
Abstract
Rates of attrition from pediatric trauma-focused treatments are high, yet few studies have examined predictors of dropout. The aim of the study was to investigate whether higher levels of caregiver- and child-reported pretreatment difficulties predicted attrition from trauma-focused therapy. One hundred seventy-two children aged 6–18 (M = 10.53, SD = 3.36; 64% female, 64% Black) and their caregivers were included in the study. Two operational definitions of attrition were utilized: (1) clinician-rated dropout and (2) whether the child received an adequate dose of treatment (i.e., 12 or more sessions). Rates of clinician-rated attrition were high (76.2%); however, 73.8% received an adequate dose. Despite expectations, higher levels of rule-breaking and aggressive behavior were related to clinician-rated dropout (d = 0.59, .63, respectively) but were not significant predictors in a logistic regression model. Child-reported symptoms were unrelated to clinician-rated attrition. Higher levels of caregiver-reported anxiety/depression, somatic complaints, and trauma-related difficulties corresponded with adequate dose (ds = 0.52–1.06). Yet only caregiver-reported sexual concerns predicted adequate dose in a regression model (OR = 1.09). Caregiver- and child-reported symptoms may be unrelated to clinician-rated treatment completion and appear to play a small role in understanding whether the child received an adequate dose of treatment.
Childhood trauma exposure is associated with a host of negative outcomes, not limited to post-traumatic stress disorder (PTSD), depression, anxiety, and externalizing difficulties (Ackerman, Newton, McPherson, Jones, & Dykman, 1998; Cicchetti & Toth, 1995; Copeland, Keeler, Angold, & Costello, 2007; Putnam, 2003). Thankfully, there is compelling empirical evidence that several pediatric trauma-focused treatments mitigate trauma-related difficulties (Cary & McMillen, 2012; Cohen et al., 2010; Cohen, Mannarino, & Deblinger, 2006; Scheeringa, Weems, Cohen, Amaya-Jackson, & Guthrie, 2011). In spite of the documented efficacy of pediatric trauma-focused interventions, between 33% and 77% of families prematurely terminate (Wamser-Nanney & Steinzor, 2016, 2017; Wamser-Nanney, Scheeringa & Weems, 2016; Cohen, Mannarino, & Ivengar, 2011; Gillies, Taylor, Gray, O’Brien, & D’Abrew, 2013; Scheeringa et al., 2011). High rates of attrition are problematic for several reasons. Most importantly, trauma-related difficulties are unlikely to spontaneously remit (Scheeringa & Zeanah, 2008), and many trauma-exposed children who do not fully complete the treatment protocol likely continue to suffer from trauma-related difficulties. Premature termination also negatively impacts clinical research by decreasing internal validity and reducing statistical power (Armbruster & Kazdin, 1994; Kazdin, Holland, & Crowley, 1997; Warnick, Gonzalez, Weersing, Scahill, & Woolston, 2012). Consequently, research devoted to identifying risk factors from child trauma-focused treatment is critical to ultimately help prevent attrition through more targeted intervention efforts.
Trauma-exposed families face several challenges when completing treatment, some of which are unique to this population. Foremost, avoidance of trauma-related content is a required symptom for a PTSD diagnosis (American Psychiatric Association, 2013), and avoidance symptoms are also common among individuals with subthreshold PTSD symptoms. Many caregivers of trauma-exposed children are trauma survivors themselves, either from prior traumatic events or from a “shared” traumatic experience with their child such as exposure to intimate partner violence. Trauma-related reminders and difficulties are naturally distressing, which understandably engenders a desire to avoid this content to prevent experiencing negative affect. Nonetheless, trauma-related content is unavoidable in the context of trauma-focused treatment. In the pediatric population, there is a “double risk” for premature termination as either the child’s or the caregiver’s avoidance may increase the risk for attrition. Caregivers may be referred to treatment by other professional systems (i.e., law enforcement, medical, Child Protective Services [CPS]) and may initially follow this recommendation for therapy but may not “buy in” or believe that intervention is needed. Finally, trauma exposure is often coupled with numerous secondary adversities such as loss of resources, changing residences or schools, legal involvement and proceedings, and placement in CPS custody (Pynoos, Steinberg, & Piacentini, 1999). In the face of these competing stressors, families may understandably prioritize basic family needs compared to treatment completion (Cohen et al., 2011).
In spite of the relative wealth of research that has established the efficacy of child trauma-focused treatment, there is a paucity of studies that have examined predictors of attrition. Child demographic factors have been routinely investigated in relation to premature termination; however, results are generally mixed. Older child age has been related to attrition in a few trauma-focused studies (Author citation; Fraynt et al., 2014), but others have not found differences (Sprang et al., 2013; Yasinski et al., 2018). Children’s gender has generally not corresponded with dropout from trauma treatment (Author citation; Author citation; Celano, NeMoyer, Stagg, & Scott, 2018; Sprang et al., 2013; Yasinski et al., 2018). Children from a racial minority group have been at higher risk for attrition in some studies (Author citation; Murphy et al., 2014; Sprang et al., 2013), but not others (Celano et al., 2018; Yasinski et al., 2018). Children with unmarried parents and families with lower household incomes may be at higher risk for dropout (Author citation; Cohen & Mannarino, 1996; Jensen et al., 2014). Taken together, it seems as though when differences are observed, older and minority children and those with unmarried parents may be more likely to prematurely terminate from trauma-focused treatment, which may be a function of fewer resources. Interestingly, several studies have reported that CPS involvement was a protective factor against attrition (Author citation; Author citation; Sprang et al., 2013; Yasinski et al., 2018). Families who are involved with CPS may be less likely to drop out as treatment may be recommended or even mandated, and this external monitoring may encourage caregivers to complete treatment.
Nevertheless, it is important to note that many of the prior trauma-focused research studies were conducted with small sample sizes, several of which included a total of 20–40 participants, and others had fewer than 20 participants per group, making them inadequately powered to detect differences between treatment completers and noncompleters (e.g., Cohen, Deblinger, Mannarino, & Steer, 2004, Cohen et al., 2011; Deblinger, McLeer, & Henry, 1990; Deblinger, Mannarino, Cohen, Runyon, & Steer, 2011; Cohen & Mannarino, 1996, 2000; King et al., 2000). Several of these studies did not observe differences between groups in terms of child and family characteristics and attrition, perhaps due to being underpowered (e.g., Cohen et al., 2004, 2011; Deblinger et al., 1990, 2011; Cohen & Mannarino, 1996, 2000). Two other studies (i.e., Celano et al., 2018; Yasinski et al., 2018) used relatively larger samples (n = 77; n = 108, respectively) and did not observe demographic differences; however, they too may have been somewhat underpowered to detect differences.
Aspects of the traumatic event have also been investigated as potential risk factors for attrition. A few studies have observed that experiencing a greater number of traumas was related to increased risk for clinician-rated treatment attrition (Author citation; Author citation; Jensen et al., 2014); however, one study found that exposure to fewer traumas was tied to dropout (Chasson, Mychailyszyn, Vincent, & Harris, 2013). Complex trauma, defined as chronic interpersonal trauma that began early in life, was also unrelated to premature termination (Author citation). Similar to child demographic factors, it is difficult to draw conclusions regarding characteristics of the trauma and attrition at this time due to the limited research in this area.
Pretreatment symptoms have also been examined in relation to premature termination. In one national sample of children receiving general trauma-focused treatment, diagnoses of PTSD, depression, oppositional defiant disorder, and generalized anxiety disorder were related to dropout (Sprang et al., 2013). However, other studies have not observed relationships between levels of symptoms and attrition from trauma-focused cognitive behavioral therapy (TF-CBT; Yasinski et al., 2018) or have reported that only select symptoms corresponded with dropout, such as somatic complaints (Author citation) or rule-breaking and aggressive behavior (Author citation). Findings also may differ depending on how attrition was operationalized. For instance, in a sample of children who received TF-CBT, neither caregiver-reported behavioral difficulties nor trauma-related difficulties were associated with clinician-rated treatment attrition (Author citation). When symptoms were examined in relation to whether or not the child received an adequate dose of treatment, defined as 12 sessions or more, caregiver-reported rule-breaking behaviors and aggression corresponded with dropout from TF-CBT (Author citation). However, among children receiving general trauma-focused therapy, higher levels of somatic complaints were tied to both clinician-rated treatment dropout and increased likelihood that the child received an inadequate dose of treatment (Author citation).
Less attention has been devoted to researching children’s level of self-reported trauma-related difficulties in relation to attrition. Children’s self-reported symptoms were unrelated to clinician-rated treatment dropout among children receiving general trauma-focused therapy (Author citation; Sprang et al., 2013; Yasinski et al., 2018) and TF-CBT (Author citation). Further, children’s symptoms have not corresponded with whether or not the child received an adequate dose of treatment, providing further evidence that children’s reports of their symptoms may not be associated with premature termination (Author citation; Author citation). Yet two of the studies in this area only examined PTSD symptoms (Sprang et al., 2013; Yasinski et al., 2018) and did not assess other trauma-related difficulties. Additional work that examines multiple types of child-reported symptoms prior to more conclusively describing the role of children’s symptoms is needed in order to better understand the risk for attrition.
Current Study
There is a relative dearth of the literature regarding factors associated with premature termination from pediatric trauma-focused treatment, despite the significant implications of attrition and the utility in identifying risk factors for dropout. To date, only two prior studies have examined multiple trauma-related difficulties in relation to attrition, and these studies only examined symptoms in relation to attrition in a bivariate manner (Author citation; Author citation). As symptoms co-occur, it is important to assess these relationships simultaneously to determine which types of difficulties may predict attrition. Research is needed to more fully delineate whether there are pretreatment factors associated with increased risk for pediatric trauma-focused treatment. Establishment of these risk factors may ultimately help prevent trauma-focused dropout by identification of families who may be more vulnerable to dropout. The aim of the current study was therefore to build upon prior work and determine whether pretreatment symptoms were related attrition. As findings have differed depending on the operational definition of attrition and to be consistent with previous studies (Author citation; Author citation; Warnick et al., 2012), two operationalizations of attrition were used: (1) clinician-rated completion and (2) an adequate dose of treatment, or a minimum number of sessions to experience clinical benefit (Kazdin, Mazurick, & Siegel, 1994). Numerous families may complete a significant portion of treatment, experience-improved functioning, and then may terminate services early due to decreased need for treatment. Yet, per their clinicians, these families would still be defined as having prematurely terminated as they did not fully complete the protocol. Others may drop out due to perceptions that treatment is ineffective. The use of two definitions allows for a more comprehensive examination of predictors of premature termination.
Exposure to more traumatic events was expected to correspond with an increased risk for clinician-rated treatment dropout and that the child would receive an inadequate dose of treatment, consistent with prior studies (Author citation; Author citation; Jensen et al., 2014). As higher levels of pretreatment symptoms may increase levels of caregiver and family stress and have been previously predicted dropout (Author citation; Author citation; Sprang et al., 2013), higher levels of caregiver-reported internalizing, externalizing, and trauma-related difficulties were hypothesized to increase the risk for clinician-rated attrition and inadequate dose. Higher levels of child-reported trauma-related difficulties were similarly anticipated to be linked with an increased likelihood of both clinician-rated dropout and an inadequate dose of treatment.
Method
Participants
One hundred seventy-two treatment-seeking children aged 6–18 (M = 10.53, SD = 3.36) and their nonoffending legal guardian(s) were included in the study. The sample was 64% female, 36% male, and the racial/ethnic composition was as follows: 64% Black, 29.6% White, 5.2% Multiracial, and 1.2% Hispanic. Due to low cell sizes, racial/ethnic status was dichotomized into minority (70.3%) and nonminority status (29.7%). Over half of the children resided with their biological parents (61.6%; 6.4% other relatives, 5.8% adoptive parents, and 26.2% nonkinship foster care placements/residential treatment facilities). Child’s residence was dichotomized into two groups: living with a biological parent or not. Household income was rated categorically from 1 (<US$10,000) to 10 (>US$90,000) in increments of US$10,000; average income was 2.01 (SD = 1.26), corresponding to US$20,000–US$30,000. Over half of the children’s parents were never married (54%; 24.6% were divorced, 12.7% were married, and 8.7% were separated). All participants had experienced at least one traumatic event (M = 3.75, SD = 2.52; range 1–11). Children’s trauma exposure was as follows: 77.7% sexual abuse, 37.8% physical abuse, 37.2% death of a loved one, 34.3% witnessed domestic violence, 23.3% emotional abuse, 22.7% neglect, 17.4% community violence, 17.4% natural disaster, 12.2% serious injury/accident, 4.7% serious illness, 4.7% homicide, 2.9% suicide, and 2.3% war/terrorism.
Procedures
The study relied upon archival data from a sample of trauma-exposed children and their nonoffending legal guardians who were seeking trauma-focused services from a child advocacy center (CAC) in a Midwestern city who consented/assented to participate in research studies. At intake, children and their legal guardians completed a battery of clinical measures. Participants were included in the study if the caregiver or the child had completed at least one of the study measures (i.e., Child Behavior Checklist [CBCL], Trauma Symptom Checklist for Young Children [TSCYC], and/or the Trauma Symptom Checklist for Children [TSCC]), and the child was deemed appropriate for individually based, trauma-focused therapy by their clinician (e.g., having experienced a traumatic event and exhibiting clinical levels of trauma-related symptoms). There were no exclusionary criteria, and children did not need to be diagnosed with PTSD to be included in the study. Clinicians in the study included clinical psychologists, master’s-level social workers and counselors, and graduate students in these disciplines under the supervision of a licensed mental health professional. Of the full sample, 75.9% of the children completed the assessment and began therapy. All of treatment was individually based, weekly, and trauma focused. Of those who received treatment, 62.9% received TF-CBT, and the remaining 37.1% received other trauma-focused treatments (e.g., Integrative Treatment for Complex Trauma [ITCT]; Briere & Lanktree, 2008) or integrative trauma-focused therapy. All of the licensed therapists had been trained in TF-CBT and ITCT, and the trainees received weekly individual as well as group supervision in addition to weekly didactic trainings in TF-CBT and ITCT. At the end of treatment, clinicians reported which treatment intervention he or she used, as well as indicated whether the client had completed treatment or not. As this was a community-based clinical setting, fidelity to structured interventions such as TF-CBT was not routinely monitored for the subset of children who received TF-CBT. Since the content of the sessions was not monitored, it cannot be presumed that each of the sessions included trauma-focused content. Consistent with prior research to operationalize adequate dose (Author citation; Author citation; Warnick et al., 2012), children were rated as having received an adequate treatment dose if they attended 12 or more sessions. The number of sessions was selected from a comprehensive review of evidence-based pediatric treatments where the mean number of sessions required was 12 across interventions (Silverman et al., 2008) and is consistent with prior research (Author citation; Author citation; Warnick et al., 2012). The study was approved by the University of Missouri- St. Louis.
Measures
Demographics
At intake, children’s legal guardians completed a demographic measure that included questions such as child’s age, gender, race/ethnicity, household income, and parents’ marital status and education. The questionnaire also asks which type(s) of trauma the child experienced including sexual and physical abuse, neglect, domestic violence, serious injury/accident, natural disaster, community violence, death of a loved one, and serious illness.
CBCL/6–18 (Achenbach & Rescorla, 2001)
The CBCL is a 113-item caregiver-report measure for children aged 6–18 that comprehensively assesses children’s symptomatology. The CBCL has eight syndrome subscales: Anxious/Depressed, Withdrawn/Depressed, Somatic Complaints, Social Problems, Thought Problems, Attention Problems, Rule-Breaking Behavior, and Aggressive Behavior, as well as three broadband total scores; internalizing, externalizing, and total problems. Cronbach’s α range from 0.78 to 1.00 and content, construct, and criterion-related validity is well-documented (Achenbach & Rescorla, 2001). Due to differing age ranges across measures, the present study included 161 completed CBCLs. In the present study, Cronbach’s α = 0.94.
TSCYC (Briere, 2005; Briere et al., 2001)
The TSCYC is a 90-item caregiver-report measure that assesses PTSD symptoms and other trauma-related symptoms in children aged 3–12. The TSCYC yields clinical subscales for anxiety, depression, anger, posttraumatic stress symptoms (PTSS), dissociation, and sexual concerns. Items are rated on a 4-point Likert-type scale, 0 = never to 3 = almost all of the time/very often. The TSCYC has previously demonstrated good reliability, with αs ranging from 0.81 to 0.93, as well as good indices of convergent and divergent validity (Briere, 2005; Briere et al., 2001). There were 167 completed TSCYCs, Cronbach’s α was 0.96.
TSCC (Briere, 1996)
The TSCC is a 54-item self-report instrument to assess trauma-related symptoms in children aged 8–16. The TSCC provides clinical subscales for anxiety, depression, anger, PTSS, dissociation, and sexual concerns. Children rate their symptoms on a 4-point Likert-type scale, 0 = never to 3 = almost all of the time. The TSCC has evidence of satisfactory psychometrics properties, with αs ranging from 0.79 to 0.89, as well as adequate convergent, divergent, and predictive validity (Briere, 1996). In the current study, 139 completed TSCCs were included, Cronbach’s α = 0.92.
Attrition
At the end of treatment, clinicians reported whether or not the child had completed treatment (i.e., yes, no), and this was used to code clinician-rated treatment completion. The number of treatment sessions was recorded to calculate whether or not the child received an adequate dose of treatment.
Data Analysis
All statistical analyses were performed with SPSS for Windows, Version 25. Potential covariates that have been previously related to attrition (e.g., child age, gender, and race, child’s relationship to the rater, parental marital status, and CPS involvement) were examined using independent samples t tests, analysis of variance, and χ2 tests. Any variable found to be significantly related to either attrition definition was included in a separate block for that regression model. T tests and χ2 tests were utilized to assess the bivariate relationships between attrition and caregiver- and child-reported symptoms. In the event that multiple clinical subscales (e.g., Depression, Anxiety) from a specific measure were significantly associated (p < .05) with an attrition definition, a logistic regression model that included these subscales would then be computed to further examine these symptom difficulties simultaneously. As noted above, the study measures were completed by caregivers or children of differing ages, thus, separate regression models were anticipated to avoid reduced statistical power due to listwise deletion.
Results
Clinician-Rated Treatment Completion
Only approximately one quarter of the sample (26.2%) completed treatment per their clinician. For completers, the average number of sessions was 20.33 (SD = 6.11, range 12–30), and for noncompleters, the mean was 10.86 (SD = 6.11, range 1–27). Child’s age, gender, and minority status were unrelated to treatment completion (see Table 1). Parent’s marital status, whether he or she was accompanied to treatment by his/her biological parent or not, and CPS involvement were also not associated with attrition. Therefore, no demographic covariates were included in the regression models. Number of traumatic events was also unrelated to clinician-rated treatment completion.
Demographic Factors by Clinician-Determined Treatment Completion.

Note. CPS = Child Protective Services.
*p < .05. **p < .01. ***p < .001.
On the CBCL, Rule-Breaking Behavior and Aggression subscales were significantly related to attrition, with higher levels of these symptoms being tied to drop out, in accordance with the hypotheses (see Table 2). On the TSCYC, only the Anger subscale corresponded with attrition. None of the TSCC subscales were related to attrition. As only the CBCL had multiple subscales that were associated with clinician-rated dropout, only one regression model was computed to simultaneously examine both of these CBCL subscales. The regression model was significant, χ2(2,155) = 14.53, p = .001; Cox & Snell r2 = .09; Nagelkerke r2 = .13. Rule-breaking behavior was not significantly related to dropout, B = −.03 B SE = .02, odds ratio (OR) = 0.96, p = .21, and a statistical trend was noted for aggression, B = −.04 B SE = .02, OR = 0.95, p = .06, with higher levels of aggressive symptoms being marginally related to attrition.
Symptom Levels by Clinician-Determined Treatment Status.
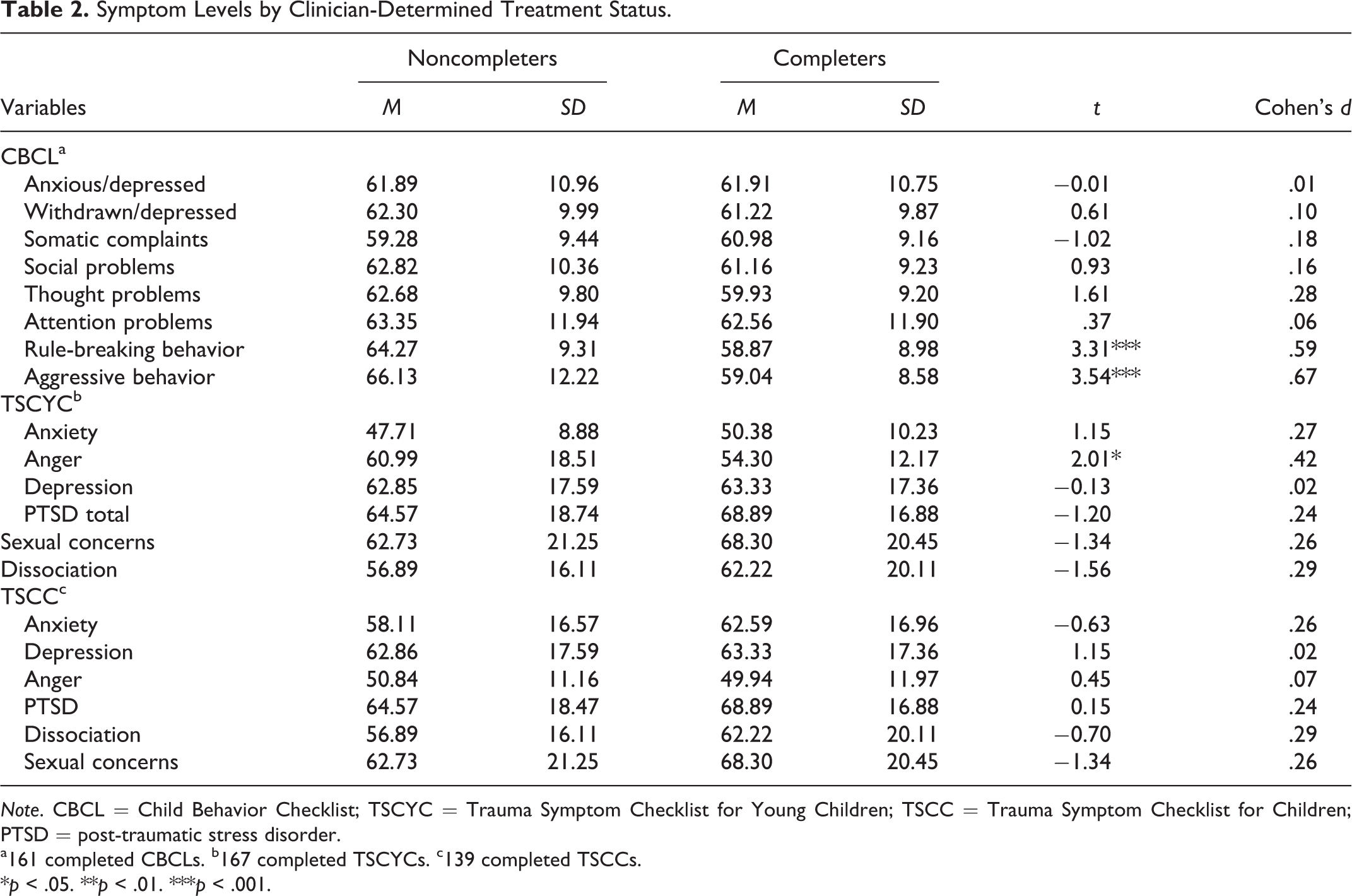
Note. CBCL = Child Behavior Checklist; TSCYC = Trauma Symptom Checklist for Young Children; TSCC = Trauma Symptom Checklist for Children; PTSD = post-traumatic stress disorder.
a161 completed CBCLs. b167 completed TSCYCs. c139 completed TSCCs.
*p < .05. **p < .01. ***p < .001.
Adequate Dose
Although only 26.2% of the children completed treatment per their clinician, 76.2% received an adequate dose of treatment. The average number of sessions for children who received an adequate dose of treatment was 19.33 (SD = 6.25, range 12–30), and for those who did not, the mean was 5.25 (SD = 4.03, range 1–11). Similar to clinician-rated treatment completion, child’s age, gender, and minority status, parent’s marital status, CPS involvement, whether the child was accompanied to treatment by his or her biological parent, and number of traumatic events were unrelated to adequate dose (see Table 3).
Demographic Factors by Adequate Dose Status.
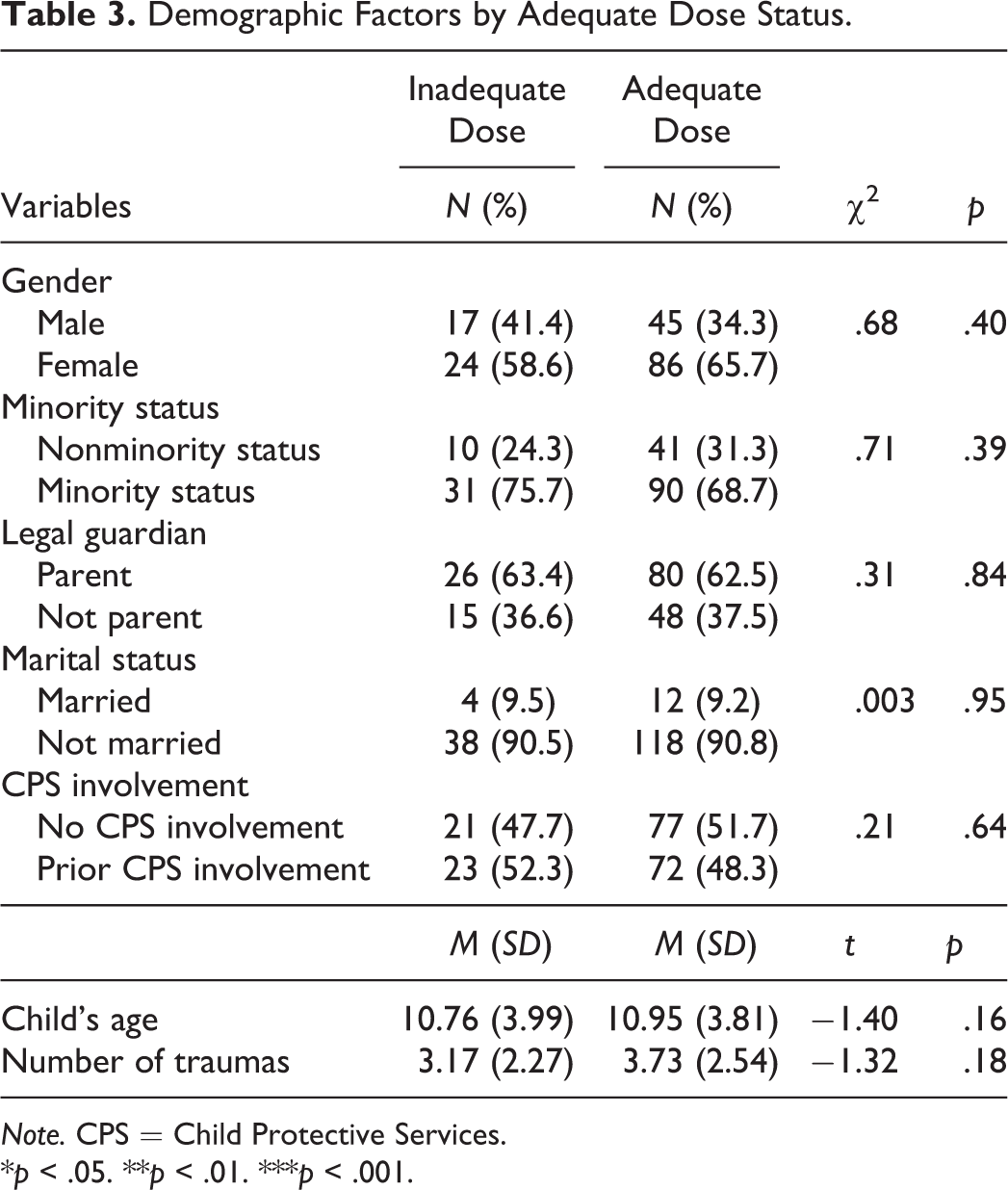
Note. CPS = Child Protective Services.
*p < .05. **p < .01. ***p < .001.
Despite expectations, higher levels of anxiety/depression symptoms and somatic complaints on the CBCL were related to the child having received an adequate dose of treatment (see Table 4). On the TSCYC, higher levels of anxiety, depression, anger, PTSD, and sexual concerns were also each associated with the child having received an adequate dose of treatment, whereas dissociative symptoms were unrelated. For child-reported difficulties on the TSCC, only higher levels of anxiety symptoms corresponded with the child having received an adequate dose of treatment. Two multivariate logistic regression models were computed for adequate dose, one for the CBCL and one for the TSCYC. For the CBCL, the regression model was significant, χ2(2,155) = 7.29, p = .02; however, neither anxiety/depression symptoms nor somatic complaints were significant predictors of adequate dose, B = .04 B SE = .02, OR = 1.04, p = .11; B = .02 B SE = .03, OR = 1.02, p = .40, respectively. Further, this model explained a relatively small amount of variance, Cox & Snell r2 = .04; Nagelkerke r2 = .07. For the TSCYC, the model was significant, χ2(5,121) = 18.25, p = .003; Cox & Snell r2 = .14; Nagelkerke r2 = .23, but only levels of sexual concerns were a significant predictor of adequate dose, B = .08 B SE = .03, OR = 1.09, p = .01. Anxiety, depression, anger, and PTSS were not significantly tied to adequate dose: B = .01 B SE = .02, OR = 1.01, p = .52; depression: B = −.007 B SE = .02, OR = 0.99, p = .79; anger: B = .01 B SE = .02, OR = 1.01, p = .48; PTSS: B = −.009 B SE = .02, OR = 0.99, p = .76.
Symptom Levels by Adequate Dose Status.

Note. CBCL = Child Behavior Checklist; TSCYC = Trauma Symptom Checklist for Young Children; TSCC = Trauma Symptom Checklist for Children; PTSD = posttraumatic stress disorder.
a161 completed CBCLs. b167 completed TSCYCs. c139 completed TSCCs.
*p < .05. **p < .01. ***p < .001.
Discussion
Relatively few children complete trauma-focused therapy (Author citation; Author citation; Cohen et al., 2011; Gillies et al., 2013; Scheeringa et al., 2011), and the research regarding factors associated with premature termination from pediatric trauma-focused treatment remains limited. Further, only two known studies to date have researched multiple trauma-related difficulties, and prior work did not investigate these relationships in a multivariate manner (Author citation; Author citation). The lack of work regarding attrition from pediatric trauma-focused treatment is unfortunate as identifying risk factors may help to specifically target high-risk families who may be more vulnerable to dropout and may ultimately help to prevent premature termination. The aim of the current study was to expand the prior pediatric trauma-focused literature and determine whether children’s pretreatment symptoms were related to two definitions of attrition: (1) clinician-rated treatment completion and (2) whether or not the child received an adequate dose of therapy.
It is important to note that rates of attrition were high in this sample—only 26.2% of children completed treatment per their clinician, consistent with prior work that has reported clinician-rated treatment completion rates of approximately 31–44% (Author citation; Author citation). Conversely, roughly three fourths (76.2%) of the sample received an adequate dose of treatment, also in line with previous studies that observed that 68–71% of children received an adequate treatment dose (Author citation; Author citation). The high discrepancy between the operational definitions of attrition has a few key implications. First, the results reiterate the need to understand, and decrease, the barriers to completing trauma-focused pediatric treatment. It is not clear that receiving 12 sessions is sufficient to mitigate trauma-related difficulties. Second, the risk for attrition after 12 sessions of treatment is very high as approximately half of the families who received an adequate dose failed to complete treatment. Trauma-exposed families may struggle to continue to attend treatment after a period of time for a variety of reasons. For some, families may experience some benefit, perceive that treatment is no longer needed, and drop out. Indeed, early treatment response, or achieving good clinical outcomes prior to the completion of a treatment protocol, is present in a significant portion of trauma-exposed children (Author citation). Relatedly, Deblinger, Mannarino, Cohen, Runyon, and Steer (2011) found that only eight sessions of TF-CBT were associated with significant treatment gains. Conversely, others may drop out after attending numerous sessions as they perceive treatment to be ineffective. Over time, the family’s level of resources may shift, or additional secondary adversities may arise, which may increase the risk for dropout. It is therefore critical to research not just when families drop out of treatment, but why. Third, the results underscore the need to examine attrition risk factors at different time points, particularly as the pattern of findings differed depending upon which operational definition was used. Far fewer relationships were observed for clinician-rated treatment completion compared to adequate dose. There may then be different risk factors for families who complete a significant portion of treatment but still drop out compared to those who complete the full treatment protocol.
Child demographic and family factors were consistently unrelated to both definitions of attrition. Demographic factors have not routinely corresponded with attrition (Author citation; Author citation; Cohen & Mannarino, 1996; Jensen et al., 2014; Sprang et al., 2013; Yasinski et al., 2018), although prior work has found that CPS involvement was a risk factor for clinician-rated treatment completion, but not adequate dose (Author citation; Author citation). It is not clear why CPS involvement was unrelated to clinician-rated treatment completion in the current sample. Nevertheless, as CPS involvement has not previously corresponded with adequate dose, this factor may not predict initial engagement in treatment. In general, the results of the present and previous studies indicate that child demographic and family factors, at least those assessed by the previous studies, likely have weak ties, if any, to drop out.
Number of traumatic events was also unrelated to both attrition definitions, in contrast to prior work that reported that a greater number of traumas predicted risk for clinician-rated treatment dropout, but not adequate dose status (Author citation; Author citation). However, one study observed that fewer traumatic events corresponded with attrition (Chasson et al., 2013). It is possible that there are subgroups of trauma-exposed families. For example, some families who have experienced more traumatic events may drop out due to higher levels of stress, whereas those who have experienced more acute traumas may be at higher risk of attrition due to lower perceived need for treatment. The links between aspects of the trauma exposure and premature termination are likely complicated and merit further attention in future studies, particularly those that examine dropout at differing points in therapy.
With regard to caregiver-reported symptoms on the CBCL, externalizing difficulties such as rule-breaking behavior and aggression were bivariate risk factors for clinician-rated treatment dropout, replicating prior work (Author citation; Author citation). While the overall regression model was significant, neither predictor was significant in the model, which suggests that when the predictors are added together, they account for a significant portion of the variance in clinician-rated attrition; however, on their own, they are not associated with dropout. For adequate dose, higher levels of anxiety/depression symptoms and somatic complaints were related to the child receiving an adequate dose of treatment. Still, neither factor was a significant predictor in a multivariate model, indicating that these symptoms have a weak relationship to adequate dose group status.
When caregiver-reported trauma-related difficulties were investigated, trauma-related anger was also related to clinician-rated attrition. Difficulties with anger have not previously been identified as an attrition risk factor in the only two studies that examined this variable (Author citation; Author citation), although this aligns with the idea that higher levels of externalizing symptoms broadly play a role, albeit a small one, in increased risk of dropout. Unlike clinician-rated treatment completion, all but the Dissociation subscale on the TSCYC initially corresponded with adequate dose, although only sexual concerns remained a significant predictor when examined simultaneously. Thus, higher levels of trauma-related difficulties, particularly sexual concerns, may then predict attendance for therapy initially, but pretreatment perceptions of symptoms may not be a long-term predictor of attrition. Higher levels of sexualized behaviors may prompt treatment completion due to the distressing nature of these difficulties, which may also be viewed as being particularly likely to be a by-product of the trauma. Only two prior studies have examined the TSCYC in relation to attrition, neither of which reported significant relationships (Author citation; Author citation). Additional replication studies will be helpful in making sense of discrepant findings.
Children’s self-reported symptoms were unrelated to clinician-rated treatment completion, in line with previous studies (Author citation; Author citation). For adequate dose, higher levels of anxiety symptoms were related to whether the child received an adequate dose of treatment. The present study is the first study to indicate a relationship between child-reported symptoms and adequate dose. Still, taken together, children’s pretreatment symptoms may not have strong ties to attrition, although they may be more predictive of dropout at earlier points in therapy. As children are likely not the literal or figurative drivers for treatment initiation and continuation, it is not terribly surprising that their own reports of their symptoms would not play a large role in understanding attrition. However, perhaps children’s symptoms are more likely to be a factor over the course of treatment, compared to at intake, particularly when examining clinician-rated treatment completion.
Limitations and Conclusions
Although the current study contributes to the small literature regarding attrition from pediatric trauma-focused therapy, the results should be contextualized in relation to their limitations. Most importantly, fidelity to the intervention was not assessed. For families who received structured treatment, fidelity to the intervention was not routinely assessed, which may be an important factor for structured treatments (e.g., TF-CBT). Therefore, the content of the sessions cannot be evaluated to determine whether the clinician was utilizing TF-CBT or other trauma-focused treatment strategies within each session. As this study was conducted at a CAC, it is likely that treatment was centered on trauma-focused approaches; however, it is possible that other, nontrauma-related content was covered in the sessions. Thus, it cannot be presumed that the groupings of “adequate” and “inadequate” treatment dose are specific to a trauma-focused treatment and instead represent individual treatment delivered in a child trauma specialty clinic. This is a major limitation of the study, and future research that monitors fidelity to an intervention, when able, is critical. Relatedly, years of experience is another therapist variable that was not monitored, and years of clinician experience, particularly regarding TF-CBT, may also be an important factor in predicting attrition.
Families who dropped out prior to completing an intake were not able to be included due to a lack of completed measures. However, these families represent a key subgroup, as those who attend only one intake session may have unique risk factors for attrition. The study relied on pretreatment symptoms; however, caregiver’s perceptions of children’s symptoms likely, and should, change over the course of treatment, and these perceptions likely influence motivation to continue or discontinue treatment. Future studies should further examine when the family terminated from therapy as there may be different risk factors at different points during trauma-focused treatment (e.g., prior to, during, or after trauma-processing). Further, families who seek treatment from a CAC, which is a child trauma specialty clinic, are likely a select subsample of trauma-exposed, treatment-seeking families. The use of this sample may introduce setting-specific confounds such as severity of trauma exposure and symptoms. It is therefore unclear whether the results would generalize to other more general treatment settings that provide trauma-focused services.
Other potential factors related to attrition, including therapeutic alliance and caregiver stress (Kazdin et al., 1997), were not assessed in the present study but should be included in future studies. Future research should prioritize including factors such as therapeutic alliance and other therapist variables, as well as aspects of treatment such as fidelity. Adequate treatment dose was defined as having received 12 or more sessions, yet approximately 50% of families who received an adequate dose did not complete treatment per their clinician. The number of sessions deemed to be a sufficient dose of treatment was based on a review of pediatric treatments which found that the mean number of sessions was 12, and this definition has been previously used in attrition research (e.g., Author citation; Author citation; Warnick et al., 2012). However, trauma-focused treatment may require a higher or lower (Deblinger et al., 2011) number of sessions to constitute an adequate dose compared to other psychological conditions. Thus, research is needed to determine the optimal number of sessions needed to make gains from trauma-focused treatment. Families may also have very different perceptions of appropriate length of time and treatment goals than clinicians. Future research should explore caregiver and child perceptions of trauma-focused treatment goals, length, and reasons for dropout.
In spite of these limitations, the present study is one of the first to examine caregiver- and child-reported trauma-related difficulties in relation to both clinician-rated treatment completion and whether the child received an adequate dose of treatment. The results replicate previous findings that child and family characteristics are not associated with either clinician-rated treatment completion or adequate dose (Author citation; Author citation). The findings thus support the preliminary conclusion that caregiver-reported and child-reported pretreatment symptoms are largely unrelated to clinician-rated treatment completion. Caregiver’s and children’s reports of certain symptoms appear to play a small role in predicting whether they will attend a portion of treatment, which may be due to this factor being assessed more proximally in time, thereby closer to the pretreatment ratings. The findings also signal the need to understand the process of attrition at different time points and identify stronger risk factors for attrition to help trauma-exposed families achieve good clinical outcomes. The high number of families who received at least 12 sessions of treatment and the lack of pretreatment attrition risk factors observed in the present study, including for factors previously thought to be related to attrition such as minority status, CPS involvement, and number of traumatic events, is positive. Thus, these findings indicate that, for many families, trauma-focused clinicians have a significant amount of time to engage families and work to mitigate trauma-focused difficulties.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.