
Abstract
Background
Venous thromboembolism (VTE), the third leading cause of cardiovascular mortality, is a common but preventable complication in hospitalized patients. However, VTE prophylaxis remains underutilized. This study aims to explore physicians’ knowledge, attitudes, practices (KAP) regarding VTE prevention in Chinese public hospitals and their interrelationships to inform improvement strategies.
Methods
A cross-sectional, multicenter online survey was conducted using a KAP-based questionnaire distributed to physicians in Chinese public hospitals. Data analysis integrated descriptive statistics, Pearson correlations, and structural equation modeling (SEM).
Results
Among 787 valid responses, KAP scores were positive (Knowledge: 4.00 ± 0.81; Attitude: 4.38 ± 0.78; Practice: 4.38 ± 0.82). Scores on knowledge of intermittent pneumatic compression usage (3.40 ± 1.24) and VTE risk assessment tools (3.98 ± 1.08) were relatively low, while only 23% and 40% of physicians reported being very familiar with them, respectively. About half strongly agreed on performing dynamic VTE/bleeding risk assessments and tailoring prophylactic measures accordingly. Poor patient awareness and adherence also hindered VTE prevention. Positive correlations were observed among KAP domains (r = 0.35 – 0.59, P < 0.001). SEM demonstrated knowledge directly influenced practice (β = 0.50, P < 0.05), while attitude facilitated knowledge-to-practice translation (β = 0.25, P < 0.05).
Conclusions
Knowledge is pivotal for VTE prophylaxis implementation. Future targeted training should focus on addressing physicians’ knowledge deficiencies, enhancing awareness of dynamic risk assessment and improving patient education to strengthen institutional VTE prevention capabilities. Given the predominance of tertiary public hospital respondents, the generalizability of these findings should be interpreted with caution.
Introduction
Venous thromboembolism (VTE), a preventable yet life-threatening complication in hospitalized patients, has an annual incidence of approximately 1 – 2 per 1,000 persons globally, with hospital-acquired VTE accounting for over 60%. 1 In China, VTE hospitalization rates surged from 3.2 to 17.5 per 100,000 persons between 2007 and 2016. 2 The DissolVE-2 study revealed that among Chinese surgical inpatients, 32.7% and 53.4% were stratified as moderate and high risk for VTE, respectively, while 36.6% of medical inpatients were high risk. Alarmingly, only 9.3% of surgical and 6.0% of medical patients received standardized prophylaxis, markedly lower than the 39.5% – 58.5% reported in the 2008 ENDORSE global study.3,4 This disparity underscores critical gaps in VTE prevention practices in China. The 2025 National Medical Quality and Safety Improvement Goals recently issued by the National Health Commission prioritizes “enhancing standardized VTE prophylaxis rates” for the fifth consecutive year, reflecting both governmental commitment and persistent challenges in implementation. 5
Physicians, as key decision-makers in VTE prevention, play a pivotal role in risk assessment, prophylaxis selection, and implementation. 6 Their knowledge determines risk assessment accuracy and intervention appropriateness, attitudes drive proactive decisions, and practices directly impact outcomes. The knowledge-attitude-practice (KAP) framework, a validated behavioral science model, widely informs health behavior research, particularly in disease prevention and patient education. 7 The KAP framework systematically examines cognitive, affective, and practice dimensions to identify clinical decision-making drivers in VTE prevention, guiding targeted intervention design. However, current evidence predominantly derives from nurses and patients.8,9 Critically insufficient systematic KAP investigations have focused on physicians, the primary prophylaxis decision-makers, thereby constraining mechanistic insights into their practice patterns.
Additionally, knowledge, attitude, and practice interact through complex mechanisms that traditional statistical methods, such as correlation or regression analysis, struggle to fully capture the dynamic relationships and indirect effects among latent variables. As an advanced multivariate statistical tool, structural equation modeling (SEM) can simultaneously analyze multiple latent variables and their observed indicators, elucidating direct and indirect effect pathways. 10 Compared with traditional approaches, SEM offers distinct advantages in exploring causal relationships among KAP dimensions, not only quantifying the strength of associations between variables but also identifying key influential pathways, providing scientific support for targeted interventions.
Building on this, our study aims to comprehensively assess clinical physicians’ KAP regarding VTE prevention using a self-designed KAP questionnaire and to explore their interrelationships through SEM. The findings are expected to provide evidence for: (1) quantifying the knowledge level, attitudinal characteristics, and practice status of Chinese physicians in VTE prevention; and (2) elucidating the dynamic relationships among KAP to inform evidence-based targeted interventions, such as knowledge training and process optimization.
Methods
Study Design and Subjects
This was a multicenter cross-sectional study conducted across China from February 9, 2025 to April 25, 2025. A stratified convenience sampling method was used in this study. Specifically, the minimum required sample size was estimated at 576 after applying a design effect of 1.5. To improve regional coverage, China was divided into eastern, central, and western strata based on the distribution of healthcare resources. The target sample was then allocated proportionally according to official statistics from the China Health Statistics Yearbook 2024 (37.4%, 29.5%, and 33.1%, respectively), corresponding to 215, 170, and 191 questionnaires. Assuming that each hospital would contribute approximately 30 valid questionnaires, about 21 hospitals were planned for inclusion, including 8 in the eastern region, 6 in the central region, and 7 in the western region. These regional allocations served as recruitment targets to enhance geographic coverage rather than as a probability-based sampling frame.
To safeguard participant privacy, all respondents remained anonymous. The questionnaire was developed based on core content from VTE-related guidelines11-13 and was refined through two rounds of expert consultation employing the Delphi method. Data collection was conducted via a professional online survey platform, with questionnaire access provided via quick response (QR) codes distributed through WeChat to clinical physicians in public hospitals. To ensure data integrity, mandatory fields were incorporated into the questionnaire, requiring the completion of essential information. The study received ethical approval from the Ethics Committee of the Second Affiliated Hospital of Xi’an Jiaotong University (Approval No.: 2024 LUNSHEN 011). Given that the survey did not involve personal privacy information, informed consent was waived.
The questionnaire consisted of four sections: demographic information, K, A, and P dimensions. In the K, A, and P sections, all items except for attention check and open-ended questions were scored using a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). Specifically, the K section included an attention check question tied to core knowledge of VTE to verify the validity of the responses. The A section comprised an open-ended question, allowing physicians to freely list additional factors that impeded the implementation of VTE prevention. Therefore, the attention check item and open-ended question were not scored and were excluded from the SEM. During the pilot survey phase, the scale underwent reliability testing, yielding a Cronbach’s α coefficient of 0.93, which reflected good internal consistency.
Statistical Analysis
Data preprocessing followed a standardized procedure, excluding invalid samples where participants selected “correct” or “unsure” in the attention check question. Continuous variables were reported as mean ± standard deviation (mean ± SD), while categorical variables were presented as frequencies and percentages (n, %). Cronbach’s α was employed to evaluate the internal consistency of the scale, with α > 0.7 deemed acceptable for reliability. For normally distributed data, two-group comparisons were conducted using independent samples t-tests, and comparisons involving three or more groups utilized one-way ANOVA. For non-normally distributed data, two-group comparisons were analyzed with the Wilcoxon rank-sum test, and comparisons of three or more groups were performed using the Kruskal-Wallis H test.
This study implemented a two-phase analytical strategy. First, Pearson correlation analysis was used to quantify pairwise linear associations among the K, A, and P domains with two-tailed significance testing (α = 0.05). Second, SEM was conducted to evaluate the direct effects of K on A, K on P, and A on P pathways using maximum likelihood estimation (MLE), with effect strength determined by standardized path coefficients (β) and significance thresholds (P < 0.05). All analyses were performed in R version 4.4.3 and AMOS 29.0.
Results
Expert Consultation Outcomes
This study utilized the Delphi method to develop a questionnaire through two rounds of expert consultation involving 15 experts with associate professor or higher academic titles and over 10 years of clinical experience in clinical pharmacy (n = 6) and clinical medicine (n = 9). The authority coefficient ratings (Cr) for the two rounds were 0.89 and 0.91, respectively, reflecting the high reliability of expert opinions. Kendall’s W coefficients were 0.41 and 0.45 (both P < 0.001), indicating strong consistency among the experts. Based on their feedback, three items were revised and one low-scoring item was deleted, resulting in a final 23-item questionnaire covering demographic information (8 items), knowledge (5 items), attitude (6 items), and practice (4 items).
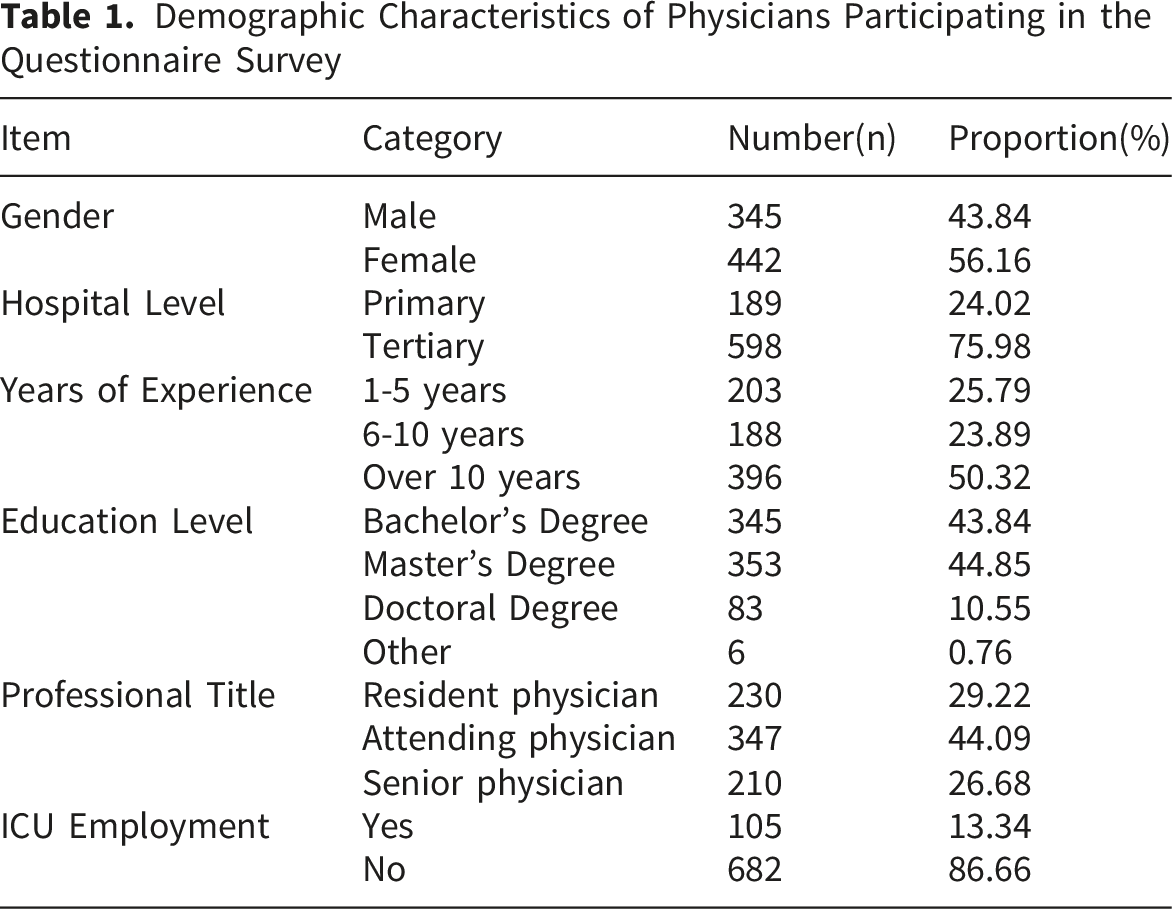
Demographic Characteristics of Physicians
The survey collected 863 questionnaires, yielding 787 valid responses and excluding 76 invalid ones.
Demographic Characteristics of Physicians Participating in the Questionnaire Survey
Questionnaire Score Distribution in Knowledge, Attitude, and Practice Dimensions
Clinical Physicians’ KAP Scores in VTE Prophylaxis
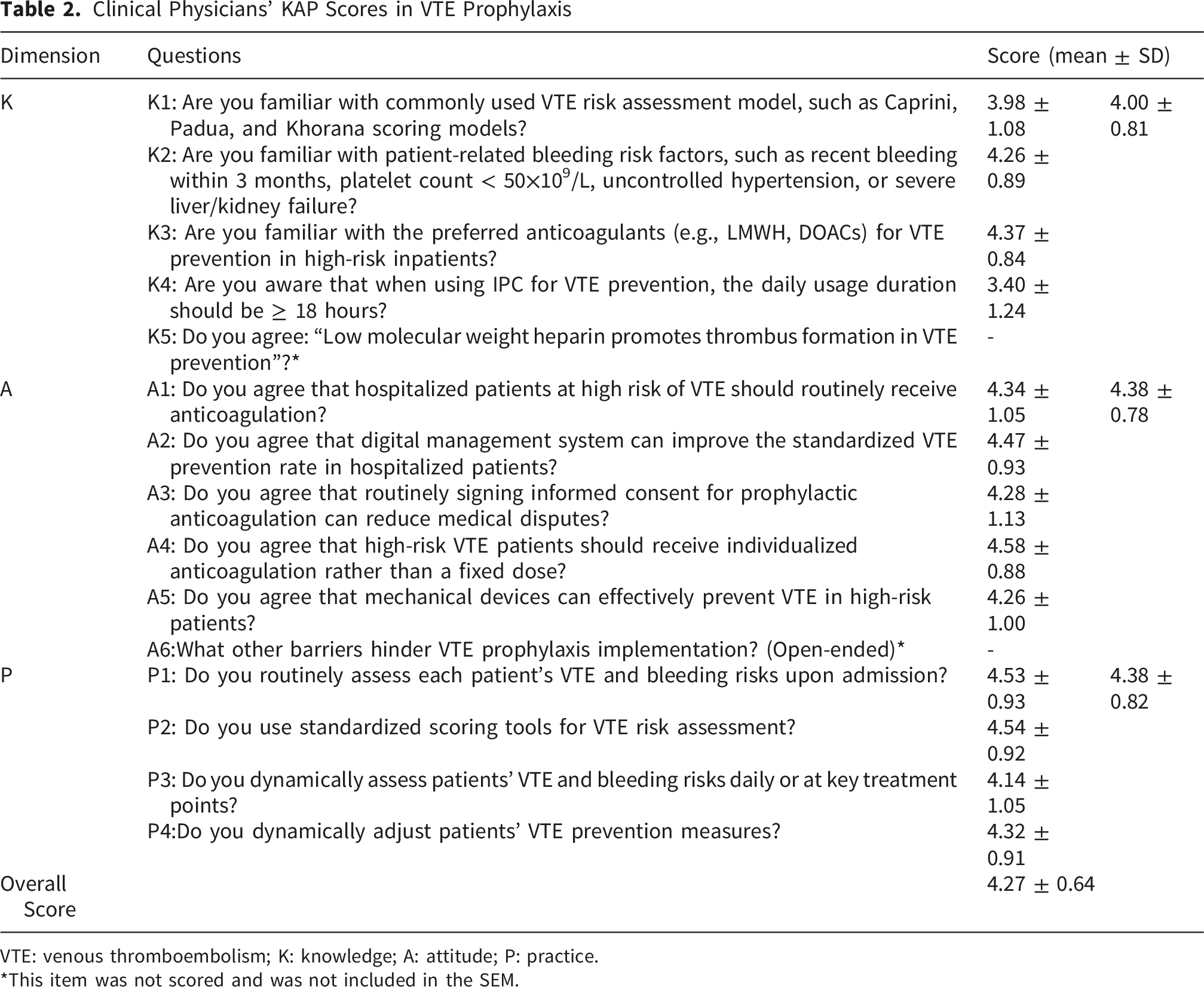
VTE: venous thromboembolism; K: knowledge; A: attitude; P: practice.
*This item was not scored and was not included in the SEM.
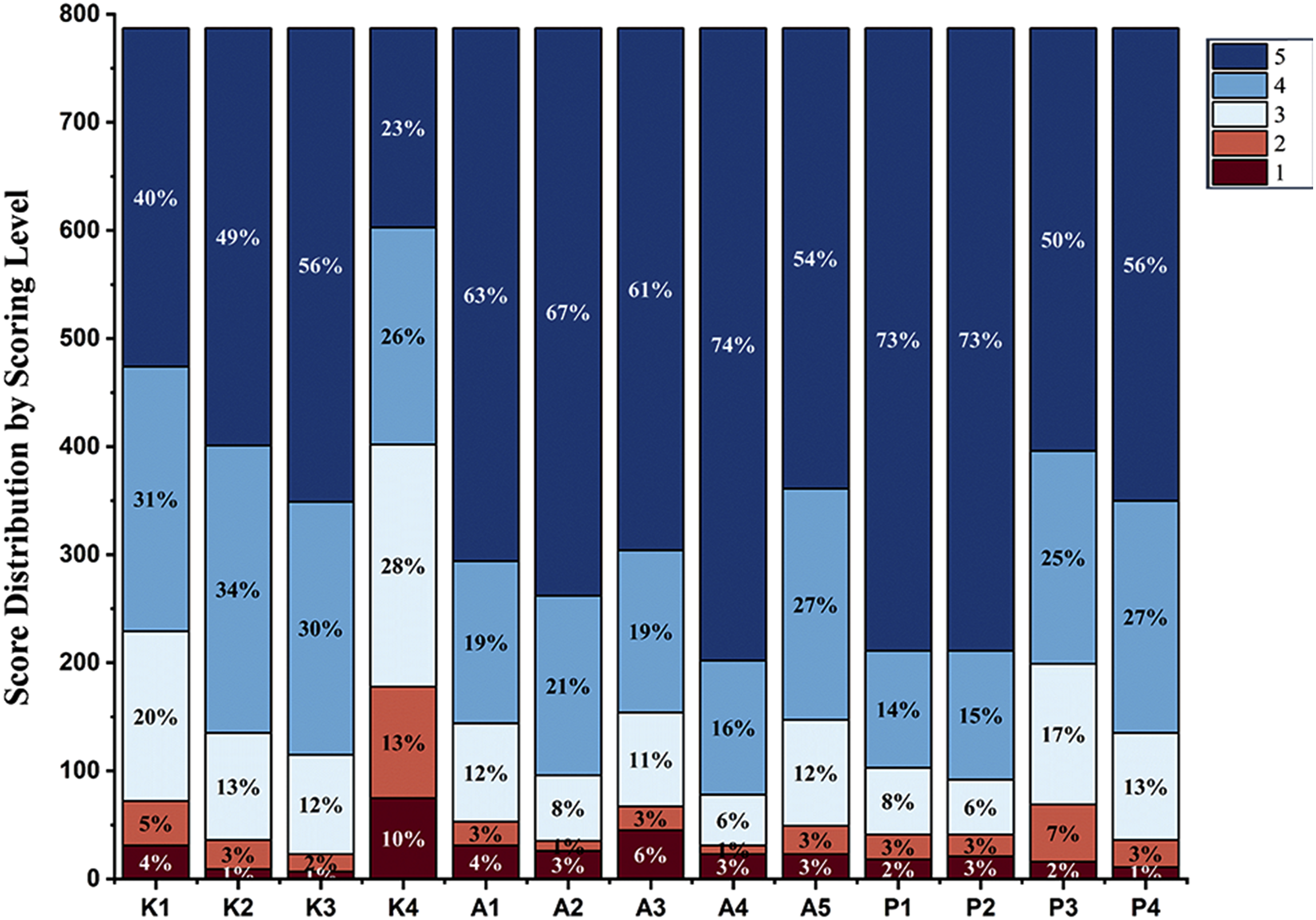
Score distribution of items in knowledge, attitude, and practice dimensions. K: knowledge; A: attitude; P: practice
Correlation Between Demographic Characteristics and VTE Prophylaxis KAP Scores
Correlation of Clinician Demographic Characteristics With VTE Prophylaxis KAP Scores
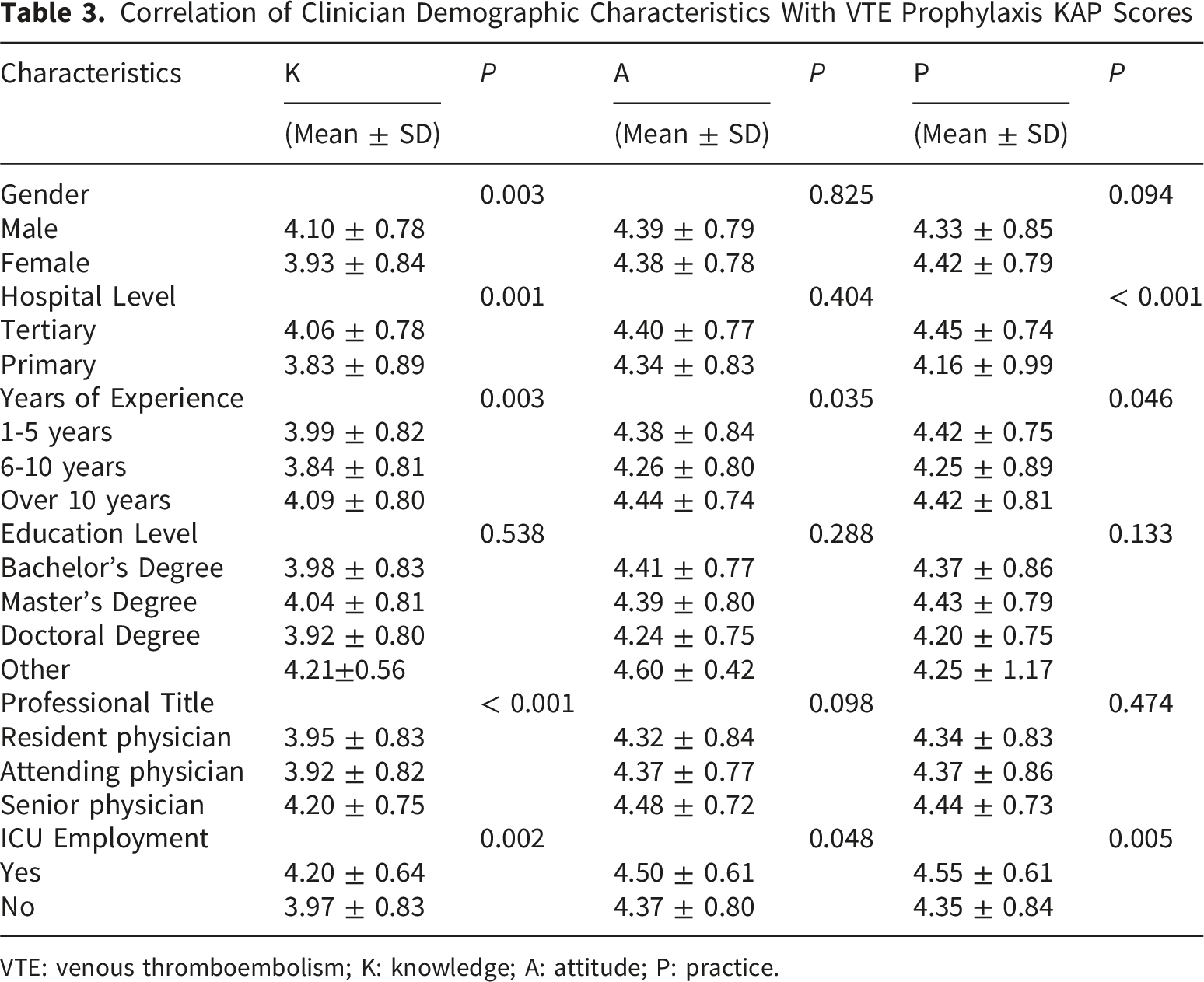
VTE: venous thromboembolism; K: knowledge; A: attitude; P: practice.
Correlational and Structural Equation Modeling Analyses of KAP
Pearson correlation analysis revealed significant positive correlations among K, A, and P (K-A: r = 0.35, P < 0.001; K-P: r = 0.59, P < 0.001; A-P: r = 0.43, P < 0.001), as shown in Table S2. A SEM model was constructed using confirmatory factor analysis to further validate these relationships. The standardized factor loadings for K (items 1-4), A (items 1-5), and P (items 1-4) ranged from 0.47 to 0.92, indicating good measurement validity. Model fit indices demonstrated an acceptable overall fit (Table S3). Although the CMIN/DF value was slightly higher than the commonly cited ideal threshold, this index is derived from the chi-square statistic and may be inflated in studies with relatively large sample sizes. In addition, the standardized root mean square residual (SRMR) was calculated to further evaluate the model fit. The SRMR value was 0.06, which was below the commonly recommended threshold of 0.08, providing additional support for acceptable model fit. To further assess model robustness, two theoretically plausible alternative models (a full mediation model and a direct effect model) were also tested (Figures S1 and S2). Compared with these alternative models, the original model showed better fit indices (Table S4 and S5) and lower AIC and BIC values (Table S6). Path analysis revealed a significant positive effect of K on A (β = 0.38, P < 0.05), with the strongest direct effect of K on P (β = 0.50, P < 0.05), and a positive effect of A on P (β = 0.25, P < 0.05). The path relationships are illustrated in Figure 2. Path relationships among KAP for VTE prevention based on SEM. VTE: venous thromboembolism; SEM: structural equation modeling; K: knowledge; A: attitude; P: practice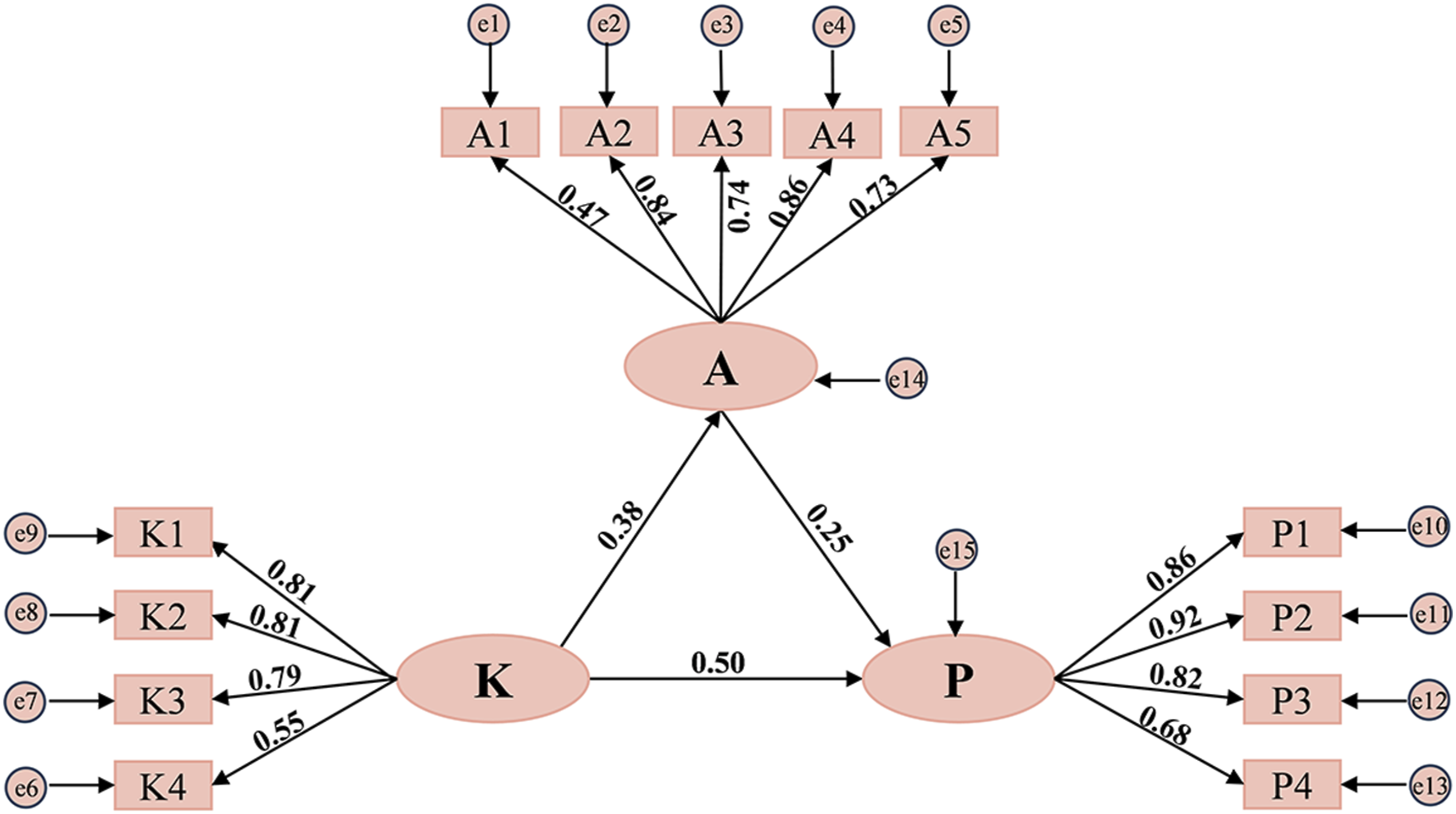
Discussion
This study utilized a cross-sectional design, administering an online survey based on the KAP framework to physicians in Chinese multicenter hospitals, yielding 787 valid responses. Results revealed that physicians exhibited a high overall knowledge level of VTE prevention (4.00 ± 0.81), though their grasp of RAM and IPC application details was limited (scores of 3.98 ± 1.08 and 3.40 ± 1.24, respectively). In the attitude domain, physicians generally displayed a positive stance toward VTE prevention (4.38 ± 0.78), strongly endorsing individualized anticoagulant use, yet showing lower recognition of IPC’s preventive efficacy. Positive attitudes toward VTE prevention were consistent among both tertiary and primary hospital physicians (P = 0.404). Behaviorally, over 70% of physicians firmly agree to perform VTE risk assessments and initiate preventive measures at patient admission, but dynamic assessment was lacking (P3: 4.14 ± 1.05). Physicians from tertiary hospitals, those with greater experience, and ICU physicians outperformed others across all KAP dimensions. Pearson correlation analysis demonstrated significant positive relationships among K, A, and P. SEM confirmed that knowledge exerted the strongest direct effect on practice (β = 0.50, P < 0.05), with attitude synergistically facilitating the knowledge-to-practice transition (β = 0.25, P < 0.05). Considering that respondents were recruited from public hospitals and were predominantly from tertiary hospitals, these findings should be interpreted within this sampling context rather than generalized to all physicians in China.
In recent years, Chinese healthcare administrative departments had advanced in-hospital VTE prevention by establishing prevention information systems, standardizing clinical pathways, and mandating RAMs to enhance medical staff’s capabilities. The “National Pulmonary Embolism and Deep Vein Thrombosis Capacity Building Project” 14 strengthens doctors’ awareness through multi-level training. Meanwhile, VTE prevention implementation and assessment rates have been integrated into medical quality indicators to ensure accountability. 15 Despite physicians’ heightened proactivity in VTE prevention, improvements in specific knowledge and implementation remain necessary.
The primary step in VTE prevention is assessing patients’ thrombosis and bleeding risks. In this survey, 73% of physicians reported using RAMs in practice, a proportion like data from a previous global survey in China. 16 However, despite their widespread implementation, physicians’ familiarity with these tools remains limited (K1: 3.98±1.08). Additionally, 23.9% of physicians identified “difficulty in risk assessment” as a significant barrier to VTE prevention, suggesting that current RAMs may be overly complex and fail to meet physicians’ practical needs for assessing VTE-related risks. A survey of U.S. physicians 17 found that “excessive concern about bleeding risks” and “inadequate RAM application” as primary obstacles to VTE prevention, with over 60% relying on personal experience rather than RAM-guided decisions. In ICUs, RAM utilization for VTE risk assessment remains below 40%. 18 Despite guideline recommendations for RAMs to balance over- and under-anticoagulation, VTE prophylaxis inadequacy persists in 74.2% of cases even in institutions with standardized RAM protocols. 19 These findings underscore that merely promoting existing RAMs cannot resolve the complexities of clinical decision-making.
Physicians exhibit a high level of knowledge about LMWH, and more than 80% of physicians are familiar with LMWH as the preferred anticoagulant for VTE prophylaxis. This finding is consistent with domestic and international guidelines, which recommend LMWH as the first-line pharmacological prophylaxis for hospitalized patients at risk of VTE.12,13,20,21 The widespread dissemination of guidelines and frequent clinical application have reinforced knowledge accumulation in this area. In contrast, physicians show a significant knowledge gap regarding the use of IPC for VTE prevention and lack confidence in its efficacy. Only 23% of physicians are fully familiar with the 18-hour daily usage requirement for IPC, and 54% strongly agree that mechanical prophylaxis is highly effective. Mechanical prophylaxis devices (graduated compression stockings [GCS]/IPC) prevent VTE by enhancing venous return without increasing bleeding risks, yet their clinical utility remains debated. The CLOTS 3 trial (2008–2012, conducted across 94 UK centers) established foundational evidence for IPC in VTE prevention. 22 Subsequent studies, however, reported no significant reduction in thrombosis incidence with GCS and increased risks of skin injury, 23 while a recent meta-analysis found no superiority of mechanical devices for VTE prevention in critically ill patients. 24 Limited evidence for mechanical prophylaxis likely contributes to physicians’ lack of confidence. Additionally, physicians generally lack knowledge about mechanical device applications in VTE prevention (mean score: 3.40 ± 1.24). This highlights the need for future training to focus on standardized use of mechanical devices, including IPC’s mechanism, indications, contraindications, sizing, pressure levels, duration, application methods, maintenance, washing, and lifespan. 25
VTE is a complex and dynamic pathophysiological process, requiring dynamic assessment of VTE and bleeding risks during hospitalization. Key time points for assessment include: within 24 hours of admission, during the postoperative phase, upon clinical status changes (e.g., new-onset infections or hemorrhagic events), and prior to discharge. This survey shows that physicians in both tertiary and primary hospitals evaluate VTE risk and initiate preventive measures upon admission. However, only approximately 50% of physicians dynamically assess VTE and bleeding risks and adjust prevention strategies correspondingly. A longitudinal study of hospitalized medical patients revealed that most VTE events occur within six weeks post-discharge, highlighting the need for patient-centered, timely, and individualized risk assessment and prevention. 26 However, research indicates that only 15% of physicians reassess VTE risk at discharge. 17 The NICE guidelines (2019) emphasize that critically ill patients, due to rapid condition changes, require at least daily evaluation of thrombosis and bleeding risks, with immediate reassessment upon any clinical change. 11 Dynamic risk assessment is critical for enhancing the quality of hospital-acquired VTE prevention.
Physicians’ knowledge and attitudes toward VTE prevention demonstrated a significant positive correlation with its implementation. Knowledge level directly influences the quality of clinical decision-making, as studies indicate that higher knowledge among healthcare providers is associated with more proactive clinical attitudes. Improved knowledge enhances attitudes, which in turn facilitates the translation of knowledge into practice.27,28 In specific domains (e.g., catheter-related infection prevention, chronic disease management),29,30 knowledge deficits lead to suboptimal practices, while systematic educational interventions effectively address these gaps. 31 In this study, physicians in tertiary hospitals outperformed those in primary hospitals in both VTE prevention knowledge and practice, further validating the pivotal role of knowledge in driving practice. Another study only on surgeons’ and anesthesiologists’ knowledge, attitude, and practice regarding postoperative VTE revealed that knowledge directly influences attitude and practice, while attitude independently affects practice, which is consistent with our own research. 32
In the future, to address the knowledge gaps identified in this study, such as insufficient mastery of RAMs and inadequate familiarity with the details of IPC use, a national public-interest online education platform for VTE prevention could be jointly developed by health authorities, professional academic organizations, and healthcare institutions. Supported by a WeChat mini-program or mobile application, this platform could help establish a more standardized, continuous, and accessible training system. The platform could include the following modular training components: (1) Specialized training module on risk assessment tools: systematic instruction on the appropriate application, scoring principles, and interpretation of tools such as the Caprini score and Padua scale. This module should also emphasize joint assessment of VTE and bleeding risks, as well as dynamic reassessment at key time points, including admission, post operation, changes in clinical condition, and before discharge. (2) Standardized training module on mechanical prophylaxis: focused instruction on the indications and contraindications of mechanical prophylaxis such as IPC, device selection, standardized operating procedures, duration of use, and management of common problems. (3) Practice translation module: use of simulated cases, case discussions, scenario-based training, and staged assessments to help physicians improve their ability to translate guideline knowledge into actual clinical decision-making and practice. In addition to structured training, clinical decision support tools embedded within hospital information systems may further help bridge gaps in knowledge recall and application. By providing automated reminders for VTE and bleeding risk assessment, prompts for dynamic reassessment at key time points, and standardized decision support for the use of RAMs, IPC, and other prophylactic measures, such tools may facilitate the translation of knowledge into routine clinical practice. Previous studies have shown that implementing a clinical decision support system within an electronic medical management system, with alert prompts provided to healthcare professionals, can increase the rate of documented VTE risk assessment within 24 hours of admission by 29.9% and improve the rate of guideline-concordant prophylaxis. 33
However, improving knowledge alone may not be sufficient to ensure effective implementation of VTE prevention. Positive attitudes are also essential for promoting VTE prevention practice. Future efforts may reinforce physicians’ positive attitudes through the following approaches: (1) Strengthening leadership and organizational support for VTE prevention. Hospitals may establish multidisciplinary VTE management teams involving administrators, clinical department leaders, and relevant functional departments. Incorporating VTE prevention into key patient safety and healthcare quality priorities, supported by policy, resources, and institutional measures, may further enhance physicians’ recognition of its importance. (2) Integrating VTE prevention into quality evaluation and performance management. Indicators such as timely risk assessment and standardized prophylaxis implementation may be included in departmental quality management and performance evaluation. Continuous monitoring and feedback may strengthen physicians’ sense of responsibility and their sustained willingness to implement VTE prevention. (3) Sharing successful cases and best practices. Case competitions, best-practice presentations, experience-sharing meetings, and peer demonstration may help disseminate successful experiences in VTE risk assessment and prevention. Such activities may further highlight the feasibility and clinical value of standardized prevention, thereby reinforcing positive attitudes and facilitating practice implementation.
Furthermore, the present survey indicates that patients’ inadequate knowledge of VTE prevention and poor adherence are critical factors hindering physicians’ implementation of VTE prophylaxis. Patient education is important in disease control and treatment, as it not only enhances patients’ awareness of the condition but also fosters active involvement in the therapeutic process. Notably, a prospective cohort study demonstrated that pharmacist-led patient education improved adherence to VTE prophylactic medications from 89.9% to 94.4% and significantly reduced instances of non-administration attributable to patient refusal. 34 Another investigation also revealed that targeted patient education interventions markedly decreased the non-administration rate of VTE prophylactic measures among hospitalized patients while elevating healthcare quality. 35 Meanwhile, international guidelines underscore that the successful implementation of VTE prevention strategies necessitates collaborative partnerships with patients, wherein patient education acts as a vital catalyst. 12 The NICE guideline advocates for VTE prevention education to be delivered to patients and caregivers at admission and discharge to bolster awareness and compliance with preventive measures. 11 In the future, patient education on venous thromboembolism could be incorporated into the healthcare quality assessment system as an integral part of standardized clinical practice, which will help further optimize thrombosis prevention strategies.
This study has several limitations. First, self-reported data are susceptible to social desirability bias, potentially leading physicians to overestimate their knowledge and practices. In particular, the practice dimension was based primarily on physicians’ self-assessment and may not fully reflect actual clinical behaviors. Future research should use more objective measures, such as indicators from hospital information systems or electronic medical records, to further validate the relationships among knowledge, attitude, and practice in the current KAP model. Second, although regional recruitment targets were set, this study used a stratified convenience sampling strategy rather than probability-based stratified sampling. The actual recruitment relied mainly on collaborating public hospitals and online QR-code dissemination. As most collaborating institutions were tertiary or teaching hospitals, physicians from tertiary hospitals were overrepresented, whereas those from primary healthcare institutions were underrepresented because of limited research collaboration channels, administrative coordination barriers, and lower response rates. Non-public hospitals were not adequately covered by the recruitment channels. Therefore, the findings may mainly reflect the KAP of physicians in public hospitals, particularly tertiary hospitals, and should not be generalized to physicians across all healthcare settings and levels. Future studies should include more physicians from primary- and secondary-level hospitals as well as non-public healthcare institutions to improve representativeness and generalizability. Finally, patient-related factors, such as patient education, patient compliance, and doctor–patient communication, were not included in the current KAP model, although they may influence the translation of physicians’ knowledge and attitudes into practice. Future research should incorporate these variables and examine their potential moderating or mediating roles to better understand how physician-related and patient-related factors jointly influence VTE prevention practice.
Conclusion
Knowledge exerts the strongest direct influence on VTE prevention practice, with attitudes playing a synergistic mediating role in translating knowledge into practice. Physicians in Chinese public hospitals demonstrated robust knowledge of VTE prevention but exhibited gaps in understanding the specific application details of RAMs and IPC. While physicians generally held positive attitudes toward VTE prevention and acknowledged its necessity, confidence in the efficacy of IPC remained low. Most physicians conducted risk assessments and implemented prophylactic measures upon patient admission; however, persistent deficiencies were observed in dynamic reassessment and adjustment of prevention strategies. Furthermore, inadequate patient knowledge and poor adherence to VTE prevention are also important factors affecting physicians’ implementation of VTE prophylaxis. Given the predominance of tertiary public hospital respondents, these findings should be interpreted primarily as reflecting physicians in Chinese public hospitals, particularly tertiary hospital settings, and should be generalized to other healthcare settings with caution. Future efforts should focus on developing standardized VTE prevention platforms or clinical decision support systems that integrate RAM-based risk assessment, IPC guidance, dynamic reassessment alerts, and individualized prophylaxis recommendations. In addition, embedding patient education and adherence-support modules into such systems may help bridge the gap between physicians’ knowledge and sustained preventive practice.
Supplemental Material
Supplemental Material - Knowledge Drives Venous Thromboembolism Prevention: Structural Equation Modeling Insights Into Physicians’ Knowledge, Attitudes and Practices in Chinese Public Hospitals
Supplemental Material for Knowledge Drives Venous Thromboembolism Prevention: Structural Equation Modeling Insights Into Physicians’ Knowledge, Attitudes and Practices in Chinese Public Hospitals by Di Wei, Yuan Wu, Jiatian Wang, Huangxin Gong, Ting Yang, Sinan Ma, Keyu Chen, Weijia Huang, Fei Xie, Ya Li, Yan Wang, Li Zhang in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgements
We would like to extend our sincere gratitude to Dr. Xiaojuan Yang (Daxing Hospital, Shaanxi), Dr. Deng Wang (Jingyang County People’s Hospital, Shaanxi), and Dr. Zhichun Gu (Renji Hospital, Shanghai Jiao Tong University School of Medicine, Chinese Alliance for Anticoagulation) for their invaluable support and assistance in questionnaire collection.
Author Contributions
W.D.: Conceptualization, Methodology, Investigation, Formal analysis, Writing – original draft, Visualization. W.Y.: Conceptualization, Methodology, Investigation, Data curation, Formal analysis, Visualization. W.J.T.: Investigation, Data curation, Formal analysis. G.H.X.: Investigation, Data curation, Formal analysis. Y.T.: Investigation, Data curation, Formal analysis. M.S.N.: Investigation, Data curation, Formal analysis. C.K.Y.: Investigation, Data curation, Formal analysis. H.W.J.: Investigation, Data curation. X.F.: Investigation, Data curation. L.Y.: Investigation, Data curation. W.Y.: Conceptualization, Methodology, Investigation, Formal analysis, Writing – review and editing, Supervision, Project administration, Funding acquisition. Z.L.: Conceptualization, Methodology, Investigation, Formal analysis, Writing – original draft, Writing – review and editing, Supervision, Project administration, Funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Scientific Research Project Funding of National Natural Science Foundation of China [grant numbers 72304221; 72274153]; Key Research and Development Program of Shaanxi Province [grant numbers 2023-YBSF-243]; the Innovation Capacity Support Plan of Shaanxi Province [grant numbers 2024ZC-KJXX-085]; the Natural Science Foundation of Shaanxi, China [grant numbers 2024JC-YBQN-0852]
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.