
Abstract
Biofilm formation is a key virulence factor in urinary tract infections, and Escherichia coli (E. coli) serves as a prominent causative agent, more resistant to antimicrobial agents. This study focused on isolation and phenotypic and genotypic characterization of E. coli from urine samples on the basis of their biofilm-forming capacity. In the present study, a total of 804 human urine samples were collected from different clinical facilities of Faisalabad. After phenotypic and genotypic affirmation, biofilm forming potential of uropathogenic E. coli (UPEC) was determined by using microtiter plate assay (MPA) and the Congo red agar method. Antimicrobial susceptibility testing was conducted, and a comparison was executed between biofilm formers and non-formers. Biofilm production by the MPA and Congo red agar methods was 88% and 68%, respectively. UPEC isolates showed maximum resistance to amoxicillin-clavulanate (97%), cefoparazone (93%), cefotaxime (91%), and ampicillin (90%). Significant association between resistance to antibiotic and biofilm formation with p value <0.05 was observed in case of piperacillin-tazobactam, imipenem, meropenem, amikacin, norfloxacin, nitrofurantoin, polymyxin B, and nalidixic acid. Biofilm producer strains were progressed for molecular characterization using polymerase chain reaction for biofilm-forming genes including fimH, csgA, bcsA, agn43, papC, and focG, which showed prevalence of 89% (118/132), 87% (116/132), 86% (114/132), 81% (107/132), 47% (61/132), and 33% (43/132), respectively.
Introduction
Urinary tract infection (UTI) is an infection of the kidney, ureter, bladder, and urethra that can be manifested as pyelonephritis, urosepsis, cystitis, and urethritis, with women being particularly more susceptible. 1 Major UTI causative agents are Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis, Enterococcus faecalis, and Candida albicans. 2
Escherichia coli (E. coli), a notably diverse bacterial species that can occur in varied forms in nature, such as probiotic, commensal, or as a harmful intestinal and/or extraintestinal pathogen affecting humans and animals by causing a spectrum of diseases such as UTI, diarrhea, septicemia, and meningitis in neonates. 3 Among various pathogenic E. coli strains, uropathogenic E. coli (UPEC) is one of them, which is the primary contributing agent of UTI that accounts for the majority of both community-acquired and hospital-acquired infections.4,5
UPEC is a key pathogen in UTI, known for its ability to evade the immune system and resist antibiotic treatment. 6 A major virulence factor contributing to the persistence of UPEC in the urinary tract is biofilm formation. 7 Biofilms allow UPEC to adhere to urinary tract tissues and medical devices such as catheters, creating a protective milieu that shields the bacteria from host immune defenses and antimicrobial agents.8,9 This biofilm-associated lifestyle leads to chronic and recurrent infections, particularly in hospitalized or catheterized patients. In addition to biofilm formation, UPEC employs a variety of additional virulence mechanisms, including adhesins (e.g., type 1 and P fimbriae), siderophores for iron acquisition, and toxins (e.g., hemolysin), all of which contribute to the UPEC capability to cause persistent infections.10,11
Extended-spectrum β-lactamases, symbolized as Extended-Spectrum Beta-Lactamase (ESBL), are microbial enzymes produced by members of Enterobacteriaceae for degradation of antimicrobial agents such as β-lactams as a defensive mechanism. 12 ESBL-producing E. coli have become more common, hence raising concerns about the efficacy of current antibiotics. The increasing prevalence of antimicrobial resistance (AMR) among UPEC strains has further complicated the treatment of UTI. 13 It is among the most prevalent infectious diseases globally, affecting an estimated 150 million people annually. 14 Studies have shown that biofilm-forming strains of E. coli exhibit greater resistance to antibiotics and the immune system. 15 Biofilm formation is a central factor in the persistence and recurrence of UPEC infections. Biofilm production is a leading cause of AMR due to the close proximity of bacterial cells, which promotes cell-to-cell communication for the transfer of determinants related to resistance. Mechanisms include horizontal gene transfer (exchange of DNA between bacteria), quorum sensing (communication system through autoinducers) and upregulation of efflux pump to limit drug penetration. 12 This represents a significant public health concern due to their frequency and the substantial economic burden they impose, with treatment cost running into billions of dollars each year. 16 Understanding the molecular mechanisms behind biofilm formation and the genetic variability of UPEC strains is essential for improving diagnostic, therapeutic and control strategies, primarily in hospital settings where nosocomial infections are rampant. 17 The primary objective of this research is to access resistance patterns between biofilm producers and non-biofilm producers UPEC, particularly focusing on the genetic markers associated with biofilm production.
Materials and Methods
Sample collection and processing
Ethical permission was obtained before starting the study from the Ethical Review Committee of Government College University Faisalabad (GCUF/ERC/24/821). A total of 804 urine samples of patients were collected from various public and private hospitals of Faisalabad. Midstream urine samples were collected in sterile disposable container and processed within 2 hours of collection in the postgraduate laboratory of Government College University Faisalabad. These samples were collected after patients consent and under the approval of the ethical review committee Ref. No. GCUF/ERC/24/617 on Dated 04-02-2024. Samples were processed further under aseptic conditions in a biosafety cabinet. Initially, samples were cultivated on CLED (Oxoid, UK) and MacConkey agar (Oxoid, UK). 18 The selected isolates were characterized based on staining reactions and biochemical characteristics. For more research work, confirmed strains were inoculated on Luria-Bertani (LB) (Oxoid, UK) and incubated at 37°C for 48 hours to obtain well-grown colonies. 19
Genomic DNA isolation and UPEC confirmation
Pure colonies of UPEC were grown in LB broth at 37°C overnight. The GeneJET Genomic DNA Purification Kit (Thermo Scientific, UK) was used for genomic DNA extraction. 20 Molecular identification was carried out through polymerase chain reaction (PCR) targeting the uidA gene, which encodes for the β-glucuronidase enzyme. Amplification was done with primer (uidA-F: ATCACCGTGGTGACGCATGTCGC and uidA-R: CACCACGATGCCATGTTCATCTGC). A reaction mixture of 25 µL was prepared, and the following conditions were accustomed in the thermocycler (BioRad, USA). 21 The PCR protocol involved an initial denaturation at 94°C for 5 minutes, followed by 35 cycles of denaturation (94°C, 30 seconds), annealing (50°C, 40 seconds), and extension (72°C, 50 seconds). A final extension step was executed at 72°C for 10 minutes. 18
Phenotypic confirmation of biofilm-forming UPEC
Congo red agar method
Confirmed UPEC strains were streaked onto a specialized solid growth medium known as Congo red agar (Oxoid, UK). This medium is formulated with BHI broth (37 g/L), sucrose (50 g/L), agar (10 g/L), and Congo red stain (0.8 g/L). Prepared Congo red solution was added to autoclaved agar medium once cooled to 55°C. The culture plates were inoculated with the bacterial strains and incubated aerobically for a period of 24–48 hours at a temperature of 37°C. 22
Microtiter plate assay for detection of biofilm
Each UPEC culture underwent individual overnight incubation in 10 mL of trypticase soy broth (TSB) (Oxoid, UK) at 37°C for a duration of 24 hours, following which they were diluted to a ratio of 1:40 in TSB supplemented with 0.25% glucose. Subsequently, 200 μL of the diluted culture was introduced into a sterile microtiter well. The microtiter plates were incubated at 37°C for an additional 24 hours to stimulate biofilm formation. After this incubation period, the contents within the wells were gently removed by tapping, and the wells were subjected to three to four times washing with phosphate buffer saline (pH = 7.4). Following this step, the biofilm in the microtiter plate well was stained with a 0.1% crystal violet solution for 30 minutes. Subsequent to rinsing with sterile distilled water and thorough drying, the adherent biofilm’s absorbed crystal violet stain that was extracted using 95% ethanol at 4°C. The liquid content within each well was transferred separately to another microtiter well, and absorbance was measured in triplicate at 595 nm utilizing an Enzyme-Linked Immunosorbent Assay plate reader (BioRad, USA). Data interpretation was done by calculating optical density (OD) and subtracting the OD of the negative control well from the OD of the test well. 23
Antibiotic susceptibility testing (AST)
The AST of confirmed UPEC strains was conducted, employing the Kirby-Bauer NCCLS modified disk diffusion assay, against a panel of various available antibiotics. Antibiotic disk (Oxoid™) potencies of 5 µg (ofloxacin, ciprofloxacin, and levofloxacin), 10 µg (ampicillin, imipenem, meropenem, amikacin, tobramycin, trimethoprim, and norfloxacin), 15 µg (clarithromycin), 30 µg (cefazolin, cefotaxime, ceftazidime, ceftriaxone, gentamicin, nalidixic acid, minocycline, and florfenicol), 75 µg (cefoparazone), 100 µg (piperacillin), and 300 µg (nitrofurantoin) were used. Synergistic antibiotics named amoxicillin-clavulanate (20/10 µg), piperacillin-tazobactam (100/10 µg), and sulfamethoxazole-trimethoprim (1.25/23.75 µg) were tested. This assessment was carried out in accordance with the Clinical and Laboratory Standards Institute 2021 guidelines. To initiate this procedure, 0.5 McFarland standard turbid suspension of colonies in sterile saline was prepared, and a sterile cotton swab was used to evenly distribute the inoculum across the surface of Muller-Hinton agar (MHA) (Oxoid, UK). Antibiotic discs of Oxoid™ were meticulously positioned in an aseptic manner onto the surface of the MHA plates, and the plates were incubated at a temperature of 37°C for a duration of 24 hours. 23
Detection of biofilm forming genes in UPEC
Screening of six biofilm-forming genes (csgA, fimH, agn43, focG, papC, and bcsA) was done by conventional PCR. All amplified PCR products were separated electrophoretically in 1% agarose gel containing ethidium bromide. After separation of bands, the gel was photographed under Ultra Violet (UV) light and a digital capture system (Slite 200 W, Taiwan). The 50-bp ladder was used as a standard to assess the molecular size of PCR products. 24 The primer sequences, thermal profile, and size of amplified fragments (base pair) are shown in Table 1.
Biofilm Forming Genes Used in This Study and Their PCR Primers
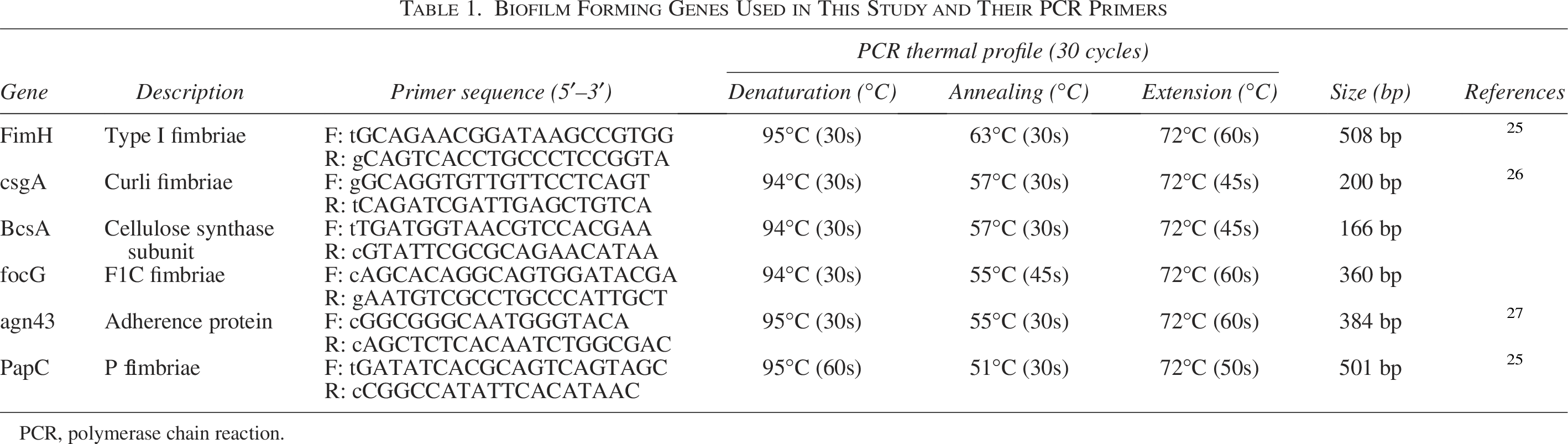
PCR, polymerase chain reaction.
Results
Phenotypic and genotypic identification of UPEC
In this study, a total of 804 urine samples was processed. From these total samples, 194 samples (24%) were positive for UPEC growth, covering 66% female and 34% male patients. Phenotypic confirmation was done by obtaining pink-colored colonies on MacConkey agar, Gram-negative rods under a microscope, γ-hemolysis (non-hemolytic nature) on blood agar, and Indole, Methyl Red, Voges-Proskauer, and Citrate biochemical tests. Phenotypically confirmed UPEC isolates were further confirmed at the genetic level by amplification of the uidA gene-specific primer. Bands of 486 bp were observed under UV light (Slite 200 W, Taiwan) in ethidium bromide-stained 1.7% agarose gel.
Phenotypic detection of biofilm-forming UPEC
The Congo red agar test was performed to assess biofilm formation, with strains showing black colonies considered positive for biofilm production. The percentage of positive biofilm-producing strains was 68%. For the microtiter plate method, bacterial cultures were incubated in TSB for 24 hours and transferred to microtiter wells for biofilm formation at 37°C for another 24 hours. Absorbance of crystal violet stained wells was measured at 595 nm to assess biofilm formation, with OD values calculated and compared to negative and positive controls. The negative control OD was 0.07, and the calculated ODc was 0.149. Based on threshold ranges, isolates were categorized as non-biofilm producers (≤0.149), weak (0.150–0.298), moderate (0.299–0.596), and strong (>0.596) according to the criteria described by Stepanovic. 28 The highest percentage was found (42%) of moderate biofilm producing UPEC followed by weak biofilm producers (32%). Strong biofilm producers were 13%. Results showed that the percentage of biofilm-producing strains was 88%. The comparison between the microtiter plate assay (MPA) and Congo Red Agar (CRA) methods is illustrated in Table 2.
Biofilm Forming and Non-Biofilm Forming UPEC Isolates by CRA and MPA Method
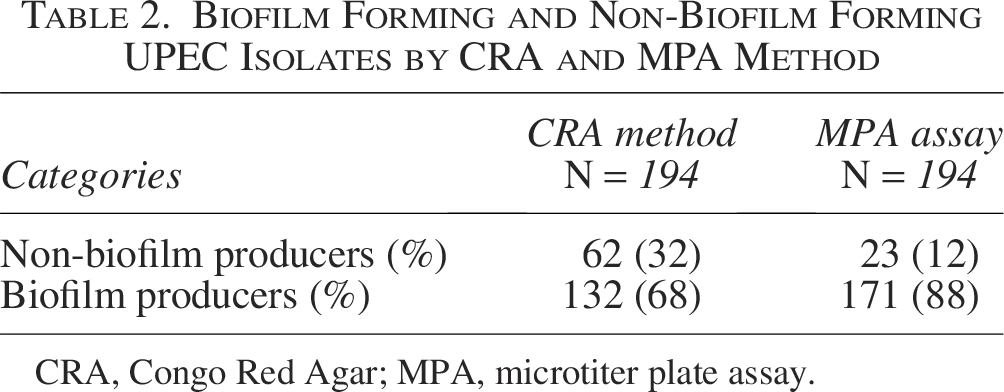
CRA, Congo Red Agar; MPA, microtiter plate assay.
Antibiogram analysis of UPEC
UPEC strain inoculum was spread smoothly on Muller-Hinton agar plates, and then antibiotic discs were positioned with a disc dispenser. After overnight incubation, results were noted. The data were analyzed by Microsoft Excel for the calculation of percentages. Statistical analysis was performed using the chi-square test in Statistical Package for the Social Sciences (Fig. 1). Sample strains showed variable levels of resistance to antibiotics. All isolates showed more than 90% resistance to ampicillin, amoxicillin-clavulanate, cefotaxime, and ceftazidime. Below these, the highest level of resistance was observed against piperacillin (88%), cefazolin (87%), ceftazidime, ceftriaxone, and levofloxacin (88%).
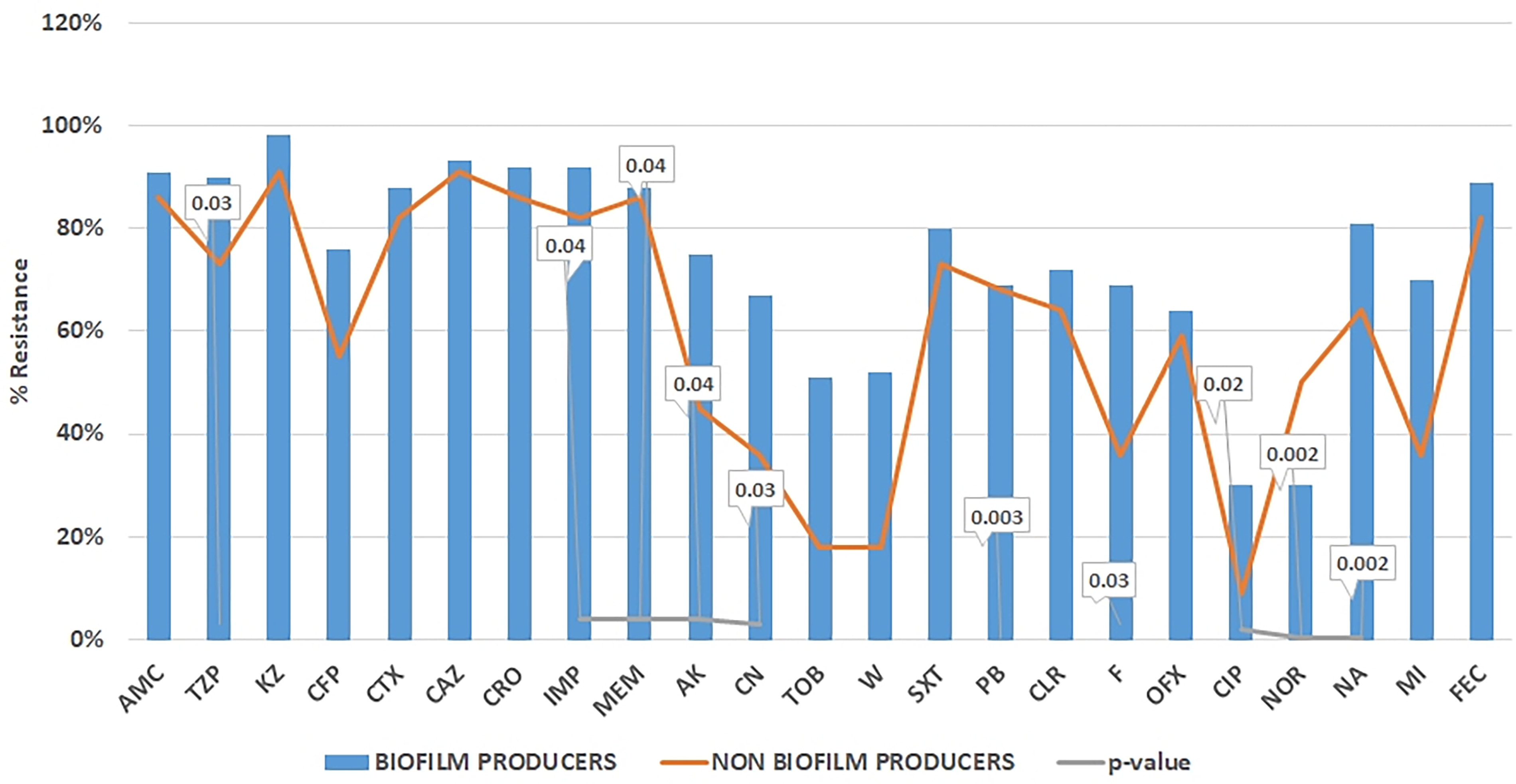
Percentage resistance among UPEC biofilm formers and non-biofilm formers. Significant p-values are displayed as callouts above corresponding antibiotic. AK, amikacin; AMP, ampicillin; AMC, amoxicillin-clavulanate; CN, gentamicin; CAZ, ceftazidime; CFP, cefoparazone; CIP, ciprofloxacin; CLR, clarithromycin; CTX, cefotaxime; CRO, ceftriaxone; F, nitrofurantoin; FEC, florfenicol; IMP, imipenem; KZ, cefazolin; LEV, levofloxacin; MI, minocycline; MEM, meropenem; NA, nalidixic acid; NOR, norfloxacin; OFX, ofloxacin; PB, polymyxinB; PRL, piperacillin; SXT, sulfamethoxazole trimethoprim; TOB, tobramycin; TZP, piperacillin-tazobactam; W, trimethoprim.
Non-biofilm-forming strains showed significantly lower resistance to key antibiotics, especially amikacin, piperacillin, gentamycin, minocycline, imipenem, polymyxin B, and nitrofurantoin. Even though there was no significant correlation of antibiotic resistance between biofilm producers and non-biofilm producers for Ampicillin, Piperacillin, AMC, Florfenicol, Tobramycin, W, and Trimethoprim. Still, higher rate of resistance among biofilm producers was observed compared to non-biofilm producer. Imipenem and nitrofurantoin showed the lowest resistance, indicating efficacy against both types of species.
Among all UPEC isolates, 15% (n = 29) were found to be Extensively Drug-Resistant (XDR), 59% (n = 114) Multi-Drug Resistance (MDR), and 26% (n = 51) showed results of non-MDR. A higher proportion of MDR isolates were biofilm producers. Distribution of resistance phenotypes among different biofilm production capacities displayed as a percentage stacked bar graph (Fig. 2). Chi-square distribution test results (χ2 = 11, df = 2 and p > 0.05) suggested a substantial correlation among biofilm producers and resistant phenotypes (MDR and XDR).
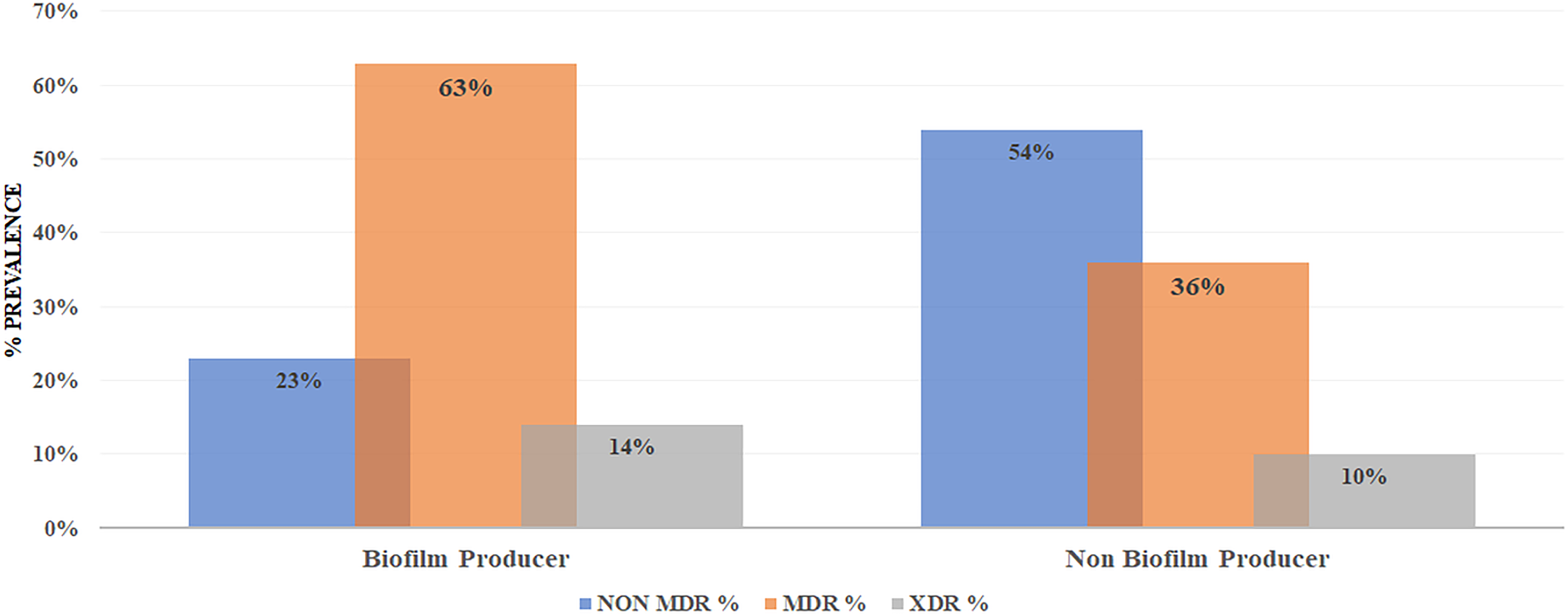
Distribution of resistance phenotypes among isolates.
Detection of biofilm-forming genes of E. coli
Specific primers (Table 1) were used to detect the presence of the csgA, fimH, agn43, focG, papC, and bcsA genes in order to demonstrate the presence of these genes in biofilm-forming UPEC isolates. The results showed that 79 out of the 88 isolates (89.65%) have fimH gene. Bands after gel electrophoresis under a UV illuminator (Slite 200 W, Taiwan) were observed (Fig. 3). The most predominant genes after fimH were csgA, bcsA, and agn43, with prevalences of 87.93% (116/132), 86.20% (114/132), and 81.03% (107/132) respectively. Moreover, less than 50% of prevalent genes were focG and papC, having prevalence of 33% and 47%, respectively.
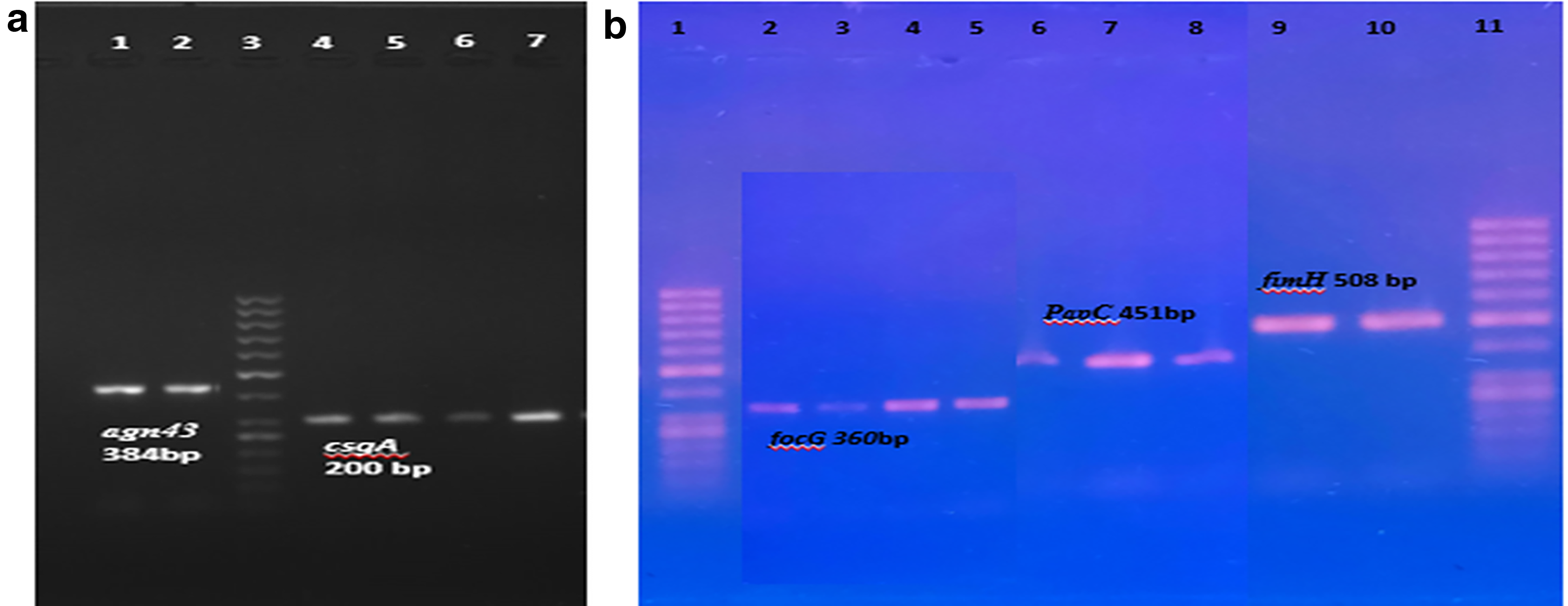
Agarose gel electrophoresis of polymerase chain reaction (PCR) product for biofilm formation genes.
Discussion
UPEC poses a major health threat globally, causing UTI. The ability of UPEC to form biofilms significantly worsens infections through biological mechanisms like horizontal gene transfer, quorum-sensing and efflux pump, making them more persistent and challenging to treat. 29 UPEC utilizes virulence factors to generate biofilms, escalating infection severity and unveiling of molecular mechanisms are crucial for its survival in the urinary tract. 8
In the present study, a total of 804 urine samples were collected, and 25% were found positive for UPEC, with most prevalence (66%) in female patients. The finding of our research in the context of prevalence was very close to the previous observations, 34% in Faisalabad, 26 33% in Multan, 30 and 34% in Lahore. 31 The lower prevalence in our results is due to inclusive sample selection criteria, as all samples received at the hospital laboratory were processed. This broader approach includes diverse cases, not just those with a high likelihood of infection, resulting in lower prevalence compared to studies with more selective criteria.
Among genotypically confirmed UPEC isolates, the majority of the isolates, 88%, were biofilm formers by MPA. This was similar to many previous studies22,32,33 who reported biofilm prevalence at the rates of 91%, 88.4%, and 71%, respectively.
The antibiotic resistance pattern of biofilm- and non-biofilm-forming UPEC isolates demonstrated a significant correlation between biofilm formation and multidrug resistance. Among all isolates 59% were found to be MDR and a higher proportion of these isolates were biofilm producers. This result is consistent with the results of 34 who reported that 87% biofilm producers are MDR. There was absolute resistance toward amoxicillin-clavulanate, cefotaxime, and ceftazidime in this study. Our study is in accordance with the reports from different centers35–37 indicating resistance against β-Lactam combination agents and 3rd-generation cephalosporins in Pakistan. In the present study, the most sensitive drugs were gentamicin, amikacin, florfenicol, and nitrofurantoin with less than 30% resistance. These results agreed with findings of.37,38
In contrast to free-floating cells, there are several mechanisms, such as quorum sensing, gene transfer, and efflux pump in biofilms, that promote AMR. 39 These mechanisms increase the resilience toward broad-spectrum antibiotics and cause complications that are difficult to treat. There is a strong affiliation of biofilm producers with multidrug-resistance especially in long-term hospital stays, that complicate general UTIs. 40 This is main challenge for antibiotic stewardship and control of infection, hence emphasizing the dire need of alternative antibiofilm therapies.
The results showed that 87.93% have the csgA gene (curli gene). This result is consistent with the results of26,41 who reported that biofilm-forming UPEC isolates carry csgA gene with prevalence rate of 65% and 91%, respectively. The results in this study show that 57 out of 60 isolates (95%) have the fimH gene, helps bacteria to attach to the epithelial cells in the urinary tract, which is considered the first step of infection and biofilm formation. The present results agreed with, 22 who detected that 96.8% of the isolates were positive for the fimH gene. Other studies submitted by42,43 demonstrated positive isolates with 53.5% and 91.8%, respectively.
The prevalence of the other 4 genes (bcsA, agn43, papC, and focG) in our study was close to the results of previous studies,38,41,44 which confirmed the prevalence of these genes in biofilm forming UPEC.
This study has limitation, regarding the evaluation of disease outcomes or any effect of recurrence in biofilm-related infections. Moreover, investigation of clinical parameters was not considered that could provide deeper insights.
Conclusion
This study investigated the complex interplay between UPEC AMR and biofilm formation, highlighting their clinical relevance in UTI. By analyzing isolates and employing methods such as Congo red agar and MPAs, along with genotypic evaluations, this study has provided significant insights.
Authors’ Contributions
Saman: Methodology, formal analysis, investigation, data curation, and writing—original draft. A.B.S.: Supervision and project administration. B.A.: Resources, editing, and validation. Z.N.: Conceptualization, editing, and visualization.
Footnotes
Funding Information
This research received no external funding.
Disclosure Statement
No competing financial of interests exist.