
Abstract
We conducted a community-based randomized control trial with intent-to-treat analysis on Promoting First Relationships® (PFR), a 10-week home visiting program. The study included 247 families with 10- to 24-month-old children who had a recent, open child protective services investigation of child maltreatment. Families were randomly assigned to receive either the 10-week home visiting PFR service or a telephone-based, three-call resource and referral (R&R) service. Across postintervention time points, parents in the PFR condition scored higher than families in the R&R condition in parent understanding of toddlers’ social emotional needs (d = .35) and observed parental sensitivity (d = .20). Children in the PFR condition scored lower than children in the comparison condition on an observational measure of atypical affective communication (d = .19) and were less likely than children in the comparison group to be placed into foster care through 1-year postintervention (6% vs. 13%, p = .042). No significant differences were found on measures of parenting stress or child social–emotional competence, behavior problems, or secure base behavior. Overall, the results show support for the promise of PFR as an intervention for enhancing parent sensitivity and preventing child removals for families in the child welfare system.
Keywords
Children aged birth to 3 years make up one third of cases that come to the attention of child welfare services (CWS) in the United States, a rate higher than any other age-group (U.S. Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau, 2015). Infants and toddlers are vulnerable to stressful experiences, especially maltreatment. Early life adversities affect later life morbidity and early mortality (Shonkoff et al., 2012). Maltreated children who become clients in CWS experience pervasive adversity and chronic stress that produce not only short-term mental and physical health problems, but also long-term health disparities and inequalities (Danese & McEwen, 2012; Jaffee & Christian, 2014; Shonkoff, Boyce, & McEwen, 2009).
The primary mechanism for intervention with child maltreatment cases is through state-supported CWS. Families reported for allegations of maltreatment to Child Protective Services (CPS) face a range of outcomes including closed cases with no services, court-mandated family services, or removal of children from the home and placement in foster care. Removal, however, may compound the adverse consequences of prior maltreatment (Newton, Litrownik, & Landsverk, 2000; Rubin, O’Reilly, Luan, & Localio, 2007). Providing parental services to CWS families to prevent removal is, as Barth et al. (2005) note, clearly a linchpin of governmental responsibility … to provide, preserve, maintain, or reunify families …. Effective CWS must rely on effective parent training and support—as this is the primary intervention that child welfare agencies provide in trying to preserve or reunify families. (p. 353)
Promoting First Relationships® (PFR)
PFR (Kelly, Sandoval, Zuckerman, & Buehlman, 2003, 2008) is a 10-week relationship- and strengths-based home visiting service that aims to help families facing adversity, including those involved in CWS. PFR seeks to increase caregivers’ awareness of their children’s social and emotional needs, including their need for a sense of safety and security, as well as increasing caregivers’ understanding of their own needs as parents. Better recognition and response to the child’s needs support the development of a more secure attachment (Bowlby, 1969, 1982). Infants rely on the parent as a source of comfort when fearful or distressed and as a base from which to explore their world. From this, they develop a sense of “felt security” that attachment figures are trustworthy and responsive.
PFR service providers are trained to focus on the relationship between the parent and child and become keen observers of this dyadic dance or the lack thereof. Providers employ these observational skills using video-based feedback with parents. The parent and child are recorded playing together 5 times during the 10-week PFR program. The PFR provider will then review a recorded play session with the parent, typically the week following the date on which the session was recorded. The provider and parent reflect on the recorded interactions, noting what the child is doing in relation to the caregiver’s behavior and what the caregiver is doing in response to the child.
PFR service providers are also trained to interact with families in a way that does not contribute to a caregiver’s shame, guilt, and/or defensiveness. This model is based on the belief that in order to effectively facilitate change in parenting and to enhance the parent–child relationship, it is essential to first establish a relationship with the parent that enhances the parent’s own feelings of safety and security (Crittenden, 2016; Graybeal, 2007; Larrieu & Zeanah, 2004). Crittenden (2016) has argued that a “bridge” should be created between the maltreating parent and the service provider’s goals of protecting the child and improving parenting. Under conditions of perceived threat, a parent relies on defensive and self-protective strategies, and this can jeopardize a parent’s ability to integrate insights with behaviors and capacities. Threats from social service providers range from the capacity to remove a child from the home to more subtle behaviors such as use of judgmental language, derogatory labels, and actions that humiliate a parent or increase his or her guilt or shame (Crittenden, 2016). Thus, addressing the interactive behavior of service providers, including their use of verbal and nonverbal communication, should be the cornerstone of any intervention serving CWS families.
Promising results in quasi-experimental studies led to the first randomized control trial (RCT) of PFR. This trial was conducted within the CWS system and enrolled foster parents, kin providers, and birth parents caring for toddlers recently placed with or returned to them. Parents in the PFR condition showed postintervention improvements compared to the control group in parent understanding of toddlers’ social–emotional needs, parent report of child competence, and observed parental sensitivity (Spieker, Oxford, Kelly, Nelson, & Fleming, 2012). Permanency outcomes (adoption or guardianship) achieved without any care disruptions were significantly higher in the PFR condition (Spieker, Oxford, & Fleming, 2014). Secondary analysis identified stronger positive effect sizes at 6-month follow-up on the subsample of dyads headed by birth parents relative to the full sample results (Oxford, Marcenko, Fleming, Lohr, & Spieker, 2016).
The Current Study
In this study, we report on the second RCT of PFR, which involved families with 10- to 24-month-old infants and toddlers who had recently been reported to CPS with allegations of child maltreatment. Like its predecessor, this RCT was a “real-world” evaluation that relied on community-based service providers to deliver PFR. Families were recruited through a partnership with Washington State Children’s Administration CPS and then randomized to the experimental or comparison conditions. We hypothesized that PFR, as delivered by community providers, would result in improved parenting and child social and emotional outcomes relative to the comparison condition, in which families received phone-based resource and referral (R&R) services. Further, we hypothesized that those receiving PFR would experience better outcomes within the child welfare system, including a lower likelihood of the child being removed from parental care and placed into foster care.
Method
Participants
The current study looks at the Supporting Parents Program (SPP). With approval from the Washington State Institutional Review Board, the SPP enrolled 247 birth parents with infants and toddlers between January 2011 and January 2014. The flow of participant recruitment, assignment, and completion of assessments is shown in Figure 1.
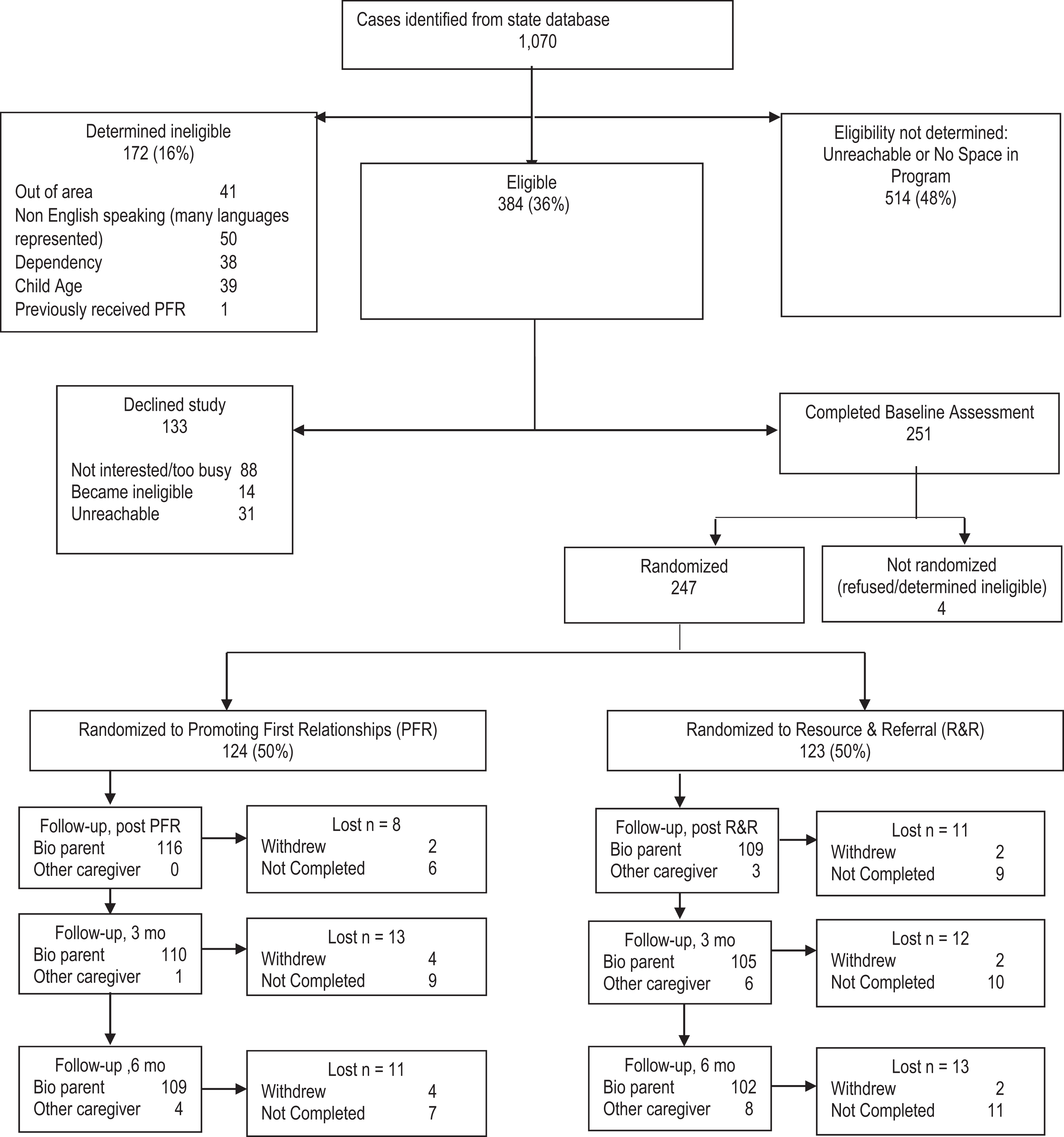
Supporting Parents Program study flowchart.
Eligibility and recruitment
Participants were eligible if they were conversant in English; had housing; and lived in Snohomish, southern Skagit, or northern King County in Washington State. Participants also had to have a child between the ages of 10–24 months and an open case with an allegation of maltreatment of any type recorded in the database of the regional CPS office at least 2 weeks prior. In 31 instances, the identified child in our target age range (10–24 months) was not the identified victim according to CPS reports. A Department of Child and Family Services (DCFS) volunteer, trained for the purpose of the study, scanned the Washington State Department of Social and Health Services (DSHS) database on a monthly basis and created a list of potentially eligible families (N = 1,070). She then went down the list, contacting potential participants and describing the study in detail. If the potential participant was eligible and interested in the study, permission was obtained to forward contact information to the research team. The DCFS volunteer continued contacting potentially eligible families on the list until seven to eight families were enrolled in the study per month. Once the study had reached the monthly enrollment quota, no more families were contacted until the following month. Overall, 514 of the 1,070 potential families (48%) did not have an initial contact, primarily because they did not answer their phones or had disconnected phones and only occasionally because the monthly quota had been reached. Among the 556 families contacted by phone, we found 172 (31%) were not eligible, reflecting the fact that database information was inaccurate or incomplete. Of the 384 eligible families, 251 agreed to an initial in-home research visit. The study research visitor met with families to obtain written consent and conduct the research visit. An additional four families were determined to be ineligible during these visits. For those eligible, the study consent form was read to and discussed with parents to ensure they were aware that participation was voluntary, that the study did not fulfill any family service requirements by DSHS, and that subject incentives were for the research visits only. Study family compensation increased from US$50 to US$100 across the research visits for a total of US$300 for all four assessments.
One parent and one child from each family were the primary participants in the interventions and were assessed at four time points (see Measures and Procedures sections for details). Following the first research visit, families were randomized to receive PFR (n = 124) or the R&R program (n = 123), using a computer randomization program that blocked families based on race and ethnicity. According to DSHS records, the 247 study families were similar to the 823 potential families identified in the DSHS database and not enrolled in terms of race, χ2(5, N = 1,070) = 8.10, p = .15, and Hispanic ethnicity, χ2(2, N = 1,070) = 1.81, p = .40. For the 216 families in which the enrolled child was the alleged victim of maltreatment according to CWS records, the mean number of weeks between initial allegation and enrollment in the research project was 8.17 (SD = 32.46) and did not differ by condition, R&R: M (SD) = 7.38 (33.76); PFR: M (SD) = 8.92 (31.28); t(211) = 0.35, p = .729. Information on demographic and other baseline characteristics is shown by condition in Table 1. Among all the variables listed in Table 1, there were no statistically significant (p < .05) differences by condition.
Baseline Characteristics by Intervention Condition.
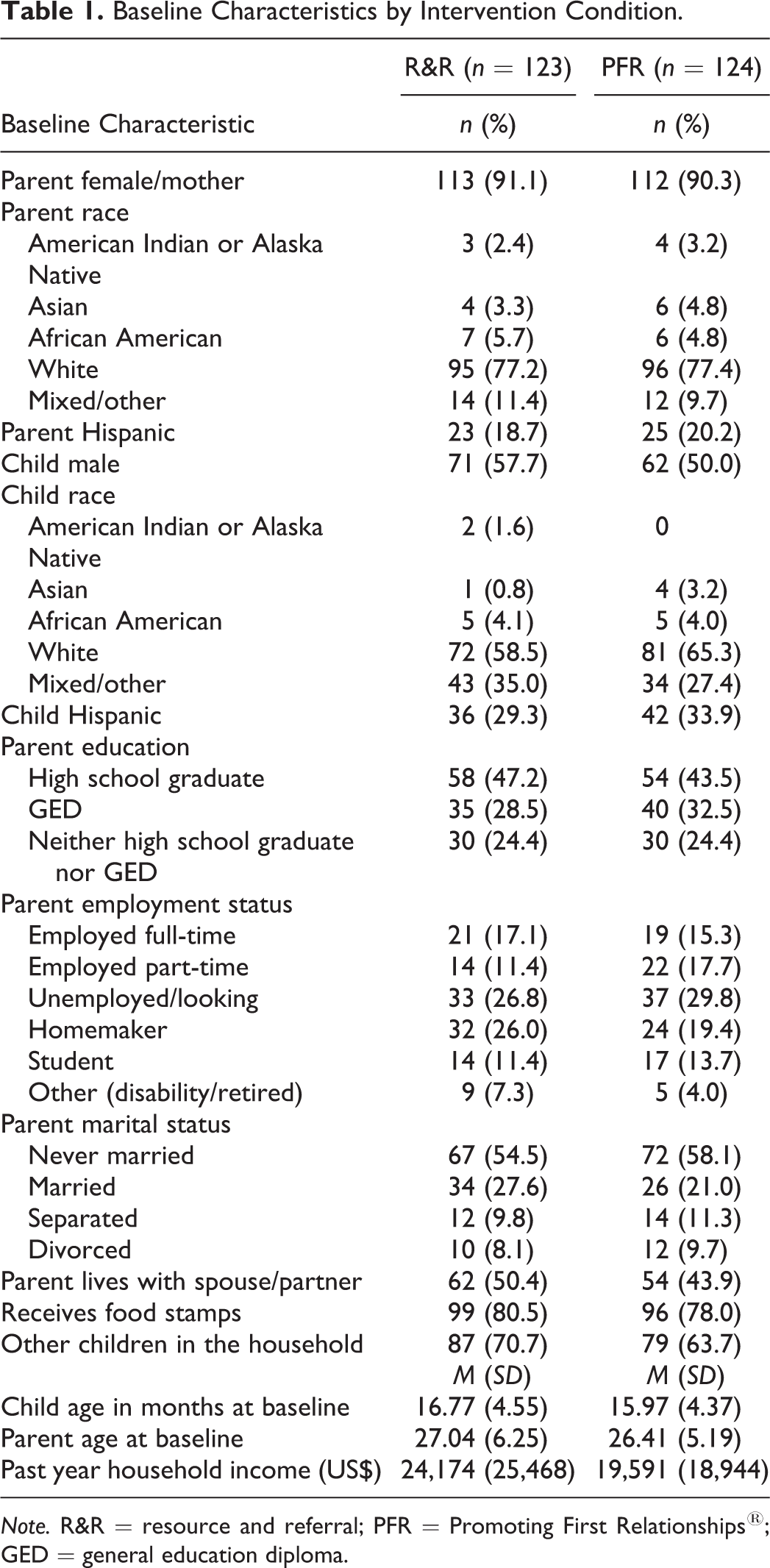
Note. R&R = resource and referral; PFR = Promoting First Relationships®; GED = general education diploma.
PFR Intervention Components
The manualized PFR intervention was delivered by two providers from a community agency. Both providers were female, Caucasian, and had master’s degrees in social work or counseling. The providers completed PFR training over a 5-month period and, after becoming certified, began meeting with study families. Throughout the study, fidelity was monitored by a PFR master trainer (Oxford, Spieker, Lohr, Fleming, Dillon, & Rees, 2016). The providers submitted videotapes of themselves working with the families (one videotaped session for each family on their caseload), which the master trainer used to rate the quality of delivery on a 1- to 5-point scale. If a provider did not maintain fidelity (i.e., received a rating < 4 for a videotaped session), she received additional one-on-one mentoring until her fidelity to PFR was reestablished. The PFR training model also included weekly reflective practice group sessions, facilitated by a PFR consultant, to support providers in their work with vulnerable families which was often stressful.
After completing the PFR program, the families were given a 10-item questionnaire to evaluate their experience with the intervention (satisfaction, effectiveness, overall experience, usefulness, and relevance), the provider (attentive, warm, affirming, and sensitive), and their recommendation of PFR. The response rate was 78.5%, and the internal consistency of the scale was good (α = .77). PFR participants rated PFR very highly (M = 3.9, SD = 0.2; range = 1–4, higher scores = greater satisfaction), and all would recommend the program (Oxford, Spieker, et al., 2016).
R&R Intervention Components
The R&R program was delivered over the phone in three sessions. A social service provider conducted a 30-min needs assessment, mailed a packet of personalized information, and followed up with two 10-min check-in calls. The main needs identified by study families were financial support, education, household items, housing, and parenting support. A standard resource list, developed by the study, was sent to each R&R family containing information on over 150 local services. In addition, the social service provider included an average of six specific resources for each individual family (range = 0–15).
Dosage
Completion rates for the two interventions were high. In the PFR condition, 86% received a full course of 10 sessions. In the R&R condition, 89% had all three telephone sessions. Most of the families were able to begin the interventions: Only 7% of the PFR families and 3% of the R&R families had no intervention sessions. Of those who started the PFR intervention, 7% missed between one and nine sessions, and in R&R, 10% missed one or two sessions. The mean number of weeks required for completion of PFR was monitored and the R&R intervention was timed such that the average time from first to last intervention visit was equivalent, R&R: M (SD) = 14.1 (3.2), range = 7–35; PFR: M (SD) = 14.3 (5.4), range = 5–36; t(213) = 0.23, p = .82.
Measures and Procedures
Infants and their caregivers were assessed in a 2-hr in-home research visits at baseline, immediately after completion of the intervention (i.e., postintervention), and at the 3- and 6-month postintervention follow-ups. Assessments were conducted by study research visitors who had master of social work (MSW) degrees, were kept blind to intervention assignment, and whose offices were not near the PFR or R&R intervention staff. Visits included the following elements: interview questions, self-report questionnaires, videotaped caregiver–child interactions of free play, a teaching task, and a brief separation procedure. Although the mean number of weeks spent completing the intervention did not differ between the conditions, the actual number of weeks between baseline assessment and the postintervention assessment was greater for dyads in the PFR condition, R&R: M (SD) = 16.64 (3.51); PFR: M (SD) = 18.47 (6.82); t(177) = 2.54, p < .05, because it took longer to schedule and complete the first PFR in-home intervention session compared to the first R&R phone session. Time between baseline and postintervention follow-up was thus included as a covariate in analyses. A child who experienced a caregiver change following the intervention completed later assessments with the new caregiver. Over the course of the study, 14 new, nonbirth parent caregivers were enrolled and completed study procedures with the study child in their custody. For the analyses of intervention effects, data for postintervention and follow-up time points come from visits with child–parent dyads that remained intact since baseline (see Figure 1). Analyses examining removals include the full sample of children.
There were few differences between dyads that remained intact and completed follow-up interviews compared to families that were not intact and/or did not complete follow-up interviews. At none of the four follow-up time points were there statistically significant differences by completion status on any of the sociodemographic variables listed in Table 1.
Caregiver outcomes
Understanding of toddlers was measured by the Raising a Baby Scale (RAB; Kelly, Korfmacher, & Buehlman, 2008) at the postintervention and 6-month follow-ups. The RAB is a measure of caregiver knowledge of infant and toddler social–emotional needs and developmentally appropriate expectations. Caregivers rated RAB items on a 4-point scale (strongly agree to strongly disagree; 16 items; αs ranged from .73 to .77). Higher scores indicate greater parental knowledge.
Parent sensitivity was measured at all four time points by a modified total score of the Nursing Child Assessment Teaching Scale (NCATS; Barnard, 1994), a videotaped interaction to assess caregiver sensitivity, stimulation of the child, and emotional responsiveness and contingent interactions between the parent and child. The scale was modified from the original measure to exclude some items that demonstrated low variability. A total score was based on 45 items that covered mutuality (e.g., contingency, gaze, and positive affect), caregiver verbal and nonverbal support of child, and sensitive instruction during the teaching task. Items were scored yes (1) or no (0), and yes scores were summed. Cronbach’s α ranged from .68 to .72, reflecting that the total sensitivity score covers a multidimensional construct. A single, blinded coder was trained to reliability by a certified NCATS instructor and passed regular reliability checks.
Parenting stress was measured by scales selected from the Parenting Stress Index (PSI-3) and the Parenting Stress Index–Short Form (PSI-SF; Abidin, 1995). The Parent–Child Dysfunctional Interaction Scale from the PSI-SF (11 items) and the Parenting Competence Scale from the PSI-3 (11 items) were used. Items were rated on 4-point scales (strongly agree to strongly disagree). Two items measuring parental educational attainment from the original Parenting Competence Scale were omitted due to excessive missing data. Higher scores indicate greater parental stress associated with feelings of incompetence or dysfunctional parent–child interactions (i.e., interactions are not reinforcing or satisfying). αs ranged from .71 to .94 across the two measures and across time points.
Child outcomes
Child social–emotional competence (11 items; αs = .69–.70) and behavior problems (31 items; αs = .77–.79) were measured by the Brief Infant Toddler Social and Emotional Assessment (BITSEA; Briggs-Gowan & Carter, 2002). Descriptions of positive and problematic social–emotional behaviors in the last month were rated on a 3-point scale (not true/rarely, somewhat true/sometimes, and very true/often).
At baseline and again at the 3-month follow-up, blinded research visitors rated the child’s behavior during administration of a standardized developmental test using the Bayley Behavior Rating Scales (BRSs; Bayley, 1993). Seven items in the BRS comprise the Emotion Regulation Scale and capture how well the child adapts to challenging stimuli and frustration (αs = .79–.83). Engagement/exploration consists of 6 items rated for exploratory behavior in the testing situation (αs = .75–.76).
Secure base behavior and atypical, affective communication were measured with the Toddler Attachment Sort-45 (TAS-45; Kirkland, Bimler, Drawneek, McKim, & Schölmerich, 2004). The TAS-45 is based on 39 items from the Attachment Q-Sort (AQS; Waters, 1987), an attachment measure that has been extensively validated (van IJzendoorn, Vereijken, Bakermans-Kranenburg, & Riksen-Walraven, 2004), plus 6 additional items tapping atypical, affective communication. Because we were dissatisfied with the TAS-45 trilemma scoring system used in our previous study (Spieker et al., 2012), in this study, we applied the five-pile sorting procedure that produced good psychometrics for an overall TAS-45 security score in the Early Childhood Longitudinal Study–Birth cohort (ECLS-B; Andreassen, Fletcher, & Park, 2006). Immediately after research home visits, the research visitors sorted cards for 45 descriptive statements of child attachment behavior into five piles representing most like to least like the child. A maximum of 18 cards could be placed in one pile. Item rankings were then used to calculate an overall security score and the orthogonal “D Hotspot” Scale representing atypical affective communication. Four research study visitors were trained over the course of the study to score the TAS-45 by taking into consideration the child’s behavior during home visits. These visits included a brief separation procedure in which the caregiver was instructed to play with the child for a minute, say good-bye, leave the home for 3 min, and then return. The research study visitor did not interact with the child during the separation. To assess reliability across the project, 88 videotaped sessions were coded by pairs of raters. Interrater reliability was r = .75 for security and r = .79 for the D Hotspot Scale. Reliability was monitored and maintained during monthly meetings of the research study visitors and coinvestigator, when videotapes of parent–child interactions were coded and discussed.
Information on allegations of child maltreatment after enrollment in the project and removals from the birth parent home was based on official CWS records obtained in September 2015. For each child in the study, we obtained records of new maltreatment allegations and CWS-initiated removals that occurred between baseline and 12 months after the child’s parent completed the PFR or R&R interventions. For cases where the parent did not start or did not fully complete the intervention, we obtained information on allegations and removals that occurred within 12 months of when the parent would have completed the intervention if the parent had done so on schedule.
Analysis
To assess PFR effects on all parent–report and observational measures, we used models that examined differences based on measures from postintervention time points, adjusting for baseline score on the given measure, age of child at baseline, and months between baseline and postintervention assessment. For measures assessed at only one postintervention time point (i.e., the two Bayley BRSs), we used regression models with the postintervention measurement as the measured, manifest dependent variable. For measures assessed at multiple postintervention time points, mixed models were estimated in which postintervention scores were nested within dyads. The intercept (representing the average score across postintervention time points) was modeled as having a random effect at the dyad level. The intercept in the mixed model was regressed on intervention condition (R&R = 0 and PFR = 1) and covariates. We also ran models that included an effect of time (with loadings of −1, 0, and 1 for the postintervention, 3-month, and 6-month follow-up time points, respectively) and the interaction between time and intervention condition. In none of the models were intervention effects on postintervention slope (i.e., change across the three postintervention time points) statistically significant nor did modeling the slope and slope-by-intervention condition change the estimated effects of intervention on intercepts in terms of direction or significance level. In no models was the variance of the random effect of time statistically significant, suggesting that there was little variability across dyads in linear change across the three time points. Thus, we present below the estimates for simpler models without the time effect. We present both unstandardized intervention effects from these models and standardized effect sizes (d) based on rerunning the models using standardized scores for the outcomes (Lipsey & Wilson, 2001).
Models were estimated using Mplus Version 7.31 (Muthén & Muthén, 1998–2015). Full Information Maximum Likelihood (FIML) estimation allowed for inclusion of all cases, even those with partially missing data, although estimates are primarily informed by data on dyads that stayed intact through follow-up and completed follow-up assessments. A small number of cases (<5) had missing data on some baseline measures and, of intact dyads that completed follow-up assessments, missing data on particular measures were minimal (<2%). FIML estimation makes the assumption that data were missing at random after taking modeled variables into account (Graham, 2009).
To assess intervention effects on allegations and child removals, we used continuous time survival models. These models assess the effect of PFR on the likelihood of an allegation or the child being removed from the home from baseline through 1-year postintervention. For children who were not removed from the home, survival model data were right censored at 1-year postintervention completion, which is approximately 15 months postbaseline (i.e., the date beyond which we did not have CWS records). The survival models included child age at baseline as a covariate.
Results
Means by condition on all continuous measures at all time points are shown in Table 2. Difference of means tests indicate one statistically significant difference at baseline, with R&R dyads receiving higher scores on NCATS parenting sensitivity, t(244) = 2.01, p < .05.
Means and Standard Deviations (SDs) by Experimental Condition at Four Assessment Time Points by Intervention Condition.
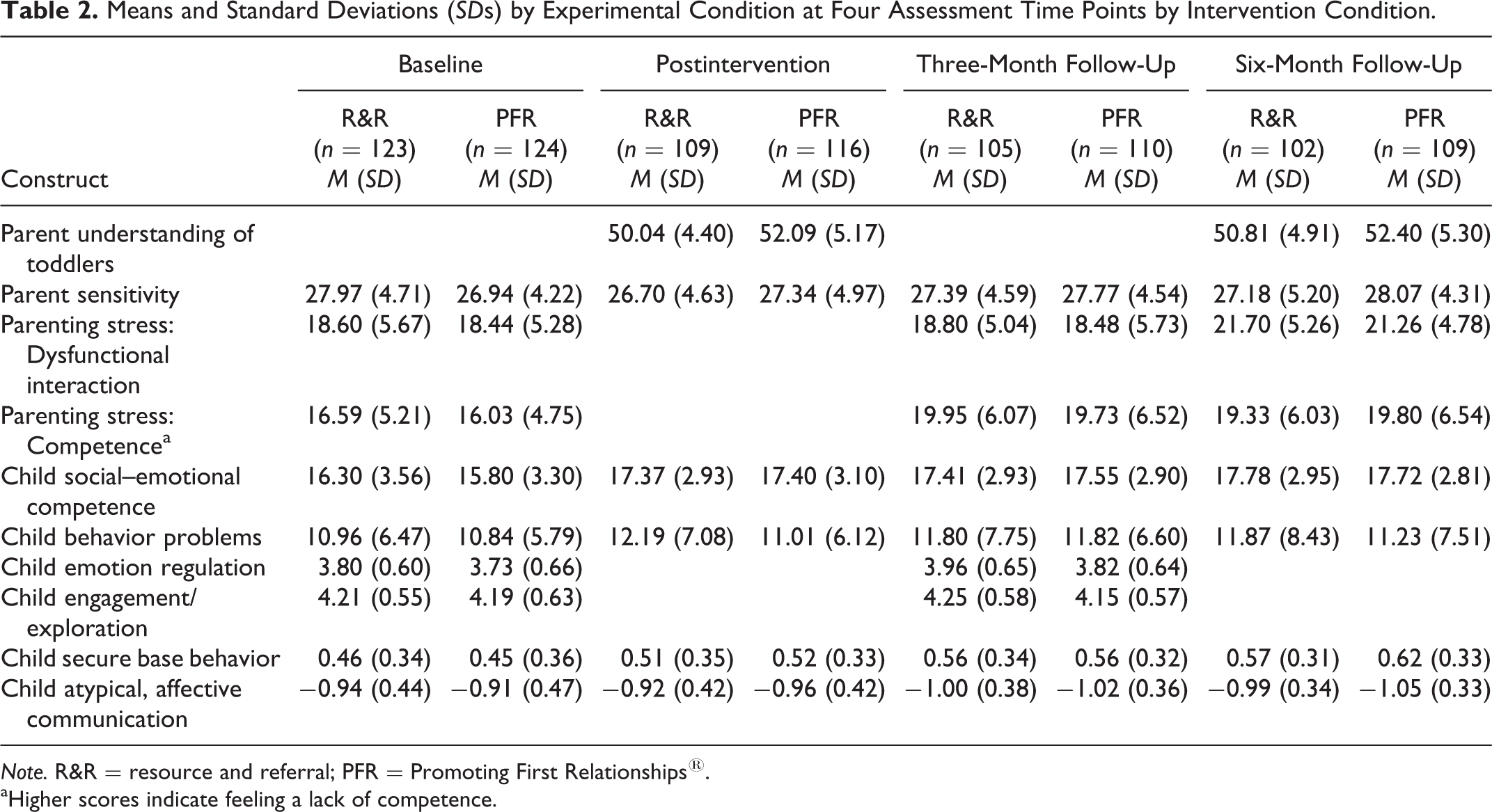
Note. R&R = resource and referral; PFR = Promoting First Relationships®.
aHigher scores indicate feeling a lack of competence.
Estimates of PFR effects on measures postintervention are shown in Table 3. PFR had a positive and statistically significant effect on parent understanding of toddlers (RAB). The effect was equivalent to 0.35 standard deviations on the measure, with parents in the PFR condition scoring higher than parents in the R&R condition. Although parents in the PFR condition scored significantly lower than R&R parents in observed sensitivity at baseline, parents in the PFR condition scored higher at all three postintervention time points. The estimated effect of PFR in the mixed model was equivalent to a fifth of a standard deviation in the outcome. Differences on parent–child interactions and parent feeling of competence as reported on the PSI were not different across condition. Child behavioral outcomes as measured both by the parent–reports and study research visitor observational ratings of emotion–regulation and engagement/exploration on the Bayley BRS, and secure base behavior on the TAS-45, also showed no evidence of PFR effects. Differences on the observation of atypical affective communication were statistically significant, with children in the PFR condition scoring a fifth of a standard deviation lower than children in the R&R condition.
Estimates of Effects of PFR on Postintervention Scores.

Note. A positive d indicates a beneficial effect of PFR. For outcomes measured at two or three postintervention time points, the PFR effect is based on estimates from mixed models with postintervention time points nested within individuals. For outcomes measured at one postintervention time point, PFR is based on estimates from a linear regression model. Effect size (d) based on effect estimate from models using standardized outcome scores. B = effect of PFR on postintervention scores; SE = standard error; d = effect size (effect of PFR in outcome standard deviation units); PFR = Promoting First Relationships®.
aHigher scores indicate feeling a lack of competence.
*p < .05. **p < .01.
Between enrollment and 1-year postintervention, there were new allegations for 36 (29.0%) children in the PFR condition and 42 (31.6%) in the R&R condition. Survival models indicated that chances of a new allegation did not differ significantly by condition, hazard ratio = 1.14, p = .577, and 95% confidence interval (CI) [0.72, 1.79]. Children in the PFR condition were, however, less likely to be removed from a birth parent’s home. Within 1-year postintervention, 7 (5.6%) children in the PFR condition had been removed from the home compared to 16 (13.0%) children in the R&R condition. Survival models indicated that chances of removal from the birth parent home were 2.5 times greater for children in the R&R condition than children in the PFR condition at any given time, hazard ratio = 2.50, p = .043, and 95% CI [1.03, 6.10]. The cumulative difference in removals is shown in Figure 2.

Cumulative proportion removed from birth parent home after baseline by condition.
Discussion
This study is part of an ongoing program of research on the effectiveness of the PFR intervention in improving parent sensitivity, parent knowledge of child development, child secure base behavior, child social and emotional outcomes, and child welfare outcomes. As in our prior RCT of PFR with families in new child welfare placements, we found evidence that PFR increases a caregiver’s knowledge of toddler social emotional needs and, based on an observational instrument, improves caregiver sensitivity to child cues and ability to engage in responsive interactions with children relative to parents in the comparison condition. These findings increase our confidence that PFR has beneficial effects on proximal outcomes of parent knowledge and parent sensitivity.
We also found an important difference in child welfare experiences. All families in the current study had drawn attention from the child welfare system due to allegations of maltreatment, primarily of the child in our study or of a sibling while the infant/toddler in our study was an additional subject of the investigation. By 15 months postbaseline, official child welfare data revealed that 13.0% of the R&R children had been removed from the home compared to 5.6% of the PFR children. This result is promising, indicating that, for some families, a PFR referral following a report of child maltreatment may prevent a future need to remove the child and place him or her into foster care. We are not aware of other studies of home visiting programs that reduced the likelihood of subsequent foster care placement (Dozier et al., 2006; Duggan et al., 2004; Gershater-Molko, Lutzker, & Wesch, 2002; Olds, 2006), and few have shown effectiveness to reduce maltreatment. A recent meta-analysis of 27 studies estimated the effect size to be d = .13 or adjusted effect size d = .02 for home visiting programs to reduce maltreatment (Euser, Alink, Stoltenborgh, Bakermans-Kranenburg, & van IJzendoorn, 2015). Our current findings are consistent with our earlier RCT, in which the PFR group had a higher rate of achieving permanency without separation for toddlers in foster or kinship care (Spieker et al., 2014). These two studies add to the evidence base that some forms of home visiting have the potential to alter an infant or toddler’s trajectory within the child welfare system. That PFR might prevent or minimize parent–child separations is an important outcome for young children in child welfare and likely has substantial cost benefits. In addition to the benefits for the child welfare system, we would anticipate that the prevention of a parent–child relationship disruption coupled with the improvements in parental sensitivity and child development knowledge would have an ongoing, generative effect beyond the 15-month follow-up time period. Further research that documents longer term outcomes would be an important next step.
In this study, we assessed secure base behavior with the five-card sort that had been used in the ECLS-B study (Andreassen et al., 2006) as opposed to the trilemma sort version we used in our prior study (Pasalich, Fleming, Oxford, Zheng, & Spieker, 2016; Spieker et al., 2012). Across both sorting methods, results using the TAS-45 in our two studies have been mixed. In both studies, we did not find main effects of PFR on child secure base behavior at least up to 6 months postintervention when children were just under 2 years of age. In follow-up analyses of our prior RCT, we found an interaction between PFR and secure base behavior, such that for toddlers with a history of four or more placements, PFR improved secure base behavior (Pasalich et al., 2016). In the current study, thus far, we have only found a PFR main effect for fewer displays of child atypical affective communication on the TAS-45.
We did not find intervention effects on child social–emotional competence or behavior problems for either parent or research visitor ratings of the child. In our prior RCT, we found positive main effects on competence but not problem behavior (Spieker et al., 2012). We also found, however, a moderated mediation, such that for toddlers with a history of more placements, PFR predicted greater secure base behavior, which in turn buffered them against the development or exacerbation of externalizing problems (Pasalich et al., 2016). Similarly, for a subsample of 43 reunified children and their birth parents in the same RCT, we found stronger effects (d = .55–.57) on problem behavior (Oxford, Marcenko, et al., 2016). It may be that finding improvements in problem behavior is more likely when the base rate of problem behavior is high or the children represent a higher risk group, as it would be in a sample of those who have experienced multiple placement disruptions or reunified children with birth parents (Villodas, Litrownik, Newton, & Davis, 2015).
As in our prior RCT, we successfully implemented the PFR intervention with fidelity in a real-world, child welfare context, employing community social service providers. We are particularly encouraged by the high rate of completion of all 10 sessions. Eighty-six percent of PFR participants completed the program, replicating what we found in our prior work (Spieker et al., 2012). Seven percent of those assigned to PFR never received an intervention visit; thus, of those who experienced at least one intervention visit, the completion rate was 93%. We believe that the specific PFR consultation strategies that seek to recognize the positive actions of parents and help them reflect on their interactions with their child with the aid of video feedback contribute to the high retention rates among those we served. All staff (PFR providers, R&R providers, and research visitors) were trained to be nonpunitive for missed appointments, flexible in scheduling (including rescheduling and evening and weekend work), and to show respect toward families. In addition, PFR is relatively short-term and is narrowly focused on the parent–child relationship compared to other long-term home visiting programs that tend to have higher dropout rates (Duggan et al., 2004; Wagner, Spiker, & Linn, 2002). In comparison to Attachment Biobehavioral Catch-Up (ABC), another short-term, relationship-focused 10-week home visiting program, ABC retained 86% of their entire sample in at least one follow-up research visit (Lind, Bernard, Ross, & Dozier, 2014) which is similar to the 91% retained for research visits in this study. However, our retention rates could also be related to the extensive contact information we collected for each family, so if a family moved or a phone was disconnected, we were able to track them down through other contacts. It is also possible that the high completion rate was related to the monetary compensation parents received for participating in the research visits, although once randomized, engaging in the intervention was not required for participating in follow-up research visits and participants were not paid for the intervention visits.
Limitations
While the results of this study are promising, we did observe a smaller effect size on parental sensitivity relative to our first RCT (Spieker et al., 2012), although the effect was retained over the course of the follow-up. Contrary to our first study, we did not find effects on parental report of child behavior. Secure base behavior moved in the correct direction in both studies but was not significant. It should be noted that this study worked with families from one geographic area in Washington State and we were not able to contact all potentially eligible families. Almost half of the families identified in the electronic database could not or were not reached to determine if they were eligible or not; of those we reached, 31% were not eligible. Thus, although they did not differ from the enrolled sample on race and Hispanic ethnicity, it is possible that those not contacted differed from those whom we did contact in important ways, which may affect the generalizability of our findings. Our findings may not be generalizable for families without access to a telephone or who do not answer their phone for unknown numbers. For those who enrolled, all of the parents were English-speaking, 77% were White, 79% received food stamps, and most lived in suburban to semirural settings. It would be important to replicate these findings with different populations and in trials conducted by researchers external to our group. Finally, future studies should include longer term follow-up, including examination of CWS records, to assess whether intervention benefits are maintained and there are even longer term impacts on CWS involvement.
Conclusions
With an expanding national policy focus on early childhood and birth-to-three services that enhance both parent and child well-being, it is increasingly important for those designing and evaluating programs to conduct studies within the populations served. To date, two clinical trials of PFR have been embedded in child welfare populations and have relied on training community providers for service delivery. High rates of participant satisfaction and retention combined with improved parental knowledge, observed sensitivity, and more stability (via child welfare outcomes) were found in both studies. PFR’s strengths- and relationship-based approach is both respectful of and appreciated by families and this, in turn, appears to keep them engaged for the entire length of the program. The program intentionally focuses on increasing reflective capacity through the use of video feedback, which enables parents to engage in the content on a more personal level and to integrate it into their experience as parents. The implications of this work suggest that PFR is feasible, acceptable, and can improve CWS outcomes and parental sensitivity. It should be noted, however, that PFR only addresses one of the many needs of the CWS population. To address this population’s more intractable problems, PFR could be paired with other programs that provide solutions related to financial support, education, household items, and housing.
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants R01 HD061362 and U54HD083091 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development.