
Abstract
Maternal adverse childhood experiences (ACEs) have been associated with negative physical and mental health outcomes in adulthood. Less is known regarding how maternal ACEs relate to perinatal depressive symptoms or the intergenerational effect of maternal childhood trauma history on birth outcomes and infant functioning. To address this gap, an at-risk sample of 398 pregnant women was recruited from Women, Infants, and Children health clinics. Participants completed a prenatal (M = 4.84 months before due date) and postnatal (M = 6.76 months after birth) assessment and provided birth outcome data. At the prenatal assessment, mothers completed an ACEs measure which assessed experiences of childhood maltreatment and household dysfunction. Self-report measures of maternal depressive symptoms were obtained at both time points. Mothers reported on infant socioemotional functioning at 6 months. Maternal ACEs predicted higher levels of prenatal depressive symptoms. Childhood maltreatment experiences, in particular, predicted higher postnatal depressive symptoms and a smaller reduction in depressive symptoms across the perinatal period. Regarding intergenerational associations, maternal childhood maltreatment directly predicted higher levels of maladaptive infant socioemotional symptoms, whereas maternal household dysfunction indirectly related to infant socioemotional symptoms through maternal age at first pregnancy and infant birth weight. Limitations and future directions are discussed.
Keywords
Adverse childhood experiences (ACEs), including childhood maltreatment and household dysfunction, have been robustly associated with a range of deleterious outcomes across the life span (Felitti et al., 1998). Childhood maltreatment includes experiences of physical, sexual, or emotional abuse or physical or emotional neglect (Cicchetti & Valentino, 2006). Household dysfunction refers to exposure to a range of traumatic or stressful experiences within the family context including household substance abuse, parental separation or divorce, having a family member with mental health difficulties or in prison, or domestic violence (Felitti et al., 1998). A large body of literature supports the association of ACEs, including both childhood maltreatment and household dysfunction, with increased risk of a range of medical conditions and internalizing and externalizing psychological symptoms (Felitti et al., 1998). For example, ACEs have been shown to explain 50–78% of the variance in population risk for adult depression, substance abuse, and suicide attempts (see Anda et al., 2006, for a review).
Thus, early trauma and life stressors during childhood have a pervasive influence on adult functioning. Less is known regarding the intergenerational influence of maternal ACEs on (1) maternal depressive symptoms during the pregnancy period or (2) subsequent infant outcomes. To address this critical gap, the present study considers pathways through which maternal experiences of childhood maltreatment and household dysfunction relate to maternal perinatal depressive symptoms, reproductive birth outcomes, and early infant functioning.
Maternal ACEs and Depressive Symptoms
Maternal ACEs are strongly associated with depression across the life span (e.g., Chapman et al., 2004; Felitti et al., 1998); however, less work has focused on depression during and after pregnancy. The perinatal period is particularly vulnerable to maternal depression due to a range of changes in physical, hormonal, and neurochemical functions (Feldman, Weller, Zagoory-Sharon, & Levine, 2007). Perinatal depression refers to symptoms during pregnancy (prenatal/antenatal) and/or the first year after birth (postpartum; Gavin et al., 2005); both prenatal and postpartum depressive symptoms are prevalent and related to important child outcomes including physical birth outcomes, responsiveness, infant sleep, and later emotional and behavioral problems (Field, 2011; Gavin et al., 2005). Therefore, examining associations between maternal ACEs and perinatal depressive symptoms is critical for identifying those at risk for depression during this period.
A growing body of literature has evaluated maternal childhood trauma history in relation to perinatal depressive symptoms, although research findings have been equivocal (for a review, see Alvarez-Segura et al., 2014). Overall, Alvarez-Segura and colleagues (2014) concluded that there is a positive association between maternal abuse histories and perinatal depressive symptoms. Several studies have reported that maternal histories of childhood maltreatment positively predicted depressive symptoms at the time of pregnancy (e.g., Benedict, Paine, Paine, Brandt, & Stallings, 1999; Chung, Mathew, Elo, Coyne, & Culhane, 2008; Mezey, Bacchus, Bewley, & White, 2005), with some reporting these associations across the entire perinatal period (Meltzer-Brody, Boschloo, Jones, Sullivan, & Penninx, 2013; Mezey et al., 2005). In contrast, other studies have reported associations between abuse histories and prenatal but not postpartum depression (e.g., De Venter et al., 2015). Importantly, few studies have considered change in depressive symptoms across the perinatal period. For example, Onoye and colleagues (2013) reported individual variability among females in the rate of change in perinatal depressive symptoms, but this study did not consider risk factors that predicted trajectories of change in depression. One study found that women who endorsed more childhood trauma manifested less reduction in depressive symptoms from the perinatal period to 3 months postpartum (Grote et al., 2012), suggesting that maternal ACEs may be related to the amount of change in depressive symptoms during this period. To clarify these findings, it is essential to examine associations between maternal ACEs history and depressive symptoms during both the prenatal and postnatal periods. The current investigation considers depressive symptoms at both time points and extends the literature by considering ACEs in relation to change in depressive symptoms across the perinatal period.
Experiences of childhood maltreatment may more strongly predict maternal perinatal depressive symptoms than experiences of broader household dysfunction. The majority of the extant literature reports significant associations between indices of childhood maltreatment and maternal perinatal depression (Alvarez-Segura et al., 2014). For example, postpartum maternal depressive symptoms have been associated with childhood experiences of violent trauma, including maltreatment, but not experiences of nonviolent trauma which may encompass broader indices of household dysfunction (Stevens, Ammerman, Putman, & Van Ginkel, 2002). Other work focused on antenatal depression indicated that only childhood sexual abuse was a significant predictor when controlling for other ACEs indices (Chung et al., 2008). In addition, childhood sexual abuse has been uniquely associated with prenatal depressive symptoms, even when controlling for verbal and physical abuse and negative life events (Benedict et al., 1999). Childhood maltreatment, as compared to household dysfunction, may be especially predictive of perinatal depressive symptoms, as these experiences may be more likely to activate negative representations and interfere with coping with changes associated with pregnancy and the onset of role as caregiver (Slade, Cohen, Sadler, & Miller, 2009). Previous contradictions in the literature regarding relations between ACEs and perinatal depression may be clarified by distinguishing between associations with childhood maltreatment and household dysfunction.
Maternal ACEs and Reproductive Birth and Infant Outcomes
Maternal ACEs have been associated with a range of adverse reproductive birth outcomes. For example, several studies have linked maternal risk factors, including social disadvantage and childhood trauma, with infant birth weight (Gavin, Hill, Hawkins, & Maas, 2011). Birth weight and gestational age positively predict a range of adaptive developmental outcomes during infancy and across the life span (e.g., Barker, Eriksson, Forsen, & Osmond, 2002). Therefore, it is critical to identify specific pathways through which maternal ACEs relates to infant birth outcomes to determine factors that characterize women at the greatest risk for poor reproductive health. In order to isolate the unique influence of ACEs on adverse birth outcomes, it is important to incorporate other known risk factors into analyses, such as African American race (e.g., Stancil, Hertz-Picciotto, Schramm, & Watt-Morse, 2000).
Maternal age at first pregnancy is associated with maternal ACEs and with adverse pregnancy indicators, suggesting that this factor is relevant to evaluate as a mediator of associations between ACEs and birth outcomes. For example, Hillis and colleagues (2004) reported a strong dose–response link between maternal ACEs and the risk of adolescent pregnancy wherein the prevalence of teen pregnancy increased directly with the number of childhood traumatic experiences endorsed. This is consistent with other research documenting associations between indicators of childhood maltreatment and early pregnancy during adolescence (Noll, Shenk, & Putnam, 2009). Younger age at first pregnancy has been linked with adverse pregnancy outcomes including fetal death, prematurity, and low birth weight (Fraser, Brockert, & Ward, 1995; Hillis et al., 2004). Despite this empirical evidence, no prior study to our knowledge has empirically examined the indirect effect of ACEs on reproductive birth outcomes through maternal age at first pregnancy.
Beyond outcomes at birth, it is essential to examine the intergenerational influence of maternal ACEs on infant postnatal functioning. In particular, little is known regarding pathways that may mediate associations between maternal ACEs history and infant development. Several studies suggest that maternal childhood abuse history may be directly associated with poor infant socioemotional outcomes, such as insecure attachment (Berthelot et al., 2015). Alternatively, maternal ACEs may be indirectly related to infant functioning via maternal depressive symptoms. Maternal psychological stress during pregnancy, including stress, anxiety, and depression, is strongly associated with infant development across multiple domains of functioning (see Kingston, Tough, & Whitfield, 2012, for review). Maternal perinatal depressive symptoms, in particular, have been associated with child socioemotional difficulties (see Field, 2011, for review), and these associations between depression and child psychopathology have been shown to be strongest among the youngest children (see Goodman et al., 2011, for meta-analysis). Therefore, the current study considers both direct and indirect associations between ACEs and infant socioemotional functioning.
The Present Study
The overall aim of the present investigation was to prospectively evaluate associations among maternal ACEs, including childhood maltreatment and household dysfunction, with perinatal depressive symptoms, reproductive outcomes, and infant socioemotional functioning. Our investigation was guided by three hypotheses. First, we anticipated that maternal ACEs would predict higher levels of pre- and postnatal depressive symptoms as well as less change in depressive symptoms across the perinatal period. Moreover, we anticipated that these associations would be stronger for experiences of childhood maltreatment than household dysfunction. Second, we hypothesized that maternal ACEs would predict poorer reproductive outcomes, including lower infant birth weight and premature delivery (e.g., younger gestational age). Further, we anticipated an indirect effect wherein this association was mediated by maternal age at first pregnancy. Third, we hypothesized that maternal ACEs would also predict poorer infant socioemotional outcomes and that this association would be mediated by maternal age at first pregnancy and infant birth weight, a known risk factor for poor infant development.
Method
Participants
Participants were 398 pregnant women whose ages ranged between 15 and 46 years (M = 24.76, SD = 5.43) at prenatal assessment. The majority of the sample was never married and racially diverse (see Table 1). Participants were recruited from local Women, Infants, and Children (WIC) offices in a medium-sized Midwestern city and had to be pregnant in order to be included in this investigation. All pregnant women who were receiving or seeking services from the WIC offices were invited to participate. Assessments were administered at two time points: (1) prenatal appointment (M = 4.84, SD = 2.14 months before due date) and (2) a 6-month postnatal follow-up (M = 6.76, SD = 0.95 months after birth).
Demographic Characteristics as a Percentage of the Sample.
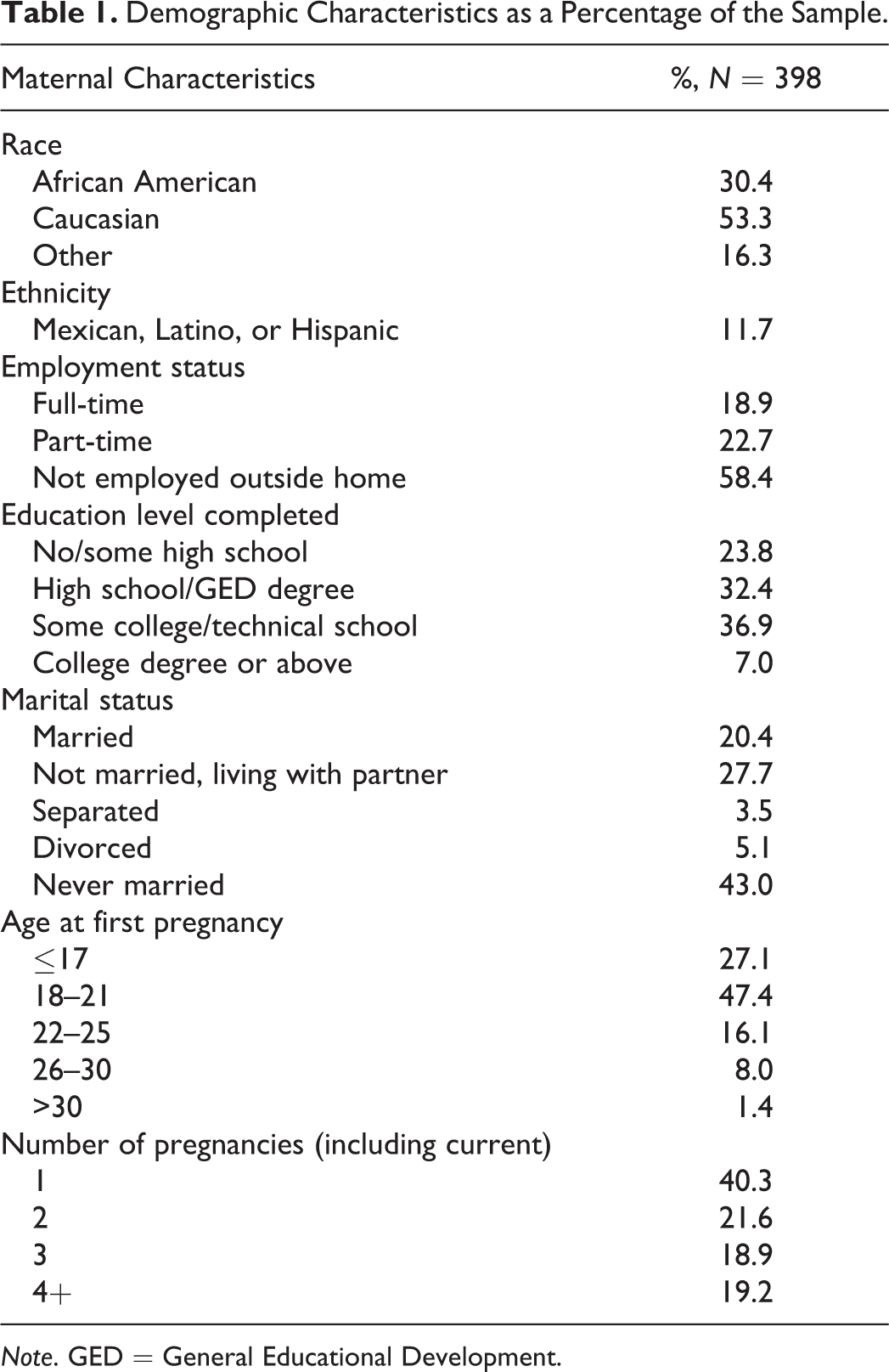
Note. GED = General Educational Development.
Procedure
WIC office staff administered assessment measures to participants during a regularly scheduled prenatal appointment. Within 4 weeks of the mothers’ due dates, research assistants obtained birth outcome data via telephone or during mothers’ first appointments following birth. Mothers reported on their expected due date and actual date of birth, and outcome data, including birth weight and date of delivery, was verified with hospital records by WIC office staff. Three hundred and fifteen women provided birth outcomes, representing 79% of the original sample. Subsequently, mothers completed assessment measures at a 6-month follow-up appointment at the WIC office with research staff. Two hundred and nine women returned for the 6-month follow-up appointment, representing 52.5% of the original sample. This attrition rate (47.5%) is comparable with rates reported in other work with high-risk community families (e.g., Cicchetti, Rogosch, & Toth, 2006; Nuttall, Valentino, & Borkowski, 2012).
Measures
Family health history questionnaire (FHHQ), female version
The FHHQ was administered at the prenatal assessment to assess maternal ACEs, demographics, and a broader range of health practices. Developed by the Centers for Disease Control and Prevention, the FHHQ has been used extensively in research with high-risk, low-income samples and in seminal studies investigating maternal ACEs (e.g., Felitti et al., 1998). Information obtained included demographic statistics, information concerning sexual practices and pregnancy history (e.g., number of sexual partners, age at first pregnancy), and information regarding traumas and/or life stressors participants may have experienced as a child. The childhood maltreatment and household dysfunction variables were calculated as the sum of dichotomous indicators of traumatic experiences. The five indicators of this variable included (1) sexual abuse (e.g., fondling, forced touching, and/or attempted or forced sexual intercourse), (2) physical abuse (e.g., ever receiving bruises/marks from being hit, or often being pushed, grabbed, shoved, slapped, etc.), (3) emotional abuse (e.g., being threatened with harm or often receiving hurtful/insulting insults or put-downs), (4) physical neglect (e.g., not having clean clothes or enough to eat or not having caretakers to protect or take care of family), and (5) emotional neglect (e.g., no one in family to support emotional needs for love, support, etc.). Consistent with Felitti and colleagues (1998), the five indicators of childhood household dysfunction were (1) household substance use (e.g., living with someone who used drugs and/or had difficulty with alcohol), (2) parental separation or divorce, (3) family member imprisoned, (4) family member with mental illness, or (5) domestic violence (e.g., physical, violent conflict toward mother). Thus, scores for both childhood maltreatment and household dysfunction ranged from 0 to 5.
Beck Depression Inventory (BDI-II)
The BDI-II (Beck, Steer, & Brown, 1996) was administered at two time points (prenatal and 6 months) to assess maternal depressive symptoms. The measure has excellent, well-established psychometric properties and contains 21 items scored on a scale from 0 to 3. Total scores range from 0 to 63, with higher scores indicating more severe depressive symptoms. In addition to total scores at each time point, a difference score variable was computed (prenatal BDI score − 6-month BDI score) to index the magnitude of reduction in depressive symptoms across this time period.
Ages and stages questionnaire-socioemotional (ASQ-SE)
The ASQ-SE was administered at the 6-month time point to assess infant socioemotional development (Squires, Bricker, & Twombly, 2002). The ASQ-SE is a developmental screening tool used to identify developmental status in the areas of social and emotional functioning among children as young as 4 months of age. Mothers endorsed and rated the frequency of certain behaviors (e.g., smiling, ability to calm down, trouble feeding, and crying) on a scale from 1 (most of the time) to 3 (never or rarely). Items were summed to yield an overall measure of developmental status. Higher scores indicate higher levels of maladaptive symptomatology and are indicative of risk. The ASQ-SE has been shown to be reliable and has established predictive validity to screen for social and emotional problems in young children (Squires, Bricker, Heo, & Twombly, 2001).
Results
Descriptive Data and Preliminary Analyses
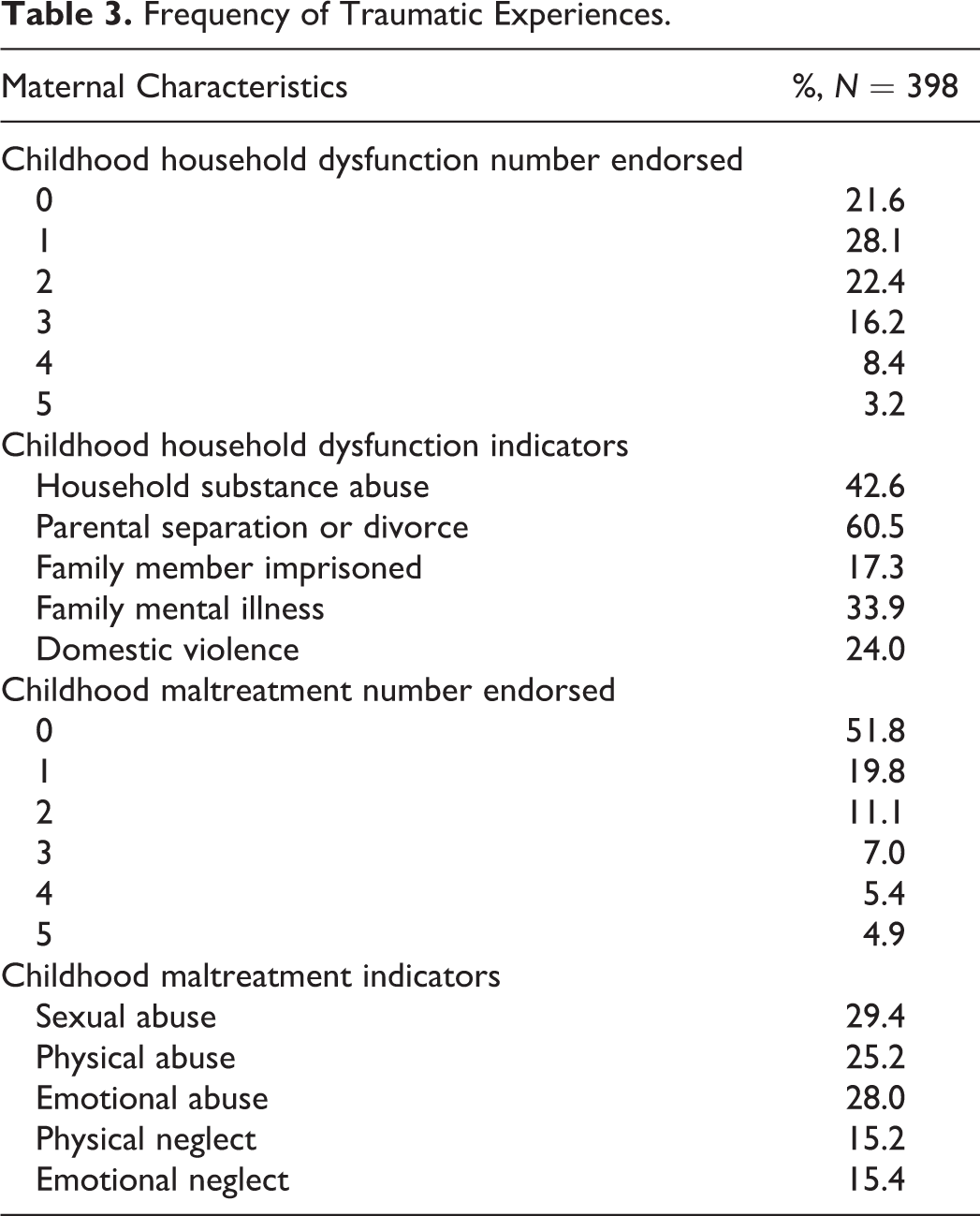
All variables were examined for normality and square root transformed in the case of significant skewness. Observed descriptive statistics, including the amount of valid, nonmissing data for each variable, are presented in Table 2. Missing data at the item level were handled via list-wise deletion, and subsequently whole variables were imputed using full information maximum likelihood (FIML) estimation for substantive analyses. The FIML estimation has been shown to be superior to other methods of estimation when there is missing data (Enders & Bandalos, 2001). Although the average level of depressive symptoms fell within subclinical levels, 26% of the sample endorsed mild to severe symptoms and 25% of the sample endorsed a history of seeking services from a therapist, psychiatrist, or psychologist. Overall, the sample endorsed a high percentage of childhood traumatic experiences (Table 3). Given the attrition of a significant portion of the sample at the 6-month time point, t-test analyses were conducted to examine whether there were significant differences on demographic or primary study variables among those who returned for the 6-month time point versus those who did not. No significant group differences were detected for any of the demographic variables (p values ranged from .14 to .97) nor for the primary study variables (p values ranged from .24 to .86).
Means and SDs of Primary Study Variables.
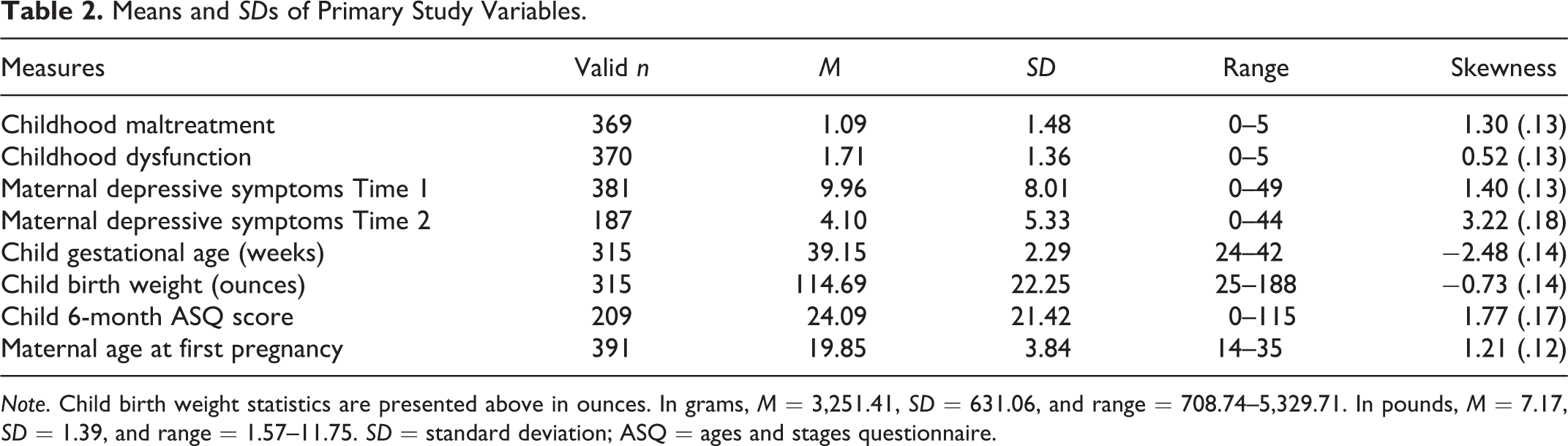
Note. Child birth weight statistics are presented above in ounces. In grams, M = 3,251.41, SD = 631.06, and range = 708.74–5,329.71. In pounds, M = 7.17, SD = 1.39, and range = 1.57–11.75. SD = standard deviation; ASQ = ages and stages questionnaire.
Frequency of Traumatic Experiences.
Correlations among the primary study variables are presented in Table 4. The childhood household dysfunction and maltreatment variables were significantly correlated with one another but demonstrated different patterns of relations with other study variables. For example, both childhood household dysfunction and maltreatment were significantly correlated with prenatal depressive symptoms, whereas only childhood maltreatment remained significantly correlated with maternal postnatal depressive symptoms at the 6-month time point. Furthermore, household dysfunction, but not childhood maltreatment, was significantly negatively correlated with maternal age at first pregnancy. In contrast, childhood maltreatment, but not household dysfunction, was significantly correlated with infant socioemotional functioning at 6 months. Child gestational age was not significantly related to any of the primary predictor variables, perhaps due to restricted range, and was therefore not considered in further analyses. Birth weight was positively correlated with maternal age at first pregnancy, and negatively correlated with infant socioemotional symptoms. Regarding covariates, maternal age at birth was significantly related to maternal age at first pregnancy and infant socioemotional symptoms. Moreover, African American race was significantly negatively related to infant birth weight. Therefore, both of these variables were included as covariates in substantive analyses that considered birth weight and/or infant socioemotional symptoms as outcomes.
Correlations Among Primary Study Variables.
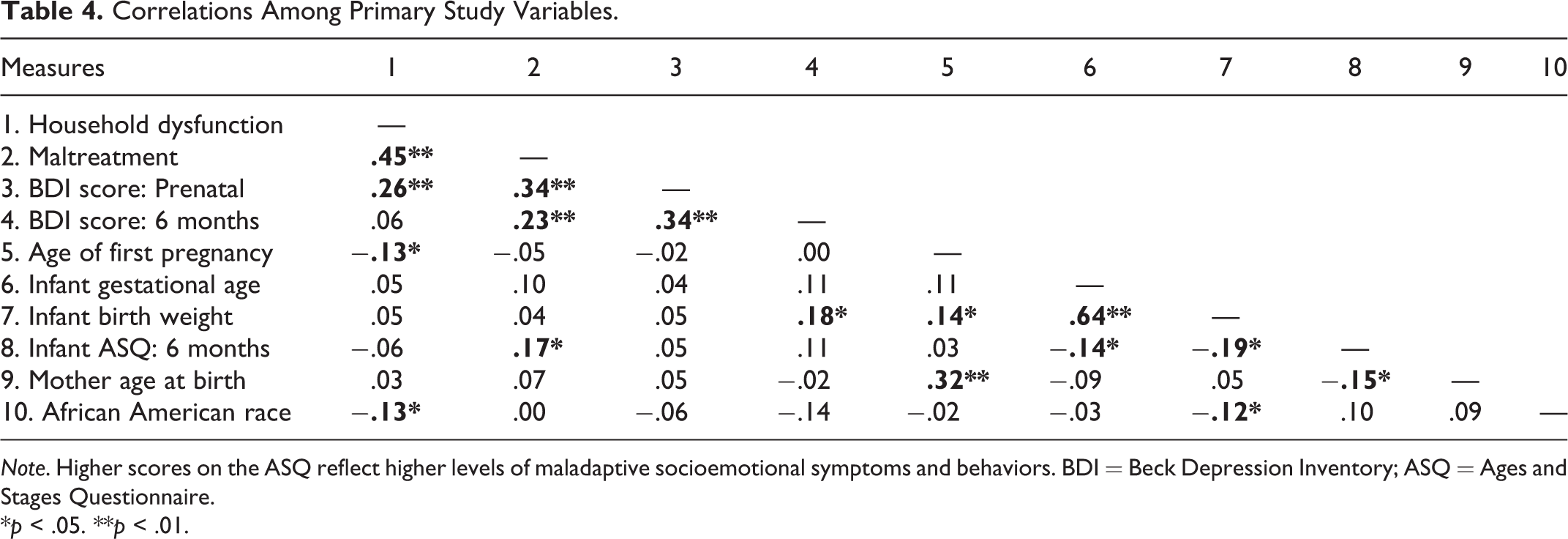
Note. Higher scores on the ASQ reflect higher levels of maladaptive socioemotional symptoms and behaviors. BDI = Beck Depression Inventory; ASQ = Ages and Stages Questionnaire.
*p < .05. **p < .01.
Main Analyses
Substantive analyses were conducted in Mplus Version 7.1 (Muthen & Muthen, 1998–2013) using the full sample (N = 398) with missing data handled via FIML. Saturated models, which provide full descriptions of the data, evaluate all paths among variables, and therefore have 0 degrees of freedom and χ2 values of 0, were utilized to evaluate the primary hypotheses. Regarding Hypothesis 1, correlational analysis yielded significant positive associations between both household dysfunction and maltreatment with prenatal depressive symptoms. However, only childhood maltreatment remained significantly positively correlated with maternal postnatal depressive symptoms at 6 months. To further examine the relative contribution of each variable to the prediction of depressive symptoms, parallel regression analyses were conducted.
First, prenatal depressive symptoms were regressed on both childhood household dysfunction and childhood maltreatment (see Table 5). Both variables significantly predicted higher levels of maternal depressive symptoms, although childhood maltreatment was a more highly significant predictor, β = .29, p < .001. This model was saturated and explained a significant portion of the variance in prenatal depressive symptoms, R 2 = .13, p < .001. Second, postnatal depressive symptoms were regressed on both childhood household dysfunction and childhood maltreatment, controlling for initial levels of prenatal depressive symptoms. Childhood maltreatment, but not household dysfunction, remained a significant predictor of maternal postnatal depressive symptoms, β = .23, p < .01. This model was saturated and explained a significant portion of the variance in depressive symptoms at 6 months, R 2 = .16, p < .01. Third, to consider whether maternal trauma history related to maternal change in depressive symptoms from the prenatal to the 6-month time point, a regression was conducted on the change score variable. Controlling for baseline levels of maternal depressive symptoms, only childhood maltreatment was significantly associated with a smaller magnitude of reduction in depressive symptoms, β = −.20, p < .01. This model was saturated and also explained a significant portion of the variance in the difference score, R 2 = .37, p < .01 (see Table 5).
Predictors of Depressive Symptoms Variables.

Note. These analyses were conducted on the full sample (N = 398), with whole variables imputed via full information maximum likelihood estimation. BDI = Beck Depression Inventory; b = unstandardized estimate; β = standardized estimate; SE = standard error; prenatal = BDI scores at initial time point; postnatal = BDI scores at 6-month time point; change score = initial BDI score − BDI score at 6 months.
*p < .05. **p < .01. ***p < .001.
To test our second and third hypotheses regarding the associations among maternal trauma history and depressive symptoms with maternal reproductive outcomes (birth weight) and infant socioemotional symptoms, structural equation modeling was utilized to examine pathways among these variables (see Figure 1). In particular, we were interested in whether maternal age at first pregnancy would mediate indirect effects between maternal trauma history and infant outcomes. We implemented the nonparametric, bias-corrected bootstrap method recommended by MacKinnon, Lockwood, and Williams (2004), using 1,000 resamples to construct unbiased 95% confidence intervals around the product coefficients of the indirect effects of interest. Given the lack of associations between depressive symptoms at either time point with any of the proposed mediator or outcome variables in preliminary analyses, only the depressive symptoms change score was considered in the model as a predictor or mediator of associations between trauma history and infant socioemotional outcomes. Maternal age at birth, African American race, and prenatal depressive symptoms were included as covariates in the model. The model was saturated. Unstandardized coefficient values are presented below for path estimates and indirect effects, whereas standardized coefficients are presented on the path diagram in Figure 1. Maternal age at birth was a significant covariate on infant socioemotional functioning (b = −.64, SE = .29, p < .05) and on maternal age at first pregnancy (b = .26, SE = .05, p < .001). African American race was a significant covariate on birth weight (b = −5.52, SE = .04, p < .05). Maternal prenatal depressive symptoms was a significant covariate on the depressive symptoms change score (b = .69, SE = .08, p < .001). Including prenatal depressive symptoms, instead of the change score, as a predictor rather than a covariate in this model did not change results and no pathways utilizing depressive symptoms were significant.
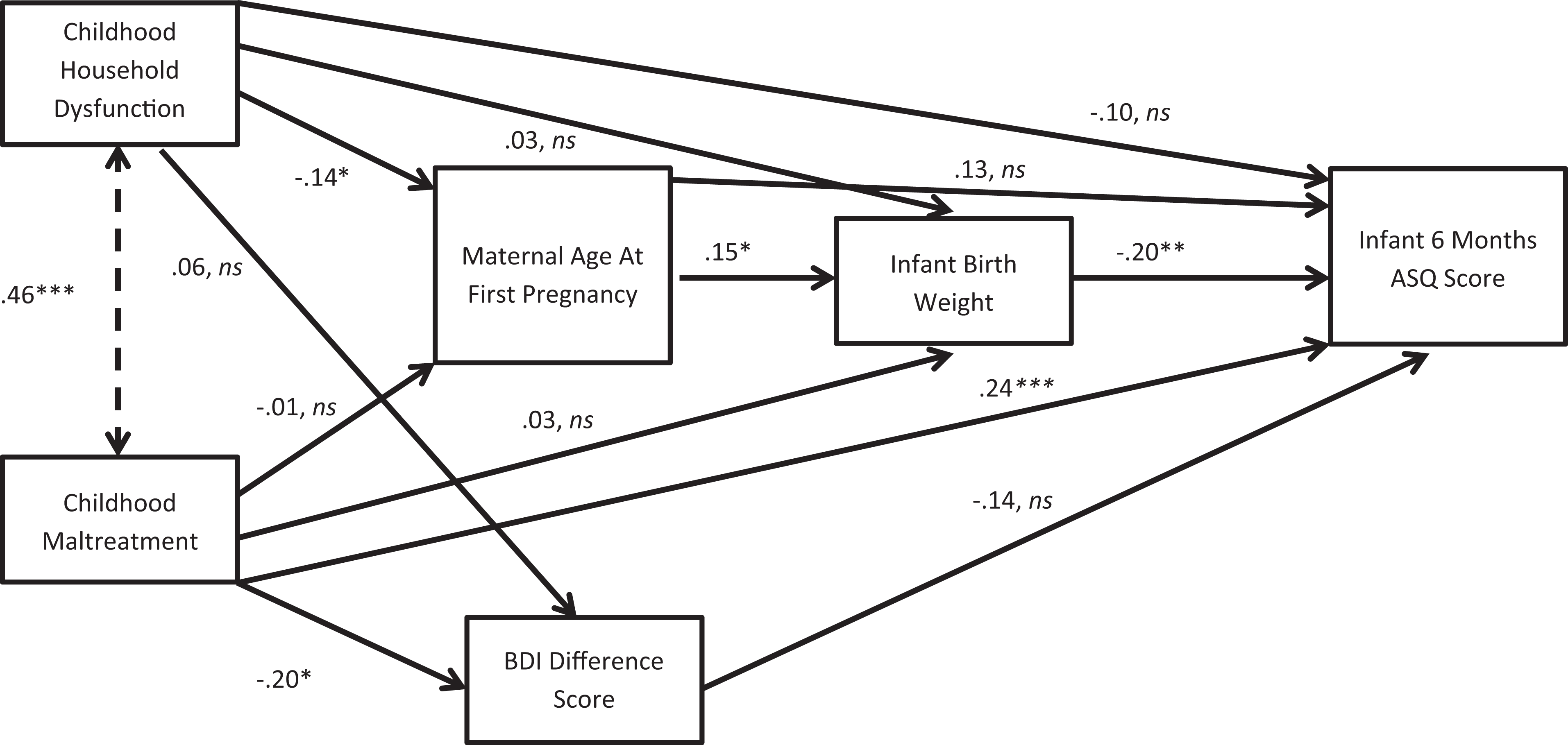
Mediation model. This model was conducted on the full sample (N = 398), with whole variables imputed via full information maximum likelihood estimation. Standardized path coefficients are reported. Controlling for maternal age at birth, African American race, and prenatal depressive symptoms, results indicate (1) a significant indirect effect from household dysfunction to infant ASQ score through maternal age at first pregnancy and infant birth weight and (2) a significant direct effect from childhood maltreatment to infant ASQ score. Influence of control variables is omitted from the diagram for ease of interpretation. *p < .05. **p < .01. ***p < .001. ns = p > .05. ASQ = Ages and Stages Questionnaire, wherein higher scores reflect higher levels of maladaptive socioemotional symptoms.
Childhood maltreatment was significantly associated with infant socioemotional functioning (b = .64, SE = .18, p < .001) and the direct effect was estimated to lie between .292 and .996 with 95% confidence interval. This confidence interval does not contain 0; therefore, the direct effect is significant and demonstrates that maternal histories of childhood maltreatment including abuse and neglect predicted higher levels of maladaptive infant socioemotional symptoms 6 months after birth. No significant indirect effects between childhood maltreatment and infant socioemotional symptoms were detected.
Childhood household dysfunction was not directly associated with infant socioemotional functioning (b = −.18, SE = .12, p > .05). However, childhood household dysfunction was significantly negatively associated with maternal age at first pregnancy (b = −.04, SE = .02, p < .05), and maternal age at first pregnancy was positively associated with infant birth weight (b = 7.88, SE = 3.43, p < .05). In turn, infant birth weight was negatively associated with maladaptive socioemotional symptoms (b = −.02, SE = .01, p < .01). The indirect effect from childhood household dysfunction to infant socioemotional symptoms through maternal age at first pregnancy and infant birth weight was estimated to lie between .001 and .025 with 95% confidence interval. As this interval does not contain 0, the indirect effect was significant and demonstrated that childhood household dysfunction predicted lower maternal age at first pregnancy, which in turn predicted lower infant birth weight. Lower infant birth weight was associated with a higher level of maladaptive infant socioemotional symptoms at 6 months.
In the same model, although there was a significant association between childhood maltreatment and the depressive symptoms change score (b = −.38, SE = .15, p < .01), there was no significant association between the change score and infant socioemotional symptoms (b = −.10, SE = .10, p > .05). The direct effect between change in depressive symptoms and infant functioning was estimated to lie between −.294 and .122 with 95% confidence interval. Because 0 lies within this confidence interval, there was no association between change in maternal depressive symptoms and infant socioemotional functioning.
Discussion
Overall, the results of the current investigation support the intergenerational influence of maternal trauma history on reproduction-related outcomes including maternal depressive symptoms at the time of pregnancy, birth weight, and infant socioemotional symptoms at 6 months postpartum. The present findings advance the literature in three primary ways. First, maternal experiences of maltreatment during childhood (1) predicted higher levels of prenatal and postnatal depressive symptoms and (2) were associated with a smaller reduction in depressive symptoms across the perinatal period. Second, maternal experiences of childhood household dysfunction were indirectly associated with higher levels of infant maladaptive socioemotional symptoms through maternal age at first pregnancy and infant birth weight. Third, maternal childhood maltreatment was directly associated with higher levels of maladaptive infant socioemotional symptoms. Results from this prospective study thereby extend the extant literature by documenting unique influences of childhood maltreatment and household dysfunction on maternal perinatal depressive symptoms and subsequent child functioning.
Maternal childhood maltreatment experiences including abuse and neglect were associated with higher levels of depressive symptoms at the pre- and postnatal time point and further predicted a smaller reduction in depressive symptoms across this period. Thus, women with more childhood maltreatment may be particularly vulnerable to higher levels of depressive symptoms that are more persistent. These findings are consistent with extant research supporting an association between abuse history and perinatal depression (Alvarez-Segura et al., 2014) and significantly extend prior work by demonstrating that childhood maltreatment prospectively predicts both levels of and change in depressive symptoms across the perinatal period.
Broader childhood household dysfunction predicted maternal prenatal depressive symptoms, although this association was weaker than the link between childhood maltreatment and prenatal depression. Moreover, childhood household dysfunction did not significantly predict postnatal nor change in depressive symptoms. This is consistent with prior work demonstrating that the number of violent but not nonviolent traumas predicted perinatal depressive symptoms (Stevens et al., 2002) and that indices of childhood maltreatment, in particular, predicted more persistent and severe levels of depressive symptoms (Benedict et al., 1999). Compared to household dysfunction, which includes indices of broader family stress (e.g., divorce), experiences of maltreatment may be more strongly related to perinatal depressive symptoms, because abuse and neglect may activate negative maternal representations that are particularly salient during and after pregnancy (Alvarez-Segura et al., 2014). Differentiating childhood maltreatment from broader household dysfunction may therefore clarify equivocal findings regarding the association between ACEs and maternal depressive symptoms.
Regarding reproductive and infant outcomes, childhood household dysfunction was indirectly related to child socioemotional symptoms at 6 months via maternal age at first pregnancy and birth weight. In particular, mothers with more childhood household dysfunction had a significantly younger age at first pregnancy, controlling for age at current birth. In turn, younger age at first pregnancy predicted lower birth weight, which was associated with higher levels of maladaptive socioemotional symptoms. This finding significantly extends the literatures documenting (1) associations between trauma history and early first pregnancy and (2) links between young maternal age and adverse reproductive outcomes by demonstrating that maternal age at first pregnancy mediates an indirect association between maternal childhood experiences and subsequent child functioning in the next generation. The association between ACEs and early pregnancy, as well as other high-risk health behaviors, may represent attempts to achieve interpersonal closeness that was lacking in early environments characterized by household dysfunction (Hillis et al., 2004), although lack of supervision or substance abuse among these families may also be contributing factors. The link between ACEs and risky health behaviors may be one manifestation of broader social disadvantage including indices of sociodemographic risk, such as poor access to contraception and health care, higher unemployment, and lower education (Smith, 1996). However, other work has demonstrated a unique role of maltreatment beyond the effects of socioeconomic risk (Garwood, Gerassi, Jonson-Reid, Plax, & Drake, 2015). Future work is needed to empirically evaluate these accounts.
Given that only 40% of mothers in this study were in their first pregnancy, the finding that age at first pregnancy is associated with birth weight, even when controlling for current maternal age, suggests that early age at first pregnancy may have adverse effects on future pregnancies. Prior work has suggested that early reproduction is associated with lasting biological changes (e.g., telomere erosion and oxidative stress) that represent maternal health risks (Shalev & Belsky, 2016); these changes may pose risk for later pregnancies. For example, adolescent pregnancy has been associated with adverse effects on blood lipids which persist several years after delivery (Gunderson et al., 2012) and may be associated with maternal cardiovascular outcomes and newborn health in future pregnancies (Charlton, Tooher, Rye, & Hennessy, 2014). Alternatively, given that young maternal age is associated with risk for rapid-repeat pregnancy (RRP; Rigsby, Macones, & Driscoll, 1998) and that short interpregnancy intervals have been associated with negative birth outcomes (see Conde-Agudelo, Rosas-Bermúdez, & Kafury-Goeta, 2006, for meta-analysis), it is important to examine RRP in relation to the variables of the current investigation.
Childhood maltreatment was directly related to infant socioemotional functioning, such that mothers who endorsed more experiences of abuse and neglect in childhood had children with higher levels of socioemotional symptoms at 6 months. This is consistent with prior studies demonstrating that mothers with abuse and neglect histories are more likely to have infants who evince socioemotional risk across a variety of indices, including insecure attachment (Berthelot et al., 2015). Maternal depressive symptoms were not directly related to birth weight or infant functioning, suggesting that maternal childhood abuse history plays a more direct role in the prediction of intergenerational child functioning. No indirect effects between childhood maltreatment and infant functioning were detected, and maternal depressive symptoms did not mediate this association. This may be explained by the subclinical levels of depressive symptoms overall in this sample. Alternatively, prior work has suggested that maternal depression may have limited power to mediate associations between trauma history, parenting, and child outcomes among low socioeconomic samples characterized by high demographic risk (Zuravin & Fontanella, 1999).
There are limitations to this investigation that should be addressed and considered in future research. First, the current study did not include evaluation of traumatic symptoms nor post-traumatic stress disorder (PTSD) diagnoses. Prior work has documented significant rates of postpartum PTSD, ranging from 3.1% in community samples to 15.7% in at-risk samples (see Grekin & O’Hara, 2014, for meta-analysis). Thus, assessment of the influence of trauma symptoms and comorbid PTSD and depression on birth and infant outcomes is a critical direction for future research with important implications for trauma-informed care for pregnant women. Moreover, ACEs were measured via self-report as dichotomous endorsement of whether an individual experienced particular types of childhood trauma. Replicating these findings with objective ratings of legal records of maltreatment, including consideration of the severity, chronicity, and timing of ACEs will be essential.
In addition, the present study involved high attrition, as roughly half of the sample was retained at the 6-month time point. However, there were no significant differences among those attrited versus retained, and longitudinal studies involving high-risk, community samples frequently report high attrition rates that have ranged over 50% (Kingston et al., 2012). Moreover, self-reported depressive symptoms were utilized rather than diagnostic depression status. Although the average level of depressive symptoms fell below clinical cutoffs, 26% of the sample endorsed mild to severe symptoms and 25% of the sample endorsed a history of seeking clinical services. Moreover, subclinical levels of depressive symptoms have been related to the variables of interest in the present study and inform our understanding of how both continuous and categorical depression measures relate to trauma history and infant outcomes. Assessment of depressive symptoms and diagnostic status at more time points across the perinatal period would extend knowledge of the longitudinal trajectories of pre- and postnatal depression. Similarly, infant socioemotional symptoms were measured via maternal report; verification with observational measures and inclusion of other indices of development (e.g., cognitive) will advance the understanding of processes promoting infant functioning. Continued longitudinal assessment will enable identification of trajectories toward adaptation versus maladaptation across early childhood.
The current findings have significant clinical implications. First, future work should consider maternal ACEs in relation to the prevention of perinatal depression or effectiveness of treatment (see Sockol, Epperson, & Barber, 2011, for review). Second, psychoeducational programs have been successfully implemented with pregnant women, including young mothers and those with significant ACEs, to enhance mental health and pregnancy outcomes (e.g., Seng et al., 2011). These programs may incorporate content regarding prevention of risks associated with young maternal age at first pregnancy or by targeting implementation among young mothers. Intervention research at multiple levels of analysis will inform knowledge of pathways toward risk and resilience among mothers with ACEs and their children.
Footnotes
Acknowledgment
We thank Sue Taylor, MS, Jamie Reinebold, MSW, and Jeanne Mattei, MSW, for their invaluable assistance as collaborators on this project and are grateful to the mothers and their children who participated.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Rodney F. Ganey, PhD Collaborative Community-Based Mini-Grant from the Center for Social Concerns at the University of Notre Dame awarded to Kristin Valentino.