
Abstract
Background:
This study aimed to determine the prevalence of carbapenem-resistant Enterobacterales (CRE), to characterize their molecular resistance mechanisms, and to assess associated clinical outcomes among intensive care unit (ICU) patients in Tunisia.
Methods:
A cross-sectional study was conducted from January to March 2025 in the ICU of Habib Thameur Hospital and included all patients with clinically significant CRE infections. Resistance determinants were identified using multiplex polymerase chain reaction with reverse dot blot hybridization.
Results:
Among 95 ICU admissions, 17 patients developed CRE infections, corresponding to an incidence density of 21.6 cases per 1,000 patient-days. All infections were hospital-acquired. The most frequent risk factors were the presence of central venous and urinary catheters (16 patients each) and mechanical ventilation (15 patients). Klebsiella pneumoniae predominated, accounting for 26 of 27 isolates, all of which were multidrug-resistant (MDR), with a median antibiotic resistance index of 1.00. The blaNDM and blaOXA-48 genes were detected in 81.5% and 77.8% of isolates, respectively, with 70.4% co-producing both carbapenemases. All K. pneumoniae isolates harbored blaSHV and/or blaCTX-M, while a single Escherichia coli isolate carried blaOXA-48. Cluster analysis revealed strong associations between β-lactamase production and resistance to aminoglycosides and fluoroquinolones, suggesting co-selection of MDR strains. Empirical antimicrobial therapy was appropriate in only 47% of cases, and ICU mortality reached 82.4%.
Conclusion:
These findings highlight an alarmingly high burden of CRE infections in this ICU, driven mainly by K. pneumoniae co-producing NDM and OXA-48, and underscore the urgent need for strengthened infection control and antimicrobial stewardship strategies.
Introduction
Antimicrobial resistance is a growing global health threat. It compromises the treatment of infections, increases morbidity and mortality, and imposes substantial health care costs.1,2 The prevalence of multidrug-resistant (MDR) organisms has been rising worldwide. Intensive care units (ICUs) are recognized as hotspots for the emergence and spread of these pathogens. 3
ICU patients are particularly vulnerable. Severe underlying illnesses, immunosuppression, and frequent invasive procedures such as mechanical ventilation, intubation, and vascular access increase the risk of infection. 4 Impaired protective mechanisms, including reduced cough and swallowing reflexes, decreased gastric acid secretion, and disrupted normal microbiota, further enhance susceptibility. 5 The burden of ICU-acquired infections is especially high in low- and middle-income countries, where resources for infection prevention and antimicrobial stewardship are limited. 6
Among MDR organisms, carbapenem-resistant Enterobacterales (CRE) are classified as critical priority pathogens by the World Health Organization (WHO). 7 CRE infections cause high morbidity, mortality rates of up to 50%, prolonged hospital stays, and increased costs. 8 Resistance mechanisms include enzymatic drug inactivation, target modification, reduced drug uptake, and active efflux. 9 These mechanisms often confer multidrug resistance and severely limit treatment options. Current therapies rely on colistin, high-dose carbapenems, and novel β-lactam/β-lactamase inhibitor combinations, whose efficacy varies depending on the carbapenemase type. 10 Phenotypic testing is essential in low-resource settings to optimize therapy.
The prevalence of CRE in Tunisia has steadily increased over time. Data from the “L’antibiorésistance en Tunisie” (LART) surveillance system demonstrates a rising trend of carbapenem resistance among Enterobacterales. 11 Despite this, data on CRE prevalence, molecular characteristics, and risk factors in ICUs remain scarce. 12 Understanding the local epidemiology is crucial for guiding infection prevention, optimizing empirical therapy, and informing antimicrobial stewardship programs. 13
This study aimed to determine the incidence, molecular characteristics, and risk factors associated with CRE infections among ICU patients at a tertiary-care hospital in Tunisia.
Methods
Study design and bacterial isolates
This cross-sectional study was conducted from January 1 to 31 March 2025, at Habib Thameur Hospital, Tunis, Tunisia. Clinical specimens were collected from patients admitted to the ICU. All patients admitted to the ICU of Habib Thameur Hospital in Tunis, regardless of the reason for admission, during the period from January to March 2025, were eligible. Patients were included if at least one of their clinical samples tested positive for CRE. Duplicate isolates from the same patient, obtained from identical specimen types with the same resistance profile, were excluded. Isolates from colonization screenings were not included.
Data collection and demographic variable definitions
Demographic, clinical, microbiological, and treatment-related data were extracted from patients’ medical records by investigators and entered into a secure, standardized data collection tool. Additional laboratory results were retrieved from local laboratory information management systems.
For each patient, data collected included demographic characteristics, underlying comorbidities, and risk factors associated with the acquisition of MDR organisms. Comprehensive details related to CRE infections were documented, including infection site, identified bacterial species, antimicrobial susceptibility profiles, resistance mechanisms, time to infection onset, and antimicrobial treatments administered.
Furthermore, information regarding the management of critically ill patients was collected, including the use of invasive procedures such as mechanical ventilation, central venous catheter placement, urinary catheterization, intra-abdominal or prosthetic device insertion, and vasopressor support. Patient outcomes, including ICU length of stay and mortality, were also analyzed. Incidence density was calculated as the number of CRE infection cases per 1,000 patient-days, using the total length of ICU stay for all included patients.
Definitions
An episode of infection was defined as the isolation of CRE in the presence of compatible signs or symptoms. 4
Health care-associated infections (HCAI) and those infections present on admission were included. Infection occurring >48 hours after admission to the hospital was defined as HCAI. 6
Empirical antibiotic therapy was considered inappropriate if it did not include at least one antibiotic active against the CRE in vitro. 10
Microbiological processing and bacterial identification
All samples were processed according to standard microbiological procedures following the recommendations of the Référentiel en Microbiologie Médicale (REMIC) guidelines. 14 Preliminary identification was based on colony morphology and Gram staining. Further biochemical identification of Enterobacterales isolates was performed using the API 20E system (bioMérieux, Marcy l’Etoile, France).
Antimicrobial susceptibility testing
Antimicrobial susceptibility of all CRE isolates was assessed using the standard Kirby-Bauer disk diffusion method on Mueller–Hinton agar (Bio-Rad, Marnes-la-Coquette, France), following the 2024 recommendations of the Antibiogram Committee of the French Society for Microbiology (CA-SFM).
The antibiotics tested included: amoxicillin (20 μg), amoxicillin/clavulanic acid (30 μg), piperacillin (30 μg), piperacillin/tazobactam (36 μg), cefepime (30 μg), ceftazidime (10 μg), cefotaxime (5 μg), cefoxitin (30 μg), ceftazidim/avibactam (14 μg), imipenem (10 μg), ertapenem (10 μg), aztreonam (30 μg), ciprofloxacin (5 μg), gentamicin (10 μg), amikacin (30 μg), and fosfomycin (200 μg). The results were interpreted according to the recommended criteria and E. coli ATCC 25922 was the quality control strain.
Colistin susceptibility testing
The minimum inhibitory concentrations (MICs) of colistin were determined using the broth microdilution method. Colistin resistance was defined as MIC > 2 mg/L.
Antibiotic resistance indexes
The antibiotic resistance index (ARI) was calculated as the ratio of the number of antibiotics to which a strain was resistant divided by the total number of antibiotics used in susceptibility testing. 15
Detection and molecular characterization of the antimicrobial-resistant genes
CRE refer to members of the Enterobacterales family that have acquired resistance to at least one carbapenem antibiotic (imipenem, meropenem, doripenem, or ertapenem), based on the MIC breakpoints defined by Comité de l'Antibiogramme de la Société Française de Microbiologie/European Committee on Antimicrobial Susceptibility Testing. 16
To characterize the resistance mechanisms involved, the identification of carbapenemase genes was performed via molecular detection methods using multiplex PCR assays, combined with an automated reverse dot blot hybridization system, to detect genes encoding the most prevalent β-lactamases. 17
These included extended-spectrum beta-lactamases (ESBLs) such as blaCTX-M and blaSHV; plasmid-mediated AmpC beta-lactamases (blaCMY, blaDHA); and carbapenemases from classes A, B, and D (blaKPC, blaGES, blaSME, blaNMC/IMI, blaVIM, blaGIM, blaSPM, blaNDM, blaSIM, blaIMP, blaOXA-23, blaOXA-24, blaOXA-48, blaOXA-51, blaOXA-58). Mutated variants of blaSHV were also screened, including blaSHV-S (G238S) and blaSHV-SK (G238S and E240K). In addition to β-lactamase genes, resistance determinants for other antibiotic classes were also targeted. These included sulfonamide resistance genes (sul-1, sul-2, sul-3), aminoglycoside resistance genes (aac(6′)-Ib, armA, rmtB, rmtC, rmtF), and plasmid-mediated quinolone resistance genes (qnrA, qnrB, qnrS). 17 Quality control was performed using Escherichia coli ATCC 25922.
Statistical analysis
Statistical analyses were performed via Statistical Package for Social Sciences (SPSS) version 23.
For descriptive analysis, categorical variables were presented as absolute numbers and their relative percentages; continuous variables were summarized as median and interquartile range (IQR). A p value of <0.05 was considered statistically significant. The Kolmogorov–Smirnov test was used to verify the normality of the distribution of quantitative variables. To visualize the relationships between resistance gene profiles, we generated correlation matrix heatmaps via the R software (version 4.3.2).
Hierarchical clustering analysis based on the binary presence/absence matrix of resistance genes was performed to assess similarity patterns among isolates. This approach enabled the visualization of groups sharing comparable antimicrobial resistance determinants.
Ethical approval
The Hospital’s Ethics Committee of Habib Thameur Teaching Hospital (IRB00014475) approved this study (Approval number HTHEC-2025-15).
Results
Clinical and epidemiological characteristics of included patients
Between January 1 and March 31, 2025, a total of 95 patients were admitted to the ICU. Among them, 17 developed an infection caused by CRE, corresponding to a proportion of 17.9%. The incidence density of CRE infections was 21.6 cases per 1,000 patient-days.
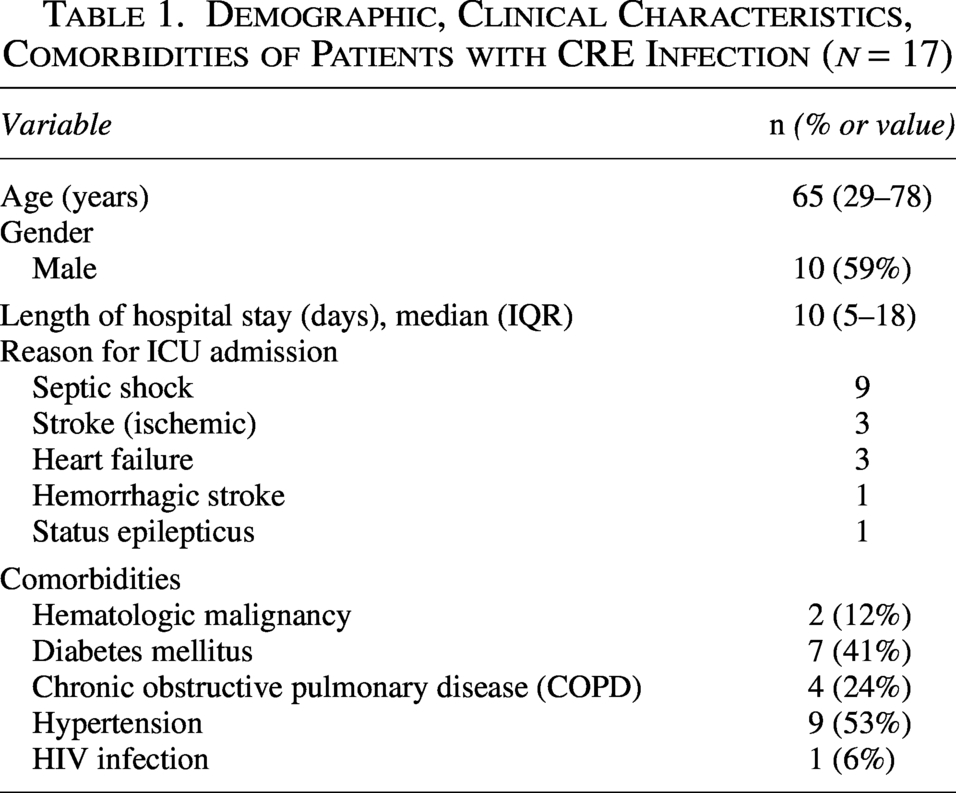
Seven out of 17 patients were female, and the median age was 65 years, with extremes ranging from 29 to 87 years. All patients had at least one underlying medical condition. The primary reasons for ICU admission were septic shock (9/17), heart failure (3/17), and stroke (3/17) (Table 1).
Demographic, Clinical Characteristics, Comorbidities of Patients with CRE Infection (n = 17)
Risk factors of MDR
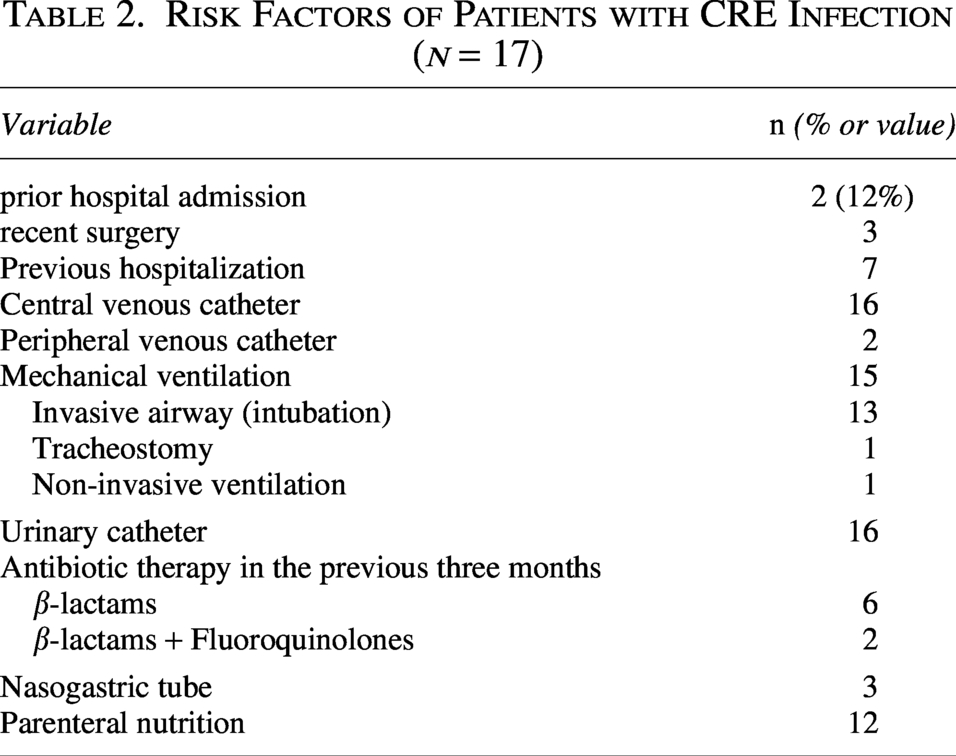
Multiple clinical and procedural factors were common among patients with CRE infection, notably the high rate of mechanical ventilation. Table 2 provides a detailed summary of these risk factors (Table 2).
Risk Factors of Patients with CRE Infection (n = 17)
Microbiological characteristics
The mean time from ICU admission to the first positive culture for CRE was 6 days, ranging from 2 to 12 days. Nosocomial acquisition was identified in 100% of cases.
A total of 27 nonduplicate CRE isolates were recovered from 17 patients, indicating multiple isolates per patient. Ten patients had a single isolate, four had two isolates, and three had three isolates.
CRE isolates were predominantly recovered from respiratory specimens, including sputum and protected tracheal aspirates (9/27), followed by urine samples (6/27). The most frequent Healthcare-Associated Infection was hospital-acquired pneumonia (9 cases). Catheter-related infections and urinary tract infections were observed with equal frequency (6 cases each). The predominant causative organism was Klebsiella pneumoniae, identified in 26 out of 27 CRE isolates, while E. coli was found in one isolate. K. pneumoniae was isolated from 16 of 17 patients.
All CRE isolates were resistant to penicillin, amoxicillin–clavulanic acid, piperacillin–tazobactam, third-generation cephalosporins, cefepime, and ertapenem. Six isolates were susceptible to ceftazidime–avibactam, while none showed susceptibility to aztreonam. Regarding fluoroquinolones, only one isolate was susceptible to ciprofloxacin. A total of 20 CRE isolates were resistant to amikacin. Notably, four isolates were pan-resistant, showing resistance even to colistin and fosfomycin (Fig. 1).
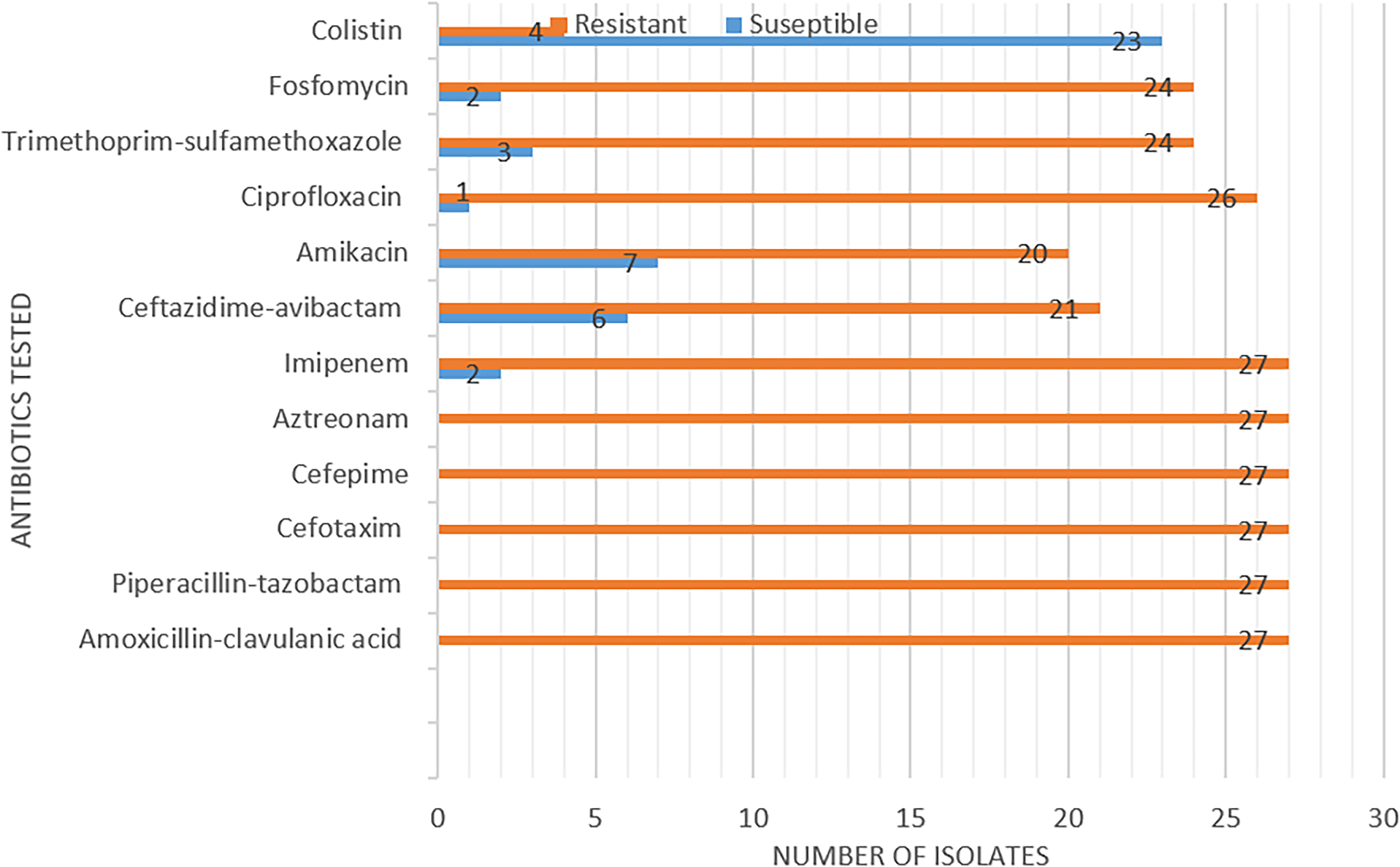
Antibiotic susceptibility profile in carbapenemase-resistant Enterobacterales (n = 27).
The ARI among all isolates ranged from 0.50 to 1.00. K. pneumoniae isolates (n = 26) demonstrated a high resistance burden, with ARI values ranging from 0.70 to 1.00 and a median ARI of 1.00. Consistently, the single E. coli isolate showed an ARI of 0.60.
Molecular characterization of carbapenemase and resistance genes
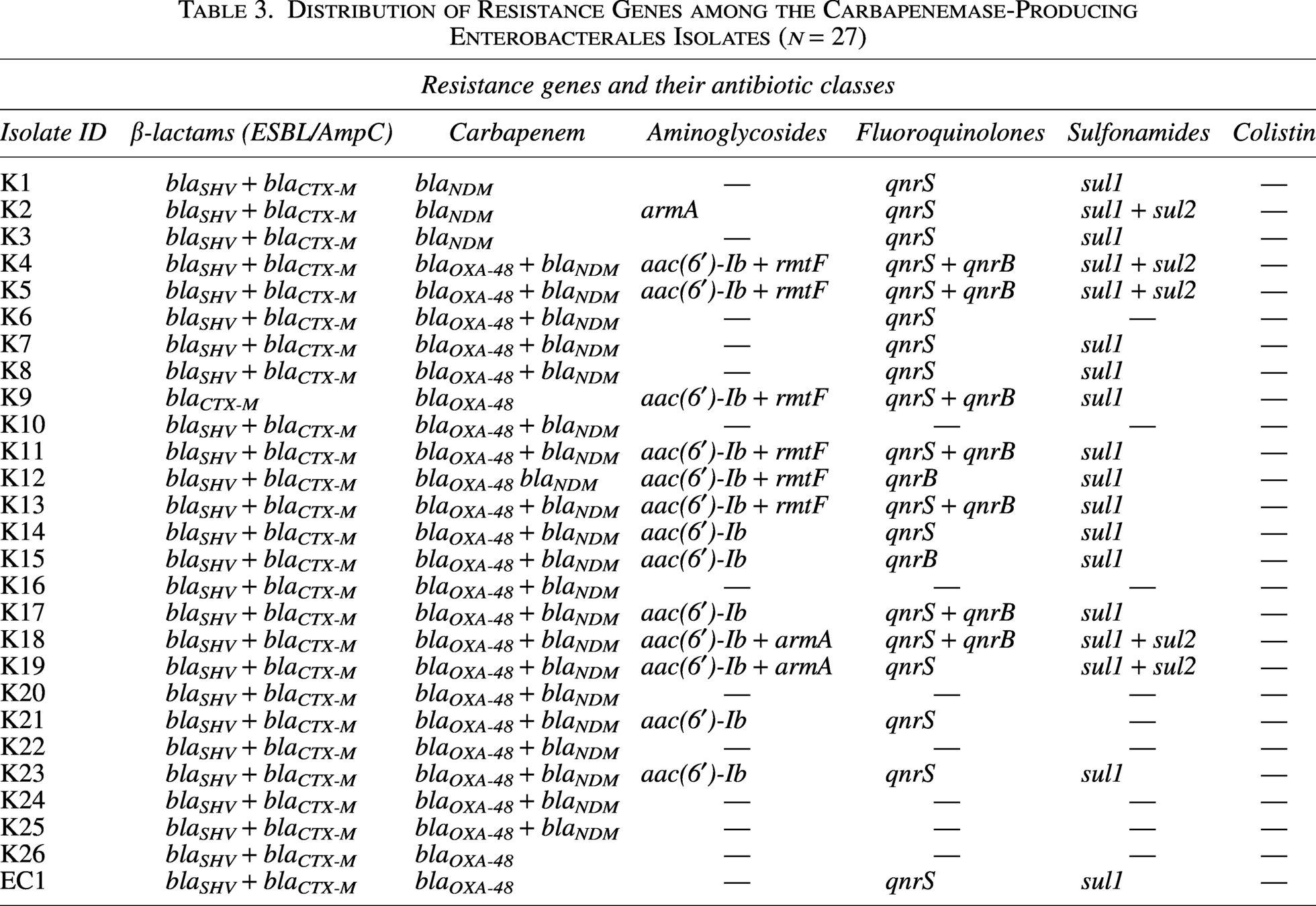
Molecular analysis revealed that all 27 CRE isolates were carbapenemase-producing Enterobacterales (CPE). The most common carbapenemase gene detected was blaNDM (22/27, 81.5%), followed by blaOXA-48 (21/27, 77.8%). Co-existence of both blaNDM and blaOXA-48 genes was observed in 70.4% (19 out of 27 isolates). Notably, for patients with multiple CRE-positive samples, the same carbapenemase gene was consistently identified across all isolates.
All isolates coharboring blaNDM and blaOXA-48 carbapenemase genes were identified as K. pneumoniae and also carried blaSHV and blaCTX-M encoding extended-spectrum β-lactamases (ESBLs). The single E. coli isolate harbored blaOXA-48, blaSHV and blaCTX-M. Additional resistance genes, including 16S rRNA methylases (armA, rmtF), aminoglycoside acetyltransferase (aac(6′)-Ib), quinolone resistance genes (qnrS, qnrB), and sulfonamide resistance genes (sul1, sul2) were variably detected among the isolates. The distribution of resistance genes among the isolates is summarized in Table 3.
Distribution of Resistance Genes among the Carbapenemase-Producing Enterobacterales Isolates (n = 27)
Clustering patterns and correlation of resistance genes
Hierarchical clustering analysis (dendrogram) revealed three main gene clusters among the CRE isolates. The first cluster grouped β-lactamase genes (blaNDM, blaOXA-48, blaCTX-M, and blaSHV). The second cluster comprised aminoglycoside and sulfonamide resistance genes (armA, sul2). The third cluster included quinolone resistance genes (qnrB, qnrS) together with aac(6′)-Ib, rmtF, and sul1.
The correlation heatmap confirmed these associations, showing strong positive correlations (r > 0.7, p < 0.01) between qnrB, aac(6′)-Ib, and rmtF, as well as between blaOXA-48, blaCTX-M, and blaSHV, consistent with their clustering pattern (Fig. 2).
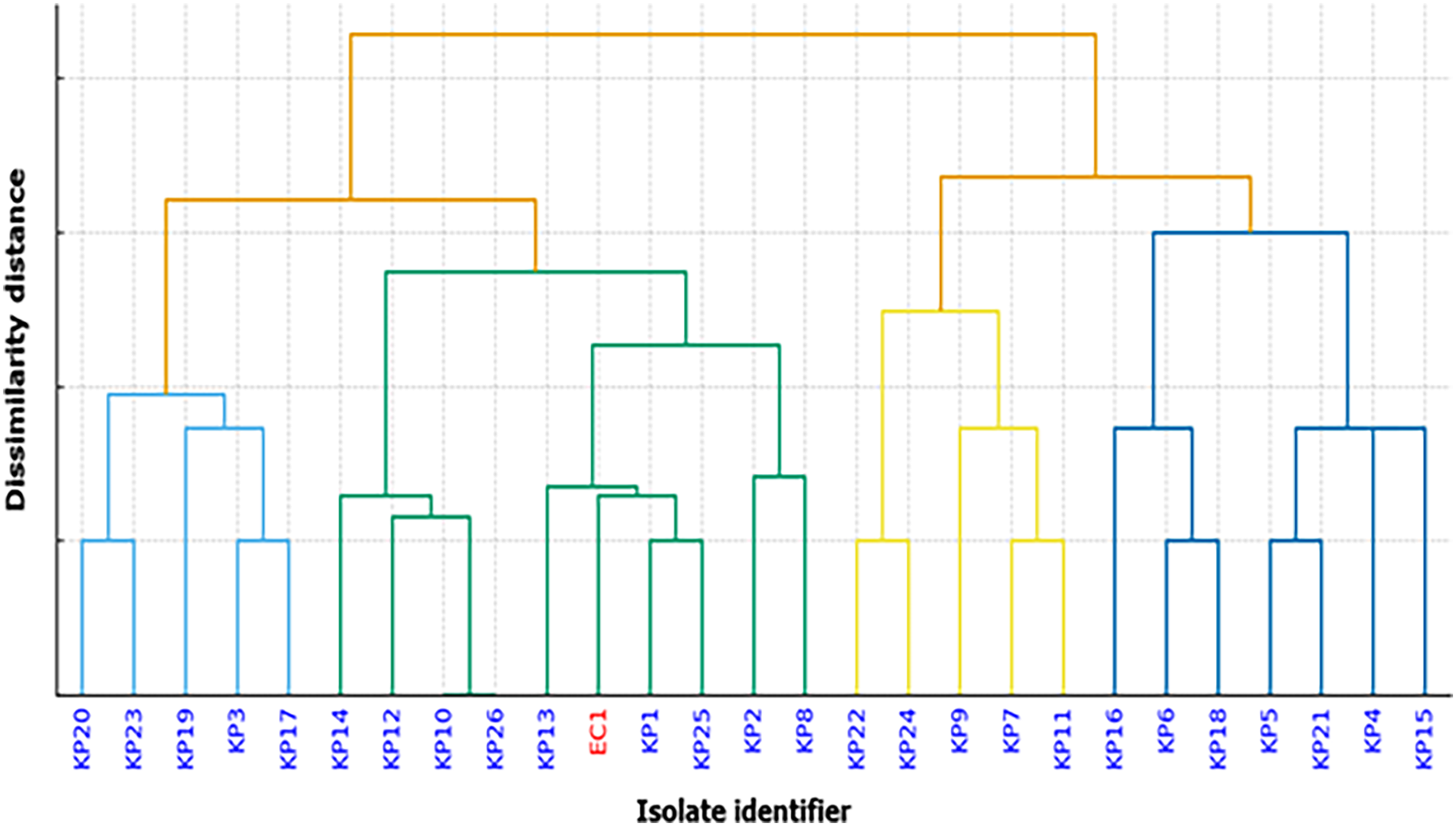
Hierarchical clustering of clinical isolates based on antimicrobial resistance gene profiles. Hierarchical clustering was performed using the presence/absence matrix of resistance genes. The dendrogram groups isolates according to similarities in their resistome composition. Species labels are color-coded for clarity (blue: K: Klebsiella pneumoniae; red: EC: Escherichia coli).
Hierarchical clustering patterns in CRE isolates
The dendrogram (Fig. 3) revealed four distinct resistance clusters among the 26 K. pneumoniae isolates and the single E. coli isolate. Interestingly, the E. coli isolate clustered closely with a subset of K. pneumoniae isolates.
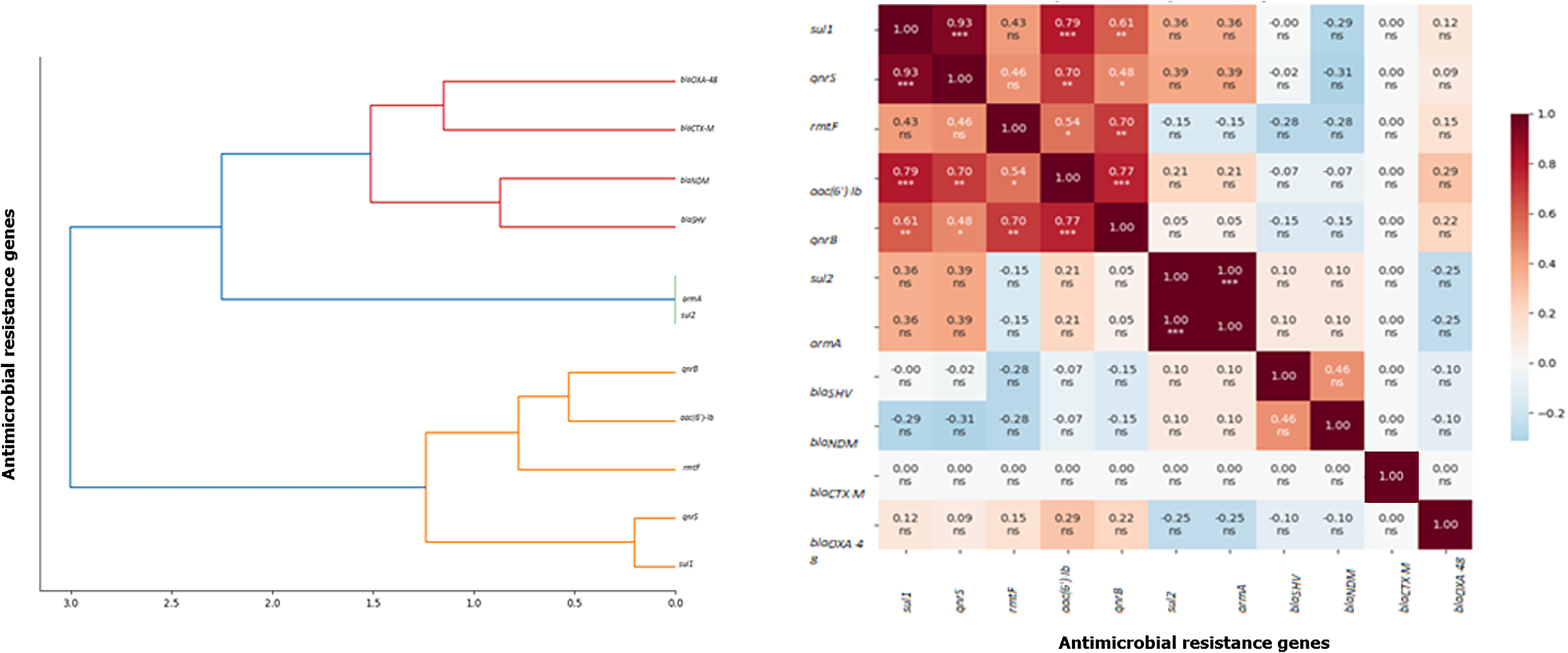
Hierarchical clustering and correlation Heatmap of antimicrobial resistance genes among carbapenem-resistant Klebsiella pneumoniae isolates. ***p < 0.001, **p < 0.01, *p < 0.05, ns: not significant, Color scale: Spearman correlation coefficient (ρ).
Treatment and clinical outcomes
Empirical antibiotic treatment was adequate (included ≥1 in vitro active agent) in 8 out of 17 cases (47%). Antibiotic therapy was subsequently adjusted in 7 patients. Empirical therapy consisted of monotherapy in 1/17 (5.9%), dual therapy in 9/17 (52.9%), and triple therapy in 4/17 (23.5%) cases. Colistin-based combinations were the most frequently prescribed regimens.
The overall mortality rate among patients was high, reaching 82.4% (14 out of 17 patients). When analyzing outcomes according to the detected carbapenemase genes, no significant difference in mortality was observed between the different genetic profiles (p = 0.88). Among patients harboring blaOXA-48, five out of six (83.3%) died, whereas the single patient carrying blaNDM also died. In contrast, among those coharboring blaOXA-48 and blaNDM, 8 out of 10 (80%) patients died.
Similarly, the median length of hospital stay did not differ significantly between groups (p = 0.86): 8 days (range 3–24) for patients with blaOXA-48, 7 days for blaNDM and 10 days (range 7–19) for those carrying both blaOXA-48 and blaNDM.
Discussion
In this study, we analyzed local epidemiological data to better characterize ICU-acquired CRE infections.
To the best of our knowledge, this is the first Tunisian study to investigate the molecular profile of resistance determinants beyond carbapenemase genes in CRE isolates causing ICU-acquired infections. Such investigations remain scarce in Tunisia and the broader Maghreb region, despite the increasing clinical impact and epidemiological spread of CRE. Our findings, therefore, fill an important gap in regional surveillance and contribute valuable data to guide antimicrobial stewardship and infection control strategies. 12
However, this study has several limitations that should be acknowledged. The relatively small sample size and short study duration may limit the statistical power and generalizability of the findings. Consequently, no multivariate analysis was performed, and potential associations should be interpreted descriptively.
In addition, although targeted molecular detection using multiplex PCR was conducted, more advanced genomic approaches, such as whole-genome sequencing, were not available, which limited further exploration of transmission dynamics and genetic relatedness.
Despite these limitations, the study provides valuable insights into the burden and molecular epidemiology of CRE in ICU settings and contributes meaningful data to a region where such information remains limited.
HAIs remain a major concern in ICUs, where critically ill and immunocompromised patients are highly exposed to invasive procedures. 3 Infection rates in ICUs are up to ten times higher than in other hospital wards, and approximately 71% of these infections involve MDR organisms. 1 Among them, CRE represent a critical threat due to their rapid spread and limited therapeutic options. 2 This high prevalence is likely attributable to the high-risk profile of our ICU population, particularly the widespread use of invasive devices such as mechanical ventilation. In our study, the proportion of ICU patients who developed ICU-acquired CRE infections reached 17.9%. The incidence density of 21.6 cases per 1,000 patient-days further highlights the substantial burden of CRE infections in our ICU. Our findings are comparable to the 27.7% reported at Sahloul University Hospital in Sousse. 18 This concordance highlights the growing burden of these pathogens in critical care settings in Tunisia. A multicenter point-prevalence survey conducted before the COVID-19 pandemic among 226 ICU patients in 9 university hospitals across Tunisia, Morocco, Egypt, and Lebanon reported CRE rates ranging from 16.1% to 69.0%, confirming the wide regional heterogeneity within the Mediterranean area. 19 Similarly, the European Centre for Disease Prevention and Control surveillance report (2022–2023) documented a CRE prevalence of 9.3% across Europe, with markedly higher rates observed in Greece (40.8%) and Romania (42.9%). 20 In contrast, a multicenter study conducted in 24 ICUs in Anhui, China, reported a lower prevalence of 8.5% for ICU-acquired CRE infections. 21 These differences likely reflect disparities in infection control policies, antibiotic consumption patterns, and local epidemiological pressures. Together, these findings emphasize the complex and dynamic nature of CRE dissemination worldwide and the need for region-specific strategies to curb their spread.
In this study, CRE were most frequently isolated from respiratory specimens (8/17), consistent with the high prevalence of ventilator-associated pneumonia among the 15 mechanically ventilated patients. These findings align with reports from an adult ICU in Marrakesh, Morocco, where pneumonia (39%), bacteremia (29%), and catheter-related bloodstream infections (17%) predominated reinforcing the well-established link between invasive procedures and CRE emergence in critically ill populations. 22
K. pneumoniae was the predominant species, accounting for 26 of 27 isolates and detected in 16 of 17 patients, corroborating its status as the leading CRE pathogen globally and regionally.23–25 Recent Egyptian ICU data report CRKP prevalence ranging from 14.2% to 66%, 26 a variability attributable to clonal expansion and horizontal gene transfer via plasmids, transposons, and integrons encoding multiple resistance determinants. 27 Given its critical threat level, the WHO (2024) designates carbapenem-resistant K. pneumoniae as a priority critical MDR organism, urgently warranting novel therapeutics. 7 In our study, the antimicrobial susceptibility patterns were alarming. All isolates were resistant to β-lactams, fluoroquinolones, and aminoglycosides, with few remaining susceptible to ceftazidime–avibactam or colistin. Four were pan-resistant. All exhibited antimicrobial resistance index scores ≥0.60, signifying extensive multidrug resistance. Notably, resistance rates to aztreonam and tobramycin exceeded those reported in a Saudi Arabian ICU (30.6–65.2%), highlighting regional disparities in resistance burden. 28
The observed MDR phenotype of our CRE isolates is well explained by the molecular findings. The blaNDM and blaOXA-48 genes were predominant and coexisted in 70% of isolates, reflecting the spread of high-risk plasmids and successful clonal lineages. 29 Such co-carriage broadens resistance spectra, enhances bacterial fitness, and accelerates dissemination in health care settings. 30 Understanding the circulating carbapenemase types is therefore crucial for guiding antimicrobial stewardship. Concurrent carriage of blaCTX-M and blaSHV extended-spectrum β-lactamases further compounds the resistance burden by compromising all β-lactam options. In Tunisia, ceftazidime–avibactam, the only available β-lactam/β-lactamase inhibitor combination, lacks activity against metallo-β-lactamase (MBL)-producing strains. Given the predominance of MBL-producing CRE, this significantly limits empirical therapeutic options.6,31 In our study, correlation analyses revealed strong genetic associations between carbapenemase and ESBL genes, as well as between aminoglycoside and quinolone resistance determinants such as qnrB, aac(6′)-Ib, and rmtF. These patterns are consistent with plasmid colocalization or coselection under antibiotic pressure, reflecting ICU-driven selective pressures and interspecies gene exchange. 27 However, in the absence of whole-genome sequencing or multilocus sequence typing (MLST), conclusions regarding transmission dynamics and plasmid architecture remain speculative.
In Tunisia, colistin resistance in clinical K. pneumoniae isolates has mainly been attributed to chromosomal mutations particularly mgrB inactivation rather than plasmid-mediated mechanisms. 31 Notably, the first Tunisian mcr-1-positive CRKP clinical isolate was identified at our institution in 2024, 32 signaling emerging plasmid-mediated colistin resistance. Given the high cost and limited availability of newer agents (e.g., aztreonam–avibactam, meropenem–vaborbactam), colistin remains a cornerstone for CRE management underscoring the urgency of molecular surveillance to preserve its efficacy.
Empirical therapy in our ICU relied predominantly on colistin- and tigecycline-based regimens, aligned with local resistance epidemiology. 29 However, clinical efficacy was limited partly due to early mortality preceding susceptibility-guided de-escalation. The near-absence of newer β-lactam/β-lactamase inhibitor and aztreonam use reflects both access barriers and the absence of standardized protocols, emphasizing the need for antimicrobial access and evidence-based stewardship in resource-limited settings. 33 In our study, mortality reached 82.4%. The reported mortality corresponds to all-cause ICU mortality and cannot be directly attributed solely to CRE infection. Delayed appropriate therapy, severe comorbidities, and antimicrobial scarcity further contributed to this high fatality rate. 34 In fact, only 34% of countries globally and fewer than 25% in the WHO African Region, including Tunisia had fully implemented national infection prevention and control (IPC) programs in 2021–2022. 35 This systemic deficiency likely fuels uncontrolled CRE transmission and delays in effective infection control, contributing directly to the alarmingly high mortality observed in our study. In the absence of robust IPC infrastructure, even targeted empirical regimens fail to offset the consequences of late appropriate therapy, severe illness, and therapeutic scarcity highlighting IPC as a non-negotiable prerequisite for improving CRE outcomes in resource-constrained ICUs.
This study highlights the need for an integrated and multidisciplinary approach to managing CRE infections in the ICU. Standardizing phenotypic methods for carbapenemase class identification represents a practical strategy to guide therapy and reinforce infection control. Given the predominance of Class B carbapenemases (blaNDM) empirical regimens should prioritize cefiderocol or the ceftazidime–avibactam and aztreonam-based combinations when available. 36 Effective prevention relies on strict hand hygiene, systematic disinfection, patient isolation, and active surveillance of CRE colonization. Continuous microbiological monitoring is essential to follow local resistance trends and adjust empirical treatment accordingly. 37
Close collaboration between clinicians, microbiologists, and hospital pharmacists is fundamental for optimal patient management—ensuring rapid identification of resistance mechanisms, appropriate antimicrobial selection, and rational antibiotic use. Finally, an integrated information system should enable real-time communication of microbiological results, resistance alerts, and antibiotic consumption data, thereby strengthening coordinated responses and limiting CRE dissemination. 38 Implementing comprehensive infection control measures, including active surveillance and screening of high-risk individuals, to effectively identify and manage carriers of CRE can prevent transmission and outbreaks.
Conclusions
These findings emphasize the urgent need to strengthen infection prevention and control measures through active surveillance, strict contact precautions, and environmental decontamination. Routine phenotypic screening for carbapenemase types is essential to guide appropriate therapy. Improved access to novel agents, such as ceftazidime–avibactam and aztreonam, is critical. Future research should incorporate whole-genome sequencing to elucidate transmission dynamics and extend to multicenter studies for broader epidemiological insight.
Authors’ Contributions
Conceptualization: M.E., I.S.; Methodology: M.E., I.S.; Formal analysis: M.E., I.S., O.B.; Investigation: M.E., I.S.; Data curation: M.E., I.S.; Writing—original draft: M.E.; Writing—review and editing: M.E., I.S., N.B.-F.; Supervision: M.E., S.C., I.S.
Footnotes
Acknowledgments
The authors gratefully acknowledge the contribution of the microbiology laboratory and ICU staff for their assistance in sample collection and clinical data acquisition.
Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
The authors declare that no funding was received for this study.