
Abstract
Background
Management of extensive inferior vena cava (IVC) thrombosis following trauma is challenging, particularly when IVC filter placement is unsuitable. The presence of concomitant injuries requiring surgical intervention further complicates decisions regarding anticoagulation and pulmonary embolism prevention.
Case Presentation
A 40-year-old man presented following a high-velocity motorcycle accident with multiple facial fractures and a left radial shaft fracture. Contrast-enhanced computed tomography demonstrated no solid organ or major vascular injury but revealed extensive thrombosis extending from the infrarenal IVC into the bilateral common iliac veins. Following hemodynamic stabilization and exclusion of intracranial and intra-abdominal hemorrhage, therapeutic unfractionated heparin infusion was initiated. Despite anticoagulation, progressive lower limb swelling developed. Given the extensive thrombus burden and the need for subsequent surgical procedures, further intervention was considered. The suprarenal IVC measured 32 mm in diameter, and concerns regarding filter stability, migration, and reduced efficacy rendered IVC filter placement suboptimal.
Intervention and Outcome
Following multidisciplinary discussion, percutaneous mechanical thrombectomy was performed using a combined ClotTriever BOLD and FlowTriever system. A 25-mm FlowTriever disc was deployed in the retrohepatic IVC for temporary embolic protection during thrombectomy. Successful thrombus extraction restored caval patency without complications. Lower limb swelling resolved within three days, allowing staged orthopedic and maxillofacial reconstruction. Thrombophilia screening was negative, and the patient completed nine months of rivaroxaban therapy without recurrence.
Conclusion
Combined ClotTriever and FlowTriever mechanical thrombectomy may be an effective treatment option for extensive traumatic iliocaval thrombosis when IVC filter placement is not feasible or considered suboptimal.
Keywords
Introduction
Inferior vena cava thrombosis represents an uncommon manifestation of venous thromboembolism, accounting for a small proportion of all deep venous thromboses.1,2 The condition may occur secondary to malignancy, thrombophilia, external venous compression, congenital caval anomalies, or trauma. Among trauma patients, extensive IVC thrombosis identified during initial evaluation is particularly rare, with only isolated cases reported in the literature. 1 Proposed mechanisms include direct endothelial injury from blunt abdominal impact, venous stasis resulting from immobilization, and trauma-induced hypercoagulability, fulfilling Virchow’s triad.
Management remains controversial because of the limited evidence base and the frequent coexistence of injuries requiring surgical intervention. While anticoagulation remains the cornerstone of treatment, patients with extensive iliocaval thrombus burden may remain at risk of pulmonary embolism despite therapeutic anticoagulation. Inferior vena cava filter placement is often considered in selected circumstances; however, anatomical limitations may preclude safe deployment. 3 Mechanical thrombectomy has emerged as a promising alternative that allows rapid thrombus debulking without the bleeding risks associated with thrombolytic therapy. We describe the successful management of extensive post-traumatic IVC thrombosis using combined ClotTriever BOLD and FlowTriever systems in a patient for whom IVC filter placement was considered suboptimal.
Case Presentation
A 40-year-old male was brought to the emergency department following a high-energy motorcycle accident in which the handlebar impacted his abdomen. On arrival, he was mildly hypotensive but responded appropriately to fluid resuscitation. Focused Assessment with Sonography for Trauma was negative. Clinical examination identified multiple facial fractures and a left midshaft radial fracture.
Given the high-energy mechanism, contrast-enhanced whole-body computed tomography was performed. No intracranial hemorrhage, solid organ injury, major arterial injury, or active bleeding was identified. However, imaging unexpectedly demonstrated extensive thrombosis extending from the infrarenal inferior vena cava into both common iliac veins, with predominant involvement of the left common iliac vein. The suprarenal IVC measured 32 mm in diameter. Figure 1 No features suggestive of May-Thurner syndrome, congenital caval anomaly, or external venous compression were identified. The patient denied previous lower limb swelling, prior venous thromboembolism, or known thrombophilia. Contrast-enhanced computed tomography (coronal view) demonstrating extensive thrombosis within the inferior vena cava extending from the infrarenal segment into the left common iliac vein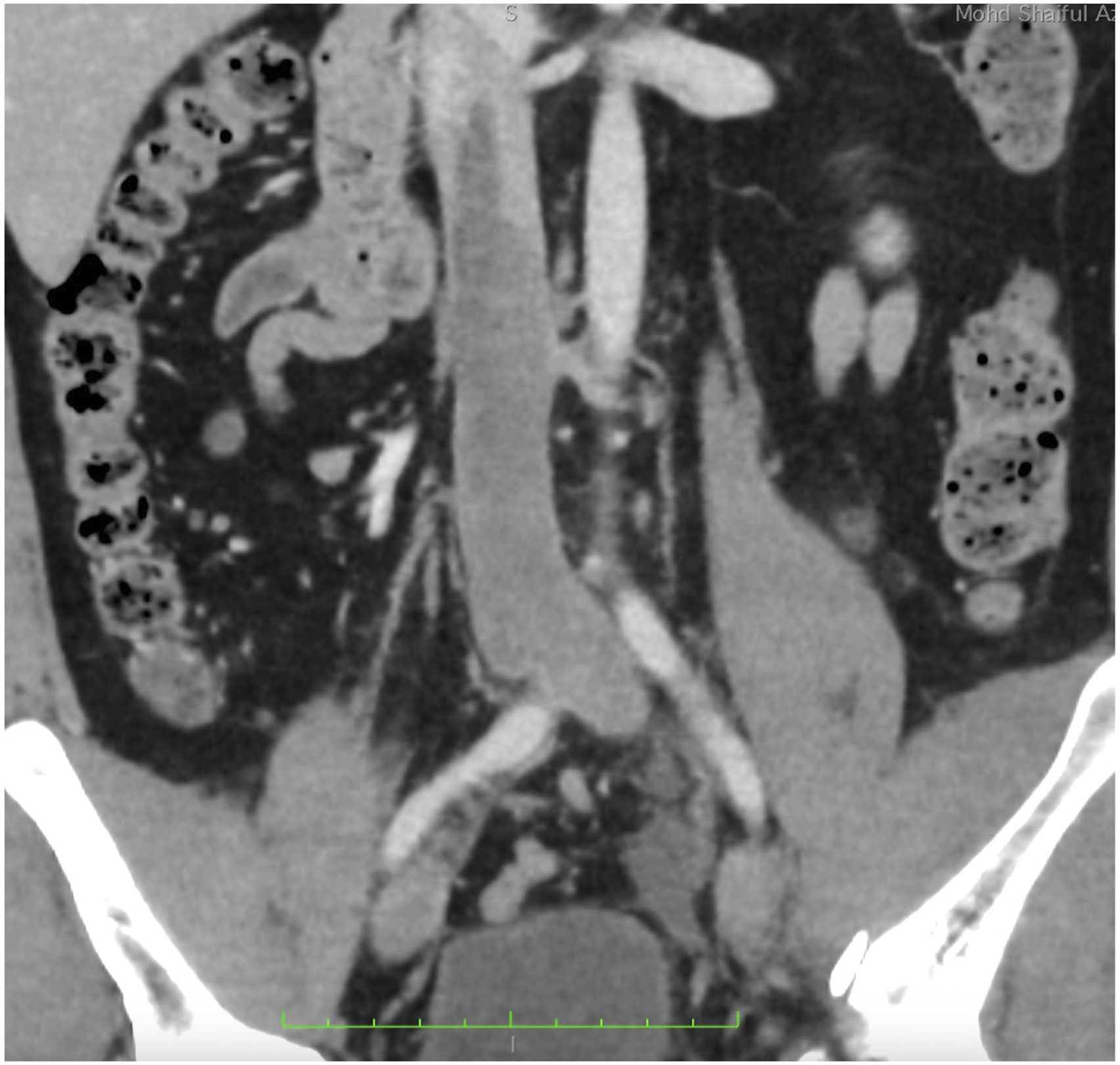
Following exclusion of active bleeding, therapeutic unfractionated heparin infusion was commenced with activated partial thromboplastin time monitoring. Initial laboratory investigations demonstrated markedly elevated D-dimer levels consistent with extensive venous thrombosis. Despite therapeutic anticoagulation, progressive bilateral lower limb swelling developed during admission, raising concerns regarding worsening venous outflow obstruction and ongoing embolic risk.
The case was reviewed in a multidisciplinary meeting involving vascular surgery, trauma surgery, orthopedic surgery, maxillofacial surgery, and interventional radiology. Definitive fixation of the fractures was considered necessary; however, the extensive iliocaval thrombus burden posed a significant perioperative risk of pulmonary embolism. IVC filter placement was discussed extensively. Although technically possible, the requirement for suprarenal deployment within a 32-mm cava raised concerns regarding incomplete wall apposition, filter migration, reduced clot-trapping efficacy, and difficulty achieving stable positioning within the available landing zone. The team therefore elected to proceed with mechanical thrombectomy before fracture fixation.
Procedural Technique
The procedure was performed under fluoroscopic guidance with the patient in the supine position. Bilateral common femoral venous access was obtained under ultrasound guidance.
A 13-Fr sheath was introduced through the right common femoral vein. Through this access, a 25-mm FlowTriever disc (Inari Medical, Irvine, California, USA) was advanced and deployed within the retrohepatic IVC below the hepatic venous confluence and above the cranial extent of thrombus. Figure 2 The device was intended to provide temporary embolic protection by intercepting large thrombus fragments generated during thrombectomy while maintaining caval flow. Intraoperative fluoroscopic image showing deployment of the FlowTriever disc in the retrohepatic inferior vena cava, functioning as a temporary embolic protection device during thrombectomy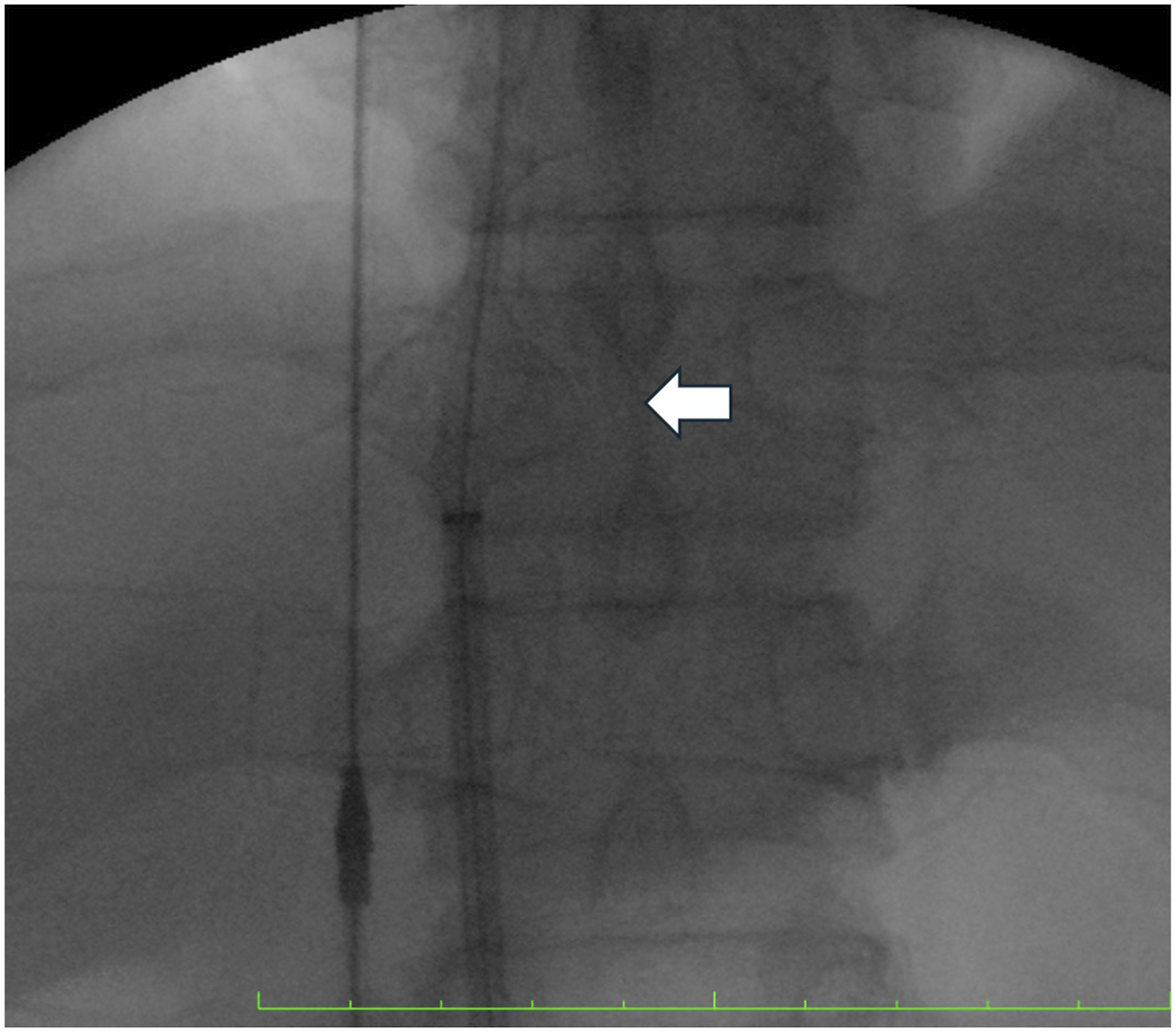
Through the left common femoral vein, a 22-Fr ClotTriever sheath was advanced. A 0.035-inch guidewire was carefully negotiated across the thrombus into the suprarenal IVC and exchanged for a stiff guidewire. Mechanical thrombectomy was then performed using the ClotTriever BOLD catheter with multiple passes through the thrombosed segment. Large volumes of organized thrombus were extracted. Completion venography demonstrated substantial restoration of caval lumen with residual thrombus localized to the iliocaval confluence. This was subsequently removed using aspiration thrombectomy with the FlowTriever system.
Final venography demonstrated near-complete restoration of flow through the inferior vena cava and bilateral iliac veins. Figure 3 The FlowTriever disc was then recaptured and removed. Hemostasis was achieved using venous closure devices. No intraprocedural complications or evidence of embolization occurred. (A) Pre-thrombectomy venogram demonstrating extensive thrombus burden involving the inferior vena cava and iliocaval confluence. (B) Completion venogram showing restoration of luminal patency with near-complete clearance of thrombus following mechanical thrombectomy
Outcome and Follow-Up
The postoperative course was uneventful. Lower limb swelling improved significantly within 48 hours and resolved completely within three days. Repeat clinical assessment showed no evidence of pulmonary embolism. Transthoracic echocardiography demonstrated no intracardiac thrombus or right ventricular strain.
Following recovery from thrombectomy, the patient underwent open reduction and internal fixation of the radial fracture. Definitive maxillofacial reconstruction was subsequently performed six weeks later. Comprehensive thrombophilia screening, including antithrombin activity, protein C, protein S, antiphospholipid antibodies, and factor V Leiden mutation, was negative.
The patient was transitioned from unfractionated heparin to rivaroxaban and completed nine months of anticoagulation. This duration was selected because of the extensive iliocaval thrombus burden and the need for multiple staged surgical procedures, exceeding the minimum recommended treatment duration for provoked venous thromboembolism. At follow-up, he remained asymptomatic without recurrence of venous thromboembolism.
Discussion
Inferior vena cava thrombosis is an uncommon manifestation of venous thromboembolism and is rarely encountered following blunt abdominal trauma. The condition is thought to arise through a combination of endothelial injury, venous stasis, and trauma-induced hypercoagulability. 4 Direct impact from the motorcycle handlebar likely resulted in localized caval endothelial injury, while the systemic inflammatory response associated with major trauma created a transient prothrombotic state. Although venous thromboembolism is common after trauma, extensive iliocaval thrombosis identified during the initial trauma evaluation remains unusual and is described only in isolated reports.
Management was complicated by the coexistence of multiple fractures requiring surgical intervention. Therapeutic unfractionated heparin was initiated after exclusion of intracranial hemorrhage and significant intra-abdominal injury; however, progressive lower limb swelling developed despite adequate anticoagulation, indicating worsening venous outflow obstruction. 5 The extensive thrombus burden involving the infrarenal IVC and bilateral common iliac veins also raised concern regarding perioperative pulmonary embolism during subsequent orthopedic and maxillofacial procedures. These competing risks required a strategy that would reduce thrombus burden while preserving the ability to proceed with definitive surgical treatment.
The potential role of an inferior vena cava filter was carefully evaluated. Current guidelines reserve filter placement primarily for patients with acute venous thromboembolism who have contraindications to anticoagulation or recurrent embolic events despite adequate anticoagulation.6,7 In this patient, the suprarenal IVC measured 32 mm in diameter and the thrombus extended close to the renal vein confluence, limiting the available landing zone. Although suprarenal filter deployment was technically feasible, concerns remained regarding incomplete wall apposition, filter tilt, migration, and uncertain embolic protection. Following multidisciplinary discussion, mechanical thrombectomy was considered a more definitive approach because it directly removed thrombus rather than relying on embolic interception alone.
Mechanical thrombectomy offers several advantages in trauma patients by achieving immediate thrombus debulking without the bleeding risks associated with thrombolytic therapy. 8 Registry data, including the CLOUT study, have demonstrated favorable technical success and symptom improvement following ClotTriever thrombectomy in patients with extensive venous thromboembolism. In the present case, the ClotTriever BOLD catheter served as the primary thrombectomy device, while the FlowTriever system was used for aspiration of residual thrombus and temporary embolic mitigation. 9 We acknowledge that the 25-mm FlowTriever disc could not achieve circumferential apposition within the 32-mm suprarenal IVC and therefore should not be considered equivalent to a conventional caval filter. Its purpose was to intercept larger thrombus fragments generated during thrombectomy rather than provide complete embolic protection. Although evidence supporting this strategy remains limited, it represented a pragmatic adjunct when conventional filter placement was considered suboptimal. 10
Successful thrombectomy restored caval patency, resolved lower limb swelling, and allowed staged orthopedic and maxillofacial procedures without thromboembolic complications. Thrombophilia screening was negative, supporting trauma as the provoking factor. Rivaroxaban was continued for nine months because of the extensive iliocaval thrombus burden and the requirement for multiple staged operations. This case demonstrates that combined ClotTriever and FlowTriever mechanical thrombectomy may provide an effective treatment option for selected patients with extensive traumatic iliocaval thrombosis when IVC filter placement is not feasible or is considered unfavorable.
Conclusion
Extensive inferior vena cava thrombosis following blunt trauma is rare and presents significant therapeutic challenges. Management requires careful balancing of thrombotic risk, bleeding risk, and the timing of necessary surgical interventions. In this patient, anatomical limitations reduced the attractiveness of conventional IVC filter placement, while anticoagulation alone was insufficient to address the extensive thrombus burden. Combined ClotTriever BOLD and FlowTriever mechanical thrombectomy achieved successful thrombus clearance, rapid symptom resolution, and facilitated safe subsequent orthopedic and maxillofacial surgery. This case supports the role of mechanical thrombectomy as a valuable treatment strategy for selected patients with extensive traumatic iliocaval thrombosis when IVC filter placement is not feasible or considered suboptimal.
Footnotes
Acknowledgments
The authors would like to acknowledge the contributions of the multidisciplinary team at Hospital Kuala Lumpur, including the trauma, interventional radiology, orthopaedic, and maxillofacial surgery teams, for their collaborative efforts in the management of this patient.
Ethical Considerations
Ethical approval was obtained in accordance with institutional policies.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data relevant to the case are included within the article. Additional details are available from the corresponding author upon reasonable request.