
Abstract
Research is needed to understand the role of gender in the stability, course and etiology of antisocial behavior. Family environment, given its proximal association with children’s behavior, holds great promise in understanding risk for antisocial behavior. The present study examined the role of parental acceptance and emotional responsivity as assessed using the HOME, caregiver report of intimate partner violence (IPV), and levels of physical abuse as assessed using the Conflict Tactics Scales, on subsequent symptoms of Oppositional Defiant Disorder (ODD), a childhood disorder characterized by antisocial behavior. Data were drawn from Waves 1-3, cohorts 3 and 6 of the Project for Human Development in Chicago Neighborhoods. Results suggest only minor gender differences in levels of ODD symptoms, with equal rates of stability from Wave 2 to 3 in symptom levels. For boys and girls, IPV was associated with an increased risk of ODD symptoms, and higher acceptance was associated with reduced risk of ODD symptoms. However, gender differences emerged in the impact of physical abuse and emotional responsiveness, in that the former was a significant predictor for girls only, and the latter was significant for boys only. Potential implications for these findings, including the role of gender socialization are discussed.
Keywords
Antisocial behavior (ASB) has far-reaching economic, legal, physical, and psychological consequences. Precursors to ASB often emerge in childhood, and ASB can persist from adolescence into adulthood (Cunningham & Boyle, 2002; Munkvold, 2011; Nagin & Tremblay, 2001). Developmental psychopathology emphasizes a need to understand the manifestation and course of all behavior across the life span, as well as risk factors that influence heterogeneity in its development across multiple levels of analyses (Cicchetti & Toth, 1995; Richters & Cicchetti, 1993; Sroufe & Rutter, 1984). Gender is a combination of biology (e.g., biological sex) and societal context (e.g., socialization), yet is often neglected in studies of ASB. The present study examined gender differences in course and risk of early ASB, in an effort to understand which aspects of family environment (e.g., harsh parenting, parental acceptance and responsiveness, and parental intimate partner violence [IPV]) influence the development of oppositional behaviors within a community sample of males and females.
Oppositional Defiant Disorder (ODD)
ODD is defined (American Psychiatric Association [APA], 2000) as pattern of defiant, disruptive, and hostile behavior. ODD is typically diagnosed before the age of 8, with prevalence rates between 2 and 16% depending on sampling methods (APA, 2000). Children with ODD may be more likely than their non-ODD peers to demonstrate a pattern of ASB into late adolescence and early adulthood (Fergusson, Boden, & Horwood, 2010; Maughan, 2004). Yet, increasingly, researchers posit that ODD may not be specifically associated with later ASB, but may reflect increased risk for many forms of psychopathology (Burke, Pardini, & Loeber, 2008; Harvey, Metcalfe, Fanton, & Herbert, 2011).
Gender and Prevalence of ASB
Many behaviors along the antisocial and externalizing spectrum are more common in boys than girls, particularly within clinical samples (Boylan, Vaillancourt, Boyle, & Szatmari, 2007; Fergusson et al., 2010; Maughan, 2004; Munkvold, 2011). Yet, studies of ASB tend to focus on large samples of clinic-referred boys (Lahey, Loeber, Burke, Rathouz, & McBurnett, 2002; Mannuzza, Klein, Abikoff, & Moulton, 2004; Speltz, McClellan, DeKlyen, & Jones, 1999), with less known about etiology and course of ASB among female and community samples. Many researchers suggest a need for increased scrutiny of potential gender differences in ASB and its associated diagnoses in the DSM (Crick & Zahn-Waxler, 2003; Zahn-Waxler, 1993; Zoccolillo, 1993).
Research on gender and ASB thus far has focused on conduct disorder (CD), which is often conceptualized as the longitudinal progression of ODD in adolescence (APA, 2000). Some (Zahn-Waxler, 1993; Zoccolillo, 1993) argue that the CD diagnosis is gender-biased, emphasizing physical aggression and behaviors that are more male-typical, over relational aggression, or more female-typical expressions of ASB. As a result, this may impede early identification of ASB in females. Some researchers propose lowering diagnostic thresholds for CD in females versus males (Crick & Zahn-Waxler, 2003; Zahn-Waxler, 1993; Zoccolillo, 1993).
Despite conceptual linkages between ODD and CD, it is unclear whether gender differences observed for CD extend to ODD. In the Christchurch Health and Development Study (Fergusson et al., 2010), ODD was equally common in a community sample of males and females (around 15%) by late adolescence (age 14–15 years). Other studies of childhood ODD also failed to find gender differences in prevalence (Lahey et al., 2000, 2002; Maughan, 2004). Although broader literature on ASB is marked by extreme gender differences, more research is needed to understand whether gender moderates the course and risk profiles associated with ODD.
Gender, Course, and Etiology of ASB
Moffitt (1993, 1997) identified two divergent pathways that characterized most ASB. The majority of antisocial youth fit within an adolescence-limited (AL) pathway, defined by a later onset of ASB, largely in response to struggles to achieve autonomy and peer influences. As the name implies, AL youth are unlikely to continue ASB into adulthood. In contrast, a smaller group of antisocial youth fit into a life-course-persistent (LCP) pathway, which is characterized by a childhood onset of ASB. The LCP pathway is accompanied by a severe profile of neurobiological and environmental risk, and exhibits stability of ASB into adulthood. Findings from the Dunedin study (Moffitt & Caspi, 2001) support this typology, particularly with regard to the absence of many risk factors among AL youth as compared to their LCP peers. Moffitt and Caspi (2001) assert that this typology applies equally across gender, but acknowledge that far fewer girls fit into both pathways.
Other researchers posit gender differences in the course of ASB in girls versus boys. Keenan and Shaw (1997) posit that in early childhood, girls may be as likely as boys to exhibit oppositional behavior, but socialization leads to differences in the longitudinal course of this behavior. That is, over time, girls exhibiting early problem behaviors may develop internalizing as oppose to externalizing disorders. This theory would suggest that early ODD might be less predictive of later ODD in girls versus boys. However, evidence suggests that within community samples, ODD may be somewhat stable across development. First, in the Christchurch Health and Development Study sample, Fergusson, Boden, and Horwood (2010) found that ODD in adolescence was equally associated with criminal and ASB in early adulthood across gender. Similarly, in a study by Diamantopoulou, Verhulst, and van der Ende (2011), ODD symptoms were quite stable across time in males and females, from ages 2–4 to 12–14 years. The present study adds to this growing literature by examining the continuity of ODD from early to middle childhood in males and females from a community sample.
Silverthorn and Frick (1999) put forth another theory to explain gender differences in both the course and etiology of ASB. According to their theory, girls demonstrate a later age of onset for ASB than most boys, but mirror the pattern of comorbidity (e.g., familial dysfunction, cognitive, and neuropsychological deficits) and continuity of ASB that is seen in boys within the LCP pathway. Silverthorn and Frick describe the female pattern of ASB as a delayed onset pathway. Indeed, Silverthorn, Frick, and Reynolds (2001) examined age of onset and correlates of ASB among N = 74 adolescents in criminal justice settings. Nearly all (94%) girls exhibited an adolescent onset (after age 12) versus 54% of boys. Furthermore, delayed onset girls demonstrated a similar risk profile to that of childhood onset boys, with significantly higher levels of poor impulse control, callous unemotional traits, and ODD symptoms as compared to AL boys. However, a few limitations limit the extension of this study to ODD. First, the study utilized a criminal justice sample, which could inflate estimates of the stability of ASB. In addition, the study used CD symptoms or police contact as markers of the onset of ASB, and cannot be used as an estimate of the etiology or course of ODD specifically. Nonetheless, this theory does suggest that girls exhibiting ASB may exhibit a severe pattern of comorbid risk similar to that of LCP boys.
Parenting and ASB
A great deal of literature suggests the importance of early environment, particularly parenting, in the development of ASB (Bowlby, 1980; Cicchetti & Toth, 1995). Child maltreatment has received much attention due to the key influence of early child–caregiver interactions on children’s attachment, affect regulation, and peer relationships (Cicchetti & Lynch, 1995; Maughan & Cicchetti, 2002; Sroufe, Fox, & Pancake, 1983). Yet, many aspects of adversity in early family environment are likely to hold importance in understanding the etiology of ODD, including other aspects of parenting, and exposure to IPV. In Moffitt and Caspi’s (2001) study of AL versus LCP youth, harsh discipline, inconsistent discipline, and family conflict were all predictive of LCP, but not AL trajectories for ASB in males and females. The current study focused on parenting practices and exposure to IPV as potential risk factors for ODD symptoms within a community sample.
The use of harsh or overly coercive physical discipline has been linked to an increased risk of ASB, particularly aggression, in numerous studies (Burnette, Oshri, Lax, Richards, & Ragbeer, 2012; Burnette & Reppucci, 2009; Cicchetti & Lynch, 1995; Fergusson & Lynskey, 1997; Knutson, DeGarmo, Koeppl, & Reid, 2005; Widom, 1989). According to Patterson’s Coercive Development model (1982), the use of coercive parenting strategies, including extreme variants, such as physical abuse, is likely to be a dynamic interaction, which is influenced by both children’s temperament and parental behavior. This dynamic evolves over time and serves to reinforce and exacerbate children’s disruptive behavior. Several longitudinal studies support this assertion (Burke et al., 2008; Jaffe, Caspi, Moffitt, & Taylor, 2004; Jaffee, Strait, & Odgers, 2012). Despite a great deal of literature more broadly on externalizing behaviors, few studies have focused specifically on the link between harsh parenting and ODD. Boden, Fergusson, and Horwood (2010) found a significant association between prior physical abuse exposure and ODD symptoms in a community sample of adolescents; however, the authors did not test for difference by gender. The present study aims to replicate this finding, examining linkages between harsh parenting and ASB, while also testing for gender differences in this pathway.
Aside from harsh physical punishment, several other aspects of parenting may add value in understanding the etiology of disruptive and ASB. One study of ODD in childhood showed that parent’s negative affect or overreaction to children’s behavior was associated with later ODD symptoms in children, as well as with the increases in this behavior over time (Harvey, Metcalfe, Fanton, & Herbert, 2011). In another study examining familial risk factors associated with comorbid ODD and CD among boys with attention deficit/hyperactivity disorder, negative or ineffective punishment by mothers was associated with both types of disruptive disorders. In contrast, low maternal warmth was specifically associated with boys who exhibited comorbidity with CD but not ODD (Pfiffner, McBurnett, Rathouz, & Judice, 2005). Parental sensitivity or nurturance, the extent to which parents anticipate and respond to children’s needs, has also emerged as a potential protective factor in reducing the risk of early behavior problems (Bradley & Corwyn, 2007a). Trentacosta et al. (2008) found that parental nurturance and involvement at age 3 mediated the impact of other environmental risk factors on ASB at age 4 within a community sample. Work by Bradley and Corwyn (2007b) suggests maternal sensitivity was beneficial for children with difficult temperaments (e.g., marked by intense moods, low adaptability) in reducing risk of externalizing behavior. In the same study, acting annoyed or angry with a child was associated with more externalizing symptoms even after adjusting for the impact of maternal sensitivity and child temperament (Bradley & Corwyn, 2007b). However, more research is needed to delineate specific parenting practices that are associated with ODD, as well as whether these patterns differ by gender.
IPV
In this study, IPV is defined as physical aggression between primary caregivers and their partners or spouses. Notably, exposure to IPV is often defined as a form of emotional maltreatment (Manly, Kim, Rogosch, & Cicchetti, 2001). Some hypothesize that exposure to extreme conflict between parents interferes with children’s sense of emotional security, and may even lead to changes in physiological reactivity (Davies, Sturge-Apple, Cicchetti, & Cummings, 2007; Davies, Winter, & Cicchetti, 2006). Exposure to IPV may be associated with increased externalizing and disruptive behaviors in young children, even after adjusting for the impact of other forms of maltreatment in the home (English et al., 2009). These effects have been replicated in children as young as 2–3 years of age (DeJongh, von Eye, Bogat, & Levendosky, 2011). However, a recent search yielded no recent studies examining the role of IPV in the etiology of ODD specifically. The current study addresses this need, by examining how the presence of IPV in the family influences male and female ODD symptoms.
Gender and parenting
Chodorow (1978) emphasizes the early influence of socialization on the conceptualization of identity for male and female children. According to her theory, girls are encouraged early in childhood to see themselves as an individual within the context of their relationships with others. In such an environment, empathy, kindness, and a low level of aggression toward others would be valued attributes. In contrast, boys are strongly socialized to establish an independent identity apart from others; hence, independence, autonomy, and assertiveness would be valued attributes. Within such a context, female ASB would represent a more severe departure from the norm and may be preceded or followed by more extreme parenting practices. Hence, the present study sought to test for gender moderation in the associations between parenting and ASB.
Current Study
As summarized above, while ODD overlaps with other disruptive and ASB disorders, emerging literature suggests a need to better understand ODD as a distinct early form of ASB. Although many studies have examined familial risk factors for externalizing and ASB, little is known about the generalizability of these findings for ODD specifically, as well as the extent to which these may differ for boys and girls. The present study examined (a) the course of ODD among a community sample of boys and girls, (b) the contribution of parenting practices and domestic violence, and (c) the extent to which these associations differed across gender.
Method
Participants
This study consisted of secondary data analyses from the Longitudinal Cohort Study of the Project on Human Development in Chicago Neighborhoods (PHDCN; see Earls, Felton, Brooks-Gunn, Raudenbush, & Sampson, 1994–2001), cohorts 3 and 6. PHDCN was a longitudinal study of child and adolescent development in racially, culturally, and economically diverse neighborhoods. The current study uses data from the Longitudinal Cohort Study, which consisted of three waves of data collection from children and their primary caregivers (parents) from several cohorts (0–6 months, 3, 6, 9, 12, 15, and 18 years). Stratified probability sampling based on socioeconomic status (SES) and race/ethnicity yielded a representative sample from various neighborhoods in Chicago, from different socioeconomic strata. The current sample was limited to 1,992 youth (49.6% male), from cohorts 3 and 6. From this sample, 1,583 (79.5%) completed the Wave 2 measures and 1,491 (74.8%) completed Wave 3 measures used in the current study. The mean age of the full sample was 4.63 years (SD = 1.54) at Wave 1, 6.77 years at Wave 2 (SD = 1.60), and 9.23 years (SD = 1.59) at Wave 3. Approximately 48.1% of participants were Hispanic, 33.3% were Black, and 14.4% were White. The PHDCN data set uses a score for SES derived from principle components analyses of three variables assessing education level of primary caregiver, household income, and a socioeconomic index score. Across Waves 2 and 3, youth missing data tended to be characterized by lower familial SES, and Hispanic ethnic identification, and were less likely to have parents who were married.
Measures
Harsh Parenting
Harsh parenting was operationalized as the use of moderate to severe physical discipline strategies. Harsh parenting was assessed at Wave 1 using the Conflict Tactics scale–Parent Child (CTS-PC, Straus, 1979), a 17-item primary-caregiver report of the frequency of physical discipline used by the caregiver in the past year. For the purpose of analyses, the physical aggression subscale was used, which included items such as throwing or kicking things at the child, pushing or grabbing the child, or hitting the child with something. For each item, caregivers indicated the frequency of the behavior in the past year on a 0 (never) to 6 (>20 times) scale. Scores were added across 7 items to create a total score (α = .60).
Acceptance and responsivity
In addition, a modified version of the HOME Observation for Measurement of the Environment (Caldwell & Bradley, 1984; Selner, 1994) assessed other parenting practices. The HOME consists of a semistructured interview and observation, which took place in the home at Wave 1. Two subscales were used. The acceptance subscale assessed parental avoidance of expressing annoyance, scolding, or use of physical punishment during the observation period (α = .60). The responsivity subscale assessed caregiver-initiated positive interactions and positive feelings toward the child conveyed during the observation (α = .78).
IPV exposure
In Wave 1, caregivers reported on the degree of physical aggression by and toward partners using the Conflict Tactics scale for Partner and Spouse (CTS-PS, Straus, 1979). The CTS-PS consists of 19 items, and assessed the extent of physical abuse perpetrated toward and by the primary caregiver’s’ partner. Items paralleled those for the CTS-PC, with the addition of 2 items assessing whether caregivers threatened their partner with a knife or other weapon, or used a knife or other weapon on their partner. Due to the low endorsement, items were used to create a dichotomous variable reflecting whether any IPV occurred in the past year.
ODD symptoms
The present study used 10 items from the Child Behavior Checklist (CBCL: Achenbach, 2001), to assess ODD symptoms. Prior studies using similar methods suggest that CBCL items mapping onto ODD symptoms correlate significantly with diagnoses from clinical interviews (Diamantopoulou, Verhulst, & van der Ende, 2011). However, when used to approximate the presence or absence of a diagnosis, CBCL methods tend to result in higher prevalence rates of ODD diagnoses as compared to interviews (Krol, De Bruyn, Coolen, & van Aarle, 2006). Items were rated by parents at Waves 2 and 3 on a 0 (not true) to 2 (very true) scale. Items mapped onto Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision symptoms for ODD, including items such as arguing with adults, having a hot temper, not getting along with others, and taunting or annoying others. For bivariate analyses, a composite score was created which represented the sum of the 10 items. For structural equation models (SEM), items were modeled at each wave as a 1-factor latent construct using MPlus with a WLSMV estimator, specifying that items were categorical. A latent continuous construct was used for ODD, rather than diagnostic status, since research suggests that dimensional rather than categorical methods of assessing ODD explain more variance in longitudinal outcomes (Fergusson et al., 2010).
Analyses
Analyses were conducted in MPlus version 6.00 (Muthén & Muthén, 1998–2010), using Full Information Maximum Likelihood to account for missing data. Gender moderation was assessed by testing for significance of interaction terms within an SEM framework, and examined within a multiple group framework (Muthén & Muthén, 1998–2010; Tabachnick & Fidell, 2001). First, a measurement model was tested, in which ODD within each wave was predicted by CBCL items for that wave, this model was also tested for gender invariance. Next, a structural model was tested. Wave 1 parenting and IPV were allowed to predict Wave 2 ODD symptoms, and Wave 2 ODD symptoms were allowed to predict Wave 3 ODD symptoms. Age and SES were entered as covariates in these models, as well as all gender interaction terms (e.g., Gender × IPV, etc.). Model fit was evaluated using global fit indices, including root mean square error of approximation (RMSEA) < .09, comparative fit index (CFI) > .05, and Tucker–Lewis Index (TLI) >.95 (Hu & Bentler, 1999). Finally, multiple group models were run to understand significant interaction terms. In this model, any pathways from the prior model that showed significant interactions with gender were permitted to vary by gender.
Results
Boys and girls were similar with respect to observed variables, exhibiting only slight differences in the level of ODD symptoms at Waves 2 and 3 (see Table 1). Bivariate analyses showed some gender differences in the associations between parenting and ODD symptoms. As shown in Table 2, harsh parenting was strongly associated with ODD symptoms at Waves 2 and 3 in girls but not boys. In contrast, lower parental responsiveness was associated with ODD at Waves 2 and 3 in boys but not girls. Lower parental acceptance as associated with ODD symptoms in boys and girls at both waves. Finally, bivariate t-tests showed that mean levels of ODD symptoms were higher among both males (Wave 2: t = −3.45, p < .001, Wave 3: t = −2.31, p < .001) and females (Wave 2: t = −3.98, p < .001, Wave 3: t = −3.52, p < .001) who had experienced IPV in the home as compared to those who had not experienced IPV.
Descriptive Statistics for Demographics, Parenting, Intimate Partner Violence Exposure, and ODD Symptoms by Gender.
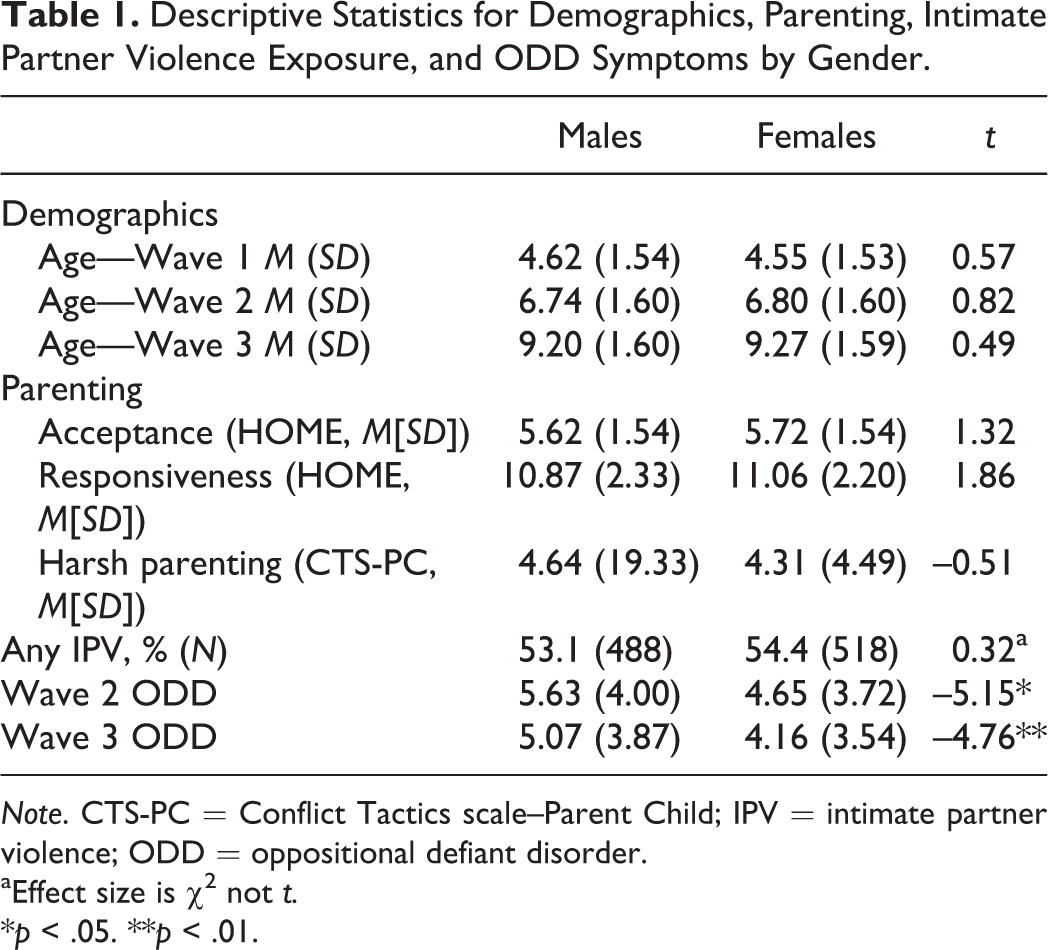
Note. CTS-PC = Conflict Tactics scale–Parent Child; IPV = intimate partner violence; ODD = oppositional defiant disorder.
aEffect size is χ2 not t.
*p < .05. **p < .01.
Correlations Between Parenting Characteristics, Physical Abuse, and ODD Symptoms by Gender.
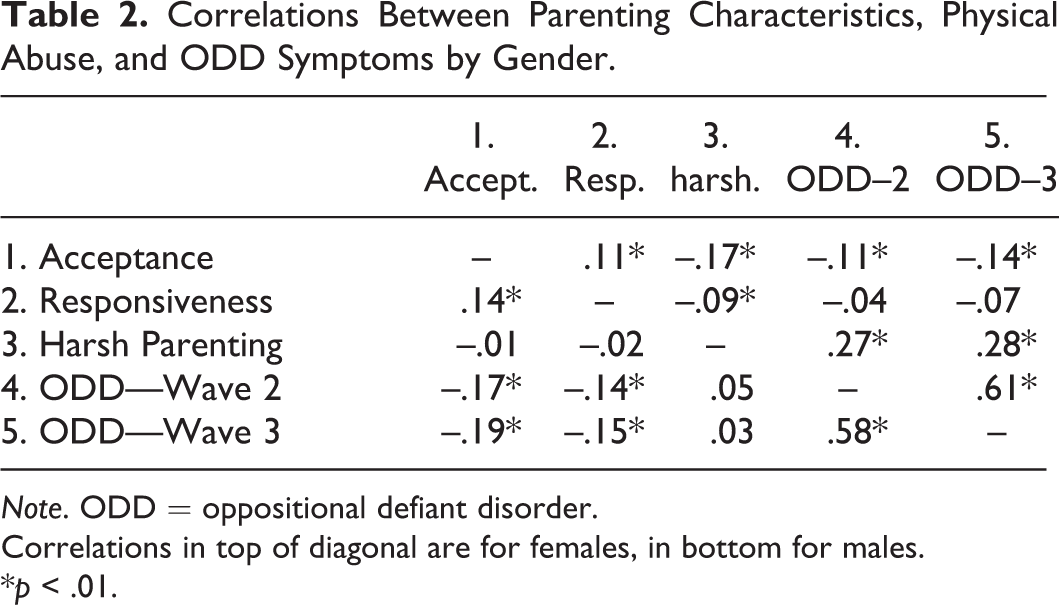
Note. ODD = oppositional defiant disorder.
Correlations in top of diagonal are for females, in bottom for males.
*p < .01.
Measurement
A measurement model of ODD in which CBCL items predicted ODD at Waves 2 and 3 provided an excellent fit to the data (χ2 = 278.8, df = 101, p < .001, CFI = .975, TLI = .990, RMSEA = .032). A test for invariance by gender did not show a significant improvement in model fit by allowing loadings to vary; therefore, the same model was used for males and females. Factor compositions of the measurement model are shown in Table 3.
Measurement Model Loadings and R 2.

Note. ODD = oppositional defiant disorder.
Stability and Risk Factors Associated With ODD
Table 4 summarizes the SEM model with interaction terms that yielded the best fit to the data (χ2 = 829.7 df = 215, p < .001, CFI = .912, TLI = .949, RMSEA = .045). In this model, ODD at Wave 2 was highly predictive of ODD at Wave 3, suggesting strong stability of symptoms from early to middle childhood. Further, harsh parenting, acceptance, and IPV exposure were each predictive of ODD symptoms at Wave 2, and there were significance interactions for Gender × Acceptance, Gender × Responsivity, and Gender × Harsh Parenting. A multiple group model in which pathways from harsh parenting, emotional responsiveness, and acceptance to ODD Wave 2 symptoms were allowed to vary is shown in Figure 1. As shown, harsh parenting was positively associated with ODD symptoms at Wave 2 for girls, but not boys; emotional responsiveness was negatively associated with ODD Wave 2 symptoms for boys, but not girls; and acceptance was negatively associated with ODD Wave 2 symptoms for both, but demonstrated a stronger association for boys versus girls.
Unstandardized Estimates From Model Predicting ODD Symptoms.
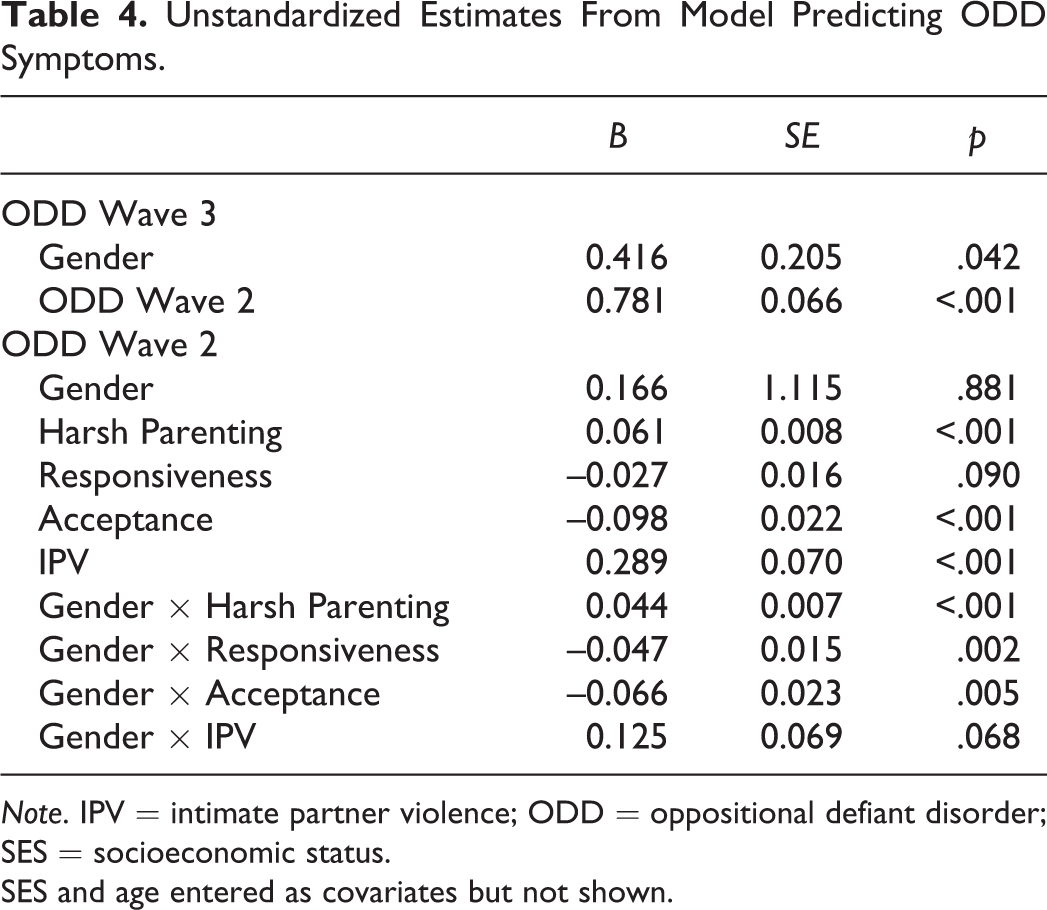
Note. IPV = intimate partner violence; ODD = oppositional defiant disorder; SES = socioeconomic status.
SES and age entered as covariates but not shown.
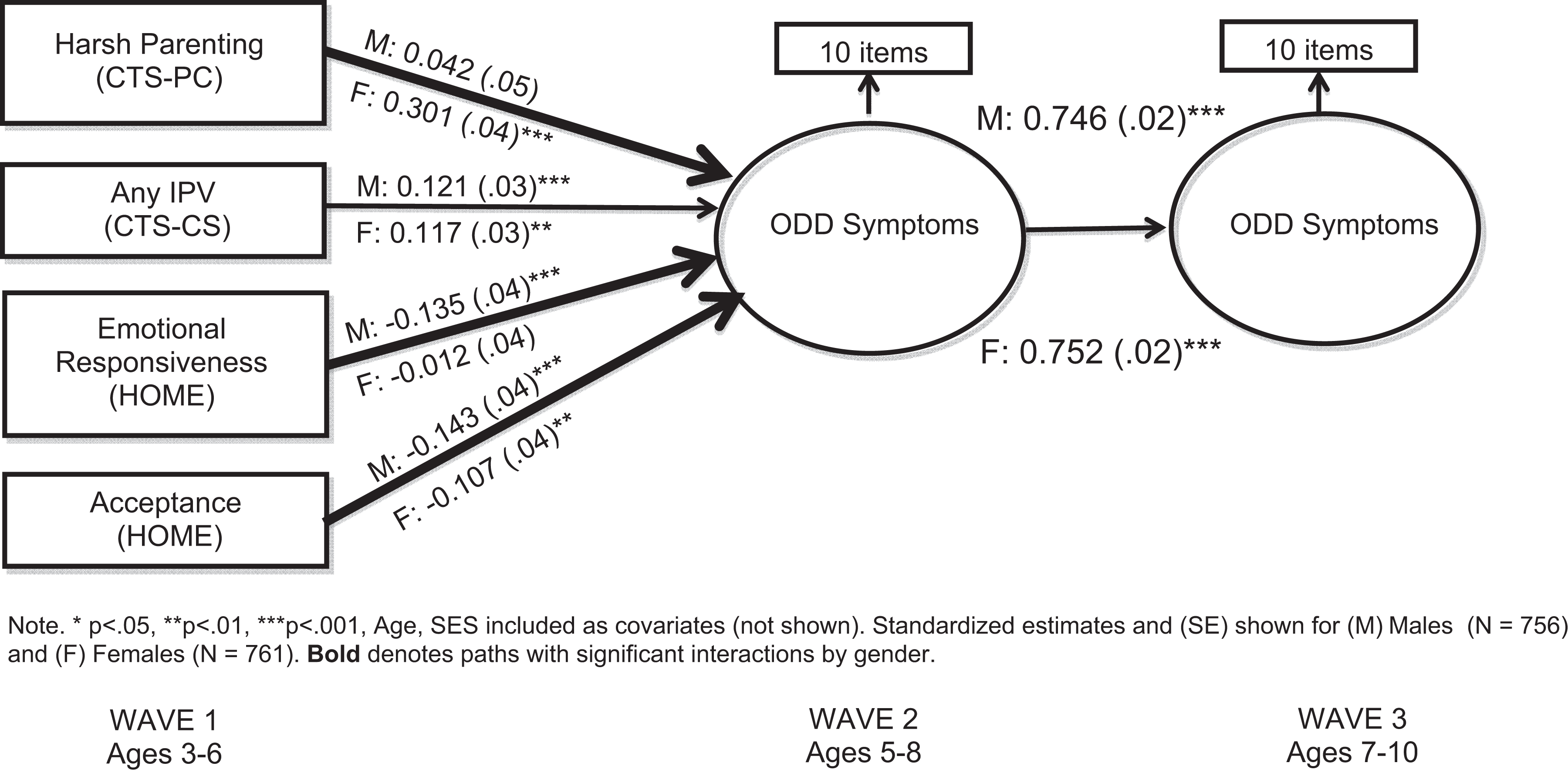
Longitudinal model predicting oppositional defiant disorder (ODD) symptoms from emotional responsiveness, parental acceptance, harsh parenting, and intimate partner violence (IPV) in the Project on Human Development in Chicago Neighborhoods (PHDCN) sample.
Discussion
The present study examined the impact of gender on the prevalence, stability, and etiology of early ASB, operationalized as ODD. In contrast to existing literature on ODD (Lahey et al., 2000; Maughan, 2004), there were small gender differences in mean levels of oppositional behaviors in boys versus girls. However, ODD symptoms in early childhood were equally associated with ODD symptoms in middle childhood in boys and girls. Results suggested differences in the influence of some aspects of parenting on children’s oppositional behavior. After adjusting for gender, age, and SES, harsh parenting was a salient risk factor for ODD symptoms in girls but not boys. In contrast, emotional responsiveness served as a protective factor against ODD in boys but not girls. Notably, exposure to IPV and low parental acceptance were associated with increased risk of ODD symptoms in boys and girls. Implications for future research on the role of gender in the stability and etiology of ASB are discussed.
Prevalence
Data from this community sample are somewhat inconsistent with a small but growing literature suggesting gender similarity in the level of oppositional behavior exhibited by boys and girls in childhood (Lahey et al., 2000; Maughan, 2004). Within this sample, mean levels of ODD symptoms were higher in boys than girls at Waves 2 and 3. However, differences were relatively small, and not as large as expected given the broader literature on gender differences in ASB. One potential explanation is that symptoms of ODD are less gender-biased than symptoms used to diagnose CD, for example, relying less on physical aggression. In fact, the ODD symptoms used in the current study included only 1 item indicative of physical aggression. If confirmed through other studies, this might suggest that ODD is a more gender-neutral means of identifying girls at risk for future ASB than CD, which is more widely studied.
Stability
More research is needed on the long-term outcomes of children with early oppositional behaviors. However, findings from this study suggest that ODD is quite stable in childhood. If ODD is linked to long-term negative outcomes, this would provide further support that ODD could be a helpful diagnostic tool in identifying girls at risk of criminality, substance use, and other forms of ASB. Once again, ODD is a diagnosis that has received less attention in this regard than CD, so future studies are needed.
However, caution is warranted, as it is equally plausible that the expression of ASB changes over time and may be influenced by environmental pressures, namely socialization. If true, smaller gender differences in ASB may be evident early in childhood, but grow more pronounced in later adolescence, as socialization grows more influential. An observational study by Chaplin, Cole, and Zahn-Waxler (2005) nicely demonstrates how parental socialization can directly impact children’s expression of emotions and associated psychopathology over time. Specifically, they observed gender differences in parents’ responses to emotional expressions of preschool-aged children, which resulted in subsequent gender differences in emotional expression and problem behaviors.
A related question is whether socialization leads girls inclined toward ASB to channel this behavior into more socially acceptable variants, namely relational aggression (Crick & Grotpeter, 1995). If so, relational aggression may hold a great deal of promise in understanding ASB more broadly for males and females. Indeed, Crick, Ostrov, and Werner (2006) showed that assessments of relational aggression do add predictive value in understanding current and future psychopathology in children, even after accounting for levels of physical aggression. The current study did not include data on ODD symptoms from early childhood to adolescence, or measures of relational aggression. A better understanding of the associations between parental socialization, ODD symptoms, and relational aggression, could contribute significantly toward understanding the course of female ASB.
Etiology
The current study does suggest that some aspects of parenting differentially influence boys’ and girls’ risk for oppositional behavior. These findings should be interpreted with care, as this is one of the first studies to evaluate this question. Tentatively speaking, the current study suggests that the use of harsh or coercive physical punishments toward girls may more directly impact subsequent oppositional behavior, as compared to the same behavior with boys. Indeed, we found no gender differences in the level of harsh parenting perpetrated toward boys or girls. One interpretation is that harsh parenting interacts with gender role norms to yield different behavioral outcomes. As noted earlier, gender socialization theories suggest that the social identities of girls and boys differ in their motivations and goals; with girls being pressured more to associate with others, and boys being encouraged to differentiate from others (Chodorow, 1978). Hence, parenting practices may interact with gender socialization practices to yield divergent behavioral outcomes for boys versus girls. Similarly, the finding that emotional responsiveness was a protective factor for boys, but not girls in the development of ODD symptoms is in keeping with the hypothesis that gender socialization may moderate linkages between parenting and ASB. Namely, boys for whom parents exhibited concern, empathy, and emotional availability may find it easier to interact with and form positive relationships with others, decreasing risk of oppositional behavior. Future studies should examine this process, to determine whether this finding can be replicated, and whether gender role may serve as a mediator of this association.
The last set of findings, that acceptance and IPV were associated with ODD symptoms in males and females, is not surprising. What the current study adds is mounting evidence that these aspects of parenting and home environment still predict ODD symptoms, even after adjusting for multiple other aspects of home environment and SES. Importantly, the current study did not assess children’s direct exposure to IPV, but simply the level of IPV within caregiver’s romantic relationships. Therefore, it would seem that any level of IPV is likely to impact children negatively, regardless of whether parents report direct exposure or not. Finally, the finding that acceptance served as a protective factor against ODD symptoms is in keeping with the premise of many early intervention programs. Interventions such as the Incredible Years curriculum, which focuses on teaching parents effective positive methods of disciplining children (Webster-Stratton & Hammond, 1997), while minimizing negative interactions, have shown great promise in reducing symptoms of CD and ODD over a 6-year period (Drugli, Larsson, Fossum, & Mörch, 2010). These data support the idea that early child–caregiver interactions that are characterized by emotional availability and avoidance of coercive practices, may reduce ASB.
Strengths and Limitations
The study is one of the few that examined ODD symptoms across gender, used a large community-based sample, and tested the simultaneous influence of several aspects of early family environment on children’s oppositional behavior longitudinally. Data were comprised of parent report (of ODD symptoms, IPV, and harsh parenting), and independent observations collected within the home (for parenting). The study also tested for gender moderation in the level and stability of ODD, as well as in the longitudinal influence of family environment on ODD.
Despite such strengths, findings should be considered in light of several limitations. First, the data represent parental report of ODD symptoms, IPV, and harsh parenting. Therefore, associations may be artificially inflated due to method bias, or may underestimate constructs of interest, as parents may have been reluctant to report IPV or use of physical punishment. The current study was also limited in its assessment of parenting practices. A broader literature emphasizes the cumulative risk associated with exposure to multiple forms of childhood abuse or maladaptive parenting practices (Manly et al., 2001; Manly, 2005). Furthermore, while parent report is a common method of assessment in the broader literature on early childhood ODD (Lahey et al., 2000), the use of collateral informants or observational data could minimize bias in the reporting of symptoms. Finally, the present study only examined the impact of parenting and family environment, and did not address several variables, such as temperament, genetic predisposition, race/ethnicity, neighborhood, or socioeconomic variables, which may impact behavior. This would be an important next step. For example, many studies show for example, that temperament and parenting styles interact to influence ASB (Bradley & Corwyn, 2007b; Lengua & Kovacs, 2005; Stright, Gallagher, & Kelley, 2008). Hence, conclusions are tentative, and future research is needed to elucidate mechanisms.
Implications and Conclusions
Nonetheless, the present study underscores several avenues for better understanding ASB in young childhood. First, there is a continued need to investigate the role of gender in the etiology of ASB across development. This work should consider multiple biological and environmental influences that may differ in boys versus girls, including gender socialization. Second, ODD appears somewhat distinct in the spectrum of ASB, with fewer gender differences in prevalence than other disruptive behavior disorders. Further research on ODD is needed to understand its course and development in large samples of females and males. Future studies should examine various aspects of family environment, in order to understand how interventions can be used to buffer stressors such as IPV or harsh parenting.
In summary, ODD showed fewer gender differences as compared to other diagnosis associated with ASB, yet demonstrated stability in childhood. While multiple adverse experiences, including IPV and harsh parenting, contributed to increased risk of ODD symptoms, positive aspects of parenting may serve as a protective buffer. Notably, the nature of these associations may differ for boys versus girls—underscoring a need to understand potential biological and environmental explanations for gender differences in the pathways to ASB.
Footnotes
Acknowledgment
The author thanks the National Institutes of Justice and the John D. and Catherine MacArthur Foundation for funding the collection and archiving of the PHDCN data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.