
Abstract
The Patient Driven Payment Model (PDPM), a major reform in the way Medicare reimburses for skilled nursing facility (SNF) care, went into effect in October 2019, prioritizing intensity of nursing care provided over volume of therapy. The purpose of this study was to understand how the PDPM shaped SNF admissions and care delivery, using SNF administrator perspectives. Findings from this qualitative thematic analysis suggest that the PDPM created incentives for SNFs to prioritize more clinically complex patients over patients requiring less complex rehabilitation, improved care coordination between hospitals and SNFs, as well as within the SNF interdisciplinary care team, and emphasized the patient documentation review required for reimbursement. Findings suggest that these changes contributed to SNF care teams better understanding patients’ care needs. When considering how best to balance efficiency and quality in patient care delivery, it is important to understand the nuanced changes the PDPM has on SNF operations.
Introduction
On October 1, 2019, the Patient Driven Payment Model (PDPM) went into effect, significantly altering how the Centers for Medicare and Medicaid Services (CMS) reimburses skilled nursing facilities (SNFs) for post-acute care (CMS, 2024b; Federal Register, 2018). Under the previous payment model, Resource Utilization Groups (RUGS), reimbursement to SNFs was based primarily on the volume of therapy provided (Bowblis & Brunt, 2014; CMS, 2019a; Rahman et al., 2022). CMS created the PDPM to prioritize the care delivered for patients’ clinical needs over therapy alone (Brady & McKittrick, 2021). Under the PDPM, SNFs were incentivized to admit patients with higher clinical and ancillary care needs to maximize reimbursement (Makam & Grabowski, 2021). In both the RUGS and the PDPM, patient documentation is required to complete Minimum Data Set (MDS) patient assessments for reimbursement. The PDPM reduced the frequency of MDS assessments from five to two required assessments while requiring more clinical details than the RUGS model (CMS, 2019b). This paper focuses on how the PDPM has re-shaped SNF admissions strategies and processes related to the delivery of patient care.
Quantitative evidence has shown that after the implementation of the PDPM, patients admitted to SNFs had, on average, slightly higher prevalence of certain chronic conditions, including diabetes, heart failure, stroke, dementia, and chronic obstructive pulmonary disorder; as reimbursement for more complex conditions such as these increased under the PDPM (Rahman et al., 2022). Research is limited, however, as to whether these differences reflect a change in the types of patients that SNFs were prioritizing for admissions. One study reported that SNF time and resources went toward training staff on proper documentation required for MDS assessments and preparing to appropriately maximizing reimbursements under the reform (Liu et al., 2024). Another study found reductions in the delivery of therapy (McGarry et al., 2021; Prusynski et al., 2021), but research examining the broader care delivery spectrum is sparse. In this paper, we share what we heard through semi-structured, in-depth interviews with SNF administrators across the Unites States on how the PDPM re-shaped decision-making around admissions, including whether or not certain patients were now prioritized due to their clinical complexity, and patient care delivery, including documentation of patient care and care team coordination.
To organize our results, we applied Donabedian’s structure, process, and outcome framework for assessing the quality of medical care (Donabedian, 1966). In Donabedian’s framework, the “structure” of health care delivery is the setting where health care occurs and includes the administrative systems that provide care delivery, such as the fiscal organization of the SNF, available medical equipment, and clinical staff qualifications. “Process” represents the actual delivery of care and includes the documentation of, and the coordination of patient care, among other factors. “Outcomes” represent the effects on the patient stemming from the structures and processes in place.
Methods
Study Design
This research is part of a larger mixed-methods project that studied the implementation of the PDPM and how COVID-19 shaped care processes in SNFs. SNF administrators participated in semi-structured interviews that were repeated four times, each 3 months apart between July 2020 and December 2021, with administrators from 40 SNFs around the United States. Other papers on varying themes stemming from the qualitative arm of the project and methodological descriptions have previously been published (Gadbois et al., 2023; Liu et al., 2024; Meehan et al., 2023). This study was not considered human subjects’ research by the Institutional Review Board at Brown University.
SNF Selection and Administrator Recruitment
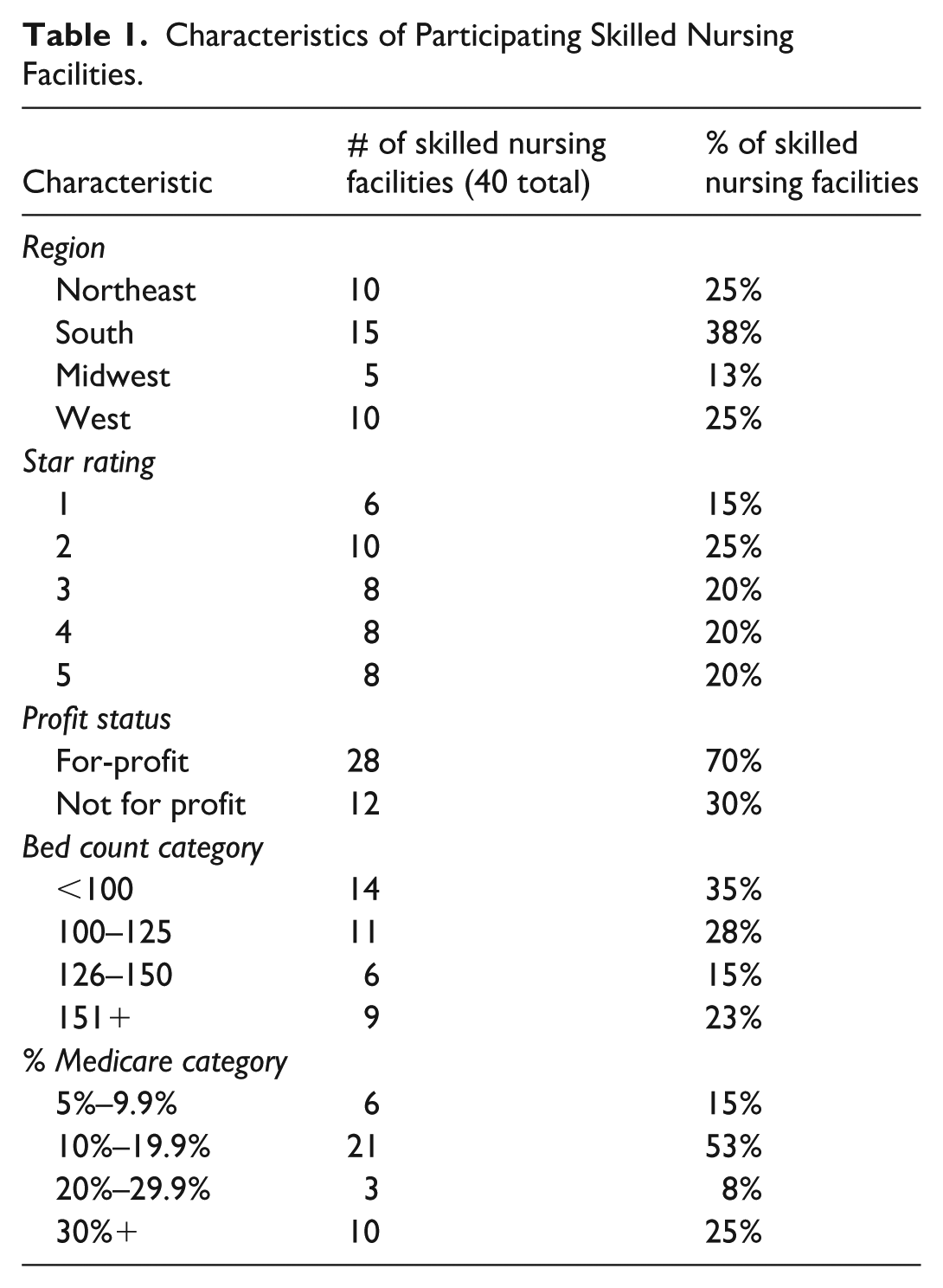
We used purposive sampling of SNFs to ensure a variety of experiences. SNFs selected for outreach varied in (a) location in one of eight health care markets in the United States that differed in terms of SNF utilization and geographic region, (b) bed count, (c) percentage of patients whose primary insurance was Medicare, (d) ownership type, and (e) CMS’s Five Star Quality Rating. Facility characteristics were ascertained from the Certification and Survey Provider Enhanced Reporting (CASPER) system using data from 2018 and publicly reported data from CMS (CMS, 2024a). SNFs with fewer than 5% of patients paid through Medicare or with fewer than 50 beds were excluded as those SNF administrators may not have sufficient knowledge or experience of the PDPM (since the PDPM is part of Medicare Part A). SNF administrators were recruited for interviews through email and phone calls.
Interview Protocol and Design
Qualitative research team members conducted interviews in teams of two via phone or Zoom, according to participant preference. Interviews averaged about an hour in length. The second interview was scheduled at the conclusion of the first, and so on until the fourth and final interview was completed. Participants received gift cards after each interview. The semi-structured interview guide was piloted and refined, and among other topics, it included similar base questions across interviews such as: “Thinking about specific changes due to the PDPM, how do you think it has impacted your staff work patterns? Patient care? Admissions?” The second and third interviews modified these questions by adding the prompt “In the three months since we spoke last . . .” and specific follow-up questions from the previous interview.
During the third interview, a report highlighting preliminary findings and emerging themes from interviews was shared and discussed, and feedback from participants was obtained. The final interview guide included prompts designed to be more reflective of the entire study period. Interviews 2 through 4 also included individualized questions based on prior responses. For example, “The last time we talked, you said that due to the PDPM, you were seeing more clinically complex patients. What does this look like at your facility?” See Online Supplemental Appendix 1 for the first and last interview guides with interview questions of focus within this paper. Interviews were given study IDs in the format SXNX where S = the health care market and N = the facility where an administrator was interviewed. All interviews were audio-recorded with verbal consent from the participant, transcribed, and imported into NVivo for data management.
Qualitative Analysis
An initial round of analysis of the interview transcripts was completed using a modified grounded theory approach (Alnsour, 2022). The modified grounded theory phase of analysis began by developing an initial codebook based on the interview guide. The team met weekly throughout the analysis to iteratively refine the codebook, reconcile coding differences after independently coding the transcripts, and discuss emerging themes. Forty-six codes and their associated coding reports (all excerpts assigned to the same code) resulted from this phase. An audit trail was maintained throughout this process, which tracked team decisions, changes to code definitions, and questions and comments.
Using coding reports generated from the first phase pertaining to admission and patient care delivery, a secondary thematic analysis was conducted to better understand participants’ experiences about the PDPM in SNFs (Braun & Clarke, 2006; Strauss et al., 1994); the results of the secondary analysis are presented in this paper. Five coding reports were selected for the thematic analysis: “PDPM-admissions,” “PDPM-coding,” “PDPM-delivery of care,” “reimbursement,” and “strategic planning.” Quotes with COVID-19-related content were excluded from the thematic analysis. New codes were inductively developed and applied during thematic analysis. For example, the “PDPM-admissions” coding report (which resulted from the initial round of analysis) was further analyzed, and codes more specific to SNF admissions strategies and patient care delivery processes were applied, such as “strategy” and “documentation.” Specific themes were then iteratively identified and discussed with the research team. Post hoc, Donabedian’s structure, process, outcome model was used as a framework to organize the identified themes. For this study’s analysis, “structure” was defined as encompassing the PDPM payment reforms and how SNF administrators evaluated their clinical capabilities, like medical equipment and training of their staff for the PDPM. The “process” was that how care was delivered included care coordination and communication and patient documentation review. The “outcomes” for this study were defined by the effects on patient care and overall wellbeing, as described by participants.
Results
Results include data from 156 interviews with administrators from 40 SNFs varying in percentage of residents, with Medicare as their primary insurance, geographic location, ownership type, CMS 5-star quality rating, and bed count. Table 1 summarizes the characteristics of participating SNFs. During thematic analysis, three general themes were generated, organized by Donabedian’s structure, process, outcome model—(a) structure: in a large shift, the PDPM reimbursement structure prioritized patient clinical characteristics rather than therapy minutes; (b) process: care coordination and communication processes between SNFs and hospitals, as well as among the interdisciplinary SNF team changed to focus on patient documentation review; (c) outcomes: SNF care teams were reported to have a better understanding of patients’ individualized care goals and needs. These concepts are examined in greater detail below.
Characteristics of Participating Skilled Nursing Facilities.
Theme 1: Structure – the PDPM Reimbursement Structure Prioritized Patient Clinical Characteristics Rather Than Therapy Minutes
Many SNF administrators reported perceived changes to reimbursement based on individual patient characteristics, rather than therapy volume. Administrators of some SNFs described strategizing how to admit patients with greater clinical complexity, such as those requiring more wound care, than they previously would have under the prior payment model. For example, some SNF administrators described enhancing their facility’s ability to provide more clinically complex care by adding clinical services such as respiratory therapists or other specialists. As one administrator noted: We have to make sure that our staff is prepared and ready to accept these new challenges that we have, whether it’s new equipment, if it’s a new device that maybe they’re not familiar with. And, to give them the assurance that they’re going to be able, or make them comfortable taking care of this new thing. Just to make sure they have that comfort level to be able to make them successful in taking care of a new device or a new modality maybe they haven’t been taking care of before. S3N3 _January 2021
Perceived changes in patient composition varied; some administrators reported that their existing structures positioned them well for the PDPM because they “take pretty complex patients as it is” (S4N4_April 2021). Other administrators reported that they did not make changes to admit more clinically complex patients as their SNF operations were geared toward accepting patients with less clinical complexity. For example, one administrator described that their referral population was patients largely in need of post-elective surgery rehabilitation: We attract a unique population [of] people. They come in, they pre-book when they’re doing elective surgeries to come in and do their rehab here. So, could we look to focus on trying to get higher acuity folks? That would have to be a balance because obviously we wouldn’t want to kind of cut off that flow that we already have. S1N2_February 2021
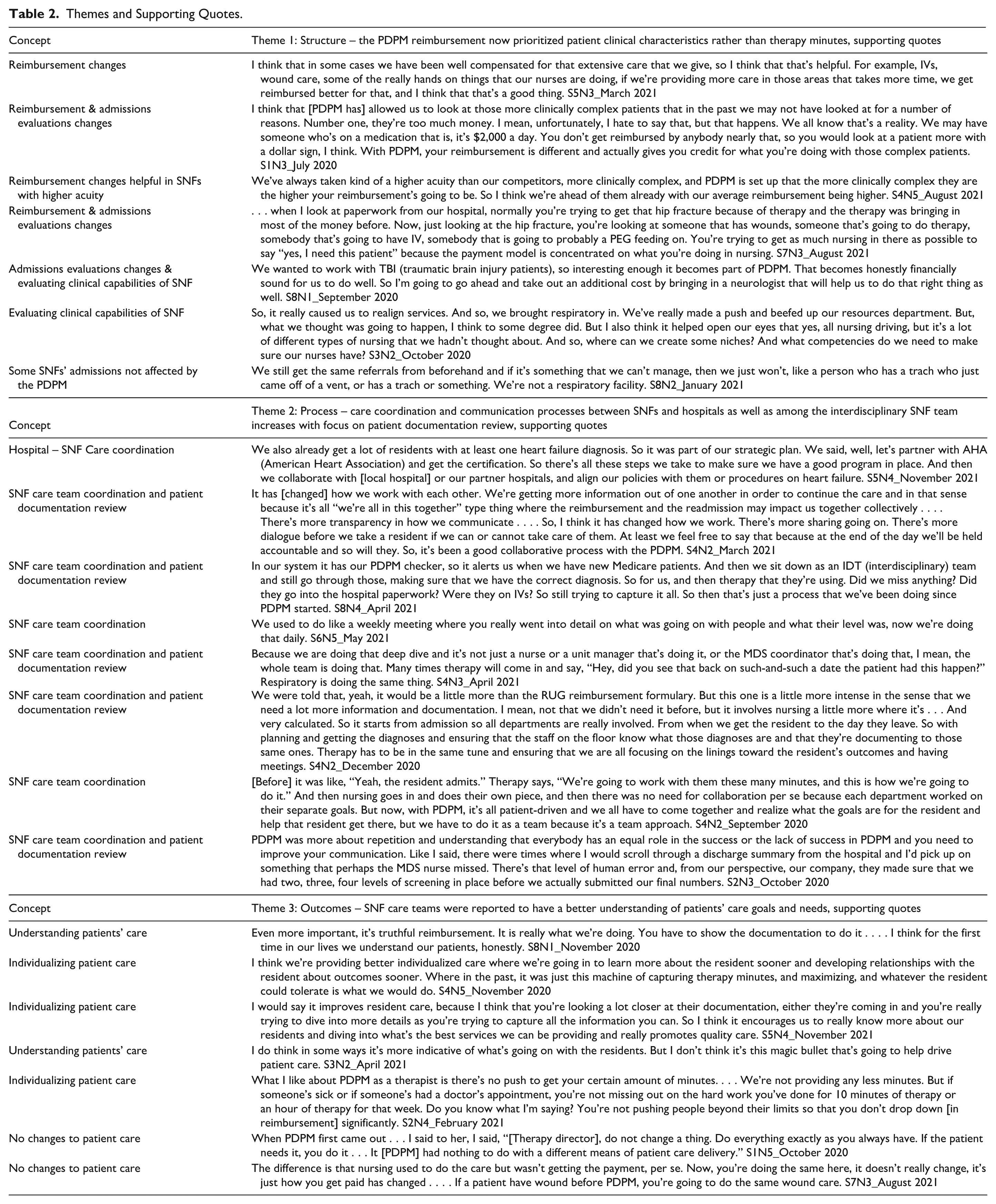
See Table 2 for additional supporting quotes.
Themes and Supporting Quotes.
Theme 2: Process – Care Coordination and Communication Processes Between SNFs and Hospitals as well as Among the Interdisciplinary SNF Team Increase With Focus on Patient Documentation Review
Administrators reported changes related to care coordination and patient documentation review to ensure proper reimbursement under the PDPM structure. Administrators reported improved coordination between SNFs and hospitals, including how hospitals provided more detailed patient information during the admissions process to guide SNF staff in admissions’ planning. Participants described communicating with hospital discharge planners to identify patients historically difficult to place in an SNF, such as patients requiring specialized cardiac care who would be reimbursed more with the PDPM. One administrator discussed enhanced collaboration with hospitals: It has [changed] how we work with each other. We’re getting more information out of one another in order to continue the care and in that sense because it’s all “we’re all in this together” type thing where the reimbursement and the readmission may impact us together collectively. S4N2_March 2021
Administrators also reported that while fewer MDS assessments are required under the PDPM, the patient documentation required to complete MDS assessments was more complex; staff now took more time to review patient medical records, extract key clinical data, and ensure patient documentation was accurate to avoid “missing opportunities” (S2N4_August 2021). The increased focus on patient documentation, including a more detailed review process during admissions, led to frequent staff meetings to discuss patients and ensure coding and documentation were “capturing everything” (S6N5_May 2021) to maximize the PDPM reimbursements. Several described how patient care team members, such as therapists, nurses, and dieticians, coordinated around patient documentation and care more frequently and in greater detail than before. One SNF administrator described: Now you need to capture more things. So, for example, before the dietitian wouldn’t come to a utilization review meeting, but now they do come because you can capture if someone was on IV fluids in the hospital. Or if they’re on a downgraded diet, or dysplasia or had a barium swallow, you can capture that. So every discipline has homework to do, so to speak. So it just helps making sure we’re capturing everything we can. S2N2_January 2021
See Table 2 for additional supporting quotes.
Theme 3: Outcomes – SNF Care Teams Reported Having a Better Understanding of Patients’ Care Goals and Needs
Many administrators told us that SNF staff’s understanding of nuances in patient health and care needs was enhanced as the overall patient documentation review process became more in-depth. For example, one administrator described having members of the care team review documentation at different times of day and notice different care needs as a result: And you may see [a patient] first thing in the morning when they’re at their prime, but as the day goes on and they wane, yes, documentation is going to be different. And nursing is documenting what nursing is seeing. Why don’t you hang out till 4:30 or 5:00 or 6:00 and do therapy with them then? We’re not lying. They may be more independent first thing in the morning, but as the day goes on and they’re tired out, they need more extensive assistance. S1N4_April 2021
Administrators reported that the PDPM reimbursement changes allowed for more flexibility in the timing of therapy, thereby allowing time to prioritize other clinical needs of the patient. The enhanced priority of clinical needs allowed a stated focus “on the overall wellbeing of the patient” (S6N2_September 2020). Other administrators said there were no changes in the delivery of either nursing care or therapy from the PDPM. As one administrator said: “PDPM is mostly a different payment model. It really has nothing to do with the care” (S7N3_August 2021).
See Table 2 for additional supporting quotes.
Discussion
We organized findings from this study using Donabedian’s structure, process, and outcome framework to better illustrate how the PDPM reimbursement structure incentivized SNF administrators to reevaluate admissions criteria and the structure of clinical care delivery within their SNFs, particularly regarding how to provide care for patients with higher clinical complexity. To be reimbursed accurately under the PDPM, administrators described changing workflow processes to facilitate more attention to patient documentation. Many administrators described how through increased attention to patient documentation review, the patient care team ultimately better understood their patients’ care goals and needs more thoroughly. It is important to note that other administrators conveyed that despite the new reimbursement structure, they did not perceive related changes to admissions strategies and patient care delivery.
As the types of patients that an SNF admits generally impacts reimbursement rates, strategizing payer patient mix may be an important consideration for the financial wellbeing of an SNF. Maximizing reimbursements may be particularly important, considering how COVID-19 negatively impacted both occupancy rates and financial performance of SNFs (Orewa, Weech-Maldonado, Davlyatov, et al., 2024; Orewa, Weech-Maldonado, Lord, et al., 2024). Many administrators interviewed for this study reported prioritizing patients with higher clinical complexity, a population historically considered less desirable not prioritized by SNFs (Shield et al., 2019), to maximize the PDPM reimbursement. Other administrators at some SNFs reported that the PDPM did not lead to adjusting their referrals or clinical capabilities, often because these SNFs either already admitted high levels of complex patients or that their patient referrals were mostly lower acuity. Some research suggests that patients with less clinical complexity, such as those needing rehabilitation from elective surgeries, are also increasingly receiving home health services instead (Werner & Bressman, 2021).
Our results also indicate the patient information obtained by SNFs from hospitals became more comprehensive although the PDPM final rule states that hospital documentation provided to SNFs “should be sufficient for addressing the payment requirements under PDPM” (Federal Register, 2019). Regardless, administrators described “more transparency” and “more dialogue” (S4N2_March 2021) with hospitals in collecting documentation required for the PDPM and more accurate clinical data upon admission. Improved hospital–SNF care coordination processes as described may be an unintended, positive change of the PDPM. This analysis also highlights how the changing documentation workflow required more coordination among members of the care team at many SNFs, which also may be an unintended change to processes under the PDPM. Nursing home leaders may want to consider how to structure their staffing to encourage interdisciplinary coordination when determining how to best complete patient documentation.
According to administrators, the PDPM, although “not a magic bullet” (S3N2_April 2021), made progress toward prioritizing the individualized clinical and ancillary needs of patients. With therapy minutes no longer being the driver for reimbursement under the PDPM, administrators reported not worrying about losing reimbursement if a patient missed scheduled therapy due to feeling sick or having a conflicting care appointment. This could help explain some of the decrease in therapy service use since the implementation of the PDPM as reported in one study of Medicare post-acute patients (Rahman et al., 2022). In addition, the greater attention to detail given to the patient documentation review process led administrators to perceive the care team as more knowledgeable about their patients’ care needs and goals. Future research could help clarify the impacts of the PDPM on other quality-of-care measures for patients with differing acuity levels, such as functionality and mobility, and hospitalizations.
Limitations
While purposive sampling was used to capture for varied experiences with the PDPM, this approach excluded some facilities, like those not in our chosen markets. Therefore, our findings may not be transferable across all SNFs in the United States. In addition, the administrators that did not take part in our study may have had a lack of capacity or other unknowable factors, possibly leading to different experiences with the PDPM. In addition, because we interviewed only SNF administrators, perspectives from others responsible for implementing the PDPM, such as nurses and therapists, would be valuable in assessing its implementation. Finally, the PDPM was first implemented in October 2019, a few months before COVID-19 began affecting the United States. The information we obtained about the impact of COVID-19 on the early implementation of the PDPM was reported previously (Meehan et al., 2024). While we made efforts to exclude excerpts pertaining to how COVID-19 specifically framed admission and reimbursement decisions, it is difficult to delineate how PDPM shaped reimbursement separate from COVID since they occurred in parallel.
The implementation of the PDPM also coincided with rising patient acuity levels at SNFs (Fashaw et al., 2020), likely due to various factors, including the availability of assisted living and home health services. While the PDPM was intended to be budget neutral, CMS found that initial implementation led to unintended increases in payment, prompting payment reductions of about 2.3% in 2023 and 2024 (CMS, 2023). As CMS considers additional changes to the PDPM, our qualitative inquiry allows a more fully rounded assessment of difficult-to-quantify policy impacts. These results illustrate that the PDPM made it more financially feasible for administrators of certain SNFs, although not all, to strategize how to provide care for patients with higher levels of clinical complexity. These shifts in admissions strategies have implications for how researchers, SNFs, and hospitals should examine how to care for patients with fewer nursing needs, such as those undergoing post-elective surgery. SNF administrators and corporate leadership should consider how best to align staffing and patient documentation processes to support patients with greater clinical complexity. Given the evidence that links care team collaboration and patient outcomes (Matthys et al., 2017), our results showing the focus on patient documentation review processes are promising that the PDPM supports a more patient-centered approach to the delivery of care.
Supplemental Material
sj-docx-1-mcr-10.1177_10775587261453971 – Supplemental material for How the Patient Driven Payment Model Shifted Admissions Strategies and Understanding of Care Needs According to Skilled Nursing Facility Administrators
Supplemental material, sj-docx-1-mcr-10.1177_10775587261453971 for How the Patient Driven Payment Model Shifted Admissions Strategies and Understanding of Care Needs According to Skilled Nursing Facility Administrators by Amy E. Meehan, Joan F. Brazier, Elizabeth White, Courtney Hawes, Brian E. McGarry, Jacy Weems, Fangli Geng, David C. Grabowski, Momotazur Rahman, Renee R. Shield and Emily A. Gadbois in Medical Care Research and Review
Footnotes
Acknowledgements
We thank Zhanqin Liu, MPH, and Christopher Santostefano, MPH, RN for their contributions to this paper.
Ethical Considerations
This study was reviewed by the Institutional Review Board at Brown University and determined not to be a human subjects’ research.
Consent to Participation
Participant consent to participate was obtained verbally at the beginning of each interview.
Consent for Publication
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Warren Alpert Foundation. The funder did not play a role in the design, methods, subject recruitment, data collection, analysis, or preparation of the article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: David Grabowski reports receiving fees unrelated to this work from the Analysis Group, EntityRisk, GRAIL, and the University of Southern California. None of the other co-authors report any potential conflicts of interest.
Data Availability Statement
Interview guides, audit trails, and coding schemes are available to share. Since the verbal consent from participants detailed sharing data in aggregate only, coding reports/transcripts are not available to share.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.