke or transient ischemic attack, and prior bleeding history), intervention-related characteristics (type of LAAC device, procedural strategy, post-procedural antithrombotic regimen), comparator-related characteristics (type of OAC therapy and prior anticoagulation exposure), and reported efficacy and safety outcomes.
Risk of Bias Assessment
The methodological quality of included studies was evaluated using the Cochrane Risk of Bias 2 (RoB 2) tool, 22 which evaluates potential bias across five predefined domains: bias arising from the randomization process, bias due to deviations from intended interventions, bias related to missing outcome data, bias in outcome measurement, and bias in the selection of reported results. Each domain was classified as “low risk of bias,” “some concerns,” or “high risk of bias” according to the RoB 2 guidance framework. Risk-of-bias assessment was independently performed by two reviewers, with disagreements resolved through discussion and consensus.
Data Synthesis
Given the substantial heterogeneity among the included trials with respect to patient risk profiles, inclusion criteria, LAAC device platforms, comparator anticoagulation regimens, procedural techniques, follow-up duration, endpoint definitions, and post-implantation antithrombotic strategies, formal quantitative pooling through meta-analysis was considered methodologically inappropriate and potentially misleading. Furthermore, the relatively limited number of available RCTs and the variability in outcome reporting further constrained the robustness of pooled statistical estimates. Therefore, a narrative synthesis approach was adopted to qualitatively integrate the available evidence.
Results
Study Selection
The study selection process is summarized in Figure 1. A comprehensive search across the PubMed and Embase databases yielded a total of 841 potentially relevant studies. After eliminating duplicates, 611 unique records were retained for initial screening based on titles and abstracts. Of these, 11 studies were identified as potentially eligible for inclusion. Upon full-text review, 7 studies were excluded because they represented post hoc analyses, secondary analyses, or subgroup analyses derived from previously published RCTs. Ultimately, four RCTs6-9 (OPTION, PRAGUE-17, PREVAIL, and PROTECT AF) were selected for inclusion in this review. The flow diagram of study selection process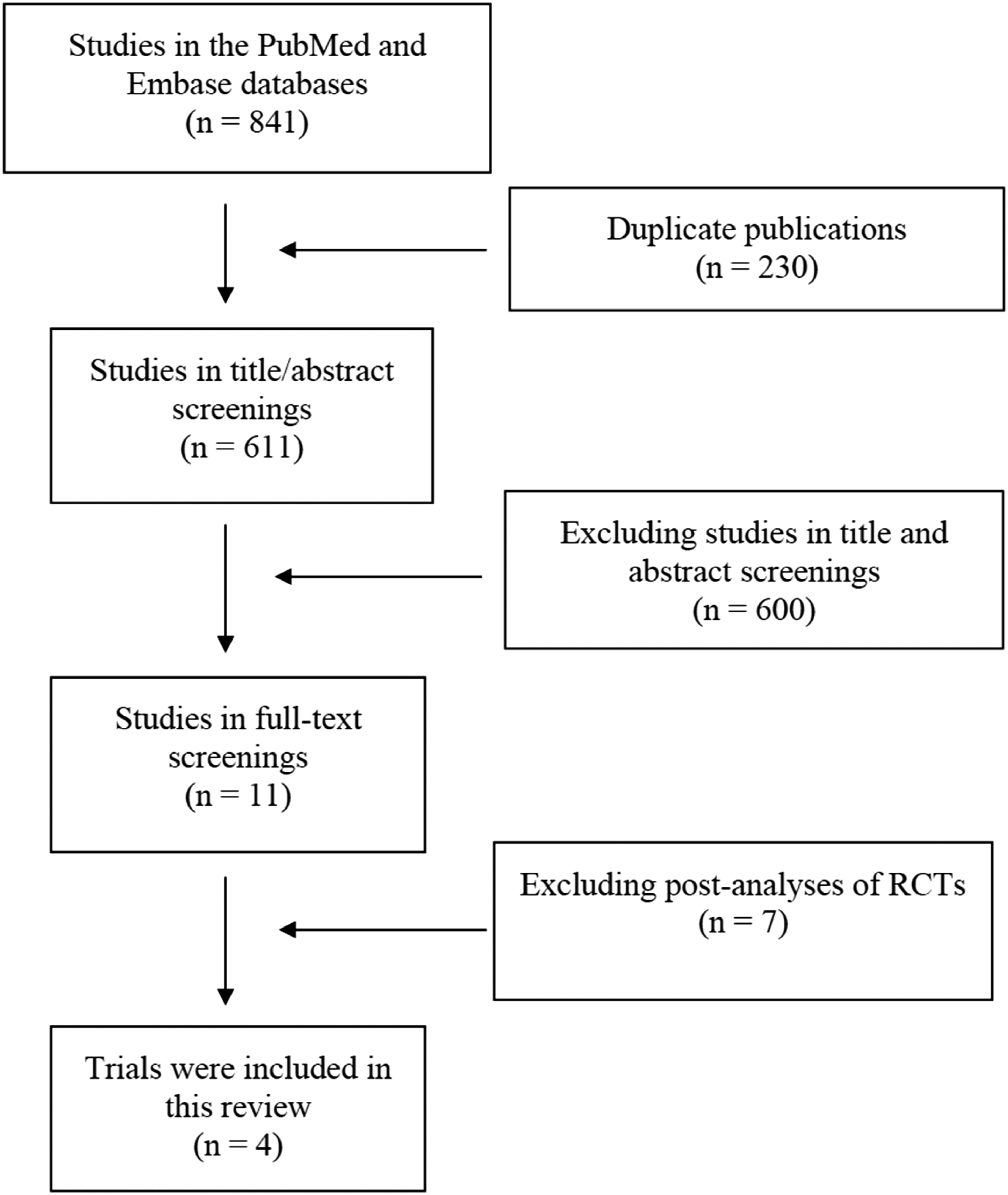
Baseline Characteristics
Baseline Characteristics of the Included Trials
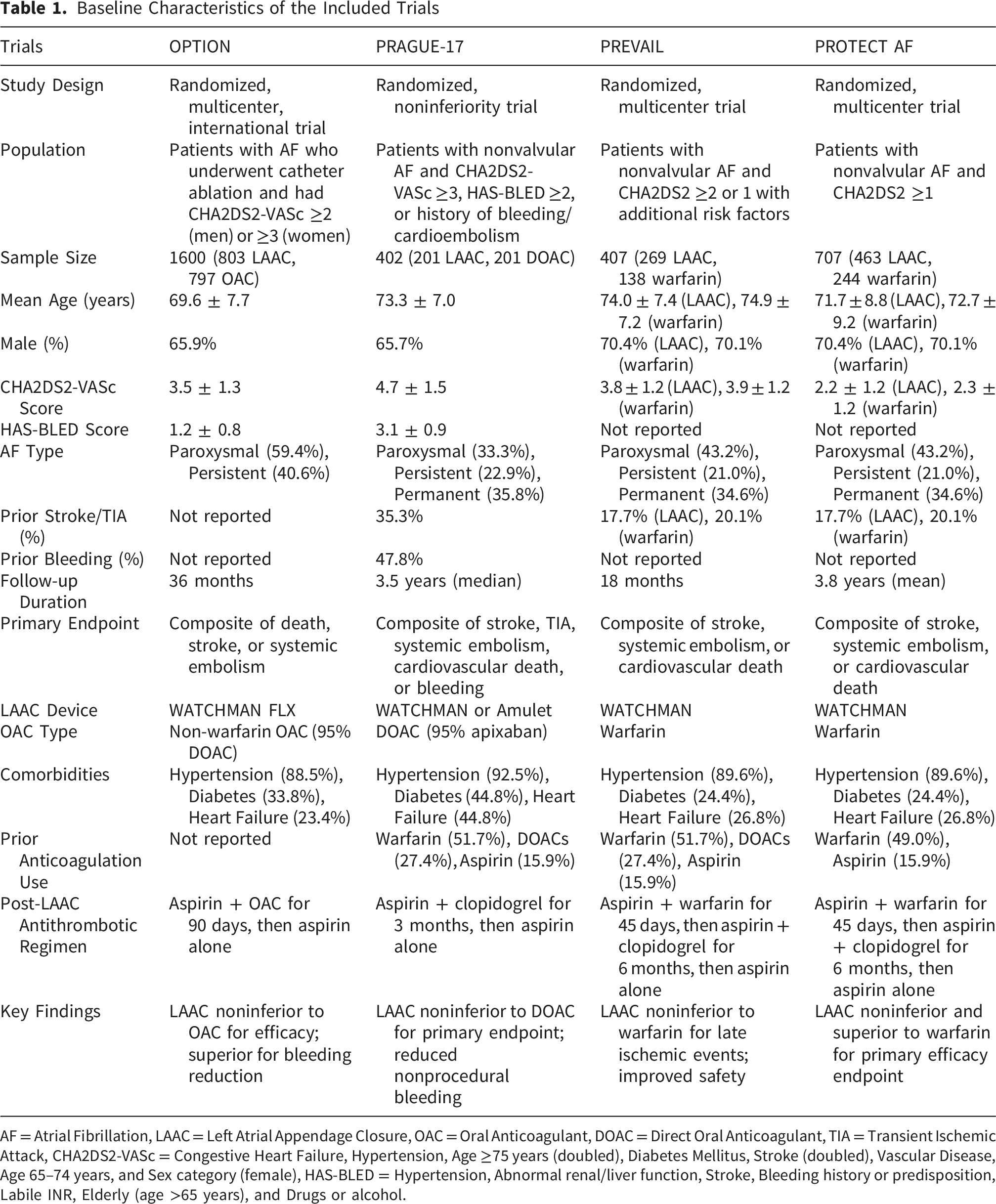
AF = Atrial Fibrillation, LAAC = Left Atrial Appendage Closure, OAC = Oral Anticoagulant, DOAC = Direct Oral Anticoagulant, TIA = Transient Ischemic Attack, CHA2DS2-VASc = Congestive Heart Failure, Hypertension, Age ≥75 years (doubled), Diabetes Mellitus, Stroke (doubled), Vascular Disease, Age 65–74 years, and Sex category (female), HAS-BLED = Hypertension, Abnormal renal/liver function, Stroke, Bleeding history or predisposition, Labile INR, Elderly (age >65 years), and Drugs or alcohol.
Baseline clinical characteristics were generally well balanced between the LAAC and OAC groups within each trial, thereby supporting the internal validity and comparability of treatment effects. The included RCTs were multinational in design and incorporated both high-volume and less-experienced procedural centers, reflecting real-world variability in operator expertise and procedural practice. Follow-up duration ranged from approximately 18 months to 3.8 years. Assessment using the Cochrane RoB 2 tool demonstrated an overall low risk of bias across the included studies, supporting the methodological robustness of the available randomized evidence.
Efficacy and Safety Outcomes of LAAC versus DOACs and Warfarin

AF = Atrial Fibrillation, LAAC = Left Atrial Appendage Closure, OAC = Oral Anticoagulant, DOAC = Direct Oral Anticoagulant, TIA = Transient Ischemic Attack, CV = Cardiovascular.
Efficacy and Safety of LAAC Versus DOACs
Efficacy
The OPTION and PRAGUE-17 trials provided the principal randomized evidence comparing LAAC with contemporary DOAC-based therapy. In the OPTION trial, LAAC demonstrated non-inferiority to DOAC therapy for the primary efficacy endpoint, defined as a composite of all-cause death, stroke, or systemic embolism at 36 months. Event rates were 5.3% in the LAAC group and 5.8% in the DOAC group, meeting the prespecified criterion for non-inferiority. Importantly, patients enrolled in OPTION had recently undergone catheter ablation for AF, which may limit extrapolation of these findings to broader non-ablation AF populations.
Similarly, the PRAGUE-17 trial demonstrated non-inferiority of LAAC compared with DOAC therapy for the composite endpoint of stroke or transient ischemic attack, systemic embolism, clinically significant bleeding, cardiovascular death, or procedure-/device-related complications during a median follow-up of 3.5 years (subdistribution hazard ratio [sHR], 0.81; 95% confidence interval [CI], 0.56–1.18). Collectively, these findings suggest that LAAC provides overall clinical efficacy comparable to contemporary DOAC therapy while reducing long-term bleeding events in selected patients with AF.
Safety
Both OPTION and PRAGUE-17 demonstrated favorable bleeding outcomes with LAAC compared with long-term DOAC therapy. In OPTION, the incidence of non–procedure-related major or clinically relevant nonmajor bleeding was significantly lower in the LAAC group than in the DOAC group (8.5% vs. 18.1%). Similarly, PRAGUE-17 reported a significant reduction in nonprocedural clinically relevant bleeding with LAAC (sHR, 0.55; 95% CI, 0.31–0.97).
Nevertheless, procedural and device-related complications remained important considerations in patients undergoing LAAC. In OPTION, device-related thrombus or hypoattenuated device thickening was identified in approximately 1.9% of patients during follow-up imaging. In PRAGUE-17, procedure-related complications occurred in 2.2% of patients. Reported complications included pericardial effusion, vascular complications, device embolization, and device-related thrombosis. These findings underscore the trade-off between the long-term reduction in bleeding events associated with LAAC and the early procedural risks inherent to device implantation. Overall, the available evidence suggests that LAAC offers a favorable long-term safety profile compared with DOAC therapy, particularly with respect to bleeding reduction.
Efficacy and Safety of LAAC Versus Warfarin
Efficacy
The PREVAIL and PROTECT AF trials established the foundational randomized evidence comparing LAAC with warfarin therapy. In PREVAIL, LAAC achieved non-inferiority to warfarin for the prevention of ischemic stroke or systemic embolism occurring beyond 7 days after randomization. However, non-inferiority was not achieved for the broader composite endpoint of stroke, systemic embolism, and cardiovascular or unexplained death, largely attributable to unexpectedly low event rates in the warfarin arm and consequent limitations in statistical power.
In contrast, the PROTECT AF trial demonstrated non-inferiority of LAAC compared with warfarin for the composite endpoint of stroke, systemic embolism, and cardiovascular death. Long-term pooled follow-up analyses from PROTECT AF and PREVAIL further suggested potential superiority of LAAC, particularly with respect to cardiovascular and all-cause mortality. These findings provided important proof-of-concept evidence supporting LAAC as a viable alternative to long-term warfarin therapy for stroke prevention in AF.
Safety
The procedural safety profile of LAAC improved substantially over time across successive trials. In PREVAIL, the rate of early safety events, including pericardial effusion requiring intervention, device embolization, and procedure-related stroke, was reduced to 2.2%, meeting the predefined procedural safety target and reflecting improvements in operator experience and device technology.
In PROTECT AF, higher rates of early procedural complications were initially observed, including pericardial effusion requiring intervention (4.8%) and procedure-related ischemic stroke (1.3%). However, complication rates progressively declined with increasing procedural experience, highlighting the presence of an operator learning curve in LAAC implantation. Despite these early procedural risks, long-term follow-up analyses demonstrated lower rates of hemorrhagic stroke and cardiovascular mortality with LAAC compared with warfarin therapy. These findings suggest that improvements in procedural expertise and device technology have progressively enhanced the long-term safety profile of LAAC.
Discussion
This systematic review synthesizes evidence from four pivotal RCTs6-9 comparing LAAC with OAC therapy in patients with AF. The available evidence demonstrates that LAAC provides thromboembolic protection broadly comparable to that achieved with both DOACs and warfarin. In the OPTION and PRAGUE-17 trials, LAAC was non-inferior to DOAC-based therapy for major composite efficacy endpoints that included stroke, systemic embolism, cardiovascular death, or clinically relevant bleeding. Similarly, the PREVAIL and PROTECT AF trials established non-inferiority of LAAC compared with warfarin, while long-term follow-up from PROTECT AF suggested potential superiority with respect to cardiovascular and all-cause mortality. More contemporary evidence from the CHAMPION-AF trial 23 further extended these observations to patients considered suitable for long-term anticoagulation, demonstrating that LAAC was non-inferior to DOAC therapy for the prevention of cardiovascular death, stroke, or systemic embolism, while significantly reducing non–procedure-related bleeding events. Collectively, these findings support the concept that LAAC represents a viable non-pharmacological alternative to chronic anticoagulation in selected patients with AF.
The mechanistic rationale for LAAC is biologically compelling. In non-valvular AF, the LAA is the predominant site of intracardiac thrombus formation, accounting for the majority of cardioembolic strokes. By mechanically excluding the LAA from systemic circulation, LAAC directly targets the principal anatomical substrate responsible for thromboembolism in AF. Unlike OAC therapy, which reduces thrombogenicity systemically, LAAC eliminates dependence on long-term anticoagulant exposure and thereby avoids many of the limitations associated with chronic pharmacological therapy, including cumulative bleeding risk, adherence challenges, drug interactions, and anticoagulation intolerance.
One of the most clinically important findings across the included RCTs is the consistent reduction in long-term bleeding events associated with LAAC. In OPTION, LAAC substantially reduced the incidence of non–procedure-related major bleeding or clinically relevant non-major bleeding compared with DOAC therapy. Similar reductions in clinically relevant bleeding were observed in PRAGUE-17. In the earlier warfarin-based trials, LAAC was additionally associated with lower rates of hemorrhagic stroke and cardiovascular mortality during long-term follow-up. These observations are clinically meaningful because bleeding complications remain one of the principal determinants of morbidity, mortality, and treatment discontinuation in anticoagulated patients with AF. Importantly, the long-term bleeding advantage of LAAC appears to emerge after the early peri-procedural period, when the one-time procedural risk has been surpassed and chronic anticoagulant exposure is avoided.
Nevertheless, LAAC is not devoid of procedural and device-related risks. Across the included trials, complications such as pericardial effusion, device embolization, vascular access complications, and procedure-related ischemic stroke were observed, particularly in earlier studies. Device-related thrombus and residual peri-device leaks also remain clinically relevant concerns because they may contribute to residual thromboembolic risk after implantation. However, procedural safety has improved substantially over time, reflecting advances in device design, imaging guidance, operator experience, and post-procedural management strategies. In PREVAIL, for example, the rate of early safety events was markedly lower than that reported in PROTECT AF, illustrating the impact of procedural learning curves and technological refinement. Contemporary next-generation devices, including the Watchman FLX platform, appear to provide improved procedural success and lower complication rates compared with earlier-generation systems, although longer-term comparative data remain limited.
Despite the overall favorable efficacy profile of LAAC, several important considerations warrant careful interpretation. Although early trials demonstrated non-inferiority relative to warfarin, ischemic stroke rates were numerically higher in the device arm during the peri-procedural phase in some studies, reflecting both procedural risk and incomplete endothelialization during the early post-implantation period. More recent comparisons with DOACs, including CHAMPION-AF, 23 similarly suggest that the reduction in long-term bleeding may be accompanied by a small absolute increase in ischemic stroke risk. This trade-off highlights the fundamentally different mechanisms underlying LAAC and systemic anticoagulation: whereas OAC therapy continuously suppresses thrombogenesis throughout the cardiovascular system, LAAC primarily addresses thrombus formation originating from the LAA and may not fully mitigate non-LAA or non-cardioembolic sources of stroke. Accordingly, LAAC should not be interpreted as a universally superior strategy to OAC therapy but rather as an alternative therapeutic approach whose benefits and limitations vary according to individual patient characteristics.23-25
From a clinical perspective, these findings reinforce the importance of individualized patient selection and shared decision-making. Current international guidelines primarily recommend LAAC for patients with contraindications to long-term anticoagulation, previous major bleeding, or unacceptably high bleeding risk. DOAC therapy remains the preferred first-line strategy for most patients eligible for anticoagulation because of its extensive evidence base, ease of administration, and favorable overall efficacy–safety profile. Routine adoption of LAAC in younger or lower-risk populations is not currently supported, particularly given the limited availability of very long-term durability data and the potential need for future device-related surveillance. Therefore, decisions regarding LAAC should incorporate multiple clinical considerations, including thromboembolic risk, bleeding history, frailty, renal function, procedural risk, anticipated life expectancy, patient preference, and local procedural expertise.
Limitations
Several limitations should be acknowledged. First, most included trials predominantly enrolled patients with paroxysmal or persistent AF, thereby limiting extrapolation to patients with permanent or long-standing persistent AF, in whom atrial remodeling and non-LAA thromboembolic mechanisms may be more prominent. Second, the number of available randomized trials remains relatively limited, and several studies enrolled modest sample sizes with variable follow-up durations. Consequently, the long-term durability of LAAC, particularly beyond 5–10 years, remains incompletely characterized. Third, the field of LAAC continues to evolve rapidly. Earlier trials primarily evaluated first-generation devices and procedural techniques that may not fully reflect current contemporary practice. Improvements in device engineering, imaging modalities, and procedural expertise may influence both efficacy and safety outcomes in modern LAAC programs. Fourth, substantial heterogeneity existed among the included studies with respect to patient risk profiles, endpoint definitions, comparator anticoagulation regimens, post-implantation antithrombotic protocols, 26 and device platforms, which complicates direct cross-trial comparisons. Finally, interpretation of bleeding outcomes requires caution because some trials, including OPTION, excluded procedure-related bleeding from primary safety analyses, potentially underestimating the total bleeding burden associated with LAAC. Recent evidence from the CLOSURE-AF trial further suggests that peri-procedural complications and early bleeding events remain clinically important, particularly in high-risk populations. Furthermore, differences in composite endpoint construction, particularly regarding the inclusion of all-cause mortality and clinically relevant bleeding, may influence interpretation of comparative efficacy across trials.
Conclusion
Current randomized evidence indicates that percutaneous LAAC is a clinically effective alternative to long-term oral anticoagulation for stroke prevention in selected patients with AF. Compared with both DOACs and warfarin, LAAC provides broadly comparable protection against thromboembolic events while offering an important long-term reduction in bleeding complications, particularly non–procedure-related bleeding. Although procedural and device-related complications remain important limitations, continued improvements in device technology, procedural techniques, and operator experience have progressively enhanced the safety profile of LAAC.
Overall, LAAC should be considered a selective therapeutic strategy rather than a universal replacement for OAC therapy. Its greatest clinical value is likely to be realized in patients at elevated bleeding risk, those with contraindications or intolerance to long-term anticoagulation, or individuals in whom sustained adherence to OAC therapy is unlikely. Future large-scale trials with extended follow-up and contemporary device platforms are needed to further clarify optimal patient selection, long-term durability, ischemic stroke risk, and the comparative net clinical benefit of LAAC relative to evolving anticoagulation strategies.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.