
Abstract
Youth involved in the juvenile justice system are at high risk for mental health problems, particularly depression. Furthermore, these youth often present with a history of childhood maltreatment. Despite research consistently demonstrating a link between childhood maltreatment and depression, our understanding of intervening factors of this relationship remains limited. This study examined impulsivity, hopelessness, and substance use as potential explanatory variables in the relationship between cumulative childhood maltreatment and depression severity among 110 incarcerated youth. The data were analyzed using path analysis. As hypothesized, cumulative maltreatment maintained a strong direct relation with depression severity in the context of the additional variables in the final model. Cumulative maltreatment also had an indirect relation with depression severity through both impulsivity and hopelessness. Contrary to expectation, substance use was not an explanatory variable in the model. These findings suggest that impulsivity and hopelessness might be important factors to consider in future studies on the relation between childhood maltreatment and depression symptoms among incarcerated youth.
Youth involved in the juvenile justice system represent one of the largest concentrations of adolescents presenting with depression (Colins, Vermeiren, Schuyten, & Broekaert, 2009; Teplin, Abram, McClelland, Dulcan, & Mericle, 2002). Research suggests that 47% of incarcerated youth have moderate or severe depression (Domalanta, Risser, Roberts, & Risser, 2003), with as many as 13% of incarcerated youth meeting criteria for major depressive disorder (Teplin et al., 2002), compared to 5% of youth in the general population (Shaffer et al., 1996). Depression and depressive symptoms in adolescence can result in significant impairment in school performance and social functioning, compromising an individual’s overall health and well-being and putting a young person at heightened risk for suicide (Coyle et al., 2003; Hauenstein, 2003; Spirito & Esposito-Smythers, 2006). Furthermore, depression symptoms are among the most consistent and strongest predictors of youth violence, alongside delinquent peer associations and antisocial personality traits (Ferguson, San Miguel, & Hartley, 2009). As a result, it is imperative that potential explanatory variables for adolescent depression are identified to prevent or address negative psychological outcomes. The investigation of the potential causes of depression among juvenile offenders remains a particularly understudied area.
Although the etiology of depression in young people is multifaceted (Tao, Moore, Mayes, & Emslie, 2007), childhood maltreatment has been consistently identified as an important risk factor (Brown, Cohen, Johnson, & Smailes, 1999; Harkness, Bruce, & Lumley, 2006). Theorists have long held that depression severity in adolescence and adulthood is precipitated by childhood maltreatment (e.g., Bowlby, 1980). Moreover, research suggests cumulative maltreatment may lead to more detrimental mental health functioning than exposure to only one subtype of childhood maltreatment. For instance, the number of maltreatment subtypes experienced in childhood has been associated with poorer mental health outcomes, including increased depression severity, among both men and women (Edwards, Holden, Felitti, & Anda, 2003; Salazar, Keller, & Courtney, 2011).
With respect to the youth involved in the juvenile justice system and childhood maltreatment, incarcerated youth are more likely to report childhood maltreatment histories than nonincarcerated youth (Stevenson, 2009). Childhood maltreatment is, in fact, widely recognized as a risk factor for involvement in criminal activity, whereby a history of abuse or neglect in childhood has been reported to increase the likelihood of antisocial and delinquent behavior (Malinosky-Rummell & Hansen, 1993; Verrecchia, Fetzer, Lemmon, & Austin, 2010). Without intervention, these maltreated youth are more likely to commit a violent offense (Widom, 1992), have an earlier onset for the initiation of delinquent behaviors (Rivera & Widom, 1990), and are at a higher risk for criminal recidivism and for involvement in the adult criminal justice system (Visher, Lattimore, & Linster, 1991). Furthermore, this effect is cumulative; youth are at increased risk for delinquency when multiple forms of maltreatment are experienced (Ford, Elhai, Connor, & Frueh, 2010), and those who are repeatedly maltreated for an extended period of time are more likely to re-offend (Chang, Chen, & Brownson, 2003).
Adolescent offenders who have experienced childhood maltreatment report a higher prevalence of depression and severity of depression symptoms compared to nonmaltreated youth (Bender, 2010). However, relatively few studies have examined the effects of cumulative childhood maltreatment on depression severity and other indicators of mental health functioning. Multiple factors might explain the relation between childhood maltreatment and depression. Here we focus on the role of three such dynamic factors that may offer insight into future research informing the development of more targeted intervention and prevention strategies.
Hopelessness, Impulsivity, and Substance Use as Potential Intervening Factors in the Relation Between Childhood Maltreatment and Depression
Hopelessness
Numerous theories have posited a relationship between depression and persistent negative expectancies and cognitions. According to Beck's cognitive theory of depression (1987), dysfunctional negative cognitions are the primary antecedents of depression symptoms. This theory has stimulated considerable interest and numerous studies have generated support for a relationship between hopelessness, as a negative cognition, and depression severity (e.g., Alloy & Abramson, 1999).
Beck's theory further postulates that negative events in the formative years can contribute to the development of persistent and maladaptive negative cognitions later on. Nonetheless, few empirical investigations have examined childhood maltreatment history as a potential precursor to hopelessness. Rose and Abramson (1992) hypothesized that individuals who infer negative self-characteristics and stable global causes from negative life events are vulnerable to the development of hopelessness and subsequent depression. In the case of childhood maltreatment, it is suggested that the child attempts to understand why the event occurred in order to avoid its recurrence. These inferences are initially hopeful and attributed to unstable and specific characteristics. However, with chronic maltreatment these inferences are continuously disconfirmed and eventually the child begins to make hopeless attributions that can generalize to other negative events (e.g., Gibb, Alloy, Abramson, & Marx, 2003). As such, negative cognitive styles, including hopelessness, could be expected to influence the relationship between childhood maltreatment and depression severity (DuRant, Getts, Cadenhead, Emans, & Woods, 1995).
Impulsivity
Early experiences of maltreatment might constitute an environmental risk factor for the development of impulsivity, which might, in turn, increase depression severity. Impulsivity has been described as a consequence of traumatic events, such as childhood maltreatment, by undermining the individual's capacity to inhibit behavior and modulate emotions (Braquehais, Oquendo, Baca-García, & Sher, 2010). Relatedly, the appraisal theory of emotional states posits that sadness arises when our potential for coping with a negative event is compromised (Scherer, 2001). Therefore, compared to their nonimpulsive counterparts, impulsive adolescents may have increased depression severity because they are more likely to employ inappropriate strategies for coping with childhood maltreatment (e.g., d'Acremont & Van der Linden, 2007).
This proposition is further supported by neurobiological evidence regarding alterations in brain development associated with childhood maltreatment (Gerra et al., 2007; Lovallo, 1997). One neurochemical mechanism for this association may relate to serotonergic function. That is, chronic or persistent maltreatment can lead to lower levels of central serotonin. Moreover, low serotonin function has been associated with impulsive behaviors. Reduced availability of serotonin leads to decreased ability of the central nervous system to dampen emotional responses to stressors (Braquehais et al., 2010). This offers one potential neurochemical explanation for the association between impulsivity and depression severity (e.g., Gerra et al., 2007). While these interrelations deserve further investigation, on the whole, research suggests that impulsivity precedes depression (d'Acremont & Van der Linden, 2007).
Substance use
The association between substance use and depression is well established, with many studies reporting greater depression severity in drug users than nondrug users (e.g., Sumnall & Cole, 2005). Several studies also have reported substance use to be a strong predictor of depression (e.g., Davidson, 1995; Swanson, Linskey, Quinero-Salinas, Pumariega, & Holzer, 1992). With respect to traumatic experiences, research has suggested that childhood maltreatment increases the risk for substance use disorders and misuse among adolescents (Gerra et al., 2007). The positive association between childhood maltreatment and substance use has been recorded across diverse samples, including incarcerated adolescents (Hawke, Jainchill, & DeLeon, 2000).
In light of the above mentioned relationships, it is possible that impulsivity and hopelessness, arising from childhood maltreatment, predicts substance use, which, in turn, could explain depression severity. In support of this contention, impulsivity has been found to be a vulnerability factor for both the acquisition and escalation of substance use disorders (Perry & Carroll, 2008; Wills & Stoolmiller, 2002) and hopelessness has been identified as an important determinant of substance use behaviors (Bolland, 2003).
The Present Study
It is widely held that childhood maltreatment is a precipitating factor for depression. However, the potential intervening factors between these variables are not well understood, particularly among incarcerated adolescents. Given their high rate of depression, understanding the possible intervening factors between maltreatment and depression among incarcerated youth may reveal critical areas to target for intervention. Thus, empirical research focusing on the dynamic factors of hopelessness, impulsivity, and drug use is an important area for investigation. The present study tested a theoretical model of the relationship between childhood maltreatment and depression severity by examining hopelessness, impulsivity, and substance use as potential explanatory factors in a sample of incarcerated juvenile offenders. Moreover, we also examined the potential intervening role of substance use in the relations between both hopelessness and impulsivity with depression. Based on the existing literature, it was hypothesized that higher levels of cumulative maltreatment would be related to higher depression severity. This relation was expected to be partially explained by impulsivity, hopelessness, and substance use such that higher levels of these intervening factors would account for some of the variance explained by cumulative maltreatment. Furthermore, it was expected that the relations between impulsivity and hopelessness on depression severity would be partially explained by substance use, whereby higher levels of substance use would account for some of the variance explained by impulsivity and hopelessness.
Method
The original study sample comprised 116 juvenile offenders (70 males and 46 females) recruited from one secure-custody and five open-custody facilities in Ontario. Data collection took place between July 2009 and August 2010. Eligibility criteria were (a) being between the ages of 12 to 24 years; (b) fluent in English; and (c) in custody at a youth justice facility under the supervision of the Ministry of Children and Youth Services (MCYS) at the time of the interview. Due to incomplete data from six youth across the measures, all analyses for this study examined a sample of N = 110 (n = 67 males and n = 43 females).
The average age of participants at the time of the interview was 16.78 years (standard deviation [SD] = 1.07) and 91.8% of participants were between the ages of 16 and 19 years. Males were on average 17.10 years of age (SD = 1.08) and females were on average 16.28 years of age (SD = 0.85). Table 1 shows the demographic and offense characteristics for the sample. Descriptive information on sample characteristics and path variables for females alone, males alone, and the entire sample are provided to give further information about sample sex differences. Although not a focus of the current study, these sex-specific details are included to inform future larger scale studies in this area, particularly given the inconsistent findings regarding sex differences with respect to the relation between maltreatment and depression severity (e.g., Arata, Langhinrichsen-Rohling, Bowers, & O'Brien, 2007; Powers, Ressler, & Bradley, 2009). Eighty-nine youth (80.9%) had completed at least 1 year of high school. The sample was diverse in terms of their ethnicity and sexual orientation. With respect to offense characteristics, violent offenses were most often reported as precipitating incarceration and half the sample reported a previous period of incarceration. The majority of the youth (60.0%) was sentenced to serve time at the facility for their most recent offense and the remainder was in custody while awaiting sentencing (i.e., in detention). Although recruitment was based on self-initiated interest in participating, and therefore not necessarily representative of the entire population of youth within the facilities, offense characteristics appear comparable to the entire population of Canadian incarcerated youths. For instance, violent offenses accounted for the largest proportion of incarcerations (Calverley, Cotter, & Halla, 2010).
Demographics and Offense Characteristics of the Sample

Note. The variation in sample size in sexual orientation is due to missing data for one male participant. Percentages add up to more than 100% for ethnicity and charges or convictions because some youth identified more than one.
Procedure
A flyer describing the study was posted at each site in a visible area accessible to the youth, directing interested youth to an on-site contact person. This contact person was a unit or facility manager not involved in the provision of clinical services or directly involved in the research. In this regard, a facility manager served as a liaison between the study coordinator and participants in order to minimize the involvement and knowledge of other staff regarding participation, to respect the privacy of youth's identities, and to minimize any perceived pressure to participate.
When youth 16 years of age and older expressed an interest in participating in the study, the on-site contact person contacted the research coordinator to schedule a time to meet the youth. In-person and prior to testing, a formal consent protocol was read to youth by the research coordinator. For youth less than 16 years of age, the on-site contact person obtained consent from a parent, guardian, or the youth's social worker (in the case of the youth being a crown ward) before a meeting was scheduled with the research coordinator to obtain assent from the youth and to complete the measures.
Each interview took approximately 50–60 min and was conducted individually in a quiet room on-site. For the majority of the interviews, the youth completed the questionnaires on their own in the presence of the study coordinator. For 15 youth (13.4%), upon request of the participant, the study coordinator read the questions aloud to the youth. No differences on the variables of interest for this study were found between participants who read the questionnaire and those who had the questionnaires read to them. Youth received $15.00 as reimbursement. Approval for this study was obtained from Ryerson University's ethics board and the (Ontario) Ministry of Community Safety and Correctional Services (MCSCS)/Ministry of Children and Youth Services (MCYS) Youth Justice Research Committee.
Measures
Childhood maltreatment
Childhood maltreatment was measured with the Childhood Trauma Questionnaire–Short Form (CTQ-SF; Bernstein et al., 2003; Bernstein & Fink, 1998). The CTQ-SF is a 28-item self-report retrospective inventory assessing childhood experiences of maltreatment. The central constructs underlying the inventory are emotional neglect and abuse, physical neglect and abuse, and sexual abuse. These subscales each contain 5 items that begin with the stem "When I was growing up," and items are summed to yield a total subscale score, with higher scores indicating greater severity of childhood maltreatment. Respondents rate the frequency of a particular incident on a 5-point Likert-type scale ranging from never true (1) to very often true (5). The CTQ-SF has been well validated with both adolescent and adult populations, and there is good support for the convergent and discriminant validity of the measure (Bernstein et al., 2003; Bernstein & Fink, 1998). Internal consistencies for subscales are good, with Cronbach's αs ranging from .81 to .95 for the abuse and emotional neglect subscales (Bernstein et al., 2003). The physical neglect subscale typically yields the lowest reliability across studies, ranging from .61 to .83 (Bernstein et al., 2003; Burton, 2008).
For the present study, a cumulative childhood maltreatment score was calculated by first dichotomizing each of the five maltreatment subscales, based on the CTQ-SF manual subscale cutoffs indicative of "moderate" to "extreme" childhood maltreatment having occurred or not, then summing the dichotomized variables to create a count score from 0 (experienced no maltreatment) to 5 (experienced each form of maltreatment). A count variable was chosen over running separate models for each type of childhood maltreatment primarily due to high interscale correlations. Cronbach's αs for this study were consistent with prior research (e.g., Bernstein et al., 2003; Burton, 2008): .96 (sexual abuse), .88 (physical abuse), .91 (emotional abuse), .76 (physical neglect), and .90 (emotional neglect).
Hopelessness
Severity of hopelessness was measured with the Beck Hopelessness scale (BHS; Beck, Weissman, Lester, & Trexler, 1974). This self-report measure consists of 20 true–false statements designed to assess the extent of negative and positive expectations about the future. Each statement is scored as a 0 or 1, and a total score is calculated by summing pessimistic responses for each of the items. Higher scores indicating a greater degree of hopelessness during the preceding week, with scores over 8 indicating a moderate to severe level of hopelessnes as defined by the instrument authors. The instrument has high internal reliability and test–retest reliability across diverse populations, including nonclinical and substance abusing adolescents (Osman, Barrios, Guitierrez, Williams, & Bailey, 2008; Subramaniam, Harrell, Huntley, & Tracy, 2009). The predictive validity of the BHS has been well established (e.g., Chapman, Specht, & Cellucci, 2005). Cronbach's α for the BHS in this study was .79.
Impulsivity
The Barratt Impulsiveness scale, Version 11 (BIS-11; Patton, Stanford, & Barratt, 1995) is a widely used, 30-item self-report questionnaire. This measure is designed to assess impulsivity as a stable trait characteristic, taking into consideration the multifaceted nature of the construct. Each item consists of a statement (e.g., “I plan tasks carefully”), and participants are asked to indicate how often they act or think in that particular way based on a 4-point scale from 1 to 4 (rarely/never, occasionally, often, almost always/always). A total score out of 120 is obtained by summing all items. The BIS has been used across a range of contexts and samples, including adolescents (e.g., Spinella, 2007). Cronbach's αs have ranged in previous studies from .79 to .83 (Patton et al., 1995). Reliability for the BIS-11 in this study was good (Cronbach's α = .86).
Substance use
Substance use was measured using drug-related questions from the Ontario Student Drug Use and Health Survey (OSDUHS) developed by the Centre for Addiction and Mental Health (CAMH, 2009). The OSDUHS is a widely used measure by government, educational, and health officials and assesses substance use across a variety of drugs based on 12-month prevalence. This self-report survey is administered across Ontario, Canada, every 2 years since 1977 to over 150 elementary and secondary schools, by employing a regionally stratified design. For the present study, respondents indicated the frequency of use over the 12 months prior to incarceration for 16 drugs, including cannabis, heroin, methylenedioxy-methamphetamine (MDMA), methamphetamine, phencyclidine (PCP), lysergic acid diethylamide (LSD), other hallucinogens, and cocaine as well as sedatives and tranquilizers without a prescription. Consistent with CAMH documentation (Paglia-Boak, Mann, Adlaf, & Rehm, 2009), participants who indicated that they did not know about a given drug were considered nonusers of that substance, and their data were retained for analyses. The 16-item scale had good reliability (Cronbach's α = .83). For purposes of analysis, we measured the variety of substances used by dichotomizing each item (0 = have not used drug, 1 = have used drug) and summing all responses to provide equal weighting across items.
Depression
The Center for Epidemiological Studies Depression scale for Children (CES-DC; Faulstich, Carey, Ruggiero, Enyart, & Gresham, 1986) is a 20-item self-report depression inventory on a 4-point scale from 0 (not at all) to 3 (a lot), with a total score obtained by summing all items. Respondents are asked to indicate how frequently over the past week they have experienced a variety of symptoms of depression. Higher CES-DC scores are indicative of higher depression severity, with scores over 15 indicating a clinically significant level of depression as defined by the instrument authors. Test–retest reliability, internal consistency, and concurrent validity were shown to be adequate, with good psychometric properties for adolescents (Faulstich et al., 1986). The total score out of 60 was used for analysis and the reliability coefficient for the CES-DC in this sample was excellent (Cronbach's α = .91).
Data Analytic Strategy
Descriptive analyses were performed using PASW 18.0. Predicted relations among childhood maltreatment, impulsivity, hopelessness, substance use, and depression severity were examined with path analyses using the software program, Analysis of Moment Structures (AMOS), Version 18.0 (Arbuckle, 2009) with maximum likelihood estimation (MLE). The sample size of N = 110 was appropriate based on the recommended minimum rules of thumb (Hoyle, 1995; Kline, 2005).
We employed a model-trimming approach beginning with the just-identified model (Kline, 2005) and including a direct relation between childhood maltreatment and depression severity as well as indirect relations including impulsivity, hopelessness, and substance use. The nonsignificant path with the lowest standard estimate was constrained to zero, which generated an overidentified model that was used as a base of comparison for subsequent nested models that were generated using the same method of path removal. To identify the most parsimonious model fitting the data reasonably well, these steps were repeated until either the model retained only those variables demonstrating significance or the model fit was found to be significantly poorer than the previous model.
Determination of the adequacy of the models in representing the data was evaluated using established critical values of goodness-of-fit indicators. These included a nonsignificant model chi-square statistic (χ2; Byrne, 2010), normed chi-square statistic (χ2/df) < 2 (Tabachnick & Fidell, 2007), standardized root mean square residual (SRMR) ≤ .08 (Jöreskog & Sörbom, 1996), comparative fit index (CFI) and Tucker-Lewis coefficient (TLI) ≥ .95 (Hu & Bentler, 1999). General use of the TLI and CFI have been recommended with MLE because they are sensitive to model misspecification and not sensitive to sample size (Hu & Bentler, 1999). The root mean square error of approximation (RMSEA) also was included as it has been recognized as one of the most informative fit indices in path analysis, taking the error of approximation in the population and the number of estimated parameters into account (Byrne, 2010). For this study, the precision of the RMSEA was estimated with its 90% confidence interval (CI) and a significance test for closeness of fit (PCLOSE). RMSEA values of .06 or less signify a good fit between the data and the hypothesized model, while standard interpretation of the PCLOSE value dictates values greater than .05, indicating the fit of the model is close (Hu & Bentler, 1999).
Data Preparation for Path Analyses
Univariate and multivariate normality was assessed before performing the analyses. Several variables were not normally distributed, with critical ratios of skew above three and/or kurtosis above four (Kline, 2005). As a result, bootstrapping was employed to estimate model parameters via nonparametric resampling of the data (2000 pseudosamples), along with corresponding confidence intervals (CIs) and statistical significance. In terms of the overall model fit, a nonsignificant Bollen-Stine corrected p value (Bollen & Stine, 1993) reflects a good fit of the model to the data. Mardia's (1970) normalized estimate of multivariate kurtosis was <5.00, indicating multivariate normality for the model (Bentler, 2005). Table 2 shows that first-order correlations among the five measured variables used in the path analysis were not greater than .60, indicating multicollinearity was not a problem (Kline, 2005). With the exception of the association between hopelessness and substance use, all variables were significantly and positively correlated with one another.
Pearson Correlation Matrix for Path Variables (n = 110)
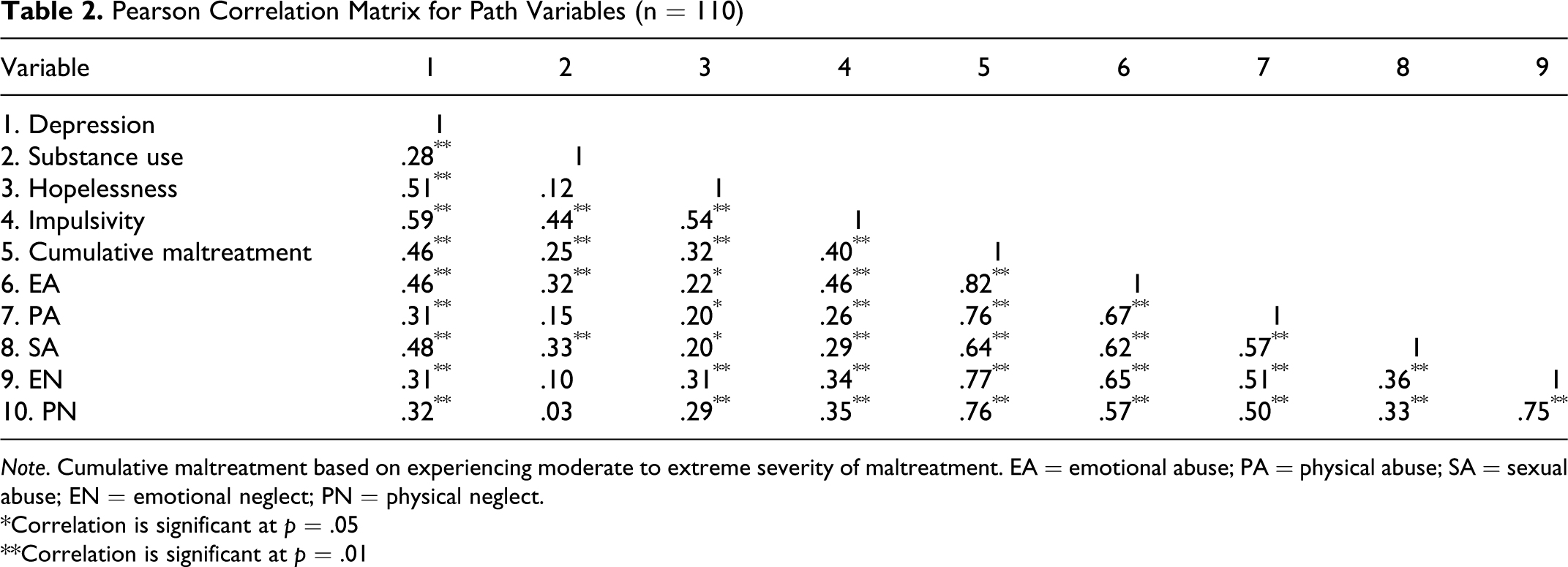
Note. Cumulative maltreatment based on experiencing moderate to extreme severity of maltreatment. EA = emotional abuse; PA = physical abuse; SA = sexual abuse; EN = emotional neglect; PN = physical neglect.
*Correlation is significant at p = .05
**Correlation is significant at p = .01
Results
Rates of Childhood Maltreatment and Depression
Means and SDs for the model variables appear in Table 3. In terms of cumulative maltreatment of moderate to extreme severity, 13.6% of participants (n = 15) endorsed a history of two subtypes of maltreatment, 14.5% (n = 16) endorsed three subtypes, 12.7% (n = 14) endorsed four subtypes, and 5.5% (n = 6) of participants endorsed experiencing all five subtypes of childhood maltreatment. Table 3 shows that this sample was also characterized by elevated rates of depression, with female reporting greater severity of depression than male youth (U = 606.50, z = −5.11, p < .001). In addition, 66.4% of participants reported depression scores within the clinical range, whereby 37 females (86.0%) and 36 males (53.7%) had scores above 15 on depression severity, and this difference was statistically significant, χ2(1, N = 110) = 12.25, p < .001. Sex differences were also identified for impulsivity, t(108) = −5.47, p < .001, and substance use (U = 611.50, z = −5.35, p < .001), with lower scores for male compared to female youth. Table 4 shows the frequency of childhood maltreatment types for the level of severity for the total sample and by biological sex. Almost 60% (n = 64) of our sample endorsed a history of moderate to extreme childhood maltreatment. This percentage increases to 77.3% (n = 85) when considering the CTQ-SF manual cutoff for any maltreatment (i.e., low through extreme severity). As presented in Table 4, a greater proportion of female than male participants endorsed extreme subtypes of emotional, physical, and sexual abuse.
Descriptive Statistics for Path Variables
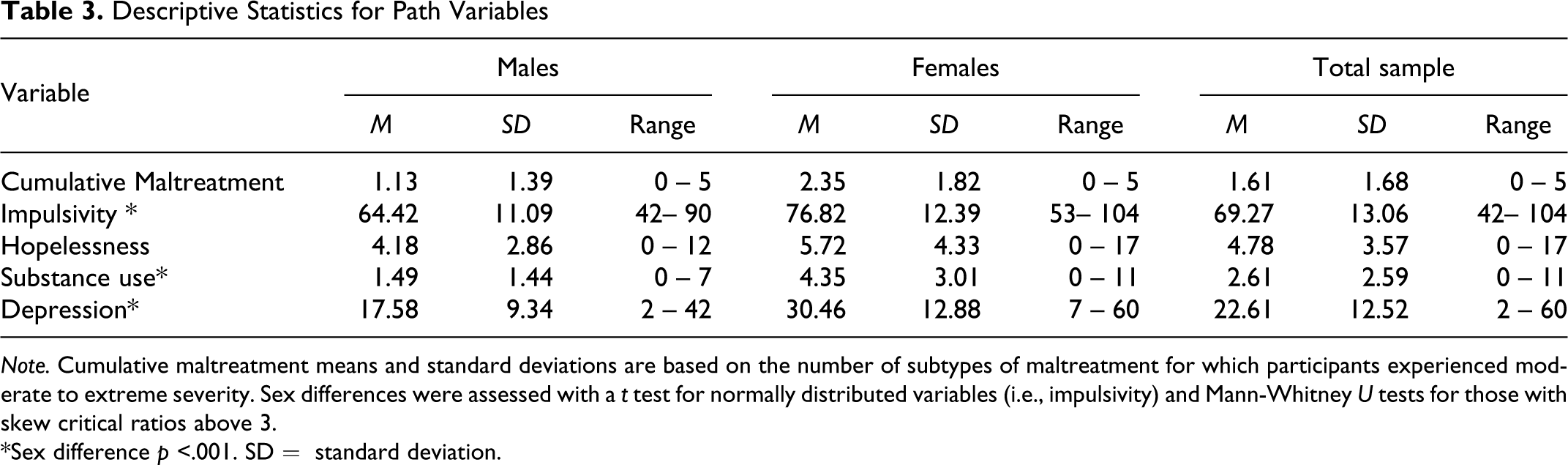
Note. Cumulative maltreatment means and standard deviations are based on the number of subtypes of maltreatment for which participants experienced moderate to extreme severity. Sex differences were assessed with a t test for normally distributed variables (i.e., impulsivity) and Mann-Whitney U tests for those with skew critical ratios above 3.
*Sex difference p <.001. SD = standard deviation.
Severity of Childhood Maltreatment
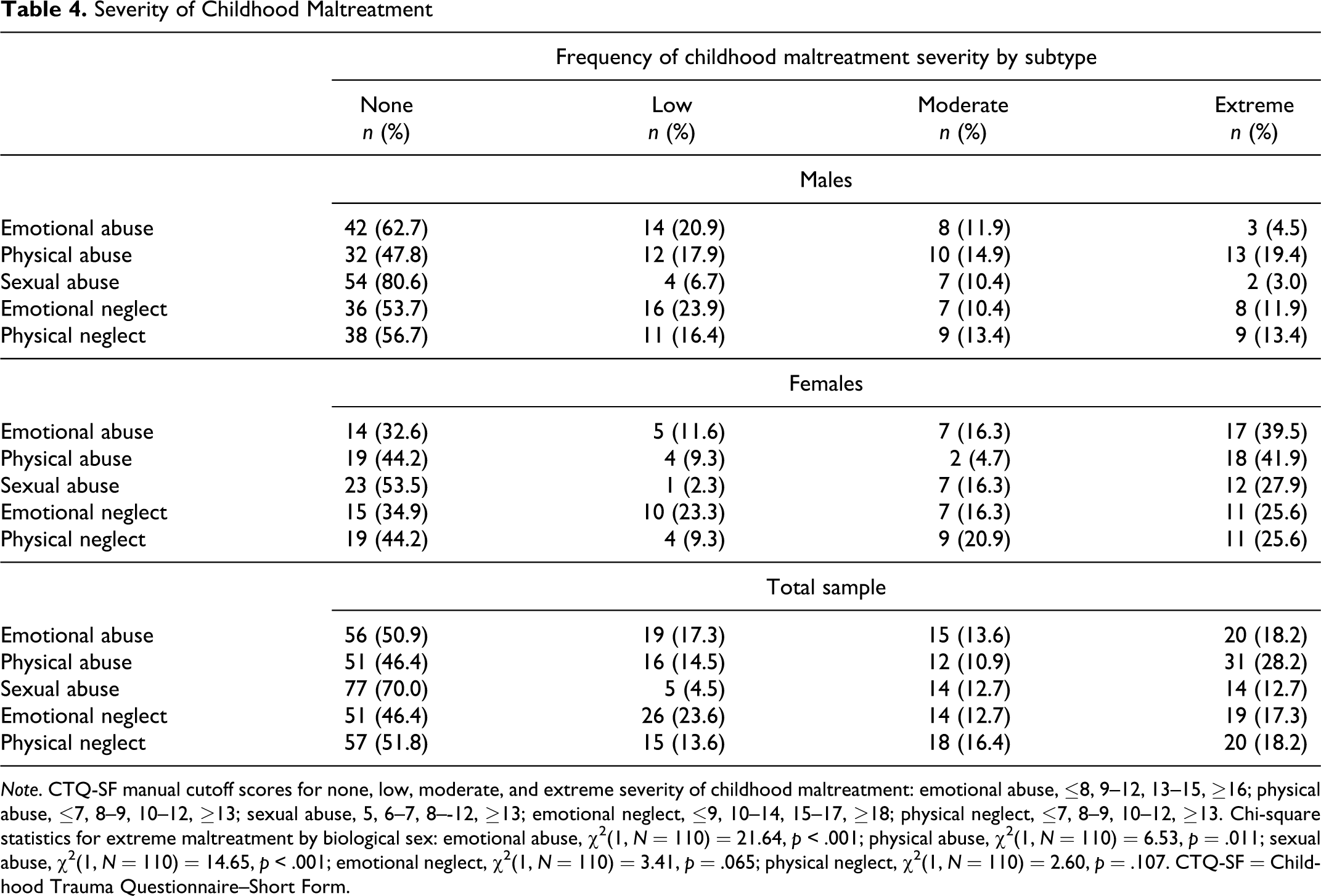
Note. CTQ-SF manual cutoff scores for none, low, moderate, and extreme severity of childhood maltreatment: emotional abuse, ≤8, 9–12, 13–15, ≥16; physical abuse, ≤7, 8–9, 10–12, ≥13; sexual abuse, 5, 6–7, 8–-12, ≥13; emotional neglect, ≤9, 10–14, 15–17, ≥18; physical neglect, ≤7, 8–9, 10–12, ≥13. Chi-square statistics for extreme maltreatment by biological sex: emotional abuse, χ2(1, N = 110) = 21.64, p < .001; physical abuse, χ2(1, N = 110) = 6.53, p = .011; sexual abuse, χ2(1, N = 110) = 14.65, p < .001; emotional neglect, χ2(1, N = 110) = 3.41, p = .065; physical neglect, χ2(1, N = 110) = 2.60, p = .107. CTQ-SF = Childhood Trauma Questionnaire–Short Form.
Model Specification
Table 5 presents the standardized regression estimates for the just-identified and final nested cumulative maltreatment models. Analysis of the just-identified model revealed that the path from substance use to depression severity was the weakest and nonsignificant (β = .04, p = .61, 95% confidence interval [CI] = [−0.12, 0.22]). This demonstrated that, despite a significant bivariate correlation, substance use no longer accounted for any substantial variance in depression in the context of childhood maltreatment, impulsivity, and hopelessness in the model. Therefore, this path was constrained to zero to form the initial Model A for subsequent comparisons. Model A demonstrated a good fit to the data, χ2(1) = 0.28, p = .59, Bollen-Stine p = .63, χ2/df = 0.28, CFI = 1.00, TLI = 1.05, SRMR < 0.01, RMSEA < 0.01, 90% CI = [0.00, 0.21], PCLOSE = .64. However, nonsignificant paths remained in the model, suggesting the complexity of the model could be reduced further. Thus, we eliminated the weakest path from cumulative maltreatment to substance use in Model A (β = .11, p = .32, 95% CI = [−0.09, 0.29]) to create Model B. All criteria for Model B indicated a good fit: χ2(2) = 1.63, p = .44, Bollen-Stine p = .51; χ2/df = 0.81, CFI = 1.00, TLI = 1.01, SRMR = 0.03, RMSEA < 0.01 (90% CI = [0.00, 0.18], PCLOSE = .53. Moreover, Model B represented a nonsignificant change in model fit (χ2 Δ2 = 1.34, p = .25, TLIΔ = 0.04), further supporting that the path from cumulative maltreatment to substance use did not substantially contribute to the model.
Standardized Regression Estimates for Nested Cumulative Maltreatment Models

Note. SD = standard deviation.
The direct path from hopelessness to substance use also failed to reach significance (β = −.16, p = .16, 95% CI = [−.36, .06]). Therefore, in the interest of parsimony, a Model C was created that constrained this path to zero. Model C demonstrated a nonsignificant difference from Model B (χ2 Δ2 = 2.44, p = .12, TLIΔ = 0.39). Moreover, Model C fit the data well, χ2(3) = 4.07, p = .25, Bollen-Stine p = .31, χ2/df = 1.36, CFI = 0.99, TLI = 0.97, SRMR = 0.04, RMSEA = 0.06, 90% CI = [0.00, 0.18], PCLOSE = .37, and all remaining paths were significant. Thus, Model C was considered the cumulative maltreatment final model. Notably, this final model accounted for 44% of the variance in depression severity (see Figure 1).

Significant standardized parameter estimates for the final trimmed cumulative childhood maltreatment model. Note the intervening roles of impulsivity and hopelessness on the relations of abuse with substance use and depression. Dotted paths indicate paths that were constrained to zero due to nonsignificance. Overall, cumulative maltreatment, impulsivity, and hopelessness explained 44% of the variance in depression severity.
Direct and Indirect Relations Between Childhood Maltreatment and Depression
AMOS assesses the strength and significance of indirect relations within the model via bootstrapping confidence limits (Arbuckle, 2009). Bootstrapping is preferred over more classical tests (e.g., Sobel), particularly in the case of multiple intervening variables, smaller samples, or deviation from normality (Bollen & Stine, 1990; Preacher & Hayes, 2008). Cumulative maltreatment maintained a strong direct relation with depression severity in the context of the additional variables in the final model (impulsivity, hopelessness, substance use). Cumulative maltreatment also had direct relations with impulsivity and hopelessness and an indirect relation with depression severity through impulsivity and hopelessness (β = .22, p < .01, 95% CI = [0.11, 0.36]). Regarding substance use, only the direct relation with impulsivity was significant (and retained in the model) and supported an indirect relation with cumulative maltreatment (β = .17, p < .01, 95% CI = [0.09, 0.28]). In summary, the model depicted in Figure 1 suggests that a substantial proportion of the relation between cumulative maltreatment and depression in this sample of juvenile offenders is linked to impulsivity and hopelessness. In the context of these variables, however, substance use failed to account for any additional variance in depression.
Discussion
Childhood maltreatment was associated with the severity of incarcerated adolescents' depression through a variety of pathways. The present study extends past research by examining the relative roles of impulsivity, hopelessness, and substance use in the relationship between cumulative childhood maltreatment and depression severity. The final model fit well and supported the intervening roles of hopelessness and impulsivity in the relation between maltreatment and depression severity. However, no support was found for the intervening role of substance use.
Consistent with other studies (e.g., Edwards et al., 2003), childhood maltreatment was positively associated with severity of depression. Results supported a direct role of cumulative maltreatment on depression over and above the role of impulsivity and hopelessness. With respect to hopelessness, results supported the association between negative events, hopeless cognitions, and symptoms of depression, as reported in the literature (e.g., DuRant et al., 1995). According to Rose and Abramson (1992; see also Cole & Turner, 1993) negative life events, and ensuing negative attributions about the future, leave individuals vulnerable to developing depression. For instance, negative attributions about the future might follow from childhood maltreatment and interfere with an individual deriving pleasure from positive events that others would find enjoyable. Notably, the clinical presentation of hopelessness may differ depending on the severity of the depressive symptoms. In the presence of severe clinical depression, the individual may be incapacitated by their symptoms and be unable to function. The results of the current study indicate that cumulative maltreatment during childhood is related to higher levels of hopelessness, which, in turn, is associated with depression severity. One possibility supported by our structural covariance model is that maltreatment in the context of hopelessness may lead to the development of depressive symptoms.
Regarding impulsivity, the findings of the present investigation accord with other studies that show that childhood maltreatment puts adolescents at higher risk to react without thinking about potential consequences, which increases the risk of depression severity. As suggested by Gerra et al. (2007), neurobiological impairment could explain the link between traumatic events, impulsivity, and depression by way of hypothalamic–pituitary–adrenal axis dysfunction. Another explanation for this relationship is borrowed from the appraisal theory of emotional states. If depression is the result of compromised coping from traumatic events (Scherer, 2001) and childhood maltreatment increases the risk for impulsivity and inappropriate coping (e.g., catastrophizing, blaming others; d'Acremont & Van der Linden, 2007), impulsivity could at least partially explain the relationship between cumulative maltreatment and depression severity in incarcerated youths. If impulsivity is an intervening variable, then behavioral and pharmacological interventions that target impulsivity also may alleviate the depression.
Contrary to expectation, results did not support the hypothesized relationships between substance use and cumulative childhood maltreatment and depression severity. It is important to clarify in this respect that the bivariate relations among these variables were significant, but these direct relations became negligible in the context of the model with intervening paths incorporating hopelessness and impulsivity. It is also of potential interest that the bivariate relations between maltreatment subtypes and substance use were specific to emotional and sexual abuse (Table 2). Future research could explore possible moderating variables, such as biological sex. For example, in a longitudinal study across adolescence and early adulthood (Lansford, Dodge, Pettit, & Bates, 2010), physical abuse was found to predict substance use for females but not males. It is also possible that underreporting of substance use underestimated its relations with depression and maltreatment. Alternatively, the lack of findings with respect to substance use may have resulted from a limitation of the study’s measurement of substance use, although statistically reliable. That is, future research might benefit from determining the degree of persistence of substance use, the prevalence of substance abuse or dependence, and/or the influence of specific types of substances on depression severity. Nonetheless, alternative analyses based on frequency of use yielded comparable results (data not shown).
Limitations and Future Directions for Research
Moving forward from these findings, it is important to consider the limitations of the present study. First, and most importantly, although the relationship between childhood maltreatment and the development of depression symptoms is well supported in the literature, the findings from the current study are limited by the cross-sectional research design, in that temporal precedence of the variables of interest could not be established. This precludes statements of causality concerning the potential role of the intervening variables. Longitudinal data are necessary to determine the timing of the maltreatment relative to the onset of the impulsivity, hopelessness, substance use, and depression symptomatology.
Second, although our sample size was adequate based on established criteria (Hoyle, 1995; Kline, 2005), a larger sample size would allow for examination of sex as a potential moderator, given greater levels of severity among females on the model variables (see Table 4). Although our sample size was sufficient for the current analyses, the reliability and complexity of a model incorporating additional factors was questionable, and, therefore, we did not incorporate sex as a control or moderator in this study. Furthermore, despite the differences in means between males and females suggesting potential moderation, it is not necessarily the case that the covariance structure would differ between the sexes. Lending support to this idea, we ran a post hoc multigroup analysis in AMOS and found that allowing path coefficients to vary between males and females failed to produce a significant difference in model fit compared to a more parsimonious model constraining all path coefficients to be equal between sexes, χ2 Δ(6) = 6.34, p = .39. Thus, under the present constraints, we believe that the current findings based on the full sample are meaningful. Of particular relevance to incarcerated samples, it might be important to explore the relation between clinical variables and offending behavior. Relatedly, this study dichotomized childhood maltreatment subtypes which results in a lack of information about the frequency of specific childhood maltreatment events and assumes equal weighting for each of the subtypes of childhood maltreatment. Nonetheless, initial analyses based on frequencies of individual subtypes yielded consistent results to that of the cumulative index model (data not shown). Future research with larger samples might benefit from a more complex research design employing nested models to compare model fit between maltreatment subtypes or the exploration of maltreatment as a latent variable using structural equation modeling.
Third, as the current study used a Canadian sample of juvenile offenders, the results may not generalize to offender samples in other jurisdictions or to adult offender populations. Fourth, common method variance may have resulted in inflated (or deflated) correlations among the variables in the model (Doty & Glick, 1998). Future studies should gather data from different sources (Reio, 2010), such as from third-party respondents, using different methods such as structured and semistructured interviews. Finally, from a statistical perspective, error associated with the measurement of intervening variables can lead to underestimation of indirect relations and model misspecification (Shrout & Bolger, 2002). However, each of the measures included in this study had good psychometric properties.
Conclusions and Implications
In considering the relative strengths and weaknesses, this study represents a preliminary step toward understanding impulsivity, hopelessness, and substance use as potential explanatory factors in the relation between cumulative childhood maltreatment and depression. Even after accounting for the influence of these variables, a significant relation between cumulative maltreatment and depression remained. This indicates additional factors should be considered when attempting to explain why maltreatment is associated with depression among incarcerated youths. Although further investigation is necessary to determine causal relations among these variables, the results suggest that cumulative maltreatment, impulsivity, and hopelessness may be important factors to address in clinical research and treatment for depression among incarcerated youth. Proper treatments could help reduce their psychological distress and may also have the additional benefit of reducing their likelihood of committing future criminal acts.
The present study suggests that careful attention in the clinical assessment and management of incarcerated juvenile offenders who present with a history of child maltreatment, hopelessness, and depression is warranted; particularly when the individual also presents with a history of risky behavior and impulsivity. Indeed, trauma-focused cognitive–behavioral therapy (TF-CBT) might be indicated to address the sequelae of symptoms in an individual with this clinical presentation (Black, Woodworth, Tremblay, & Carpenter, 2012). Depression-focused treatments may also be relevant, such as cognitive–behavioral treatment for depressed adolescents (e.g., Cuipers, Munoz, Clarke, & Lewinsohn, 2009), which has been found to reduce depression for juvenile justice-involved adolescents (Rohde, Clarke, Mace, Jorgensen, & Seeley, 2004).
Similar to depression severity and a history of maltreatment, impulsivity (Herrenkohl et al., 2000) and hopelessness (Lorion & Saltzman, 1993) have both been implicated as risk factors for criminal offending. Because cumulative maltreatment, impulsivity, and hopelessness might be antecedents of both depression severity and general antisocial behavior, they may be particularly important risk factors to address during periods of correctional confinement where treatment programming may be most accessible to these young people. Positive outcomes with CBT have been demonstrated for impulsivity (Baer & Nietzel, 1991) and hopelessness (Daniel & Goldston, 2009). When the individual presents with comorbid features, a multifaceted approach may be warranted, including a combination of CBT, coupled with possible stimulant medication for the impulsivity, and family-based therapy to address parental cognitions that might be maintaining the maladaptive behaviors (Chronis, Jones, & Raggi, 2006; Sandy & McCarty, 2005). Finally, dialectical behavior therapy appears to be a promising approach to address suicidal ideation, self-harming behaviors, and poor impulse control among juvenile offenders (Quinn & Shera, 2009).
Footnotes
Acknowledgments
We thank Dr. Feiring and the three reviewers for their constructive comments in revising the manuscript.
Authors’ Note
This study was conducted as a master's thesis by the first author under the supervision of the second author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Funding for this study was provided to David M. Day and Trevor A. Hart from the Ryerson Fund for Interdisciplinary Research (RFIS). Trevor A. Hart was supported by a New Investigator Salary Award from the Canadian Institutes of Health Research.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.