
Abstract
Researchers found that sexual abuse in childhood leads to increased adolescent depressive symptomatology, though this link may vary due to the relationship between the victim and the perpetrator as well as the age of the child when the abuse began. A sample of 444 sexually abused youth provided data for the National Survey of Child and Adolescent Well-Being I. Growth mixture modeling was used to identify trajectories of depressive symptoms and test the effects of parental perpetration and age of abuse onset. Results supported the following three growth trajectories of depressive symptoms in adolescence: falling, rising, and flat. Youth who were sexually abused by a parent were more likely to follow the rising and falling trajectories. Also, youth who experienced sexual abuse at a younger age were more likely to be classified in the falling trajectory. Findings can inform intervention programming on the links between sexual abuse characteristics and subsequent patterns of adolescent depressive symptomology.
Keywords
Sexually abused youth are at significant risk for the development of depressive symptoms in adolescence (Trickett, Noll, & Putnam, 2011). However, not all sexually abused youth develop similar levels of depressive symptoms (DuMont, Widom, & Czaja, 2007; Widom & White, 1997). Such heterogeneity in the development of depressive symptoms is evident in studies of community samples of nonmaltreated youth, which consistently documented distinct patterns of depressive symptom development (Mezulis, Salk, Hyde, Priess-Groben, & Simonson, 2014; Wickrama, Wickrama, & Lott, 2009). Some researchers identified two emerging risk factors for depression among youth with sexual abuse histories: the relational closeness between the victim and perpetrator (Freyd, 1996; McCrae, Chapman, & Christ, 2006) and children’s age at initial sexual abuse documentation (Feiring, Taska, & Lewis, 1999). However, more research is needed to fully identify how these risk factors influence heterogeneity in depressive symptomology development. The present study aims to address these gaps by identifying developmental patterns of depressive symptoms among a sample of youth with documented child sexual abuse (CSA) histories. Also, the current study aims to test the effects of parental compared to nonparental CSA perpetration as well as the age of CSA onset on the development of depressive symptom trajectories in adolescence.
Adolescent Depressive Symptom Trajectories and Person-Centered Methodologies
Researchers documented significant individual differences in rate and change in the development of adolescent depressive symptoms (DuMont et al., 2007; Wickrama et al., 2009), often identifying between three and four trajectories of adolescent depressive symptoms characterized by consistently high, consistently low, increasing, and/or decreasing patterns (Brendgen, Wanner, Morin, & Vitaro, 2005; Frye & Liem, 2011; Mezulis et al., 2014; Reinke, Eddy, Dishion, & Reid, 2012; Wickrama et al., 2009). In addition, scholars consistently reported that exposure to early adversity is an antecedent risk factor that significantly affects adolescent depressive symptom development such that youth with increased early adversity are more likely to follow increasing or high stable symptom trajectories (Brendgen et al., 2005; Frye & Liem, 2011). However, researchers have yet to document the developmental patterns of depressive symptoms among sexually abused youth.
Statisticians refer to methodologies quantifying interindividual differences in individual change and severity of depressive symptomatology over time as person-centered approaches. Specifically, these methods enable researchers to detect unobserved subgroups characterized by their unique patterns of change and severity in depressive symptoms. Studying patterns of depressive symptom development among sexually abused youth can add to and complement existing knowledge on the link between CSA and depressive symptom development in adolescence. Although more traditional means-based statistical approaches (i.e., variable-centered analyses) have effectively been used to identify associations between CSA experiences and heightened depressive symptom severity, the existence of unobserved patterns of these symptoms among sexually abused youth remains unknown. Scholars can use novel modeling-based approaches permitting the integration of variable- and person-centered statistical strategies to examine unobserved subgroups while testing for the influence of key sexual abuse characteristics (Vermunt, 2010). For example, growth mixture modeling is a longitudinal, person-centered methodology that can be used to examine latent or unobserved trajectories representing developmental growth patterns unidentifiable at the mean level as well as the testing of associations between putative antecedent variables (e.g., parental perpetration, age of abuse onset) and the documented trajectories (Jung & Wickrama, 2008).
CSA and the Development of Depressive Symptoms
Child sexual abuse, a type of child maltreatment defined as sexual contact between a child and caregiver or another adult (Barnett, Manly, & Cicchetti, 1993), is linked to the victim’s development of psychopathology symptomology such as depressive symptoms in adolescence (Maniglio, 2010). Researchers have identified links between CSA and depressive symptomatology even after accounting for the effects of other forms of child maltreatment (Lewis, McElroy, Harlaar, & Runyan, 2016). Despite this known association between CSA and depressive symptoms, some studies evince significant variability in the effect of CSA on depressive symptoms (DuMont et al., 2007; Widom & White, 1997). Further, risk factors that moderate the risk of depression among sexually abused youth likely affect this variability in symptomology. In the present study, we focus on two risky sexual abuse characteristics—parental perpetration and age of abuse onset—due to the sparse information on parental perpetration (McCrae et al., 2006) and the inconsistent findings on age of abuse onset (Bulik, Prescott, & Kendler, 2001; Dunn, McLaughlin, Slopen, Rosand, & Smoller, 2013) regarding their influence on youth risk of depressive symptomology.
Parental Perpetration of Sexual Abuse and Depressive Symptom Development
Researchers have found that perpetrators of varying relational closeness to the victim (e.g., strangers, relatives) commit CSA (U.S. Department of Health & Human Services, 2018). This difference in relational proximity significantly influences downstream victim psychopathology symptoms such that greater closeness is related to increased symptomology (Ullman, 2007). For example, youth victimized by caregivers evince increased internalizing and externalizing behaviors compared to youth victimized by noncaregivers (McCrae et al., 2006). Similarly, sexual abuse perpetrated by victims’ acquaintances and relatives, compared to sexual abuse perpetrated by strangers, more strongly associates with post-traumatic stress disorder diagnoses (Molnar, Buka, & Kessler, 2001). Lastly, perpetration by family members, compared to perpetration by nonfamily members, leads to heightened post-traumatic stress disorder symptoms among adolescent victims (Ullman, 2007).
Investigators can use the betrayal trauma theory to explain the association between CSA victim–perpetrator relationship closeness and victim psychopathology symptoms. From a betrayal trauma theory perspective, abused children emotionally struggle with reconciling traumatic events, especially abuse perpetrated by trusted caregivers (Freyd, 1996). Victims feel an increased sense of betrayal and decreased trust towards their perpetrator, which can lead to heightened risk of psychopathology symptomology (Gobin & Freyd, 2014). Indeed, existing data suggest that depressive symptoms are common among victims perpetrated on by previously trusted persons (Alto, Handley, Rogosch, Cicchetti, & Toth, 2018). Parental perpetration of CSA, which refers to sexual abuse committed by a biological or stepparent, may represent a more severe violation of trust compared to victimization by a relationally distant family member or an unrelated person, ultimately exacerbating the victim’s development of depressive symptomology. However, the current literature lacks studies that test the effect of parental compared to nonparental perpetration of CSA on youth depressive symptom development.
Age of Sexual Abuse Onset and Depressive Symptom Development
Based on the developmental psychopathology perspective (Cicchetti & Toth, 1995), younger youth are more vulnerable to adversity due to their increased psychological and biological sensitivity to stressful events (Granic & Hollenstein, 2003). Indeed, researchers have documented associations between earlier onset of child maltreatment with increased subsequent depressive symptomology (Thornberry, Henry, Ireland, & Smith, 2010). However, they have failed to conclusively detail how the age of CSA onset influences the development of mental health problems. Some investigators found that sexual abuse in childhood culminates into greater symptomology compared to sexual abuse in adolescence (Bulik et al., 2001; Dunn et al., 2013), while others identified that sexual abuse in adolescence is related to increased psychopathological symptomology compared to sexual abuse in childhood (Cutajar et al., 2010; Ruggiero, McLeer, & Dixon, 2000). In one study on the effect of age of CSA onset on depressive symptoms, youth victimized in adolescence showed heightened depressive symptomology compared to youth sexually abused in childhood (Feiring et al., 1999). However, researchers need to conduct more longitudinal research to understand the influence of CSA age of onset on the development of youth depressive symptoms in adolescence as many previous studies included retrospective and/or cross-sectional data (Bulik et al., 2001; Dunn et al., 2013; Feiring et al., 1999; Ruggiero et al., 2000) or symptomology assessed at a single time point (Cutajar et al., 2010).
Aims
Researchers documented that CSA leads to the development of depressive symptoms, but less is known about the longitudinal course of depressive symptoms among CSA youth as well as how CSA factors such as the victim–perpetrator relationship and age of abuse onset influence symptom development. The current study first aimed to document trajectories of adolescent depressive symptoms among sexually abused youth. Secondly, the investigation aimed to examine the effects of parental CSA perpetration on depressive symptomology growth patterns. The third aim was to test the association between age of CSA onset and youth depressive symptom trajectories. Based on previous research, the current hypotheses were as follows: First, we anticipated that differential trajectories would emerge for depression among sexually abused youth, providing a better explanation of depressive symptom development than a mean-level trajectory. Second, we expected that parental perpetration of CSA compared to nonparental perpetration of CSA would predict heightened depressive symptoms patterns. Third, we made no directional hypotheses regarding the age of CSA onset and depressive symptom patterns due to sparse and inconsistent findings in the current literature.
Method
Data were obtained from the National Survey of Child and Adolescent Well-Being I (NSCAW-I). The NSCAW-I is a longitudinal, nationally representative data set of children and families involved with child protective services (CPS; NSCAW Research Group et al., 2002). State and county child welfare agencies were directly recruited to the project by NSCAW-I staff. Upon the admittance of an agency to the study, NSCAW-I field representatives began recruiting eligible families served by that agency via in-person communication or by postcard depending on that state’s laws and CPS agency’s procedures regarding confidentiality (Dowd et al., 2007). NSCAW-I field staff initially interviewed focal children (N = 5,501) as well as their caregivers, teachers, and CPS caseworkers in 1999. The current study utilized data from a subsample of youth who were reported to CPS for CSA victimization (n = 444; M ageWave1 = 10.86; rangeageWave1 = 7–15; 72.70% female; 56.8% White; 26.4% Black; 80.4% non-Hispanic). NSCAW-I staff collected baseline data 2–6 months after investigations into sexual abuse allegations closed (Dowd et al., 2007). The majority of youth experienced sexual abuse before adolescence (68.6% before Age 12). The current data are from four waves: baseline (M ageWave1 = 10.86, SD ageWave1 = 2.45), 18-month (M ageWave2 = 12.23, SD ageWave2 = 2.48), 36-month (M ageWave3 = 13.49, SD ageWave3 = 2.44), and 72-month postbaseline (M ageWave4 = 17.36, SD ageWave4 = 2.18). At each wave, NSCAW-I research assistants who previously attended a 12-day training program on data collection procedures conducted in-person interviews with youth, their caregivers, and their caseworkers. Computer-assisted personal interview and audio computer–assisted self-interview programs ensured confidentiality and reduced reporting biases. More information on sampling procedures, recruitment, and other NSCAW-I project details exist elsewhere (Dowd et al., 2007; NSCAW Research Group et al., 2002). The institutional review board of the authors’ university approved this analysis of secondary data.
Measures
Inclusion criteria: Child sexual abuse (Wave 1)
The details of CSA cases were reported via a modified version (English & LONGSCAN Investigators, 1997) of the maltreatment classification system (MCS; Manly, Cicchetti, & Barnett, 1994). The MCS was developed to use CPS documentation of maltreatment investigations to obtain abuse and neglect information. For the NSCAW-I project, formally trained research assistants used the modified MCS to code CPS notes into specific maltreatment details such as maltreatment type and severity. Cases in which the caseworkers indicated that youth were reported for CSA were included in the current sample. These were initial reports of CSA victimization and not follow-up reports of sexual revictimization.
Predictors: Sexual abuse characteristics and other covariates (Wave 1).
Parental perpetration
Trained CPS caseworkers reported who perpetrated the CSA via the modified MCS (Barnett et al., 1993; English & LONGSCAN Investigators, 1997). For the current study, parental perpetration was examined. Parental perpetration was assessed by combining cases where the biological father or stepfather (n = 144) or biological mother or stepmother (n = 17) perpetrated the sexual abuse. The parental perpetration group was coded as 1. The reference group was created by combining cases with nonparental perpetrators of CSA and was coded as 1 (n = 203). 1
Age of sexual abuse onset
The age at which CSA began was calculated by subtracting the CPS caseworker’s report of CSA duration from the caregiver’s report of the child’s age at Wave 1. This method has been previously used to accurately determine age of maltreatment onset with official maltreatment records (Perlman & Fantuzzo, 2010). Due to their non-normal distribution, the age of CSA onset data was winsorized to three standard deviations above the mean (Ghosh & Vogt, 2012), thereby permitting their use as predictors in the current analyses due to statistical assumptions of data normality.
Covariates
The primary caregiver reported their child’s minority status (i.e., non-White race and/or Hispanic ethnicity) and gender as well as their yearly household income. The severity of sexually abusive acts (i.e., penetration) was reported by the caseworker via the MCS. Penetration (vaginal, anal, or oral) of the child was coded as 1 and other forms of sexual abuse were coded as 0.
Trajectories: Depressive symptoms (Waves 1–4)
Youth depressive symptoms were assessed using the Children’s Depression Inventory (CDI; Kovacs, 1985). The CDI is a child self-reported measure of depressive symptomology with 27 items answered on a 3-point scale (0 = absence of symptom, 1 = mild symptom, and 2 = definite symptom). The standardized, norm-referenced total scores were used for the current study and evinced strong internal reliability (α M = .83). All four waves (baseline, 18-, 36-, and 72-month postbaseline) of data collection were included in the modeling of adolescent depressive symptoms trajectories.
Analytic Plan
GMM: Aims 1 and 2
To address the aims of the current manuscript, growth mixture modeling (GMM) was used to identify patterns of severity and change in the development of depressive symptomology across late childhood and through adolescence. Growth mixture modeling allows for the classification of groups of youth based on the severity (i.e., level) and rate of change (i.e., growth) in depressive symptoms across adolescence via assignment of class membership probabilities ranging from 0 (0% likelihood of belonging to that trajectory) to 1 (100% likelihood of belonging to that trajectory; Jung & Wickrama, 2008). The analyses were conducted in sequential steps via a procedure designed to ensure independence between the classification solution and the subsequent analyses of predictors and covariates (Lanza, Tan, & Bray, 2013).
To address the first aim, an unconditional growth curve model was run to examine the sample’s mean level of change (i.e., mean trajectory) of adolescent depressive symptoms. The interindividual variability in change of depressive symptoms across the four waves of data was probed by examining the variances of the intercept, slope, and quadratic estimates. Upon finding variability in interindividual change in depressive symptoms, the second analytical step was pursued in which GMM was conducted to identify subgroups (i.e., latent trajectories) that were distinct in individual change of depressive symptomology (Wang & Bodner, 2007). The number of random sets of starting values, final optimizations, and start iterations was set to 200, 20, and 20, respectively, to ensure successful convergence in the exploration of multiple trajectory solutions and avoid problems related to local maxima (Jung & Wickrama, 2008). To determine the optimal trajectory solution for the GMM, key model fit indicators were used, including the Akaike information criterion (AIC), Bayesian information criterion (BIC), sample-size adjusted Bayesian information criterion (A-BIC), and entropy (Jung & Wickrama, 2008; Wang & Bodner, 2007). In addition and per recommendations by Nylund, Asparouhov, and Muthén (2007), substantive consideration (e.g., model parsimony, previous research, existing theory, and interpretive value) was used to evaluate the optimal model selection. To examine the second and third aims, the last model included a multinomial logistic regression framework to test associations between key predictor variables (i.e., parental perpetration, age of CSA onset) and covariates (i.e., child minority status, gender, household income, and abuse severity) with the resultant adolescent depressive symptom trajectory solution.
Data management
All analyses were conducted in Mplus 7.4 (L. K. Muthén & Muthén, 2017). The maximum likelihood estimation with robust standard errors was used to control for non-normality. Given that the data met criteria for missing at random (Buhi, Goddson, & Neilands, 2008; Johnson & Young, 2011; Little & Rubin, 2002; Schlomer, Bauman, & Card, 2010), the full information maximum likelihood estimation was used to model missing data. Post hoc power analyses via z-tests were conducted using G*Power (Faul, Erdfelder, Lang, & Buchner, 2007). The logistic regression paths from predictors and covariates to class memberships were tested, and the odds ratios (OR) of those associations were the units of analysis. The results revealed that most analyses were powered higher than 80% (α = .05). Average missing data were 12.61%, 19.59%, 18.69%, and 67.80% for Waves 1, 2, 3, and 4, respectively. Youth who were older at the onset of abuse had more missing data (p = .001), which was due to attrition in most cases. Missing data at later waves were unrelated to depressive symptomology at baseline (p > .2). Item nonresponse or refusal was minimal (NSCAW Research Group et al., 2002), likely due to the use of computer-assisted survey administration as opposed to other methods (i.e., interviewer administered) that might have compromised respondents’ sense of privacy (Biemer, Herget, Morton, & Willis, 2000). Eleven cases were automatically dropped from the analyses due to missing depressive symptom data on all four waves.
Use of the NSCAW-I data set
Sampling weights were included in all models to account for initial participant nonresponse as well as for deliberate oversampling in the NSCAW-I sample. The NSCAW-I staff intentionally recruited more families with infants, sexual abuse allegations, and ongoing services post-investigation than was nationally representative at the time to ensure that there would be sufficient power to specifically examine those groups in statistical analyses. Due to the two-stage stratified sample design of the NSCAW-I sample, stratification and clustering weights were also included in all models to control for the unique effects of the nine sampling strata as well as the 92 clustered primary sampling units; thus, permitting findings to be inferred to the national level of children and families investigated for sexual abuse (NSCAW Research Group et al., 2002). More information about the NSCAW-I sampling procedures and specific analytic recommendations can be found elsewhere (Dowd et al., 2007).
Results
See Table 1 for study variable descriptive statistics and Table 2 for correlations between variables.
Descriptive Statistics.

Note. N = 444. Frequency and percentage shown instead of mean and standard deviation for dichotomous variables: parental perpetrator = 0 (no), 1 (yes); CSA severity = 0 (less severe acts), 1 (intercourse or insertion); gender = 1 (female), 1 (male); minority status = 0 (White/non-Hispanic), 1 (minority race/minority ethnicity). Age of abuse onset reported in years. Family income reported via range and the mean range was 5 (US$20,000–24,999). Depression Wx = depressive symptoms at Wave x. SD = standard deviation; CSA = child sexual abuse.
*p < .05.
Bivariate Correlations.
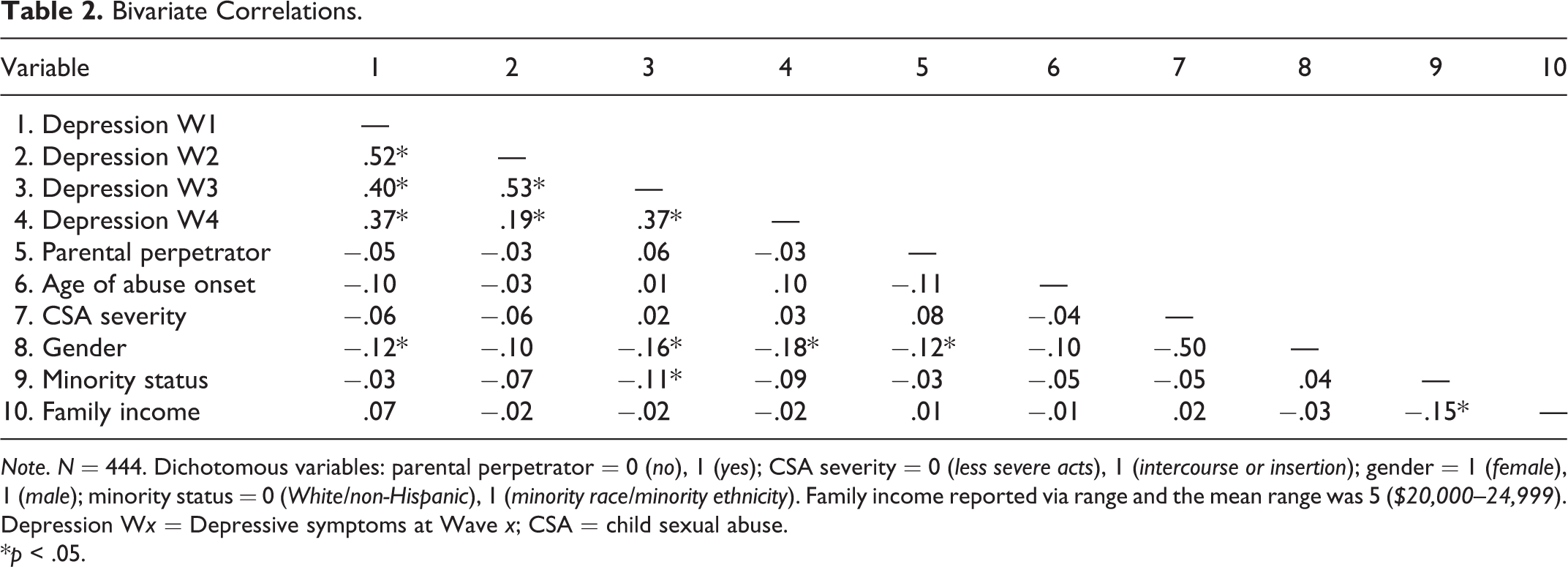
Note. N = 444. Dichotomous variables: parental perpetrator = 0 (no), 1 (yes); CSA severity = 0 (less severe acts), 1 (intercourse or insertion); gender = 1 (female), 1 (male); minority status = 0 (White/non-Hispanic), 1 (minority race/minority ethnicity). Family income reported via range and the mean range was 5 ($20,000–24,999). Depression Wx = Depressive symptoms at Wave x; CSA = child sexual abuse.
*p < .05.
Aim 1: Unconditional Growth Curve and Mixture Models
Results from an unconditional growth curve model indicated that the sample evinced a high initial mean level of depressive symptoms (B = 53.68, p = .001) followed by a decline (B = −3.55, p = .002) with a convex curve (B = .56, p = .023) that lead to a plateau over time. The model showed good fit with the data: χ2(1) = 0.17, p = .68; comparative fit index = 1.00; root mean square error of approximation = .00; standardized root mean square residual = .01. The results also identified significant variance in the intercept (s 2 = 119.41, p = .001), slope (s 2 = 84.53, p = .001), and quadratic estimates (s 2 = 3.32, p = .009). See Table 3 for more details.
Parameter Estimates for Unconditional Growth Curve and Mixture Models.

Note. N = 444. Est. = estimate; SE = standard error.
a Variance was significant at p < .05. *p < .05.
An unconditional growth mixture model was performed to probe for unobserved heterogeneity in the sample’s growth of depressive symptoms over time. The variance of the final wave of depressive symptoms was fixed to zero to ameliorate convergence issues due to nonsignificant negative residual variance. The three-trajectory solution showed better model fit than the one- and two-trajectory models as indicated by lower values of AIC, BIC, and A-BIC. The four-trajectory model evinced higher values of entropy than previous trajectory solutions; however, the four-trajectory model included a class that was too small for trustworthy generalization (i.e., n < 5%; B. Muthén & Muthén, 2000) and contained two classes with similar trajectories, thus diminishing model parsimony. We did not formally pursue models with five or more classes due to similar problems. Based on the adequate model fit statistics, previous findings on adolescent depressive symptom trajectories, and substantial pattern separation with clear interpretations, we chose the three-trajectory model as the optimal class solution. This solution comprised the following growth patterns: low depressive symptoms at all four waves (flat; n = 343, 79.16% of sample); moderate depressive symptoms at Wave 1, high depressive symptoms at Waves 2 and 3, and moderate depressive symptoms at Wave 4 (rising; n = 54, 12.39% of sample); and high depressive symptoms at Wave 1, moderate depressive symptoms at Wave 2, low depressive symptoms at Wave 3, and moderate depressive symptoms at Wave 4 (falling; n = 37, 8.45% of sample). See Table 4 and Figure 1 for more details.
Fit Statistics for Depressive Symptom Growth Mixture Models.
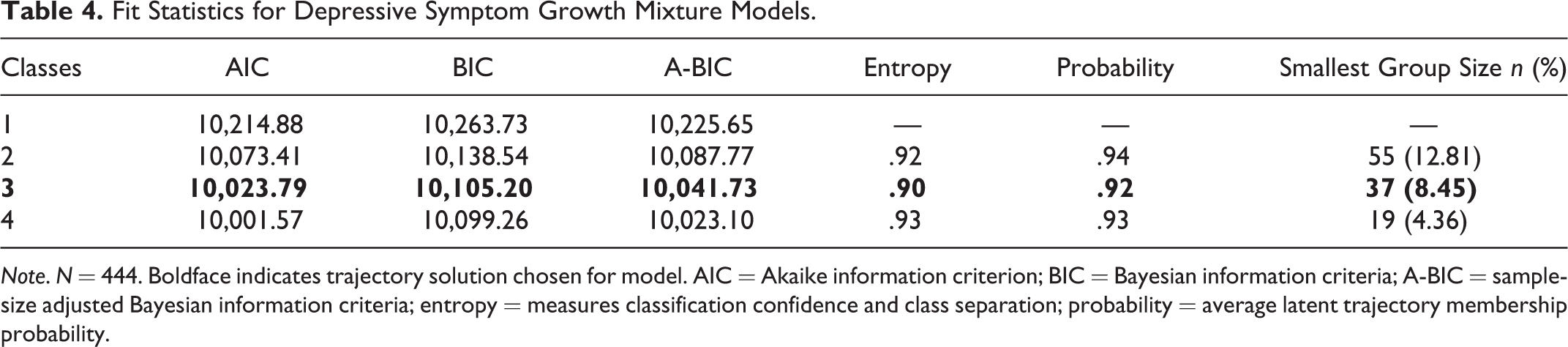
Note. N = 444. Boldface indicates trajectory solution chosen for model. AIC = Akaike information criterion; BIC = Bayesian information criteria; A-BIC = sample-size adjusted Bayesian information criteria; entropy = measures classification confidence and class separation; probability = average latent trajectory membership probability.
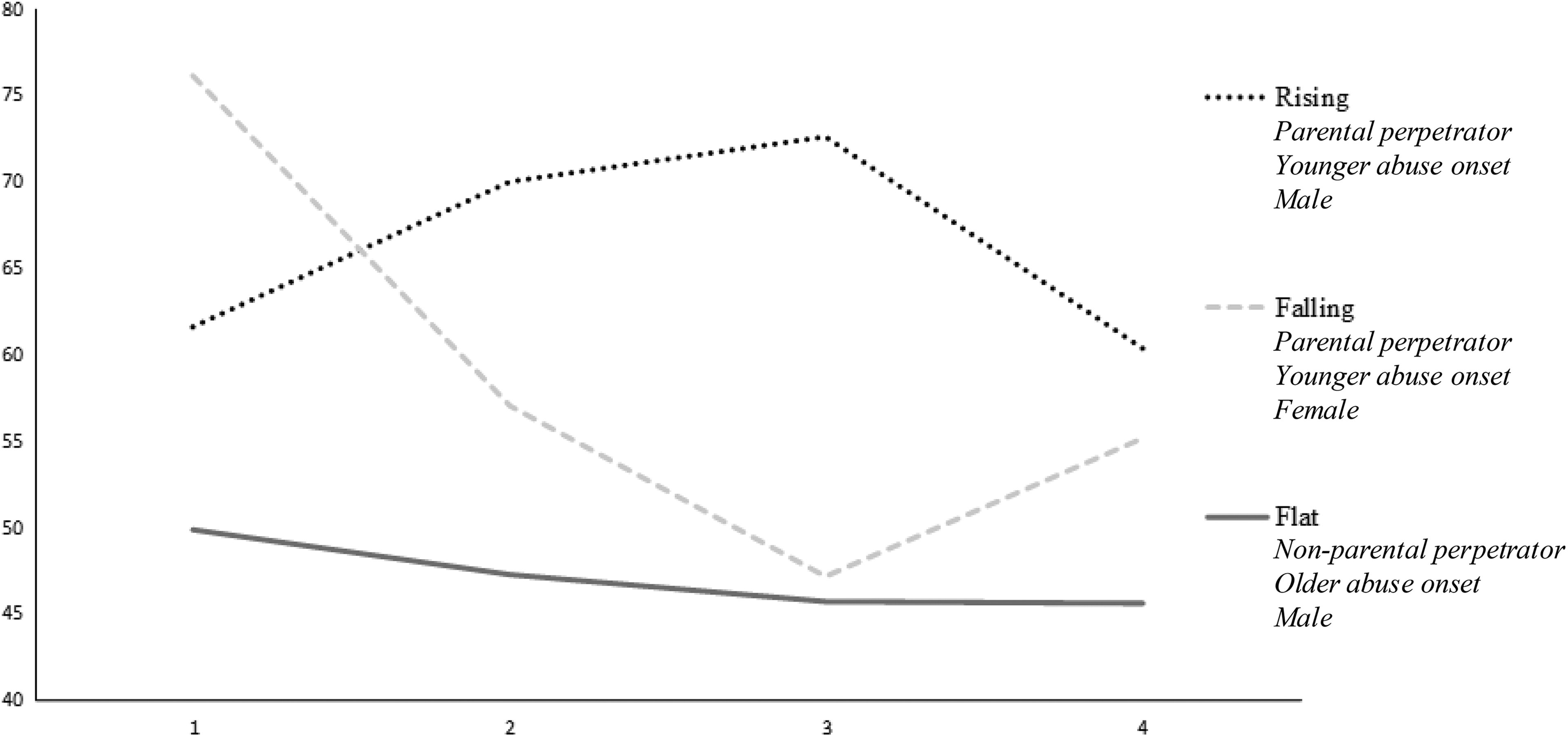
Three-trajectory solution of depressive symptom trajectories among sexually abused youth (N = 444). Estimated means shown here. Variables associated with trajectories are displayed in italics below trajectory nomenclature. The y-axis refers to depressive symptom T-scores (range: 34–100), and the x-axis refers to the data collection wave (range: 1–4). Trajectory sizes: flat (n = 343), rising (n = 54), and falling (n = 37).
Aims 2 and 3: Conditional Growth Mixture Model (With Predictors and Covariates)
Parental perpetration, age of abuse onset, and covariates were simultaneously entered into a multinomial logistic regression framework to test their probabilistic associations with trajectories from the resultant class solution. Youth who were victimized by parental compared to nonparental perpetrators were more likely to be classified into the rising and falling trajectories compared to the flat trajectory (respectively: OR = 3.08, p = .042; OR = 2.50, p = .049). Youth who were older at the abuse onset were less likely to follow the falling trajectory compared to the flat (OR = .73, p = .017) and rising trajectories (OR = .60, p = .001). Males were less likely to evince membership in the flat (OR = .10, p < .027 and rising trajectories (OR = .09, p = .045) compared to the falling trajectory.
Discussion
CSA is a stressful, traumatic experience for youth and is associated with significant risk for the development of depressive symptomatology in adolescence (Trickett et al., 2011). Researchers documented heterogeneous patterns in the development of depressive symptoms among community samples of adolescents (Brendgen et al., 2005; Frye & Liem, 2011; Mezulis et al., 2014; Reinke et al., 2012; Wickrama et al., 2009), yet similar research with sexually abused youth is scarce. Further, some scholars suggested that the effect of sexual abuse on the development of adolescent depressive symptoms varies significantly due to key aspects of the CSA experience such as the victim–perpetrator relationship (McCrae et al., 2006) and age of abuse onset (Feiring et al., 1999). The current study addressed these gaps by using a person-centered approach to model depressive symptom development across adolescence. Also, the effect of parental CSA perpetration and age of CSA onset on the hypothesized heterogeneity in depressive symptom development was examined. Findings showed that sexually abused youth composed three distinct trajectories of depressive symptomology across adolescence (i.e., rising, falling, and flat). Compared to youth with nonparental CSA perpetration, youth with parental CSA perpetration had increased membership in the rising and falling trajectories compared to the flat trajectory. Youth sexually abused at an earlier age followed the falling pattern compared to the flat and rising trajectories, whereas youth sexually abused at a later age followed the rising trajectory compared to the falling trajectory.
Aim 1: Depressive Symptom Trajectories Among Sexually Abused Youth
Our first aim was to identify patterns of change in depressive symptomatology among youth with documented histories of CSA. Researchers examining depressive symptom patterns among community samples of youth typically identified three or four depressive symptom trajectories characterized by increasing, decreasing, consistently low, and/or consistently high patterning (Reinke et al., 2012; Wickrama et al., 2009). Our findings are consistent with previously documented typologies of depressive symptom development in adolescence (Mezulis et al., 2014). Specifically, the current results replicated three distinct trajectories of depressive symptomology across adolescence (i.e., rising, falling, and flat) among an at-risk group of sexually abused youth. These trajectories are similar to three depressive symptom patterns commonly identified among community youth: increasing, decreasing, and consistently low symptoms, respectively (Brendgen et al., 2005; Frye & Liem, 2011; Mezulis et al., 2014; Reinke et al., 2012; Wickrama et al., 2009). A consistently high class, often documented among non-CPS involved samples (Reinke et al., 2012; Wickrama et al., 2009), was not identified in the current typology. This typological difference may be a result of distinctions between community youth and youth exposed to adverse childhood experiences such as CSA (Mezulis et al., 2014; Wickrama et al., 2009). It is possible that, due to the current sample’s CSA histories, the present three-trajectory solution might, if combined, compose a consistently high trajectory of depressive symptoms when examined in comparison to trajectories of youth without sexual abuse histories. This possibility points to the importance of examining samples of maltreated youth in isolation from nonmaltreated youth, as there is likely some risk of failing to find variability in symptomology when comparing maltreated and nonmaltreated samples.
The youth in the rising and falling trajectories evinced significant quadratic growth in depressive symptoms, suggesting that there is discontinuity in the development of depressive symptoms across adolescence among sexually abused youth. These findings support previous evidence of quadratic growth of depressive symptom development across adolescence as well as researchers who argue that youth depressive symptom patterning over time is best explained by nonlinear paths (Garber, Keiley, & Martin, 2002). The present study adds to existing knowledge on depressive symptoms among sexually abused youth by suggesting that the development of depressive symptomology among youth with CSA is not always a stable, continuous process (Cicchetti & Toth, 1995). Documenting this nonlinear pattern is critical as many treatments for youth psychopathology symptoms presume stability in the course of mental illnesses, leading to an underestimation of symptom recurrence likelihood (Drake & Whitley, 2014). Importantly, youth in the rising and falling classes evinced moderate levels of depressive symptoms at the final wave of data collection, though they demonstrated distinct pathways of depressive symptom development in previous waves. Discontinuity in depressive symptomology across adolescence may culminate into instances of equifinality as seen in the common ending point of depressive symptomology between the rising and falling classes (Cicchetti & Rogosch, 1996). However, it is unclear what the implications of depressive symptom pathway vis-à-vis ending point may have on other developmental outcomes if any. Researchers can examine the consequences of pathways versus endpoints of symptomology among youth exposed to adversity.
The majority of youth followed the flat trajectory, indicating that low levels of symptomology may be the normative pattern of depressive symptom growth among sexually abused youth. This finding is consistent with previous longitudinal research on maltreated youth documenting that—despite the known association between forms of maltreatment such as sexual abuse and resulting psychopathology symptoms (Oddone Paolucci, Genuis, & Violato, 2001)—the majority of abused and neglected individuals do not grow up to evince substantial psychological problems (Cutajar et al., 2010; Widom & White, 1997). Researchers can continue to investigate how to assist this population in the recovery from experiences of adversity while recognizing that most maltreated youth will evince resilient developmental outcomes (McGloin & Widom, 2001).
Gender was a significant covariate in the current analyses, such that females were more likely to be in the falling class compared to the rising and flat classes. As youth in the falling class were younger at abuse onset, this finding corroborates previous scholarship suggesting that girls experience sexual abuse at a younger age than boys (Putnam, 2003). Much more research is needed to understand how gender influences CSA onset and the course of depressive symptoms among sexually abused youth.
Aim 2: Parental Perpetration of Sexual Abuse and Depressive Symptom Trajectories
Our second aim was to test the effect of parental compared to nonparental CSA perpetration on adolescent depressive symptom growth patterns. Based on the previous research (McCrae et al., 2006; Molnar et al., 2001; Ullman, 2007), we hypothesized that parental perpetration of CSA would predict heightened depressive symptom patterning. Our findings supported this hypothesis, demonstrating that CSA perpetrated by parents compared to nonparents induced youth to follow heightened patterns of depressive symptom growth. These results are consistent with the findings of other researchers who found that closer relational ties between the victim and perpetrator lead to increased victim symptomatology (McCrae et al., 2006; Molnar et al., 2001; Ullman, 2007). Notably, parental perpetration was not correlated with depressive symptoms in bivariate analyses (see Table 2) but predicted membership in the rising and falling trajectories (see Table 5) compared to the flat trajectory. This finding suggests that the influence of sexual abuse characteristics such as parental perpetration may not always be identifiable when examining mean-level changes in the presence of substantial symptomology variability. The current results supported the literature on betrayal trauma theory (Freyd, 1996). According to betrayal trauma theory, parental perpetration leads to greater psychopathology symptoms due to the victim’s enhanced sense of betrayal and loss of trust toward the previously entrusted person.
Multinomial Logistic Regression Framework Testing Associations Between Predictors and Covariates With Depressive Symptom Trajectories.

Note. N = 444. Gender coded as −1 = female and 1 = male. Nonsignificant covariate effects (i.e., sexual abuse severity, minority status, and family income) not shown for clarity. OR = odds ratio; CI = confidence interval.
*p < .05.
Aim 3: Age of Sexual Abuse Onset and Depressive Symptom Trajectories
Our third aim was to test the link between the documented age of CSA onset and depressive symptom trajectories. Thus far, literature on the association between age of CSA onset and subsequent psychopathology symptom severity has been inconclusive. Some researchers reported that risk of symptomatology is higher among youth victimized in childhood (Dunn et al., 2013), while other researchers found that youth victimized in adolescence are at heightened psychopathological risk (Ruggiero et al., 2000). The current analyses found that earlier CSA onset was linked to the falling pattern, whereas later CSA onset was related to the rising pattern, suggesting that both childhood and adolescence are developmental periods of sensitivity to depressive symptomology, though they resulted in different pathways of depressive symptom development. The falling trajectory, composed of younger youth, evinced increased initial symptoms after the abuse, which is consistent with other maltreatment research on the increased negative effects of abuse at younger ages (Thornberry et al., 2010). Heightened initial symptomology among children may reflect increased sensitivity to stressful experiences due to vulnerable, developing brain regions (Granic & Hollenstein, 2003). The depressive symptoms of the falling trajectory ebbed through late childhood and did not begin to ascend again until approximately age 12. Alternatively, the rising group, composed of older youth, experienced rising and chronically high levels of depressive symptoms across adolescence. The persisting elevation of the rising trajectory and the delayed rise of the falling trajectory appear to coincide with the developmental period of adolescence in which youths’ sexual awareness is emerging (i.e., early adolescence; Cutajar et al., 2010). This timing may place youth at an increased risk of depressive symptomology due to their enhanced understanding of the sexually violating nature of CSA acts. More research is needed to clarify the mechanisms underlying developmental periods that incur vulnerability for the development of psychopathology symptoms.
Limitations
The present study utilized four waves of multi-reporter data from a nationally representative sample of youth reported to CPS for sexual abuse victimization. Despite noteworthy strengths, there are some limitations to the current findings. First, official government CSA data are more robust to the biases inherent in self-report measures (Edwards et al., 2001), although authorities are not able to detect all instances of sexual abuse (London, Bruck, Ceci, & Shuman, 2005). Thus, the representativeness of the current findings to sexually abused youth not investigated by CPS is unclear. Second and despite using a large sample of youth with documented CSA histories, we still found two small trajectories of depressive symptoms (i.e., the falling and rising groups). If possible, researchers should use larger samples to further validate the current findings. Third, the current study extended previous research on the effect of victim–perpetrator relationship on youth psychopathology symptomology by examining the influence of parental CSA perpetration on adolescent depressive symptom growth. However, some researchers found that measuring the length of time the victim lived with the perpetrator may be a better estimate of victim–perpetrator relational closeness than genetic relation or relationship category (Berman & Knight, 2015). Future studies may benefit from using multiple indicators (e.g., time living together, perceived trust, and relationship status) to probe how aspects of the victim–perpetrator relationship are related to victim symptomology. Fourth and based on the previous literature, we chose to examine the effect of sexual abuse perpetration by parents. Based on the protocols of other research examining parental perpetration of child maltreatment (Annerbäck, Svedin, & Gustafsson, 2010; Coohey, 2003), we limited the scope of “parent” to father, mother, stepfather, and stepmother. We excluded unmarried romantic partners as some researchers suggested that unmarried romantic partners play a different familial role than biological or stepparents (Margolin, 1992; Radhakrishna, Bou-Saada, Hunter, Catellier, & Kotch, 2001). However, it is possible that these romantic partners as well as relatives such as aunts, uncles, and siblings may play the role of a parent and would incur increased victim psychopathology following sexual abuse perpetration, though more research is needed to assess this. Lastly, the current study examined the role of some sexual abuse characteristics (i.e., victim–perpetrator relationship, age of abuse onset) in depressive development patterning, though other aspects of the child maltreatment such as number of perpetrators (Briere & Elliott, 2003) and frequency of abuse (Filipas & Ullman, 2006) are known to impact victim psychopathology symptoms. Future studies can consider the impact of these variables when examining depressive symptom heterogeneity in samples of sexually abused youth.
Conclusion and Implications for Prevention, Policy, and Future Research
The current study builds upon existing knowledge about CSA, adolescent depressive symptomology patterns, parental perpetration of CSA, and age of CSA onset. Sexually abused youth evinced three trajectories of depressive symptoms development (i.e., falling, rising, and flat) with most youth exhibiting consistently low symptomology (i.e., flat). Youth with parental CSA perpetration followed trajectories of heightened adolescent depressive symptoms (i.e., falling and rising). Additionally, youth with earlier CSA onset followed a trajectory with initially higher symptoms that decreased (i.e., falling), and youth with later CSA onset followed a trajectory that evinced initially lower symptoms that increased (i.e., rising).
The findings of the current study have implications for preventive interventions, public policy, and future research. Interventionists can use this information by screening CSA cases for characteristics that signal a need for enhanced psychological treatment (e.g., having a parental perpetrator). Additionally, clinicians providing treatments for both youth abused in childhood and youth abused in adolescence can be aware of the differing but similarly elevated courses of depressive symptoms that youth may experience. Policy makers can consider the results of the present study and make more effective programmatic decisions for CSA cases as well as allocate additional treatment funding for victims with increased risk factors (e.g., parental perpetrator). Lastly, researchers can build on the findings of the present study by examining more intricate comparisons of parental sexual abuse perpetrators (e.g., biological versus stepparents), inspecting potential mechanisms in the link between victim–perpetrator relationship and victim psychopathology symptoms, and testing hypotheses about age of CSA onset and the role of sexual awareness in depressive symptom development postsexual abuse. Furthermore and based on the research showing that sexual revictimization is common among sexually abused youth (Arata, 2002; Classen, Palesh, & Aggarwal, 2005) and that age at sexual abuse onset is linked with revictimization risk (Casey & Nurius, 2005; Simmel, Postmus, & Lee, 2012), future researchers can inspect how repeated sexual victimizations across developmental stages interact with concurrent depressive symptom trajectories.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.